Adult acquired flatfoot - Stage II reconstruction, Stage III-IV arthrodesis
- Most common cause of adult acquired flatfoot deformity
- Too many toes sign and failed single heel raise test are key clinical findings
- Stage II flexible - reconstruct: MDCO + FDL transfer ± lateral column lengthening
- Stage III rigid - fuse: triple arthrodesis or tibiotalocalcaneal fusion
- Weight-bearing radiographs essential for talonavicular coverage assessment
- “Single heel raise test: patient cannot invert heel on affected side
- “Too many toes sign: see more than 2 lateral toes from behind
- “Assess flexibility with heel in valgus - correctable = Stage II, fixed = Stage III
- “Stage IV adds deltoid failure with ankle valgus
Posterior Tibial Tendon Dysfunction (PTTD)
Never Complain, My Feet Constantly CrampPTT Insertion Sites
Hook:Think of the PTT as a broad fan insertion supporting the entire medial and plantar arch - NOT just the navicular
FIDO HAS PAINPTTD Risk Factors
Hook:Think of the typical patient: Female In her 50s with Diabetes, Obesity, Hypertension - these systemic factors predispose to tendon degeneration
Overview and Epidemiology
Definition
Posterior tibial tendon dysfunction (PTTD) represents a progressive degenerative condition of the posterior tibial tendon resulting in medial longitudinal arch collapse and hindfoot valgus deformity. It is the most common cause of adult acquired flatfoot deformity.
Epidemiology
- Peak incidence: 5th-6th decade of life
- Gender: Female predominance (3-10:1 ratio)
- Prevalence: 3.3% in women over 40 years
- Bilateral involvement: 10-20% of cases (usually asymmetric presentation)
- Obesity: BMI over 30 (strongest modifiable risk factor)
- Hypertension: Associated with tendon degeneration
- Diabetes mellitus: Impaired tendon healing and neuropathy
- Inflammatory arthropathy: Rheumatoid arthritis, seronegative arthropathy (psoriatic, reactive)
- Corticosteroid exposure: Intra-tendinous injection (CONTRAINDICATED), systemic steroids
- Fluoroquinolone antibiotics: Associated with tendinopathy
- Pre-existing pes planus: Constitutional flatfoot with hypermobility
- Hindfoot valgus alignment: Increased eccentric loading on PTT
- First ray hypermobility: Loss of medial column stability
- Gastrocnemius contracture: Hindfoot equinus increases pronation moment
Without treatment, PTTD typically progresses:
- Stage I → II: 6-18 months (tendinitis to flexible deformity)
- Stage II → III: Years (flexible to rigid peritalar arthritis)
- Stage III → IV: Variable (rigid flatfoot to ankle valgus)
Early intervention with orthotics in Stage I can prevent progression in 70-80% of cases. Once Stage II deformity develops, progression to Stage III is common without surgical reconstruction.
Pathophysiology and Anatomy
Pathophysiology
The posterior tibial tendon undergoes degenerative changes rather than inflammatory tendinitis. The pathophysiological cascade involves:
-
Zone of hypovascularity: 2-6cm proximal to navicular insertion represents a watershed zone between:
- Musculotendinous blood supply (proximally)
- Osseous blood supply from navicular (distally)
-
Repetitive microtrauma: Eccentric loading during stance phase causes:
- Tendon fiber microtears
- Myxoid degeneration
- Collagen disorganization
- Loss of type I collagen (replaced by type III)
-
Tendon elongation: Mechanical failure under physiological loads leads to:
- Loss of dynamic arch support
- Inability to control hindfoot eversion
- Progression from tendinosis to partial/complete rupture
- Spring ligament attenuation: As PTT fails, increased load on spring ligament causes:
- Superomedial band elongation
- Plantar bands attenuation/rupture
- Loss of static support to talar head
- Talar head plantarflexion and medial displacement
-
Hindfoot valgus: Calcaneal eversion from:
- Loss of PTT inverter function
- Unopposed peroneal eversion force
- Achilles tendon lateral vector (valgus thrust)
-
Peritalar subluxation: Progressive malalignment causes:
- Talonavicular joint uncovering (forefoot abduction)
- Subtalar joint subluxation (hindfoot valgus)
- Calcaneocuboid joint impingement
-
Forefoot supination: Compensatory forefoot varus develops:
- Relative to hindfoot valgus
- First ray plantarflexion
- Lateral column overload
-
Rigid peritalar arthritis: Chronic malalignment leads to:
- Subtalar joint arthritis
- Talonavicular joint arthritis
- Calcaneocuboid joint arthritis
- Transition from flexible (Stage II) to rigid (Stage III)
-
Deltoid ligament insufficiency: Late-stage ankle involvement:
- Medial ankle instability
- Ankle valgus tilt (talar tilt in mortise)
- Lateral tibiotalar impingement
- Stage IV disease
- Loss of windlass mechanism: Plantar fascia cannot tighten arch with dorsiflexion
- Decreased Achilles mechanical advantage: Calcaneal eversion shortens moment arm
- Lateral column overload: Calcaneocuboid joint bears increased load (sinus tarsi pain)
- Forefoot pressures: Increased lateral forefoot pressures, risk of ulceration in diabetics
