UHMWPE | XLPE Manufacturing | Wear Reduction | Clinical Outcomes
- UHMWPE: molecular weight 3-6 million Da (1000x higher than standard polyethylene)
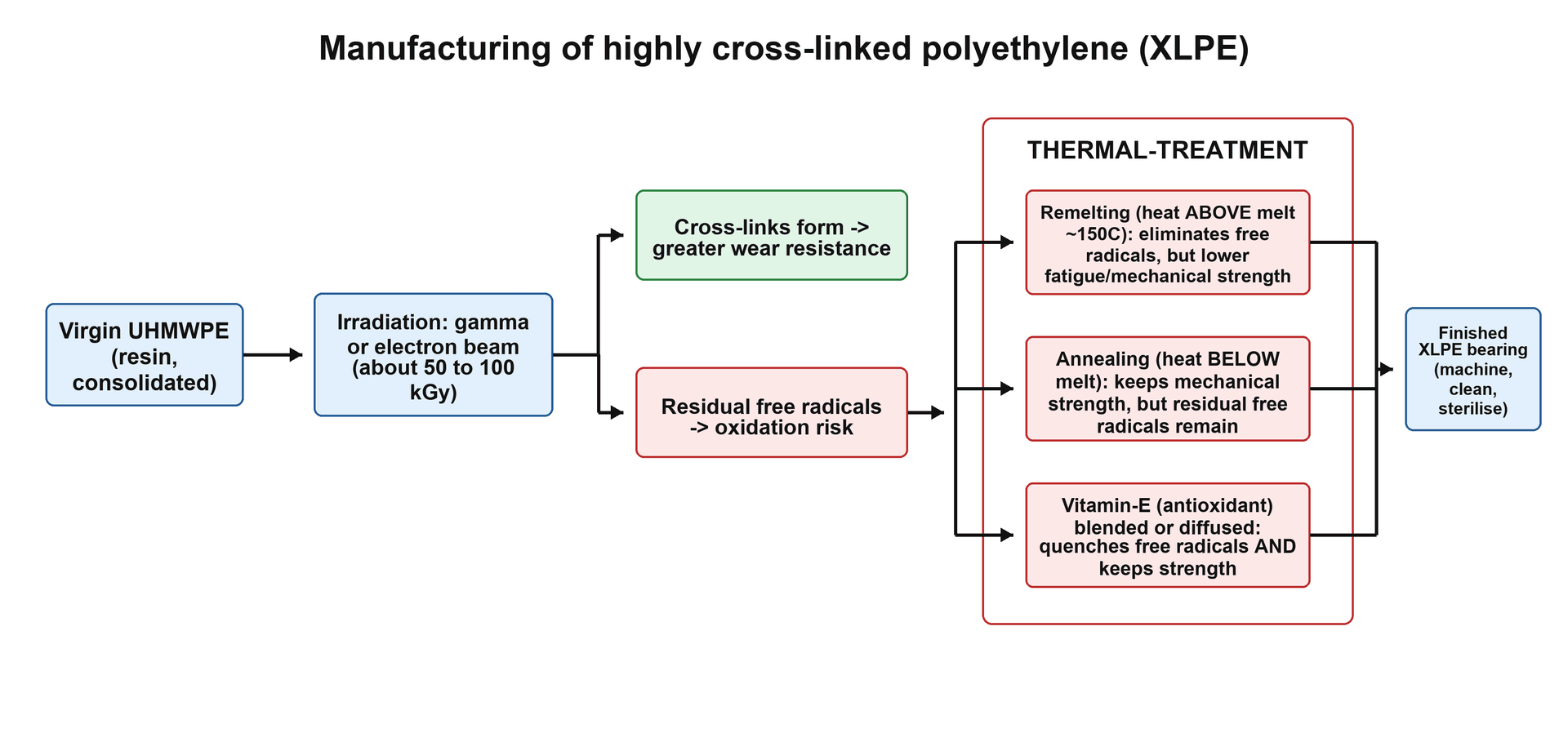
- XLPE manufacturing: high-dose radiation (50-100 kGy) creates crosslinks, then thermal treatment removes free radicals
- Remelting (above 137C) eliminates all free radicals but reduces crystallinity and toughness
- Annealing (below 137C) preserves crystallinity but leaves some free radicals (slower oxidation)
- XLPE reduces volumetric wear 90% but has reduced fracture toughness (minimum 6-8mm thickness required)
- “Conventional PE gamma sterilized in air oxidizes over time, causing delamination and fatigue failure
- “XLPE trade-off: increased wear resistance vs decreased fracture toughness and impact strength
- “Vitamin E stabilized PE: antioxidant prevents oxidation without reducing toughness as much
- “Minimum XLPE liner thickness 6-8mm to prevent rim fracture and maintain fatigue resistance
Molecular weight 3-6 million Da. Linear chains of ethylene monomers (C2H4). High molecular weight provides strength and toughness. Semicrystalline: 40-50% crystalline, 50-60% amorphous regions.
Radiation creates C-C bonds between chains. Gamma or e-beam (50-100 kGy) breaks C-H bonds, creating free radicals. Radicals recombine forming crosslinks. Increases wear resistance but reduces toughness.
Remelting (over 137C): Eliminates free radicals completely, reduces crystallinity. Annealing (below 137C): Preserves crystallinity, leaves residual free radicals. Trade-off: oxidation resistance vs mechanical properties.
Conventional PE: 0.1-0.2mm/year linear wear. XLPE: under 0.05mm/year (90% reduction). Volumetric wear below osteolysis threshold. 15+ year data confirms durability and low revision rates.
