Reverse Bankart | McLaughlin | Capsulorrhaphy | Bone Loss
- 2-5% of dislocations but frequently MISSED
- FAIR position of risk (flexion, adduction, internal rotation)
- Reverse Bankart = posterior labral tear
- McLaughlin lesion = reverse Hill-Sachs on anterior humeral head
- Posterior bone loss rare but important
- “Jerk test and Kim test specific for posterior labral lesions
- “Lightbulb sign on AP X-ray = locked posterior dislocation
- “Seizure patients have high rate of bilateral posterior dislocations
- “Avoid surgery for voluntary dislocators
Posterior dislocations frequently missed (up to 60% initially). Always get axillary or scapular Y view. Suspect with seizure/electrocution.
Flexion, Adduction, Internal Rotation is position of risk. Mechanism is posterior force with arm in this position.
Posterior labral tear = reverse Bankart. Key pathology for surgical stabilization. Analogous to anterior Bankart.
Reverse Hill-Sachs = impaction fracture anterior humeral head. McLaughlin procedure transfers subscapularis into defect.
- Posterior
- 2-5%
- Anterior
- 95%+
- Posterior
- FAIR (flex, add, IR)
- Anterior
- ABER (abd, ext rot)
- Posterior
- Reverse Bankart (posterior)
- Anterior
- Bankart (anterior)
- Posterior
- McLaughlin (anterior)
- Anterior
- Hill-Sachs (posterior)
- Posterior
- Posterior glenoid (reverse bony Bankart)
- Anterior
- Anterior glenoid
FAIRPosition of Risk
Hook:FAIR position is NOT fair to posterior shoulder!
JKPosterior Instability Tests
Hook:JK tests for posterior labral tears!
Overview and Epidemiology
Posterior dislocations missed in up to 60% of initial presentations. Always suspect with seizure, electrocution, or failure to externally rotate. Get axillary view.
- 2-5% of shoulder dislocations
- Higher in epileptic patients
- Overhead athletes (backhanders, linemen)
- Males greater than females
- Often bilateral with seizure
- Seizure/electrocution: Massive muscle contraction
- Trauma: Posterior force in FAIR position
- Sports: Repetitive microtrauma (overhead)
- Voluntary: Psychological component
- Internal rotators overpower external (seizure)
Pathophysiology and Mechanisms

Posterior Stabilizers
Posterior glenoid rim provides bony stability.
Posterior fibrocartilaginous rim deepens socket.
Posterior capsule and posterior band IGHL.
Infraspinatus, teres minor (external rotators).
The posterior capsule is thinner than anterior - less robust stabilization.
Locked posterior dislocation = humeral head trapped behind glenoid with McLaughlin engaging posteriorly. Requires specific reduction technique or open reduction.
SEEPPosterior Dislocation Causes
Hook:SEEP causes arm to SEEP backward!
The Posterior Capsulolabral Lesion Spectrum
Not every posterior instability is a reverse Bankart. Recognising the full spectrum matters because the site of the lesion dictates where the repair must be placed - a glenoid-sided labral repair will fail if the true lesion is on the humeral side.
- What it is
- Avulsion of the posterior labrum from the glenoid
- Why it matters
- Commonest lesion; glenoid-sided suture-anchor repair
- What it is
- Incomplete, concealed avulsion of the deep posteroinferior labrum beneath an intact superficial labrum
- Why it matters
- Looks normal at arthroscopy - must be probed, converted to a complete tear and repaired
- What it is
- Posterior labral avulsion with a glenoid rim fracture / bone loss
- Why it matters
- Bone loss must be quantified; large defects need a bone block
- What it is
- Posterior labrocapsular periosteal sleeve avulsion - labrum and capsuloperiosteum stripped as an intact sleeve (the posterior analogue of an ALPSA)
- Why it matters
- A medialised, malunited sleeve must be mobilised and re-tensioned to the rim
- What it is
- Humeral-sided avulsion of the posterior band of the IGHL from the humeral neck
- Why it matters
- A glenoid-sided labral repair will NOT address it - it needs humeral-sided repair; a classic cause of 'failed' stabilisation
If posterior instability recurs after an apparently sound labral repair, think of a missed reverse HAGL (humeral-sided posterior capsular avulsion) or a concealed Kim lesion. The reverse HAGL is repaired on the humeral side, not the glenoid - look for capsular extravasation / a J-sign of the posterior capsule on MR arthrogram.