Tendon degeneration in hypovascular zone (NOT inflammatory tendinitis) with myxoid change and collagen disorganization leading to mechanical failure under eccentric load
Spring ligament attenuation allows talar head plantarflexion and medial displacement, creating valgus hindfoot and peritalar subluxation with uncovering
Rigid peritalar arthritis develops from chronic malalignment, eventually progressing to deltoid insufficiency and ankle valgus in Stage IV disease
Surgical Anatomy
-
Origin:
- Posterior tibia (interosseous border)
- Interosseous membrane
- Proximal fibula (small contribution)
-
Course:
- Posterior compartment of leg
- Behind medial malleolus (beneath flexor retinaculum)
- Curves beneath sustentaculum tali
- Fans out to multiple insertions
-
Primary insertion: Navicular tuberosity (plantar-medial surface)
-
Secondary insertions (broad fan attachment):
- All three cuneiforms (medial, intermediate, lateral)
- Metatarsal bases 2-4
- Cuboid (occasional slips)
- Spring ligament fibrocartilage (functional support)
-
Blood supply:
- Musculotendinous junction: Posterior tibial artery branches
- Distal tendon: Navicular osseous vessels
- Watershed zone: 2-6cm proximal to insertion (critical zone for degeneration)
-
Function:
- Primary: Hindfoot inversion, adduction
- Secondary: Ankle plantarflexion, medial arch support
- Dynamic arch stabilizer: Controls pronation during stance phase
-
Components (three bands):
- Superomedial band (strongest): Sustentaculum tali to navicular
- Medioplantar oblique band: Middle calcaneus to navicular
- Inferior plantar longitudinal band: Plantar calcaneus to navicular
-
Function:
- Primary static support to talar head
- Prevents talar plantarflexion and medial displacement
- Fibrocartilaginous articulation with talar head
-
Pathology in PTTD:
- Attenuates secondarily after PTT failure
- Superomedial band most commonly affected
- Requires reconstruction if Grade 3-4 tear (Bluman classification)
- Plantar fascia: Windlass mechanism, arch support
- Long plantar ligament: Lateral column stabilization
- Interosseous talocalcaneal ligament: Subtalar stability
- Deltoid ligament: Medial ankle stability (fails in Stage IV)
- Tibialis posterior: Primary arch stabilizer
- Flexor digitorum longus: Transfer donor, secondary arch support
- Flexor hallucis longus: Secondary arch support
- Tibialis anterior: Counterbalances tibialis posterior
- Peroneus longus: Plantarflexes first ray, lateral column support
- Gastrocnemius-soleus: Achilles loads hindfoot (equinus increases valgus)
Zones of PTT Pathology (surgical planning):
- Zone 1: Myotendinous junction to medial malleolus (rare pathology)
- Zone 2: Behind medial malleolus (tenosynovitis, stenosing tenosynovitis)
- Zone 3: Inframalleolar to navicular insertion (most common zone of degeneration)
- Zone 4: Insertion to navicular (insertional tendinopathy, avulsion)
Classification Systems
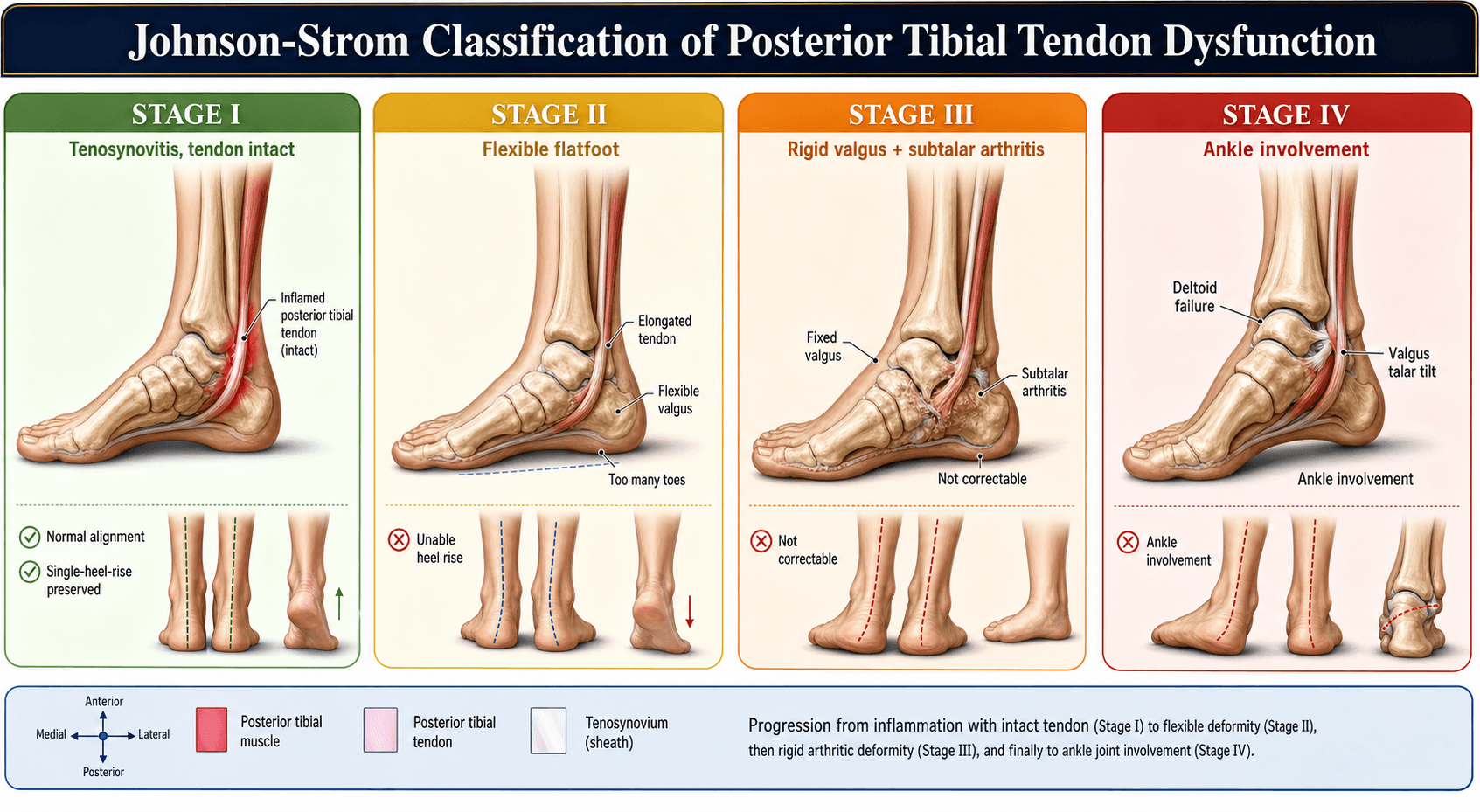
Johnson & Strom Classification (Modified by Myerson)
The Johnson & Strom classification, modified by Myerson to include Stage IV, is the gold standard for staging PTTD. Staging determines treatment: conservative vs reconstruction vs arthrodesis.
Stage I: Tendinitis Without Deformity
- Tendon inflammation/degeneration
- Intact tendon function
- No architectural deformity
- Pain: Medial ankle pain along PTT course
- Swelling: Tenosynovitis, fusiform swelling posterior to medial malleolus
- Function: Can perform single heel raise with heel inversion
- Deformity: None - normal arch height maintained
- Weight-bearing radiographs: Normal arch parameters
- MRI: Increased T2 signal within tendon, peritendinous edema, thickening
- Conservative management: 70-80% success rate
- CAM walker boot immobilization 4-6 weeks
- Transition to UCBL orthotic
- Physiotherapy for strengthening
- Surgical (if failed conservative): Tendon debridement ± synovectomy
- Good response to conservative management
- Risk of progression to Stage II if biomechanical factors not addressed
Early intervention at this stage prevents progression to more advanced disease.
Stage IIA vs IIB: Critical Distinction
Critical examination skill: Passively correct hindfoot valgus by inverting heel while palpating talonavicular joint. If deformity fully corrects → Stage II (flexible). If peritalar joints are rigid → Stage III. This determines reconstruction vs arthrodesis.
Examiner question: "How do you differentiate Stage II from Stage III?"
Answer: "Passive hindfoot inversion with stress - if the valgus and arch collapse correct, it's flexible Stage II suitable for reconstruction. If rigid, it's Stage III requiring arthrodesis."
Bluman Classification (Spring Ligament Pathology)
Used to grade spring ligament pathology on MRI or intraoperative assessment:
- Grade 1: Attenuation only (elongation without rupture)
- Grade 2: Partial-thickness tear
- Grade 3: Full-thickness rupture
- Grade 4: Complete disruption with talar head uncovering
Surgical relevance: Grade 3-4 requires spring ligament reconstruction with allograft augmentation or direct repair.