Overview and Introduction
Polyethylene has been the primary bearing surface material in total joint arthroplasty for over 50 years. Ultra-high molecular weight polyethylene (UHMWPE) provides excellent wear resistance and biocompatibility, but conventional formulations generated wear particles causing osteolysis. Highly crosslinked polyethylene (XLPE) reduces wear by 90 percent through radiation-induced crosslinking, dramatically improving implant longevity.
Historical Context
Evolution of Polyethylene in Arthroplasty
Timeline of polyethylene development:
1960s-1970s: Introduction of UHMWPE
- Sir John Charnley pioneered use of UHMWPE in total hip arthroplasty
- Low friction arthroplasty: metal femoral head on UHMWPE acetabular cup
- Sterilized by gamma radiation in air (25-40 kGy)
- Wear rates: 0.1-0.2mm/year, acceptable for era
1980s-1990s: Oxidation problems emerge
- Long-term follow-up revealed osteolysis from wear particles
- Shelf aging: gamma sterilized PE oxidized during storage
- In vivo oxidation: continued degradation after implantation
- Delamination and catastrophic failures (Hylamer disaster)
1990s-2000s: Development of XLPE
- Recognition that crosslinking reduces wear
- First generation XLPE: high-dose radiation with remelting
- 90% reduction in wear rates demonstrated
- Trade-off: reduced fracture toughness
2000s-present: Refinement and optimization
- Annealed XLPE: better mechanical properties
- Vitamin E stabilized: antioxidant protection
- Long-term data: 15+ years confirms durability
- XLPE becomes standard of care
Principles of Polyethylene Engineering
Fundamental Principles of Polyethylene Engineering
Polymer Chemistry Basics:
Polyethylene is a simple polymer consisting of repeating ethylene (C2H4) units forming long chains:
- Monomer: Ethylene (-CH2=CH2-)
- Polymer: Polyethylene (-CH2-CH2-)n
- Chain length: Determined by molecular weight (higher MW = longer chains)
Molecular Weight and Properties:
- Low MW (under 100k)
- Low
- High MW (1M)
- Moderate
- UHMW (3-6M)
- High
- Low MW (under 100k)
- Brittle
- High MW (1M)
- Moderate
- UHMW (3-6M)
- Excellent
- Low MW (under 100k)
- Poor
- High MW (1M)
- Moderate
- UHMW (3-6M)
- Excellent
- Low MW (under 100k)
- Easy (melt flow)
- High MW (1M)
- Moderate
- UHMW (3-6M)
- Difficult (cannot melt)
Crystallinity and Structure:
UHMWPE is semicrystalline:
- Crystalline regions (40-50%): Ordered lamellae provide strength
- Amorphous regions (50-60%): Disordered entangled chains provide toughness
- Chain folding: Polymer chains fold back and forth in crystalline lamellae
- Tie molecules: Chains connecting crystalline regions through amorphous zones
How Crystallinity Affects Properties:
- Higher crystallinity = greater strength and stiffness
- Lower crystallinity = better toughness and ductility
- Remelting XLPE reduces crystallinity (30-35%) sacrificing toughness for oxidation resistance
Crosslinking Chemistry
- Radiation breaks C-H bonds: Ionizing radiation knocks hydrogen atoms off carbon backbone
- Carbon radical formation: Carbon atoms with unpaired electrons (R-C•)
- Radical recombination: Adjacent radicals combine forming C-C bonds (crosslinks)
- Network formation: Crosslinks create three-dimensional polymer network
- Dose-response: Higher radiation = more crosslinks = better wear resistance
- Diminishing returns: Above 100 kGy, mechanical properties degrade excessively
- Optimal dose: 50-100 kGy balances wear reduction and mechanical properties
- Restrict chain mobility (chains cannot slide past each other)
- Increase hardness and scratch resistance
- Reduce adhesive wear (less material transfer)
- Reduce abrasive wear (harder to plough)
- Chains cannot slide to dissipate energy (less ductility)
- Network cannot elongate before fracture (lower impact strength)
- Crack propagation easier (less energy absorption)
UHMWPE Structure and Properties
Molecular Structure
Ultra-High Molecular Weight Polyethylene (UHMWPE) is a linear polymer of ethylene monomers (C2H4) with extremely high molecular weight.
Key structural features:
- Linear chains: Repeating -CH2-CH2- units forming long polymer chains
- Molecular weight: 3-6 million Daltons (1000x higher than standard polyethylene)
- Semicrystalline: 40-50% crystalline lamellae, 50-60% amorphous regions
- Entanglement: Long chains entangle providing strength and toughness
Physical Properties
- Standard PE
- 20,000-40,000 Da
- UHMWPE
- 3-6 million Da
- Clinical Significance
- Higher MW = greater strength and toughness
- Standard PE
- 20-30 MPa
- UHMWPE
- 40-50 MPa
- Clinical Significance
- UHMWPE can withstand higher loads
- Standard PE
- Low
- UHMWPE
- High
- Clinical Significance
- UHMWPE suitable for bearing surface
- Standard PE
- Melt processable
- UHMWPE
- Not melt processable
- Clinical Significance
- UHMWPE requires compression molding or RAM extrusion
Why UHMWPE cannot be melted and molded:
- Viscosity too high (chains too long and entangled)
- Requires compression molding from powder or RAM (resin as molded) extrusion
- GUR resin: most common starting material (compression molded sheets)
Medical-Grade Resin: GUR Grades and the Calcium Stearate Story
Implant UHMWPE begins as a fine resin powder (polymerised by the Ziegler process) supplied under the GUR trade designation. Two medical grades dominate, differing chiefly in molecular weight; the four-digit code is informative - the second digit historically denoted the presence (1) or absence (0) of calcium stearate, and the third digit tracks molecular weight (2 lower, 5 higher).