Classification Systems
Posterior Instability Types
- Mechanism
- Seizure, electrocution
- Features
- Often locked, bilateral
- Treatment Approach
- Closed reduction if possible
- Mechanism
- Previous dislocation
- Features
- Apprehension, recurrence
- Treatment Approach
- Surgical stabilization
- Mechanism
- Microtrauma, laxity
- Features
- Athletes, overhead sports
- Treatment Approach
- Rehab first, surgery if fails
- Mechanism
- Patient induced
- Features
- Psychological aspect
- Treatment Approach
- Avoid surgery
Clinical Assessment
- Mechanism: Seizure, electrocution, FAIR trauma
- Pain: Posterior shoulder
- Restricted motion: Cannot externally rotate
- Recurrence: Prior events
- Voluntary: Patient can demonstrate
- Position: Arm held in IR, adducted
- ROM: Blocked external rotation (key finding)
- Jerk test: Positive for posterior labral tear
- Kim test: Posterior subluxation
- Posterior apprehension: FAIR position loading
Patient supine. Arm at 90 degrees flexion and internal rotation. Examiner applies axial load and adducts across body. Positive: Posterior subluxation followed by clunk as it reduces when arm is returned to neutral.
Key Clinical Pearls
Inability to externally rotate should raise suspicion for locked posterior dislocation.
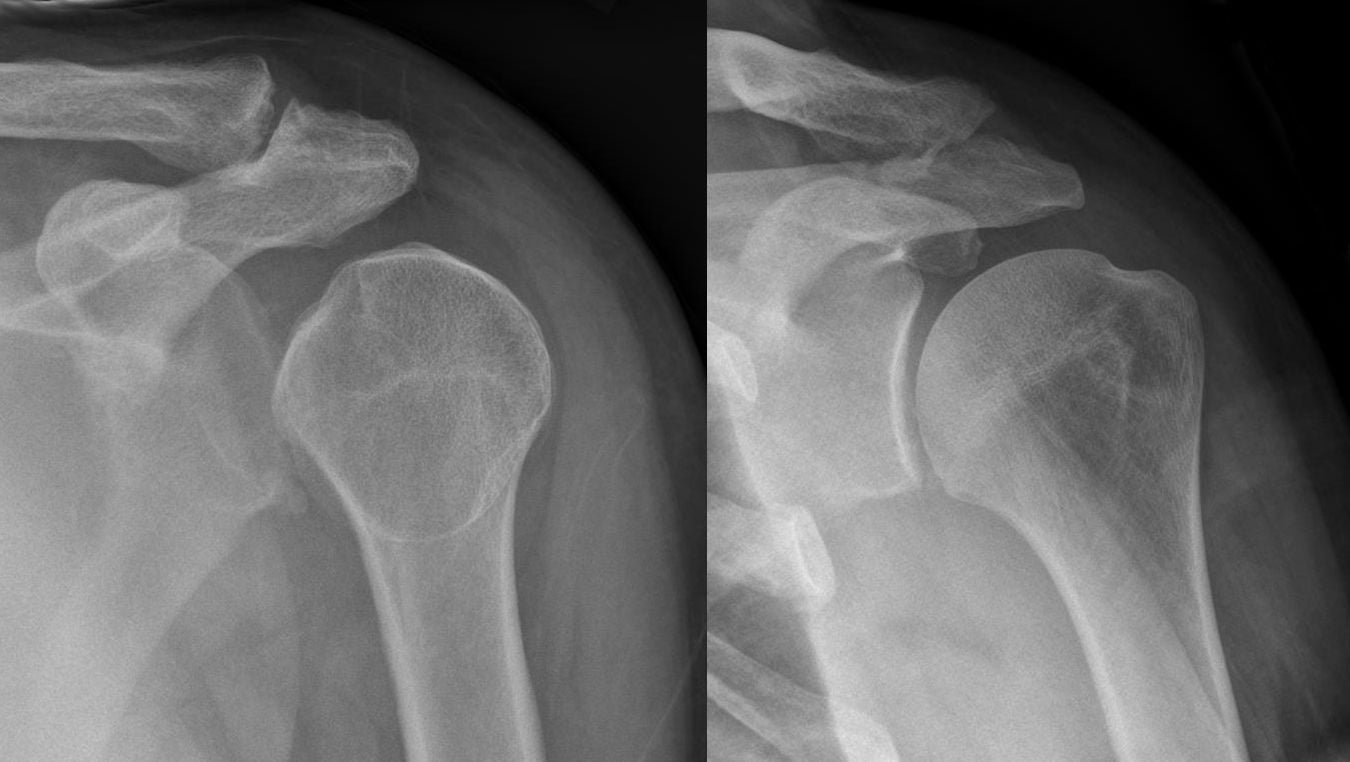
On AP view, humeral head appears like a lightbulb (internally rotated appearance) - suggests locked posterior dislocation.
Differential Diagnosis
- Key discriminator
- Pain/apprehension in FAIR; positive jerk and Kim tests
- Best test
- MR arthrogram + dynamic exam
- Key discriminator
- Apprehension in ABER (abduction-external rotation)
- Best test
- Anterior apprehension/relocation
- Key discriminator