Clinical Presentation and Examination
History
- Location: Medial ankle/hindfoot (along PTT course from medial malleolus to navicular)
- Character: Aching, exacerbated by activity
- Progression: Insidious onset over months to years
- Exacerbating factors: Prolonged standing, walking on uneven ground, stairs
- Medial ankle swelling: Worse with activity, improves with rest
- Tenosynovitis: Fusiform swelling posterior to medial malleolus
- Progressive flatfoot: Gradual arch collapse
- Shoe wear changes: Medial heel breakdown, difficulty fitting shoes
- Gait abnormality: Antalgic gait, foot external rotation
- Difficulty with stairs (especially descent)
- Problems on uneven ground
- Unable to run or perform sports
- Prolonged standing painful
- Acute onset: Rare (suggests rupture after steroid injection)
- Insidious onset: Typical (months to years)
- Progression:
- Stage I symptoms: 6-18 months before deformity
- Stage II: Years before rigidity
- Stage III-IV: Variable progression
- Systemic: Obesity, hypertension, diabetes, inflammatory arthropathy
- Medications: Corticosteroids (injection or systemic), fluoroquinolones
- Biomechanical: Pre-existing flatfoot, hypermobility
- Occupational: Prolonged standing, repetitive impact activities
Physical Examination
Observation (Standing):
"Too Many Toes Sign" (pathognomonic):
- Technique: Stand behind patient, observe feet
- Normal: See heel and 1-1.5 lateral toes
- PTTD: See heel and over 2 lateral toes (forefoot abduction)
- Severity: More toes visible = greater forefoot abduction
- Normal: 5-7 degrees valgus
- PTTD: Over 10 degrees valgus (compare to contralateral)
- Asymmetry: Side-to-side comparison critical
- Loss of medial longitudinal arch: Talar head prominence medially
- Medial ankle bulge: Displaced talus palpable
- Lateral column: Relative shortening
- Forefoot varus: Relative forefoot supination (compensatory to hindfoot valgus)
- First ray: Plantarflexion, callosity under first metatarsal head
- Antalgic gait: Shortened stance phase on affected side
- Foot progression angle: Excessive external rotation
- Heel strike: Valgus thrust with loading
- Tenderness: Along PTT from behind medial malleolus to navicular insertion
- Swelling: Tenosynovitis (fusiform vs nodular thickening)
- Gap: Palpable defect suggests rupture (rare)
- Navicular tuberosity: Prominence with spring ligament failure
- Talar head: Medial and plantar prominence
- Sustentaculum tali: Tenderness
- Sinus tarsi: Lateral hindfoot impingement pain (calcaneocuboid)
Single Heel Raise Test (GOLD STANDARD)
- Patient stands on one leg (affected side)
- Patient raises heel off ground
- Observe hindfoot from behind
- Heel inverts as patient rises onto forefoot
- Arch reconstitutes
- Can perform 10+ repetitions
- Stage I: Can perform but painful, normal inversion
- Stage II-IV: CANNOT perform OR performs without heel inversion
- Bilateral testing: Compare to contralateral side
- Sensitivity: 100% for Stage II or greater
- Specificity: 85% (other flatfoot causes may also fail test)
Passive Correction Test (Stage II vs III Differentiation)
- Patient sitting or supine
- Examiner inverts heel manually
- Palpate talonavicular joint while inverting
- Assess if arch reconstitutes
- Stage II (flexible): Deformity fully corrects, talonavicular reduces
- Stage III (rigid): Deformity persists, peritalar joints rigid, crepitus
Coleman Block Test (Forefoot vs Hindfoot Driven)
- Stand patient on 1-inch block under lateral foot (5th metatarsal hangs off)
- Observe hindfoot alignment
- Forefoot-driven: Hindfoot valgus corrects (flexible forefoot varus)
- Hindfoot-driven: Hindfoot valgus persists (PTTD pattern)
- Inversion/eversion: Compare to contralateral
- Stage II: Flexible but deformed
- Stage III: Rigid, crepitus
- Flexible: Corrects with hindfoot neutral positioning
- Fixed: Persistent forefoot varus (rare in PTTD)
- Hypermobile: Dorsiflexion/plantarflexion over 10mm
- Contributes to: Medial column instability
Neurovascular Examination
- Dorsalis pedis pulse: Palpate, document
- Posterior tibial pulse: Palpate, document
- Ankle-brachial index: If PVD suspected (diabetics, smokers)
- Sensation: Light touch, 2-point discrimination (exclude neuropathy)
- Motor: Tibialis posterior (inversion strength), peroneals, ankle dorsiflexors
- Reflexes: Achilles reflex
- Tinel's sign: Tap posterior tibial nerve behind medial malleolus
- Positive: Paresthesias in plantar foot (coexisting in 10% PTTD)
- Sensory: Medial and lateral plantar nerve distributions
Patient stands on one leg and raises heel off ground. Normal: Heel inverts with raise, arch reconstitutes. PTTD Stage II-IV: Cannot perform OR performs without inversion. Most sensitive clinical test.
Examiner inverts heel while palpating talonavicular joint. Flexible (Stage II): Full correction of valgus and arch. Rigid (Stage III): No correction - peritalar arthritis present. Determines reconstruction vs fusion.
Differential Diagnosis
- Rheumatoid arthritis, psoriatic arthritis
- Features: Polyarticular involvement, systemic symptoms, synovitis
- Differentiation: Inflammatory markers, rheumatoid factor, anti-CCP
- Features: Rigid flatfoot since adolescence, limited subtalar motion
- Differentiation: C-sign on lateral radiograph, CT confirms coalition
- Features: Diabetic neuropathy, midfoot collapse, rocker-bottom deformity
- Differentiation: Loss of protective sensation, midfoot warmth/swelling, fragmentation on radiograph
- Features: Traumatic onset, midfoot swelling, abduction stress pain
- Differentiation: History of trauma, midfoot tenderness, radiographic diastasis
- Features: Acute medial arch pain, palpable defect, previous plantar fasciitis
- Differentiation: History of sudden pain (often during sports), bruising
- Features: Burning paresthesias, positive Tinel's, night symptoms
- Differentiation: Nerve conduction studies, predominantly sensory symptoms
- Features: Acute trauma, lateral ankle ecchymosis (eversion mechanism)
- Differentiation: History of trauma, ankle stress radiographs
- Features: Prominence since childhood, os naviculare on radiograph
- Differentiation: Longstanding symptoms, characteristic radiographic appearance
Differential Diagnosis of Adult Acquired Flatfoot / Medial Hindfoot Pain
Investigations and Imaging
Radiography
Weight-bearing radiographs are MANDATORY for PTTD assessment. Non-weight-bearing films grossly underestimate deformity severity. Examiners will fail candidates who order non-weight-bearing foot films for PTTD staging.