- Approx. molecular weight
- approximately 3.5 million Da
- Calcium stearate
- None (modern grade)
- Typical use
- Marginally better fatigue/fracture resistance; favoured for tibial inserts
- Approx. molecular weight
- approximately 5.5 to 6 million Da
- Calcium stearate
- None (modern grade)
- Typical use
- Higher molecular weight, most wear resistant; common for acetabular liners
- Approx. molecular weight
- 1120 lower, 1150 higher
- Calcium stearate
- Calcium stearate added
- Typical use
- Withdrawn from modern implant use because of stearate-related fusion defects
Calcium stearate was historically added as a processing aid and acid scavenger. It was implicated in fusion defects - poorly consolidated micro-regions (classically called "Type 1" defects, or "white specks"/"dimples") that act as crack-initiation sites and reduce fatigue strength. Modern implant resins (GUR 1020 and 1050) are therefore supplied calcium-stearate-free.
Both modern medical resins are calcium-stearate-free; the practical difference is molecular weight. GUR 1050 has the higher molecular weight (approximately 5.5 to 6 million Da) and the best wear resistance, favouring acetabular bearings, whereas GUR 1020 (approximately 3.5 million Da) offers marginally better resistance to fatigue crack propagation, useful where cyclic contact stress is high. The historical lesson is that calcium stearate in the older 1120/1150 grades caused fusion defects and was abandoned.
Biocompatibility
UHMWPE is highly biocompatible:
- Inert: No toxic degradation products
- Non-allergenic: No hypersensitivity reactions
- Stable: Does not corrode or dissolve in biological fluids
- Limitation: Wear particles activate macrophages causing osteolysis (size-dependent: 0.1-10 microns)
Conventional UHMWPE and Historical Problems
Gamma Sterilization in Air
Historical conventional PE was sterilized with gamma radiation (25-40 kGy) in air.
- Sterilization: Kill bacteria and spores
- Dose: 25-40 kGy (lower than XLPE crosslinking)
- Result: Sterile implant ready for surgery
- Problem: Unintended oxidation in presence of air
- Free radicals: Radiation creates C-H bond breaks
- Oxygen reaction: Radicals react with O2 forming peroxides
- Chain scission: Peroxides break polymer chains over time
- Degradation: Loss of mechanical properties, delamination
Shelf Aging and In Vivo Oxidation
- Gamma sterilized PE stored in air oxidizes over months to years
- Mechanical properties deteriorate before implantation
- Surface becomes brittle and prone to delamination
- Implanted PE continues to oxidize in the body (oxygen from synovial fluid)
- Accelerated by lipids in synovial fluid
- Leads to subsurface cracking, delamination, and accelerated wear
Hylamer PE (1990s) - worst case example: Sterilized with gamma in air, then packaged in air. Severe oxidation caused catastrophic delamination and osteolysis within 5-10 years. Led to widespread recalls and revisions. Lesson: oxidation is the enemy of PE longevity.
The Subsurface "White Band" and How Oxidised Polyethylene Fails
The damage from gamma-air sterilisation is concentrated beneath the surface, not on it. As oxygen diffuses inward and reacts with the radiation-generated free radicals, the oxidation rate peaks a short distance below the surface - producing a brittle, embrittled zone roughly 1 to 2mm deep that appears as a subsurface "white band" on thin sections and corresponds to a peak in the oxidation index measured by FTIR.
Its clinical importance is one of unfortunate geometry: the depth of maximum oxidation coincides with the depth of maximum subsurface shear (von Mises) stress generated by a non-conforming articulation - precisely the situation in the knee. A brittle band sitting exactly where cyclic stress peaks is the recipe for delamination: a crack initiates at or below the white band and propagates parallel to the surface until a sheet of polyethylene lifts off.
- Appearance
- Smooth, shiny region
- Mechanism
- Adhesive removal of surface asperities
- Where it dominates
- Hip (conforming, low contact stress)
- Appearance
- Small surface craters
- Mechanism
- Localised surface fatigue, third-body indentation
- Where it dominates
- Knee
- Appearance
- Sheet-like lift-off, subsurface crack
- Mechanism
- Subsurface fatigue at the oxidised white band under high contact stress
- Where it dominates
- Knee (the classic oxidised-PE failure)
- Appearance
- Linear scratches, embedded particles
- Mechanism
- Third-body (cement, bone, metal) abrasion
- Where it dominates
- Both
This is why oxidation matters far more for the knee than the hip. The conforming, low-stress hip bearing wears mainly by adhesion and abrasion and tolerates a degree of oxidation, whereas the non-conforming, high-contact-stress knee bearing is vulnerable to fatigue-driven delamination once a brittle band develops. It is also why the oxidation index (carbonyl-peak ratio on FTIR) is the standard retrieval and quality-control metric, and why every modern strategy - inert-gas sterilisation, barrier packaging, post-irradiation remelting and antioxidant (vitamin E) stabilisation - is aimed at preventing this subsurface band from ever forming.
The oxidation maximum sits about 1 to 2mm below the surface (the "white band"), exactly where the subsurface shear stress peaks under a non-conforming knee articulation. A brittle layer at the depth of peak cyclic stress drives delamination - the catastrophic failure mode of gamma-air-sterilised, shelf-aged tibial inserts (epitomised by the Hylamer experience). The conforming, low-stress hip is far more forgiving, which is why oxidation-driven delamination is fundamentally a knee problem.