- Global laxity, sulcus sign, often bilateral, atraumatic
- Best test
- Sulcus sign, generalised laxity (Beighton)
- Key discriminator
- Fixed internal rotation, blocked external rotation
- Best test
- Axillary radiograph (humeral head behind glenoid)
- Key discriminator
- Pain on overhead throwing, positive O'Brien
- Best test
- MR arthrogram, dynamic labral tests
- Key discriminator
- Weakness, scapular winging, no true subluxation
- Best test
- Scapular assistance test, cuff strength
Investigations
X-ray Assessment
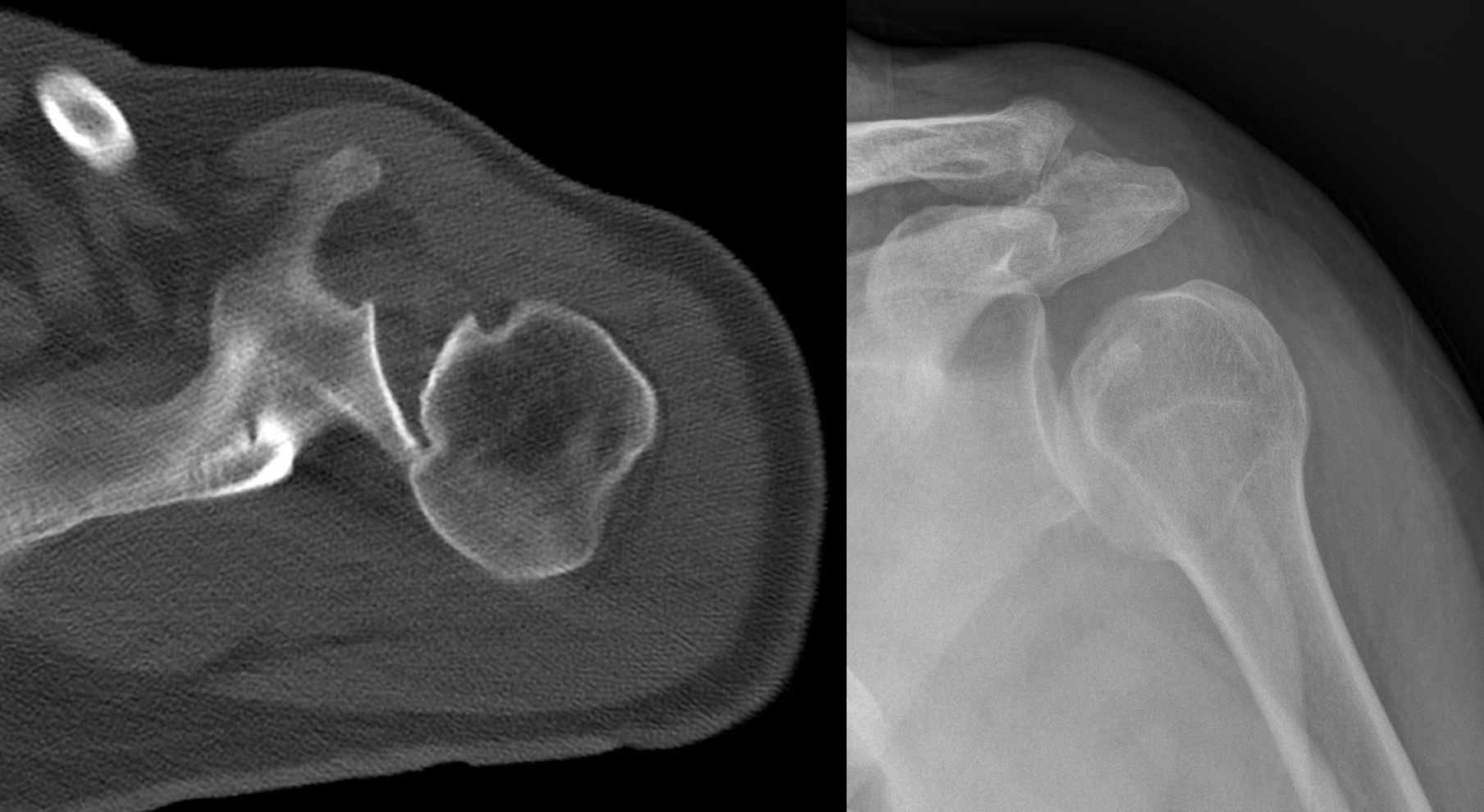
AP, axillary (essential), scapular Y.
Humeral head internally rotated on AP view.
Increased space between humeral head and glenoid.
Overlap of head and glenoid (Y view).
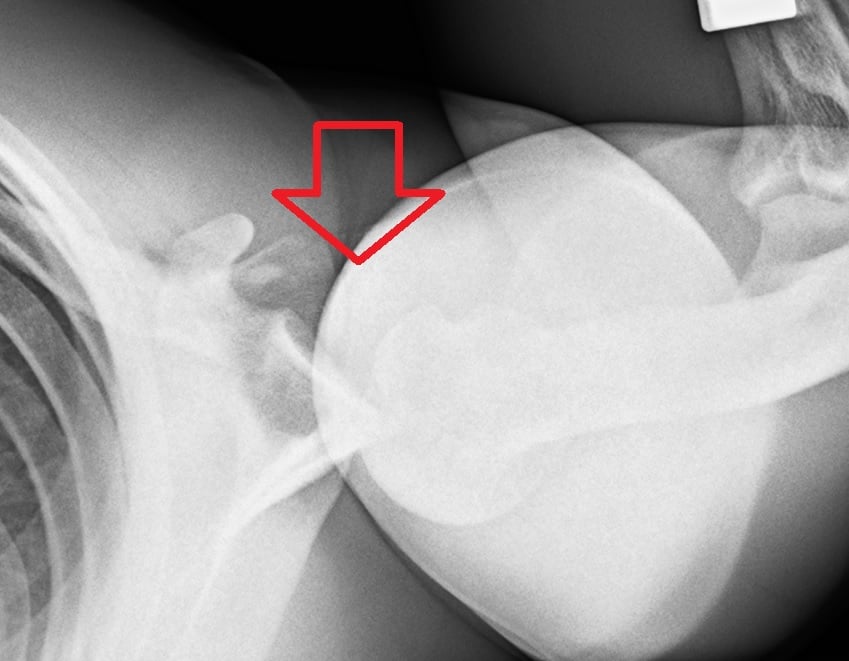
Axillary view is essential and diagnostic - posterior position of head.