Standard Views (ALL weight-bearing):
AP Foot
Talonavicular coverage angle (most important):
- Technique: Angle between midline of talus and midline of navicular
- Normal: Less than 7 degrees
- Stage IIA: 7-20 degrees (mild-moderate forefoot abduction)
- Stage IIB: Over 20 degrees (severe forefoot abduction requiring LCL)
- Clinical significance: Determines need for lateral column lengthening
- Technique: Angle between long axis of talus and 1st metatarsal
- Normal: 0-4 degrees (aligned)
- PTTD: Over 15 degrees (forefoot abduction)
- Technique: Percentage of talar head uncovered laterally
- Normal: Less than 10%
- Stage IIA: 10-30%
- Stage IIB: Over 30% (significant uncovering)
- Metatarsal divergence: Increased intermetatarsal angles
- First-second intermetatarsal angle: May be increased
Lateral Foot
- Technique: Angle between long axis of talus and 1st metatarsal on lateral view
- Normal: 0-4 degrees (colinear)
- PTTD: Over 15 degrees (sagittal plane sag)
- Severe: Over 30 degrees
- Technique: Angle between plantar calcaneus and horizontal plane
- Normal: 18-25 degrees
- PTTD: Under 15 degrees (arch collapse)
- Severe: Under 10 degrees
- Normal: Parallel dorsal cortices
- PTTD: Talar plantarflexion, navicular dorsal subluxation
- Normal: Smooth S-curve (calcaneocuboid + talonavicular joint line)
- PTTD: Disrupted, stepped (peritalar subluxation)
Hindfoot Alignment View (Saltzman View)
- Patient stands on blocks with feet 15cm apart
- Ankle centered on cassette
- X-ray beam parallel to floor (horizontal)
- Shows coronal hindfoot alignment
- Tibial-calcaneal angle: Angle between tibial axis and calcaneal axis
- Normal: 0-5 degrees valgus
- PTTD: Over 10 degrees valgus (significant deformity)
- Quantify hindfoot valgus severity
- Preoperative planning for MDCO
- Monitor post-reconstruction correction
Ankle AP and Mortise (Stage IV Assessment)
- Medial clear space: Over 2mm greater than lateral = deltoid insufficiency
- Talar tilt angle: Over 5 degrees (ankle valgus)
- Tibiotalar joint space narrowing
- Lateral gutter impingement
- Subchondral sclerosis/cysts
Talonavicular coverage angle (most important): Normal under 7°, Stage IIA 7-20°, Stage IIB over 20°. Measures forefoot abduction - determines need for lateral column lengthening.
Calcaneal pitch: Normal 18-25°, PTTD under 15°. Measures arch height. Meary's angle: Normal 0-4°, PTTD over 15°. Measures sagittal plane collapse and talar sag.
Saltzman view: Measures tibial-calcaneal angle. Normal 0-5° valgus. PTTD over 10° valgus. Critical for pre-operative planning to quantify hindfoot valgus severity and monitor correction.
Advanced Imaging
MRI
- Confirm PTT pathology and grade severity
- Assess spring ligament integrity
- Exclude occult pathology (coalition, tumor, osteochondral lesion)
- Preoperative planning for Stage I debridement
- Assess FDL for transfer quality
- T1-weighted: Tendon morphology, muscle bulk
- T2-weighted/STIR: Tendon signal, peritendinous edema
- Proton density: Detailed tendon microstructure
- Increased T2 signal within tendon (tendinosis)
- Tendon thickening (over 6mm)
- Peritendinous fluid (tenosynovitis)
- Normal tendon continuity
- Tendon elongation (attenuation)
- Partial-thickness tear (focal signal)
- Complete tear (tendon discontinuity)
- Spring ligament abnormality (increased signal, thickening)
- Tendon rupture or severe attenuation
- Spring ligament disruption
- Peritalar joint effusions
- Cartilage loss
- Bone marrow edema
- Grade 1: Attenuation - thickening, increased T2 signal, intact
- Grade 2: Partial tear - focal defect, less than 50% thickness
- Grade 3: Full-thickness rupture - complete discontinuity
- Grade 4: Complete disruption - talar head uncovering
CT Scan
- Rigid deformity (Stage III) - assess peritalar arthritis
- Preoperative planning for triple arthrodesis
- Exclude tarsal coalition (confirm bony vs fibrous)
- Post-fusion assessment (union evaluation)
- Axial, coronal, sagittal reconstructions
- Bone windows
- 3D reconstructions for complex deformity
- Stage III: Subtalar, talonavicular, calcaneocuboid arthritis
- Joint space narrowing
- Subchondral sclerosis and cysts
- Osteophytes
- Peritalar subluxation
Ultrasound
- Dynamic assessment of tendon excursion
- Tenosynovitis confirmation
- Operator-dependent
- Less reliable than MRI
- Tendon thickening
- Peritendinous fluid
- Focal hypoechogenicity (partial tear)
Management Algorithm
Non-Operative Management
- Stage I: ALL patients initially (first-line treatment)
- Stage II-IV: Medical comorbidities precluding surgery, patient preference, non-ambulatory
- Contraindication to surgery: Severe peripheral vascular disease, uncontrolled diabetes, active infection
- Progressive deformity despite bracing (Stage II)
- Failed trial of appropriate conservative measures
- Patient desire for deformity correction (conservative does NOT correct)
Phase 1: Acute Immobilization (Stage I)
- Duration: 4-6 weeks strict immobilization
- Rationale: Reduce tendon inflammation, prevent microtrauma, allow healing
- Weight-bearing: Full weight-bearing in boot
- Mobilization: Gradual transition to orthotics over 2 weeks
- 70-80% of Stage I patients improve with immobilization
- Does NOT reverse deformity if present
- Prevents progression in compliant patients
Phase 2: Orthotic Management
- Rigid custom foot orthotic (molded from cast)
- High medial flange (supports arch)
- Lateral flange (controls forefoot abduction)
- Deep heel cup (controls hindfoot valgus)
- Stage I (after immobilization)
- Stage II non-surgical candidates
- Post-reconstruction (protective bracing)
- Gold standard for Stage I
- Better arch support than standard orthotics
- Requires shoe with removable insole
- Compliance issues (bulk, shoe limitations)
- Leather double-upright AFO
- Lateral upright controls hindfoot valgus
- Medial arch support integrated
- Ankle motion preserved
- Stage II non-surgical candidates (better control than UCBL)
- Stage III palliative management
- Post-triple arthrodesis (temporary)
- Better valgus control than UCBL
- Allows ankle motion (vs rigid AFO)
- Significant compliance issues (bulk, cosmesis, shoe limitations)
- Semi-rigid thermoplastic
- Medial posting
- Arch support
- Mild Stage I only
- Preventive in at-risk patients
- Less control than UCBL
- Insufficient for Stage II or greater
- Good compliance (fits regular shoes)
Shoe Modifications
- 4-6mm medial build-up
- Controls hindfoot valgus
- Shifts ground reaction force laterally
- Reduces forefoot stress
- Assists toe-off
- Reduces PTT eccentric load
- Accommodates forefoot abduction
- Prevents lateral toe compression
Key Points
- Conservative management controls pain and prevents progression
- Does NOT reverse established deformity
- Compliance critical for success
- Stage II deformity will progress despite bracing in most cases
Orthotic management remains the foundation of conservative PTTD treatment.