Solution Approaches
- Mechanism
- Sterilize in nitrogen or argon (no oxygen)
- Effectiveness
- Prevents shelf aging, some in vivo oxidation
- Current Use
- Replaced by XLPE, rarely used
- Mechanism
- No radiation, no free radicals
- Effectiveness
- No oxidation, but no crosslinking
- Current Use
- Some conventional PE liners use this
- Mechanism
- Vacuum seal prevents oxygen contact
- Effectiveness
- Effective for shelf storage
- Current Use
- Standard for conventional PE if used
Highly Crosslinked Polyethylene (XLPE)
Crosslinking Concept
Crosslinking creates covalent C-C bonds between polymer chains, forming a three-dimensional network.
Mechanism:
- Irradiation: Gamma or e-beam radiation (50-100 kGy) breaks C-H bonds
- Free radical formation: Hydrogen atoms removed, leaving carbon radicals
- Recombination: Adjacent radicals combine forming C-C crosslinks
- Network formation: Crosslinks restrict chain mobility and increase wear resistance
Manufacturing Methods
Remelting Method (First Generation XLPE)
- Irradiation: Gamma or e-beam (50-100 kGy) in inert atmosphere
- Crosslinking: C-C bonds form between chains
- Remelting: Heat above melting point (over 137C, typically 150C)
- Cooling: Controlled cooling to room temperature
- Machining: Fabricate into liners
- Eliminate all free radicals: Heating allows radicals to recombine or be quenched
- Prevent oxidation: No residual radicals means no oxygen reaction
- Shelf stability: Can be stored indefinitely without degradation
- Crystallinity reduced: Melting destroys crystalline lamellae, reduces from 45% to 30-35%
- Toughness reduced: Lower crystallinity means lower fracture toughness and impact strength
- Fatigue resistance reduced: More prone to crack propagation under cyclic loading
Remelted XLPE requires minimum 6-8mm thickness to prevent rim fracture.
This completes the remelting method description.
Wear Performance
- Linear Wear Rate
- 0.1-0.2 mm/year
- Volumetric Wear
- 40-60 mm³/year
- Osteolysis Rate (15 years)
- 15-30%
- Linear Wear Rate
- 0.08-0.15 mm/year
- Volumetric Wear
- 30-50 mm³/year
- Osteolysis Rate (15 years)
- 10-20%
- Linear Wear Rate
- under 0.05 mm/year
- Volumetric Wear
- under 10 mm³/year
- Osteolysis Rate (15 years)
- under 5%
- Linear Wear Rate
- under 0.05 mm/year
- Volumetric Wear
- under 10 mm³/year
- Osteolysis Rate (15 years)
- under 5%
Clinical significance:
- XLPE reduces wear 90% compared to conventional PE
- Linear wear below 0.1mm/year threshold for osteolysis
- Volumetric wear below critical 40-50 mm³/year threshold
- Osteolysis rates dramatically reduced with XLPE
Anatomy
Polymer Morphology and Microstructure:
- Ordered lamellae of folded polymer chains
- Chain-folded crystals approximately 10-50nm thick
- Orthorhombic crystal structure (most stable)
- Mechanical strength and stiffness
- Wear resistance (hard crystalline phase)
- Chemical resistance
- Disordered, entangled polymer chains
- Random coil configuration
- Tie molecules connecting crystalline lamellae
- Toughness and impact resistance
- Ductility (ability to deform before fracture)
- Energy absorption
- Crystalline Phase
- Higher (1.00 g/cm³)
- Amorphous Phase
- Lower (0.855 g/cm³)
- Clinical Relevance
- Overall density reflects crystallinity
- Crystalline Phase
- High (provides rigidity)
- Amorphous Phase
- Low (flexible)
- Clinical Relevance
- Crystallinity determines stiffness
- Crystalline Phase
- Brittle on own
- Amorphous Phase
- High (energy absorption)
- Clinical Relevance
- Amorphous phase critical for impact resistance
- Crystalline Phase
- Low (ordered structure)
- Amorphous Phase
- High (gaps between chains)
- Clinical Relevance
- Lipid absorption occurs in amorphous phase
UHMWPE is semicrystalline - neither fully crystalline nor fully amorphous. The crystalline lamellae provide strength and wear resistance, while amorphous regions provide toughness. Tie molecules bridge between crystalline regions through amorphous zones, creating a strong interconnected network. Remelting XLPE reduces crystallinity from 45% to 30-35%, explaining the reduced toughness.
Classification
Classification of Polyethylene Types in Arthroplasty:
- Type
- Conventional UHMWPE
- Manufacturing
- Gamma sterilized in air (25-40 kGy)
- Key Features
- Oxidation and shelf aging problems
- Type
- Improved conventional PE
- Manufacturing
- Gamma in inert gas or barrier packaging
- Key Features
- Reduced shelf aging, some oxidation
- Type
- First-gen XLPE (remelted)
- Manufacturing
- 50-100 kGy + remelting (greater than 137°C)
- Key Features
- 90% wear reduction, reduced toughness
- Type
- Annealed XLPE
- Manufacturing
- 50-100 kGy + annealing (less than 137°C)
- Key Features
- Better toughness, some residual radicals
- Type
- Vitamin E XLPE
- Manufacturing
- Vitamin E blending or diffusion
- Key Features
- Antioxidant protection, maintained toughness
- Temperature greater than 137°C (melting point)
- All free radicals eliminated
- Crystallinity reduced (30-35%)
- Toughness reduced 20-30%
- Temperature less than 137°C
- Residual free radicals (5-10%)
- Crystallinity preserved (40-45%)
- Better mechanical properties
- Most common application
- Fixed or modular liners
- XLPE standard of care
- Higher conformity than THA
- Lower cross-shear wear
- XLPE increasingly used
- Glenoid components (TSA)
- Dual mobility constructs
- Constrained liners
XLPE can be classified by thermal treatment:
- First-generation XLPE = remelted (eliminates radicals, reduces toughness)
- Second-generation XLPE = annealed (preserves toughness, some radicals remain)
- Third-generation XLPE = vitamin E stabilized (antioxidant protection without toughness loss)
All generations achieve approximately 90% wear reduction compared to conventional PE.