Lightbulb sign = internally rotated humerus on AP view looks like a lightbulb. Indicates locked posterior dislocation due to inability to externally rotate. DO NOT MISS.

Management Algorithm
Acute Posterior Dislocation
Acute Management
High suspicion with seizure/electrocution. Get axillary view. Check for locked dislocation.
CT to assess humeral head defect size. Less than 20% good prognosis.
Traction, gentle external rotation. If less than 6 weeks old, may succeed.
Brace in neutral or external rotation. Avoid internal rotation.
Surgical Technique
Posterior Labral Repair (Arthroscopic)
Beach chair or lateral decubitus.
Standard posterior (viewing), anterior, and posterolateral (working).
- Mobilize labrum from glenoid
- Prepare glenoid rim bleeding bone bed
- Place suture anchors (2-4) on glenoid face
- Shuttle sutures through labrum
- Tie knots to reduce labrum to glenoid
Consider capsular plication for laxity.
Avoid overtightening posterior capsule which leads to loss of internal rotation and anterior subluxation. Balance is important.
Glenoid Version, Dysplasia and Posterior Glenoid Osteotomy
Posterior bone loss (a reverse bony Bankart) is addressed by a bone block, but a separate structural problem is excessive glenoid retroversion or posteroinferior dysplasia / hypoplasia, which biomechanically directs the head posteriorly and is a recognised cause of soft-tissue repair failure.
- Glenoid version is measured on an axial CT, commonly by the Friedman method (a line from the medial scapular border to the glenoid centre as the reference axis).
- The normal glenoid is slightly retroverted (around 2 to 7 degrees); pathological retroversion is generally taken as more than about 10 degrees.
- Posteroinferior glenoid dysplasia - a deficient, rounded or hypoplastic ("lazy-J") posteroinferior glenoid - is a developmental contributor identified on CT/MRI.
- Reserved for instability driven by excessive retroversion (often quoted as more than about 10 to 15 degrees) where soft-tissue work alone is likely to fail.
- It is technically demanding with a historically high complication rate - graft-site fracture, avascular necrosis, intra-articular penetration, and over-correction producing anterior subluxation - so it is used selectively and in specialist centres.
Distinguish posterior glenoid bone loss (reverse bony Bankart → bone block) from excessive retroversion / dysplasia (→ consider a posterior opening-wedge glenoid osteotomy). Measure version on axial CT (Friedman); normal is roughly 2 to 7 degrees of retroversion, and pathological retroversion (more than about 10 degrees) both causes instability and predicts failure of an isolated labral repair.
Complications
- Cause
- Missed pathology, undertightening
- Prevention
- Address all lesions
- Management
- Revision surgery
- Cause
- Overtightening, immobilization
- Prevention
- Balanced repair
- Management
- Physical therapy
- Cause
- Overtightening posterior
- Prevention
- Avoid overtightening
- Management
- Rare, may need revision
- Cause
- Portal placement
- Prevention
- Safe portal placement
- Management
- Observation usually
Recurrence after posterior stabilization: 5-15% in experienced hands. Worse with voluntary instability (avoid surgery), bone loss, and unrecognized pathology.
Postoperative Care
Posterior Stabilization Rehabilitation
Sling in neutral rotation (not internal rotation). Pendulums, elbow and wrist ROM.
Progressive ROM. Avoid combined flexion, adduction, internal rotation. Start external rotation.
Progressive strengthening. Rotator cuff and scapular stabilizers. Pool exercises.
Sport-specific training. Full return at 6-9 months if strength and stability adequate.