Success Rates of Conservative Management
- Success rate: 70-80% respond to immobilization + UCBL orthotic
- Definition of success: Pain reduction, functional improvement, no progression
- Duration of trial: 6 months minimum before considering surgical intervention
- Success rate: 30-40% achieve symptom control with Arizona AFO
- Limitation: Does NOT correct deformity, only controls symptoms
- Natural history: Most progress to Stage III despite bracing
- Role: Palliative only
- Limitation: Does not prevent progression
- Indication: Non-surgical candidates only
Complications and Management
Intraoperative Complications
Neurovascular injury:
Sural nerve injury (most common):
- Incidence: 5-10% in lateral approaches (MDCO, lateral column lengthening, triple arthrodesis)
- Prevention: Careful identification and protection throughout procedure
- Management:
- If identified: Primary repair if transection
- Postoperative neuropathic pain: Gabapentin, referral to pain specialist
- Incidence: 5% in medial approach (FDL transfer)
- Prevention: Retract anteriorly during dissection
- Management: Avoid ligation of saphenous vein if possible, nerve injury as above
- At risk: Medial approach, aggressive retraction
- Prevention: Gentle retraction, awareness of anatomy
- Management: Vascular repair if injury, nerve repair/reconstruction
- Incidence: 2-5%
- Cause: Aggressive osteotome use, osteoporotic bone
- Prevention: Oscillating saw for osteotomy, gentle technique
- Management:
- Intraoperative: Fixation with additional screws/plate
- Alter postoperative protocol: Longer non-weight-bearing
- At risk: Triple arthrodesis (aggressive preparation)
- Prevention: Careful joint preparation, avoid excessive subchondral bone removal
- Management: Fixation, bone graft, prolonged immobilization
Early Postoperative Complications (Under 6 Weeks)
- Incidence: 5-10% (higher in diabetics, smokers, obese patients)
- Risk factors: Diabetes, smoking, obesity, malnutrition, steroid use
- Prevention:
- Optimize comorbidities preoperatively
- Careful tissue handling
- Avoid excessive tension on closure
- Avoid hematoma (use drain if large dissection)
- Management:
- Minor: Local wound care, allow to heal by secondary intention
- Major: Debridement, delayed closure vs flap coverage
- Incidence: 2-5%
- Risk factors: Diabetes, immunosuppression, prolonged surgery, hematoma
- Presentation: Fever, wound erythema, purulent drainage
- Management:
- Early (under 3 weeks): Debridement, irrigation, retain hardware if stable
- Late (over 3 weeks): Debridement, consider hardware removal, IV antibiotics (6 weeks)
- Organisms: Staphylococcus aureus (most common), MRSA, Gram-negatives
- Incidence: 5%
- Prevention: Meticulous hemostasis, drain placement (remove 24-48 hours)
- Management:
- Small: Observation
- Large/expanding: Evacuation
- Prevention: Adequate padding, cast checks, education
- Management: Cast removal, wound care
- Rare: Under 1%
- Presentation: Severe pain out of proportion, pain with passive stretch
- Management: Emergency cast removal, assessment, fasciotomy if confirmed
Late Postoperative Complications (Over 6 Weeks)
Non-union
- Incidence: 2-5%
- Risk factors: Smoking, diabetes, inadequate fixation, infection
- Presentation: Persistent pain at osteotomy site, hardware failure
- Diagnosis: Radiographs (lucency, sclerosis, no bridging bone), CT scan
- Management:
- Symptomatic: Revision osteotomy, bone graft, rigid fixation
- Asymptomatic: Observation
- Incidence: 10-15% overall
- Talonavicular: 5% (lowest)
- Subtalar: 10%
- Calcaneocuboid: 15% (highest)
- Risk factors: Smoking, diabetes, obesity, inadequate fixation, malnutrition
- Presentation: Persistent pain, inability to weight-bear
- Diagnosis: Radiographs, CT scan (gold standard)
- Management:
- Revision fusion with bone graft (iliac crest autograft or BMP)
- Rigid fixation (plate and screws)
- Address risk factors (smoking cessation, diabetes control)
- Incidence: 5-10%
- Cause: Under-correction during surgery, inadequate MDCO medial displacement
- Prevention: Intraoperative fluoroscopy, assess alignment
- Management:
- Mild: Orthotics, observation
- Severe: Revision osteotomy
- Incidence: 2-5%
- Cause: Excessive MDCO medial displacement
- Presentation: Lateral foot overload, 5th metatarsal pain, inversion instability
- Management:
- Orthotics (lateral heel wedge)
- Revision osteotomy if severe
- Incidence: 10-15%
- Presentation: Palpable hardware, pain, skin irritation
- Management: Hardware removal after union (minimum 12 months post-surgery)
- Incidence: 5%
- Cause: Non-union, inadequate fixation, premature weight-bearing
- Management: Revision fixation with bone graft
- Incidence: 10-15% at 5 years
- Causes:
- Unrecognized Stage IIB (inadequate lateral column lengthening)
- Inadequate MDCO correction
- Spring ligament failure
- Progressive peritalar arthritis (Stage III)
- Presentation: Return of pain, deformity, functional limitation
- Management:
- Flexible recurrence: Revision reconstruction (repeat MDCO, add LCL if not done)
- Rigid arthritis: Triple arthrodesis
- Incidence: 5%
- Cause: Inadequate fixation, premature mobilization
- Presentation: Recurrent arch collapse
- Management: Revision transfer or progress to triple arthrodesis
Ankle arthritis (post-triple arthrodesis):
- Incidence: 20-30% at 10 years
- Cause: Altered biomechanics, increased ankle stress
- Presentation: Ankle pain, stiffness, reduced range of motion
- Management:
- Conservative: Orthotics, NSAIDs, activity modification
- Surgical: Ankle arthrodesis or ankle replacement (consider TTC fusion)
Midfoot arthritis (post-pantalar fusion):
- Incidence: 30-40% at 10 years
- Cause: Complete loss of ankle/hindfoot motion, stress on midfoot
- Presentation: Midfoot pain, TMT joint arthritis
- Management: Midfoot fusion, orthotics
Complex regional pain syndrome (CRPS):
- Incidence: 2-5%
- Presentation: Severe pain out of proportion, allodynia, skin changes (color, temperature), edema
- Management:
- Early recognition critical
- Physiotherapy (desensitization)
- Medications (gabapentin, pregabalin, ketamine)
- Nerve blocks (sympathetic blocks)
- Referral to pain specialist
Surgical Management
Indications for Surgery
- Failed conservative management over 6 months
- Persistent pain limiting activities of daily living
- MRI-confirmed tendinosis or partial tear
- Failed conservative management (3-6 months trial)
- Progressive deformity despite appropriate bracing
- Functional impairment affecting quality of life
- Patient desire for deformity correction
- Symptomatic rigid deformity
- Failed conservative management
- Functional limitation
- Progressive ankle valgus deformity
- Pain and dysfunction
- Patient fit for major surgery
Contraindications
- Active infection
- Severe peripheral vascular disease precluding healing
- Non-ambulatory patient (surgery provides no functional benefit)
- Uncontrolled diabetes: HbA1c over 8% (optimize to under 7.5%)
- Smoking: Advise cessation minimum 6 weeks, ideally 12 weeks
- Obesity: BMI over 40 (encourage weight loss, assess realistic goals)
- Peripheral neuropathy: Risk of Charcot arthropathy post-surgery
- Poor bone quality: Osteoporosis (assess with DEXA if indicated)
- Inflammatory arthropathy: Active synovitis (optimize medical management)
Preoperative Optimization
- Target HbA1c under 7.5% (preferably under 7%)
- Defer elective surgery if over 8%
- Involve endocrinology/diabetes team
- Minimum 6 weeks preoperatively
- Ideally 12 weeks
- Counseling, nicotine replacement therapy
- Document compliance
- BMI reduction improves outcomes
- Realistic goal: 5-10% body weight reduction
- Dietitian referral
- Bariatric surgery consideration if BMI over 40
- Indications: Diabetes, smoking, peripheral vascular disease symptoms
- Ankle-brachial index: Abnormal if under 0.9
- Referral to vascular surgery: If ABI under 0.7 or claudication
- Indications: Major surgery (triple arthrodesis, pantalar fusion)
- Functional capacity: Assess exercise tolerance
- Cardiology referral: If poor functional capacity or cardiac history
Critical principle: PTTD surgery is stage-dependent. Stage I = tendon debridement, Stage II = reconstruction, Stage III-IV = arthrodesis. Examiners will immediately fail candidates who offer Stage II reconstruction procedures (FDL transfer, MDCO) for rigid Stage III deformity.