Investigations
Quality Control and Clinical Assessment Methods:
- Tensile strength (ASTM D638)
- Impact strength (Izod/Charpy)
- Crystallinity (DSC - differential scanning calorimetry)
- Oxidation index (FTIR spectroscopy)
- Crosslink density (gel content, swell ratio)
- Free radical content (ESR spectroscopy)
- Linear penetration (mm/year)
- Compare to baseline post-op X-ray
- Software-assisted measurement (PolyWare, RSA)
- 3D volumetric wear analysis
- More accurate than plain X-ray
- Research setting primarily
- Accuracy
- ±0.5-1.0mm
- Advantages
- Widely available, low cost
- Limitations
- Low precision, requires consistent positioning
- Accuracy
- ±0.1-0.2mm
- Advantages
- Better precision, standardized method
- Limitations
- Software required, still 2D limitation
- Accuracy
- ±0.01-0.05mm
- Advantages
- Highest precision, gold standard research
- Limitations
- Requires tantalum beads at surgery, expensive
- Accuracy
- ±0.05-0.1mm
- Advantages
- 3D analysis, no beads needed
- Limitations
- Higher radiation, cost, research setting
Linear wear rate is measured as femoral head penetration into the liner (mm/year). With XLPE, expect less than 0.05mm/year (often unmeasurable on plain X-rays). Bedding-in (initial creep) occurs in first 1-2 years and should not be confused with true wear. Subtract baseline post-op X-ray position from follow-up measurements.
Management
Implant Selection and Decision-Making:
First-line choice for THA:
- XLPE preferred over conventional PE (90% wear reduction)
- AOANJRR data confirms lower revision rates
- Cost-effective long-term despite higher initial cost
No routine indication for conventional PE in THA
- Age and activity level (XLPE for all)
- Acetabular size (affects liner thickness)
- Expected lifespan (younger = more cycles)
- Minimum 6-8mm liner thickness
- Head size selection
- Cup design compatibility
- PE Type
- XLPE
- Head Size
- 32-36mm
- Rationale
- Standard of care, balance stability and thickness
- PE Type
- XLPE
- Head Size
- 28-32mm (smaller head)
- Rationale
- Maintain 6-8mm thickness, sacrifice head size
- PE Type
- XLPE
- Head Size
- 36-40mm
- Rationale
- Larger head for stability if adequate thickness
- PE Type
- XLPE
- Head Size
- Based on shell size
- Rationale
- Always XLPE in revision to minimize future wear
Balance head size with liner thickness:
- Larger head = better stability (higher jump distance, greater ROM)
- Larger head = thinner liner (for same cup size)
- Rule: Never sacrifice minimum 6-8mm thickness for larger head size
- 32mm head with 8mm liner is safer than 40mm head with 4mm liner
Surgical Technique
Liner Selection and Intraoperative Considerations:
- Cup outer diameter determines liner options
- Head size selected based on liner thickness
- Offset options (neutral, elevated lip, lateralized)
- 32mm head: ~10mm liner thickness (ideal)
- 36mm head: ~8mm liner thickness (acceptable)
- 40mm head: ~6mm liner thickness (minimum)
Final decisions made after reaming:
- Confirm final cup size after press-fit
- Select liner to achieve adequate thickness
- Choose offset for stability optimization
- Trial before final implantation
- Description
- Standard liner, symmetric
- Indication
- Standard primary THA
- Trade-off
- Baseline stability, no impingement risk
- Description
- Asymmetric raised rim
- Indication
- High dislocation risk, revision
- Trade-off
- Better posterior stability, may cause impingement if malpositioned
- Description
- Offset center of rotation laterally
- Indication
- Abductor tension, leg length
- Trade-off
- Increases offset, may thin medial wall
Ensure complete liner seating:
- Modular liners must fully engage locking mechanism
- Incomplete seating = micromotion = accelerated backside wear
- Confirm circumferential seating with visual and tactile check
- Some designs use audible "click" confirmation
Complications
PE wear particles cause osteolysis:
- Particles 0.1-10 microns activate macrophages
- Release of IL-1, IL-6, TNF-alpha, PGE2
- Osteoclast activation and bone resorption
- Progressive bone loss around implants
XLPE reduces wear 90% - dramatically lower osteolysis
- Rim fracture (reduced toughness)
- Fatigue failure (thin liners)
- Oxidation (annealed XLPE, long-term)
Minimum 6-8mm thickness, proper cup positioning
- Conventional PE
- 15-30% at 15 years
- XLPE
- Under 5% at 15 years
- Prevention
- XLPE reduces wear particles below osteolysis threshold
- Conventional PE
- Possible with high wear rates
- XLPE
- Extremely rare
- Prevention
- Annual surveillance X-rays
- Conventional PE
- Rare (high toughness)
- XLPE
- Reported (reduced toughness)
- Prevention
- Minimum 6-8mm thickness, proper cup position
- Conventional PE
- High (if gamma in air)
- XLPE
- Low with proper manufacturing
- Prevention
- Remelting, annealing, or vitamin E
Osteolysis is the main reason for PE-related revision:
- Caused by macrophage reaction to wear particles
- Leads to bone loss, component loosening, periprosthetic fracture
- Threshold: approximately 40-50 mm³/year volumetric wear
- XLPE reduces wear below this threshold in most patients
Postoperative Care
Surveillance and Monitoring for PE Wear:
Recommended intervals:
- 6 weeks: Wound check, early X-ray
- 3 months: Clinical assessment
- 1 year: Baseline X-ray for wear comparison
- Annually: Clinical review, X-rays every 1-2 years
- Long-term: Continue surveillance indefinitely
What to look for:
- Linear penetration (head into liner)
- Osteolytic lesions (lucencies around components)
- Component migration or loosening
- Cup position (abduction, anteversion)
Compare to immediate post-op baseline
- Wear Finding
- Bedding-in (creep), not true wear
- Osteolysis
- None expected
- Action
- Baseline established
- Wear Finding
- Minimal (less than 0.05mm/year)
- Osteolysis
- Rare (under 2%)
- Action
- Continue surveillance
- Wear Finding
- Still minimal, often unmeasurable
- Osteolysis
- Under 5%
- Action
- Continue surveillance
- Wear Finding
- Less than 1mm total linear wear
- Osteolysis
- Under 5%
- Action
- Excellent long-term performance
Bedding-in (creep) occurs in first 1-2 years as the femoral head settles into the liner under load. This is not true wear and should not be included in wear rate calculations. To calculate true wear rate, compare X-rays from 2 years post-op onwards. Linear wear with XLPE should be less than 0.05mm/year (often unmeasurable on plain X-rays).
Outcomes
Key outcome improvements with XLPE:
- Linear wear: 0.02-0.05 mm/year vs 0.1-0.2 mm/year (80-90% reduction)
- Osteolysis at 10+ years: Less than 5% vs 15-30%
- Revision for wear/osteolysis: Dramatically reduced
- 15-year survivorship: Over 95% for THA and TKA
AOANJRR 2023 Report:
- THA with XLPE: 95.4% at 15 years
- Conventional PE (historical): 89% at 15 years
- Revision for loosening/osteolysis: 1.2% (XLPE) vs 6.8% (conventional) at 15 years
- Young patients (under 55): Greatest benefit from XLPE
- Conventional PE
- 0.1-0.2
- XLPE (1st Gen)
- 0.02-0.05
- Vitamin E XLPE
- 0.01-0.03
- Conventional PE
- 50-100
- XLPE (1st Gen)
- 10-30
- Vitamin E XLPE
- 5-20
- Conventional PE
- 15-30%
- XLPE (1st Gen)
- 2-5%
- Vitamin E XLPE
- Under 2% (limited data)
- Conventional PE
- 8-12%
- XLPE (1st Gen)
- Under 2%
- Vitamin E XLPE
- Under 1%
- Conventional PE
- Rare
- XLPE (1st Gen)
- 1-2% (if thin)
- Vitamin E XLPE
- Under 1%
- Conventional PE
- 85-90%
- XLPE (1st Gen)
- 93-96%
- Vitamin E XLPE
- 95%+ (extrapolated)
Before XLPE, polyethylene wear was the Achilles heel of THA - the main cause of late revision. With XLPE achieving wear rates below the osteolysis threshold (less than 40-50 mm³/year), young active patients can now expect implant longevity approaching their lifetime. Registry data confirms over 95% 15-year survivorship with XLPE bearings.
Clinical Relevance and Applications
Bearing Surface Selection in Arthroplasty
XLPE is now standard of care for THA bearing surfaces:
- All primary THA: Standard choice for most patients
- Young active patients: Low wear critical for longevity
- Revision THA: Reducing future wear-related complications
- Large femoral heads: XLPE enables 36-40mm heads safely
- Small acetabular components: May not achieve minimum 6-8mm thickness
- Dual mobility constructs: Some use conventional PE (design-specific)
- Metal-on-metal alternative: XLPE replaced MoM for wear concerns
- Cost considerations: XLPE more expensive than conventional (justified by outcomes)
Clinical Decision-Making
Factors influencing PE selection:
-
Patient age and activity
- Young active: XLPE essential (high cumulative cycles)
- Elderly low demand: XLPE still preferred (same cost, better outcomes)
-
Acetabular component size
- Large enough for minimum 6-8mm liner: use XLPE with desired head size
- Small acetabulum: smaller head to maintain adequate thickness
-
Head size selection
- 32mm: Standard for smaller acetabula (50-54mm cups)
- 36mm: Preferred for larger acetabula (56mm+ cups) if adequate thickness
- 40mm: Selected cases (revision, high dislocation risk) with large cups
-
Revision considerations
- Always use XLPE in revision (reducing future wear)
- Head-liner exchange: Replace both even if head appears acceptable
Mechanical Properties and Clinical Considerations
Fracture Toughness Trade-off
XLPE mechanical properties vs conventional PE:
- Conventional PE
- Baseline
- XLPE (Remelted)
- 10x improvement
- Change
- Much better
- Conventional PE
- High (baseline)
- XLPE (Remelted)
- Reduced 20-30%
- Change
- Worse
- Conventional PE
- 40-50 MPa
- XLPE (Remelted)
- 35-45 MPa
- Change
- Slightly worse
- Conventional PE
- Baseline
- XLPE (Remelted)
- Reduced 30-40%
- Change
- Worse
Why toughness decreases:
- Crosslinks restrict chain mobility (chains cannot slide past each other to dissipate energy)
- Remelting reduces crystallinity (crystalline regions provide mechanical strength)
- Less ductility (cannot elongate as much before fracture)
Minimum Thickness Requirements
- Rim fracture risk: Edge loading concentrates stress at liner rim (thin liners crack)
- Fatigue failure: Cyclic loading causes subsurface crack propagation (thin liners fail faster)
- Oxidation: Higher surface area to volume ratio in thin liners (accelerated aging)
- Impact resistance: Thin liners more susceptible to impingement and fracture
- Minimum 6mm XLPE thickness (preferably 8mm)
- Use larger femoral heads (36-40mm) only if adequate liner thickness achieved
- 32mm head with 6-8mm liner is safer than 40mm head with 4mm liner
Guidelines, Registries & Global Practice
Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR):
- XLPE with ceramic head: 48% of primary THA (most common)
- XLPE with metal head: 38% of primary THA
- Ceramic-on-ceramic: 9% (declining)
- Metal-on-metal: Less than 0.5% (near-abandoned)
XLPE with ceramic femoral head has lowest revision rate of all bearing combinations in AOANJRR
- XLPE is standard of care for all primary THA
- Minimum liner thickness: 8mm recommended
- Head size: 32-36mm optimal (balance stability vs wear)
- Ceramic heads: Preferred in patients under 65
- Vitamin E XLPE: Increasingly used, registry tracking ongoing
- Target 15-year all-cause revision: Under 5%
- Wear-related revision: Under 2%
The AOANJRR is one of the world's largest and most comprehensive joint registries with over 1.5 million procedures recorded. It provides real-world outcome data that informs international practice alongside the UK NJR, the Nordic registries and the US AJRR. In any fellowship examination, quoting registry revision rates and hazard ratios demonstrates knowledge of evidence-based, globally applicable practice.
MCQ Practice Points
Q: What is the molecular weight range of ultra-high molecular weight polyethylene (UHMWPE)? A: 3-6 million Daltons - This is approximately 1000 times higher than standard polyethylene (20,000-40,000 Da). The high molecular weight provides strength, toughness, and wear resistance.
Q: What radiation dose is used to create highly crosslinked polyethylene (XLPE)? A: 50-100 kGy - This is 2-4 times higher than the 25-40 kGy dose used for conventional gamma sterilization. The high dose creates C-C crosslinks between polymer chains.
Q: By what percentage does highly crosslinked polyethylene reduce volumetric wear compared to conventional polyethylene? A: 90% - XLPE reduces linear wear to under 0.05mm/year vs 0.1-0.2mm/year for conventional PE. This reduces osteolysis rates from 15-30% to under 5% at 15 years.
Q: What is the minimum recommended thickness for XLPE liners in total hip arthroplasty? A: 6-8mm (preferably 8mm) - XLPE has reduced fracture toughness due to crosslinking and reduced crystallinity from remelting. Thinner liners are at risk for rim fracture with edge loading.
At a Glance
Ultra-high molecular weight polyethylene (UHMWPE) has a molecular weight of 3-6 million Daltons (1000× standard PE), providing the strength required for arthroplasty bearings. Highly crosslinked polyethylene (XLPE) is manufactured by high-dose radiation (50-100 kGy) creating C-C crosslinks between polymer chains, followed by thermal treatment to remove free radicals. Remelting (greater than 137°C) eliminates all free radicals but reduces crystallinity and toughness; annealing (less than 137°C) preserves crystallinity but leaves residual radicals susceptible to slow oxidation. XLPE achieves 90% wear reduction (linear wear less than 0.05mm/year vs 0.1-0.2mm/year conventional PE), but requires minimum 6-8mm thickness due to reduced fracture toughness. Vitamin E-stabilized PE provides antioxidant protection without as much toughness reduction.
RICHXLPE Manufacturing Steps
Hook:XLPE gets RICH: Radiation, Increased crosslinks, Cool/reheat, High wear resistance!
RACRemelting vs Annealing Trade-offs
Hook:RAC trade-off: Remelting eliminates radicals, Annealing preserves crystallinity, Crystallinity matters!
FROGFactors Requiring Minimum XLPE Thickness
Hook:XLPE thickness FROG rule: Fracture risk, Rim loading, Oxidation, Greater than 6mm minimum!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old active male is 5 years post THA with XLPE liner. He presents with sudden onset pain and instability. X-ray shows the cup is in 60 degrees abduction. What is your differential diagnosis and management?”
“A 45-year-old active male requires primary THA for hip dysplasia with secondary OA. He is concerned about implant longevity. How do you counsel him about bearing surface options?”
“An examiner asks you to justify your choice of bearing surface for a 55-year-old female undergoing primary THA. What evidence do you use?”