Avoid FAIR position (flexion, adduction, internal rotation) during early rehabilitation - this stresses the posterior repair. Progress to full ROM gradually.
Outcomes and Prognosis
Prognosis by Type
Good outcomes with surgery. 85-90% stability.
May respond to physiotherapy. Surgery if fails.
Poor surgical outcomes. Avoid surgery. Psychological counseling.
Worse prognosis. May need arthroplasty if engaging.
Controversies and Areas of Uncertainty
- Bone-loss threshold: the exact posterior glenoid loss at which soft-tissue repair fails (often quoted 20-25%) is not well defined and remains debated.
- Open vs arthroscopic bone block: posterior bone-block techniques are less standardised than the anterior Latarjet, with no high-level comparative data.
- Optimal immobilisation: neutral vs external-rotation bracing after reduction or repair lacks robust evidence.
- Classification: the Stanmore polar (structural / muscular-patterning / atraumatic) framework increasingly guides whether to operate, replacing rigid traumatic vs voluntary dichotomy.
- Throwing athletes: consistently return to pre-injury level less often, so counselling and graded return-to-throw protocols are emphasised.
- Thermal capsulorrhaphy: abandoned due to chondrolysis and capsular necrosis - mentioned only to be rejected in vivas.
Guidelines, Registries & Global Practice
- Posterior instability is around 2-5% of all glenohumeral instability
- Acute locked posterior fracture-dislocation incidence around 0.6 per 100,000 per year (Robinson, Edinburgh population)
- Peak in middle-aged men (seizure, electrocution, high-energy trauma)
- A second peak in young overhead/collision athletes (atraumatic, repetitive microtrauma)
- Up to 50-79% of acute posterior dislocations are missed at first presentation
- No single dedicated international guideline exists - practice is consensus and registry-informed
- AAOS / ASES (US), BESS-BOA (UK), AO Foundation, and EFORT/SECEC (Europe) converge on the same principles
- Axillary or modified axial radiograph is mandatory in every suspected dislocation
- Atraumatic instability: structured physiotherapy first; surgery only after a failed dedicated rehab trial
- Voluntary/positional (muscular-pattern) instability: non-operative, with psychological input where relevant
- AAOS / ASES (US)
- Axillary lateral mandatory; CT for bone loss
- BESS-BOA (UK)
- Trauma series + axial/Velpeau view; CT if locked
- AO Foundation / EFORT (Europe)
- AO: axial view essential; CT to template head defect
- AAOS / ASES (US)
- Supervised rehab, scapular/cuff control
- BESS-BOA (UK)
- Physiotherapy-led muscle-patterning programme first
- AO Foundation / EFORT (Europe)
- Conservative rehab; surgery reserved for structural lesions
- AAOS / ASES (US)
- Arthroscopic capsulolabral repair with anchors
- BESS-BOA (UK)
- Arthroscopic labral repair / capsular plication
- AO Foundation / EFORT (Europe)
- Arthroscopic repair; posterior bone block (autograft) for bone loss
- AAOS / ASES (US)
- Subscap or lesser-tuberosity transfer (20-40%)
- BESS-BOA (UK)
- Modified McLaughlin; arthroplasty if greater than 40-50%
- AO Foundation / EFORT (Europe)
- AO: ORIF + grafting acutely; transfer/arthroplasty if neglected
- AAOS / ASES (US)
- Avoid surgery; psychological assessment
- BESS-BOA (UK)
- Non-operative; biofeedback rehab (Stanmore type 3)
- AO Foundation / EFORT (Europe)
- Conservative; surgery only if proven structural lesion
- Registry data for posterior instability are limited compared with arthroplasty (no large dedicated instability registry). Most evidence is single-centre cohorts and the DeLong/Bradley meta-analysis. National arthroplasty registries (NJR, AJRR, AOANJRR) capture only the small subset progressing to reverse shoulder arthroplasty for chronic locked fracture-dislocation.
- High-resource settings: MR arthrography and CT bone-loss templating are routine; arthroscopic suture-anchor repair is the default.