Stage I: PTT Debridement ± Synovectomy
- Stage I PTTD with MRI-confirmed tendinosis
- Failed 6 months conservative management
- No architectural deformity present
- Tendon structurally intact (under 50% cross-sectional involvement)
- Deformity present (Stage II) - reconstruction required
- Over 50% tendon cross-sectional involvement - augment with FDL transfer
Surgical Technique
- Supine
- Bump under ipsilateral hip (15-20 degrees internal rotation)
- Thigh tourniquet
- Longitudinal incision centered 1cm posterior to medial malleolus
- Extends from 4cm proximal to medial malleolus to navicular insertion
- Length: 8-10cm
- Identify and protect saphenous vein and nerve (retract anteriorly)
- Incise flexor retinaculum longitudinally (preserves pulley function for later repair)
- Expose PTT from myotendinous junction to navicular insertion
- Inspect entire tendon course for pathology
- Zone of degeneration: Typically Zone 3 (2-6cm proximal to navicular)
- Extent: Measure percentage of cross-sectional involvement
- Decision point: If over 50%, augment with FDL transfer (see Stage II tab)
- Longitudinal tenotomy along degenerated segment
- Excise all degenerate tissue:
- Macroscopically abnormal (yellow-brown discoloration)
- Friable, myxoid consistency
- Loss of normal tendon striations
- Preserve healthy tendon margins
- Assess remaining tendon: Should have intact, healthy tendon maintaining structural integrity
- Excise all inflamed synovium
- Inspect entire tendon course for additional pathology
- Repair flexor retinaculum: Maintains tendon pulley function
- Subcutaneous layer: Absorbable sutures
- Skin: Monofilament non-absorbable or absorbable subcuticular
- Backslab: Below-knee plaster backslab
Postoperative Protocol
- Non-weight-bearing cast: 4 weeks
- Weight-bearing cast: 2 weeks
- Total immobilization: 6 weeks
- CAM walker boot: 2 weeks with progressive weight-bearing
- Transition to UCBL orthotic: Week 8
- Physiotherapy: Range of motion, strengthening
- Light activities: 3 months
- Full return to sports: 4-6 months
- Orthotic use: Long-term
Outcomes
Success rate: 70-80% good-excellent results at 2-5 years
- No deformity pre-operatively
- Under 50% tendon involvement
- Appropriate patient selection
- Underlying biomechanical factors not addressed (flatfoot, hypermobility)
- Progression to Stage II deformity
- Inadequate post-operative orthotic use
- Wound healing problems: 5%
- Sural nerve injury: 2%
- Saphenous nerve injury: 5%
- Progression to Stage II: 20-30% over 5 years
Clinical note: Isolated debridement is rarely performed as most patients have progressed to Stage II by presentation.
MEDIALStage II PTTD Surgical Reconstruction
Hook:MEDIAL approach to PTTD Stage II reconstruction - systematic checklist for complete correction
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old woman with BMI 32 presents with progressive right medial ankle pain and flatfoot deformity over 2 years. Failed 6 months conservative management with UCBL orthotic. On examination: too many toes sign positive, failed single heel raise test, flexible deformity corrects with passive heel inversion. Weight-bearing AP foot radiograph shows 35% talonavicular uncovering, lateral radiograph shows calcaneal pitch 12 degrees, Meary's angle 22 degrees.”
“You are asked to assess a 62-year-old man with chronic flatfoot and medial ankle pain. On examination you notice hindfoot valgus, arch collapse, and he cannot perform single heel raise. The examiner asks you to demonstrate how you would differentiate Stage II from Stage III PTTD.”
“A 55-year-old woman had FDL transfer and MDCO 18 months ago for Stage II PTTD. She initially did well but now at 18 months complains of recurrent medial ankle pain, arch collapse, and difficulty walking. On examination the arch has collapsed again, too many toes sign is positive, and passive correction test shows some flexibility but less than expected.”
“A 52-year-old woman was diagnosed with PTTD Stage I by her GP 6 weeks ago. She was given a corticosteroid injection for 'tendinitis' behind the medial malleolus. She now presents to your clinic with sudden onset severe medial ankle pain 4 days ago while walking, now unable to weight-bear, severe flatfoot deformity, cannot perform heel raise. On examination: marked hindfoot valgus, arch completely collapsed, swelling medial ankle, tender along PTT course.”