UHMWPE Structure
- Molecular weight: 3-6 million Da (1000x standard PE)
- Semicrystalline: 40-50% crystalline, 50-60% amorphous
- Linear chains of ethylene monomers (C2H4)
- Cannot melt process (too viscous, requires compression molding)
XLPE Manufacturing
- Radiation: 50-100 kGy gamma or e-beam (2-4x conventional sterilization)
- Crosslinking: C-C bonds between chains increase wear resistance
- Remelting (over 137C): eliminates radicals, reduces crystallinity (30-35%)
- Annealing (below 137C): preserves crystallinity (40-45%), leaves residual radicals
Wear Performance
- Conventional PE: 0.1-0.2mm/year linear wear (osteolysis risk)
- XLPE: under 0.05mm/year (90% reduction)
- Osteolysis: conventional 15-30%, XLPE under 5% at 15 years
- Critical particle size for osteolysis: 0.1-10 microns
Mechanical Trade-offs
- XLPE wear resistance: 10x better than conventional
- XLPE fracture toughness: 20-30% lower (crosslinks restrict mobility)
- XLPE impact strength: 30-40% lower (reduced crystallinity)
- Minimum thickness: 6-8mm (preferably 8mm) to prevent rim fracture
Clinical Applications
- XLPE is standard of care for THA bearing surfaces
- Enables larger femoral heads (36-40mm) without prohibitive wear
- Head size selection based on maintaining adequate liner thickness
- 32mm heads for smaller acetabula, 36-40mm for larger
Advanced Formulations
- Vitamin E stabilized: antioxidant prevents oxidation without remelting
- Better toughness than remelted XLPE (can use lower radiation or skip remelting)
- Diffusion method: soak in vitamin E (surface distribution)
- Blending method: mix vitamin E into powder (uniform distribution)
Evidence Base
Long-term Survivorship
XLPE vs UHMWPE: 7-Year Wear (Double-Blind RCT, RSA)
- Double-blind RCT: 54 patients randomised to highly cross-linked (Longevity) vs conventional UHMWPE liners, assessed by radiostereometric analysis (RSA)
- Steady-state wear rate: XLPE 0.005 mm/year vs conventional 0.037 mm/year at minimum 7 years (p = 0.007)
- Total femoral head penetration: 0.33 mm (XLPE) vs 0.55 mm (UHMWPE) at 7 years (p = 0.005)
- No XLPE patient exceeded the 0.1 mm/year osteolysis threshold, compared with 9% of the UHMWPE group
First-Generation XLPE: Systematic Review of Wear and Osteolysis
- Systematic review: 28 studies (1503 hips) for XLPE penetration vs 18 studies (695 hips) for conventional UHMWPE
- Weighted mean 2D linear penetration: 0.042 mm/year (XLPE) vs 0.137 mm/year (conventional UHMWPE)
- Pooled odds ratio for osteolysis (XLPE vs conventional) was 0.13 (95% CI 0.06 to 0.27) at minimum 5-year follow-up, an 87% lower risk
- Wear or osteolysis reduction not established for large (greater than 32mm) metallic heads or ceramic heads of any size; few data in TKA
Vitamin E-Diffused XLPE at 5 Years (RCT, RSA)
- Blinded RCT: vitamin E-diffused XLPE (E1, 32 patients) vs medium cross-linked control (ArComXL, 35 patients), assessed by radiostereometric analysis
- Five-year median proximal head penetration: -0.05 mm (E1) vs 0.07 mm (ArComXL); penetration significantly greater in the control at 3 and 5 years (p = 0.019 at 5 years)
- Patient-reported outcomes improved significantly and remained favourable at 5 years, with no difference between groups
- Longest-term RCT comparing vitamin E-diffused XLPE with a prior-generation crosslinked control
Registry Evidence on Revision Risk
Conventional PE vs HXLPE: Revision Risk in a US Registry
- Kaiser Permanente registry cohort: 26,823 primary THAs (1815 metal-on-conventional PE, 25,008 metal-on-HXLPE), 2001 to 2011
- Seven-year cumulative revision: 5.4% (conventional PE) vs 2.8% (HXLPE)
- Adjusted all-cause revision hazard ratio 1.75 (95% CI 1.37 to 2.24) and aseptic revision HR 1.91 (95% CI 1.46 to 2.50) for conventional PE vs HXLPE (both p less than 0.001)
- Findings consistent within manufacturer designs sharing the same femoral and acetabular components
AOANJRR: Crosslinked PE and Lower Revision Rates
- Australian Orthopaedic Association National Joint Replacement Registry, 1999 to 2018, capturing greater than 98% of national arthroplasties
- Surgeons with the lowest revision rates (THA 10-year CPR 2.7% vs 5.9%; TKA 2.6% vs 6.4%) differed mainly in modifiable implant and technical factors
- Low-revision-rate TKA surgeons were more likely to use highly crosslinked polyethylene, patellar resurfacing and AOANJRR best-performing prosthesis combinations
- Patient factors were broadly similar between groups, highlighting implant selection as a modifiable driver
Material Property Trade-off
Crosslinking and the Wear-Fracture Trade-off
- High-dose irradiation used to crosslink UHMWPE markedly improves wear resistance
- Crosslinking simultaneously reduces ductility and resistance to fatigue crack propagation
- Highly crosslinked UHMWPE may be more susceptible than conventional UHMWPE to fracture under severe loading such as impingement or edge loading
- Hip and knee simulators screen wear well, but standardised methods to screen fracture resistance are lacking
Large Femoral Heads with XLPE
XLPE enables use of larger femoral heads (36-40mm) without prohibitive wear.
- Lower dislocation: Higher head-to-neck ratio, greater jump distance
- Greater ROM: Reduced impingement, better function
- Improved stability: Especially in revision or high-risk patients
- Patient satisfaction: Better subjective outcomes
- Conventional PE: Large heads prohibitive (volumetric wear proportional to head size)
- XLPE: Wear so low that large head penalty is acceptable
- Prerequisite: Adequate liner thickness (minimum 6mm, ideally 8mm+)
- Clinical practice: 36mm standard, 40mm for revision or high dislocation risk