- Limited-resource settings: diagnosis rests on a careful axillary/Velpeau radiograph and clinical exam; open posterior repair, open McLaughlin/lesser-tuberosity transfer, and ORIF remain valid where arthroscopy or advanced imaging is unavailable. The priority everywhere is recognising the missed dislocation early.
Posterior shoulder instability is high-yield because it is commonly missed. Know the FAIR position of risk, the lightbulb sign and mandatory axillary view, why voluntary/muscular-pattern dislocators should not have surgery, and the size-based treatment of the reverse Hill-Sachs (McLaughlin) lesion. Examiners worldwide expect the same principles regardless of country.
MCQ Practice Points
Q: What position causes posterior shoulder instability? A: FAIR - Flexion, Adduction, Internal Rotation. This is opposite to ABER for anterior instability.
Q: Most common cause of acute posterior dislocation? A: Seizure (grand mal). Also electrocution. Internal rotators overpower external rotators during convulsion.
Q: What is the lightbulb sign? A: Internally rotated humeral head on AP X-ray with locked posterior dislocation. Looks like a lightbulb.
Q: What is a McLaughlin lesion? A: Reverse Hill-Sachs. Impaction fracture of anteromedial humeral head. May engage on posterior glenoid.
Q: What X-ray view is diagnostic for posterior dislocation? A: Axillary view. Shows posterior position of humeral head relative to glenoid. AP can miss 60%.
Q: Should you operate on voluntary dislocators? A: NO. Poor surgical outcomes, high recurrence. Physiotherapy and psychological assessment indicated.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old epileptic presents after a grand mal seizure with bilateral shoulder pain. He cannot externally rotate either shoulder. AP X-rays appear normal. How would you manage this?”
“A 25-year-old tennis player has recurrent posterior shoulder subluxation episodes during serving. He has failed 6 months of physiotherapy. MRI shows a posterior labral tear. What would you recommend?”
“A 20-year-old can voluntarily dislocate her shoulders by positioning them. She has some pain and asks for surgical stabilization to stop the dislocations. What is your approach?”
Key Differences from Anterior
- 2-5% vs 95% of dislocations
- FAIR position (flex, add, IR) vs ABER
- Reverse Bankart (posterior labrum)
- McLaughlin lesion (anterior head)
Causes (SEEP)
- Seizure (most common)
- Electrocution
- Ethanol (withdrawal seizures)
- Posterior trauma
Imaging
- Lightbulb sign on AP = locked posterior
- Axillary view is DIAGNOSTIC
- CT for McLaughlin size
- MRI for labral tear
Key Clinical Tests
- Jerk test: axial load and adduction
- Kim test: posterior force with elevation
- Blocked external rotation = locked
- Posterior apprehension in FAIR
McLaughlin Lesion Treatment
- Less than 20%: conservative/soft tissue
- 20-40%: McLaughlin procedure
- Greater than 40%: allograft or arthroplasty
- Fill the engaging defect
Critical Pearls
- Often missed - 60% initially
- Always get axillary view
- Avoid surgery for voluntary
- Immobilize in neutral (not IR)
Evidence Base and Key Studies
Arthroscopic Posterior Capsulolabral Reconstruction (100 shoulders)
- 91 athletes (100 shoulders) with unidirectional recurrent posterior instability, mean 27-month follow-up
- Mean ASES score improved from 50.4 to 85.7 (p less than 0.001)
- 89% returned to sport; 67% returned at the same level
- Posterior-instability shoulders had significantly greater chondrolabral and osseous retroversion than controls
Arthroscopic Posterior Capsulolabral Reconstruction (200 shoulders)
- 183 athletes (200 shoulders), mean 36-month follow-up - the largest single-series cohort
- Mean ASES score improved from 45.9 to 85.1 (p less than 0.001)
- 90% returned to sport; suture-anchor plication gave significantly higher ASES and return-to-play rates than anchorless repair
- Contact athletes did as well as the overall cohort