Must-Know Classifications
- Johnson & Strom (Myerson Modification): Stage I (tendinitis, no deformity), Stage II (flexible flatfoot), Stage III (rigid flatfoot), Stage IV (ankle valgus)
- Stage IIA (hindfoot valgus, under 30% uncovering) vs IIB (over 30% uncovering requiring LCL)
- Bluman spring ligament: Grade 1 (attenuation), Grade 2 (partial tear), Grade 3 (full rupture), Grade 4 (complete disruption)
- PTT zones: Zone 1 (myotendinous), Zone 2 (behind malleolus), Zone 3 (inframalleolar - most common), Zone 4 (insertion)
Clinical Examination Pearls
- Too many toes sign: See over 2 lateral toes from behind (forefoot abduction)
- Single heel raise test: Cannot perform OR performs without heel inversion (gold standard for Stage II+)
- Passive correction test: Invert heel while palpating talonavicular - corrects = Stage II, rigid = Stage III
- Coleman block test: Stand on 1-inch block under lateral foot - hindfoot corrects if forefoot-driven varus
Radiographic Measurements (Weight-Bearing Mandatory)
- Talonavicular coverage angle (AP): Normal under 7°, IIA 7-20°, IIB over 20° (determines need for LCL)
- Calcaneal pitch (lateral): Normal 18-25°, PTTD under 15° (arch collapse)
- Meary's angle (lateral): Normal 0-4°, PTTD over 15° (sagittal sag)
- Saltzman view (hindfoot alignment): Normal 0-5° valgus, PTTD over 10° valgus
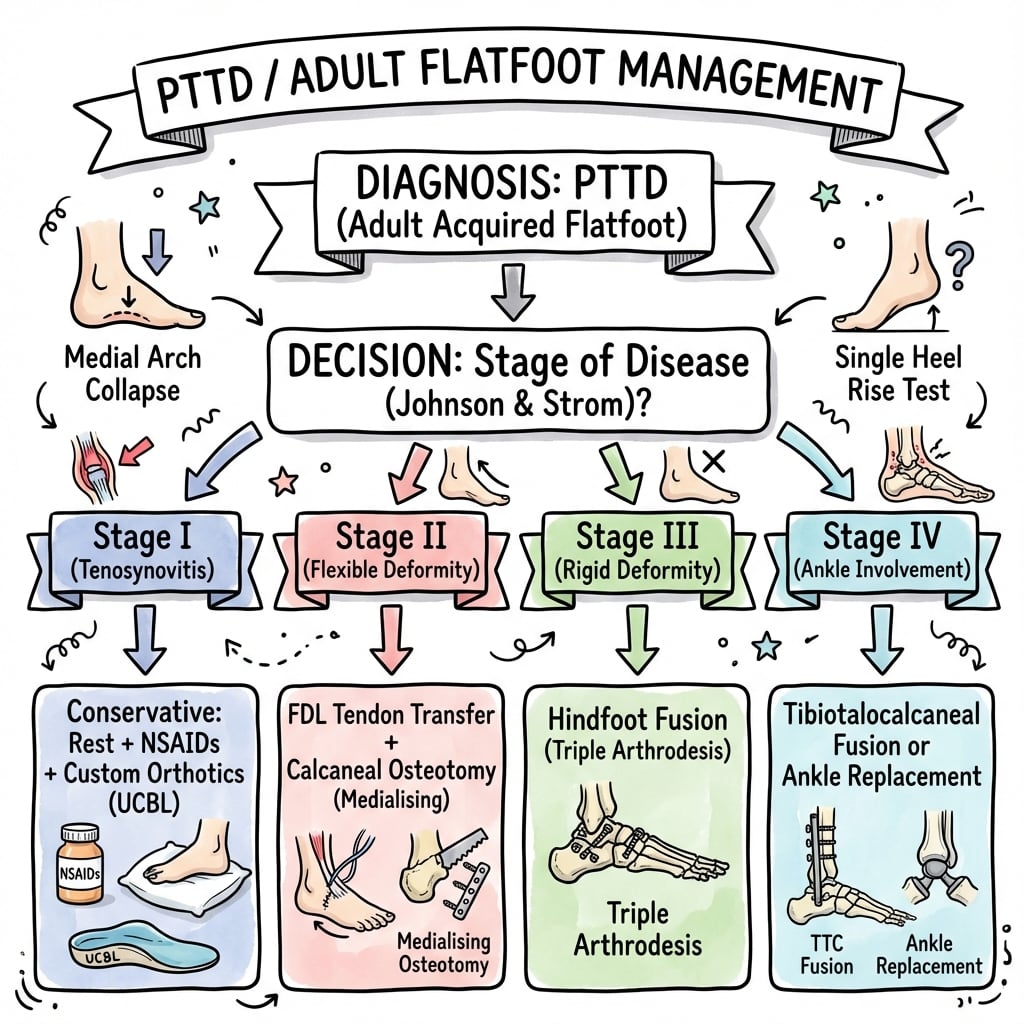
Stage-Appropriate Treatment (Critical)
- Stage I: Conservative first-line (CAM boot 4-6 weeks → UCBL orthotic). Surgery if failed 6 months: PTT debridement
- Stage IIA: FDL transfer + MDCO (medial procedures alone)
- Stage IIB: FDL transfer + MDCO + Lateral column lengthening (Evans or Cotton) - LCL essential if over 30% uncovering
- Stage III: Triple arthrodesis (subtalar + talonavicular + calcaneocuboid fusion). Reconstruction will FAIL
- Stage IV: Pantalar fusion or tibiotalocalcaneal fusion with IM nail
Surgical Techniques - Stage II Reconstruction
- FDL transfer: Harvest at master knot of Henry, Pulvertaft weave into PTT, set tension in neutral foot position
- MDCO: Oblique osteotomy 1-1.5cm posterior to calcaneocuboid joint, medialize 10-15mm, fix with 2x 6.5mm screws
- Evans osteotomy (LCL): Transverse cut 1-1.5cm posterior to calcaneocuboid, distract 8-12mm, tricortical iliac crest graft
- Spring ligament: Grade 3-4 requires allograft augmentation or direct repair
Contraindications and Cautions
- Corticosteroid injection ABSOLUTELY CONTRAINDICATED - causes tendon rupture (examiners will fail you if you recommend this)
- Weight-bearing radiographs MANDATORY - non-weight-bearing grossly underestimates deformity
- Do NOT offer Stage II reconstruction (FDL, MDCO) for Stage III rigid deformity - will fail due to arthritis
- Pre-op optimization critical: HbA1c under 7.5%, smoking cessation 12 weeks, BMI reduction
Complications and Success Rates
- Stage I conservative: 70-80% success. Stage II conservative: 30-40% symptom control only, does NOT reverse deformity
- Stage IIA reconstruction: 85-90% good outcomes at 5 years
- Stage IIB reconstruction: 80-85% good outcomes (lower due to lateral column pain, non-union risk)
- Triple arthrodesis: 75-85% good outcomes, non-union 10-15% (calcaneocuboid highest), adjacent joint arthritis 20-30% at 10 years
- Sural nerve injury: 5-10% in lateral approaches (MDCO, LCL, triple)
Viva Survival - Common Questions
- How differentiate Stage II from Stage III? Passive correction test - flexible = II (reconstruct), rigid = III (fuse)
- Why is LCL needed for Stage IIB? Forefoot abduction over 30% cannot be corrected by medial procedures alone - will recur without LCL
- What if Stage II reconstruction fails? Assess flexibility and imaging - flexible = revise reconstruction, rigid = triple arthrodesis
- Why no steroids? Degenerative not inflammatory, steroids cause collagen degradation and rupture risk, no evidence of benefit
Evidence Base and Literature
Landmark Studies and Systematic Reviews
Structured Non-Operative Protocol for Stage I-II PTTD
- 47 consecutive patients with Stage I or II PTTD treated with an articulated AFO/foot orthosis plus a high-repetition strengthening and gastrocsoleus stretching programme
- After a median of 10 physiotherapy visits over a median of 4 months, 39/47 (83%) had successful subjective and functional outcomes
- 42/47 (89%) were satisfied with the outcome
- Only 5/47 (11%) required surgery after failure of non-operative treatment
- Significant pre-treatment concentric and eccentric weakness across all ankle muscle groups (p less than 0.001)
FDL Transfer + Medial Displacement Calcaneal Osteotomy for Stage II
- 51 patients with classical Johnson & Strom Stage II PTTD treated with MDCO plus FDL transfer; 44 reviewed at a mean follow-up of 51 months
- Mean AOFAS ankle/hindfoot score improved from 48.8 pre-operatively to 88.5 at follow-up
- 43/44 rated good-to-excellent for pain and function; 36/44 good-to-excellent for alignment
- The procedure failed in only 2 patients, who subsequently underwent calcaneocuboid fusion
- Joint-sparing reconstruction gave durable medium-term results without sacrificing hindfoot motion
Lateral Column Lengthening (Evans vs Hintermann) for Flexible Flatfoot
- 53 patients with flexible flatfoot deformity: 17 Evans and 36 Hintermann lateral lengthening calcaneal osteotomies
- Both groups showed significant improvement in FAOS, pain (NRS) and SF-36 scores (p less than 0.05)
- Significant radiographic correction of talus-second metatarsal angle, talonavicular coverage and naviculocuneiform overlap (p less than 0.05)
- Calcaneocuboid degenerative change occurred in 41% after Evans vs 25% after Hintermann osteotomy; subtalar change 18% vs 14% - clinically silent in both
- No secondary arthrodesis required; no significant difference in clinical outcome between techniques
Triple Arthrodesis for the Rigid Arthritic (Stage III) Flatfoot
- Dual-incision triple arthrodesis remains the traditional, reliable and reproducible treatment for the rigid, arthritic adult flatfoot
- Early complications include lateral wound problems, malunion and non-union
- Long-term adjacent-joint (ankle and midfoot) arthritis is an expected consequence rather than a failure of the procedure
- A single medial incision reduces lateral wound complications but limits calcaneocuboid fixation and precludes lateral column lengthening
- Double or modified-double arthrodesis can spare minimally degenerate subtalar or calcaneocuboid joints in selected patients
Anatomical Spring Ligament Reconstruction (Biomechanical Basis)
- Simulated 5-15 degrees talonavicular abduction flatfoot deformity in 10 cadaver foot-ankle specimens under 357 N vertical load
- Three peroneus longus tendon reconstructions of the failed spring ligament were compared
- A superomedial/plantar passage through the calcaneus and navicular best corrected the deformity (talonavicular joint from 9.1 degrees abducted to 1.0 degree adducted)
- Subtalar joint corrected from 3.1 degrees everted to 0.4 degrees inverted with the same construct
- Provides the biomechanical rationale for adding anatomical spring ligament reconstruction to soft-tissue flatfoot correction
Johnson & Strom Staging Classification (Defining Landmark)
- Described the original three-stage classification of tibialis posterior tendon dysfunction (later modified by Myerson to add Stage IV ankle valgus)
- Each stage has characteristic pain symptoms, clinical signs and radiographic changes
- Staging clarifies expected pathology and directs surgical treatment
- Stage I: tenosynovitis, no deformity; Stage II: flexible flatfoot; Stage III: fixed deformity
- Emphasised the role of the tibialis posterior tendon in normal hindfoot function
PTTD as the Commonest, Frequently Overlooked Cause of Adult Flatfoot
- PTTD is the most common cause of adult acquired flatfoot, arising from degenerative change in the posterior tibial tendon
- Untreated disease progresses to fixed deformity and degenerative change in surrounding joints
- Key clinical signs are the 'too many toes' sign and inability to perform a single heel raise
- X-ray, ultrasound and MRI help stage disease and guide management
- Early identification and prompt treatment can halt progression
Guidelines, Registries and Global Practice
Global Epidemiology
PTTD is the most common cause of adult acquired flatfoot deformity (AAFD), driven by degenerative (not inflammatory) change in the tendon and progressing to fixed deformity if untreated (Bubra et al. 2015, J Family Med Prim Care; DOI). It predominantly affects women in the fifth-to-sixth decades, with obesity, hypertension and diabetes as the principal systemic associations. There is no national joint-replacement-style registry for flatfoot reconstruction; surgical-volume and outcome data derive from institutional series and the foot-and-ankle literature rather than population registries. Prevalence is anticipated to rise internationally as populations age and rates of overweight/obesity and diabetes increase.
Terminology Shift (Important for Modern Practice)
In 2020 an international expert consensus (Myerson, Deland and colleagues) recommended retiring the terms "PTTD" and "AAFD" in favour of "progressive collapsing foot deformity (PCFD)", replacing the linear Johnson & Strom/Myerson stages with a flexible/rigid classification across multiple deformity classes (A-E: hindfoot valgus, midfoot/forefoot abduction, forefoot varus, peritalar subluxation/dislocation, ankle valgus). The traditional Johnson & Strom (Myerson-modified) staging (Johnson & Strom 1989, Clin Orthop Relat Res; DOI not assigned, PMID 2912622) remains the dominant examination framework and is used throughout this topic, but candidates should recognise PCFD nomenclature.
Side-by-Side Guidance and Practice Variation
Stage-Based Management - International Consensus Themes
Evidence Level
The evidence base is predominantly Level II-IV cohort and comparative series (e.g. Wacker/Saxby 2002; Ettinger 2019), with biomechanical/cadaveric support for soft-tissue reconstruction (Choi/Deland 2003) and expert-consensus classification work (Johnson & Strom 1989; PCFD consensus 2020). High-quality RCTs comparing reconstruction strategies are lacking, so recommendations are graded on expert consensus and cohort outcomes rather than Level I data.
Current Controversies and Ongoing Research
Controversy 1: Isolated MDCO vs MDCO + FDL Transfer for Stage IIA
- Less invasive
- Preserves FDL function (digital flexion)
- Some studies show 75% success with isolated MDCO in Stage IIA
- Strong medium-term cohort support (Wacker/Saxby 2002: mean AOFAS 48.8 to 88.5, only 2/44 failures)
- Addresses tendon pathology directly and restores dynamic arch support
- Durable correction with preserved subtalar motion
Current consensus: MDCO + FDL transfer is the standard joint-sparing reconstruction, but isolated MDCO is acceptable in highly selected Stage IIA patients with minimal tendon pathology.
Controversy 2: Evans vs Cotton Osteotomy for Stage IIB
- Addresses lateral column shortening directly
- Higher non-union rate (10%)
- Lateral column pain common (30%, usually resolves)
- Addresses first ray hypermobility
- Lower non-union rate (5%)
- Does not address lateral column directly
Current consensus: Evans preferred for most Stage IIB cases, Cotton reserved for patients with first ray hypermobility or calcaneocuboid arthritis.
Controversy 3: Early Weight-Bearing Post-Surgery
Traditional protocol: Non-weight-bearing 6-12 weeks
Accelerated protocol: Protected weight-bearing at 2-4 weeks in CAM boot
Evidence: Limited RCTs. Some studies suggest accelerated weight-bearing safe with rigid internal fixation (locking plates), but higher risk of hardware failure and non-union. Current consensus: Non-weight-bearing until radiographic evidence of healing.
Future Directions
Ongoing research:
- Biologic augmentation (PRP, stem cells) for Stage I tendon healing
- Patient-specific 3D-printed cutting guides for osteotomies (improved accuracy)
- Minimally invasive techniques for FDL transfer
- Ankle replacement (vs fusion) for Stage IV with good bone stock
- Long-term outcomes of spring ligament reconstruction (over 10 years)