Congenital Posteromedial Bowing | Angle Remodels, Length Lags | Calcaneovalgus + Ankle Sequelae | NOT NF1
- Two separate problems: the ANGULAR bow remodels spontaneously, but the LIMB-LENGTH DISCREPANCY is progressive and is the main long-term issue
- LLD is NOT trivial — mean 3-4 cm at maturity (Hofmann & Wenger 1981); greater initial bow predicts greater final shortening (Pappas 1984)
- Reduced ankle dorsiflexion often persists and does not fully normalise with growth
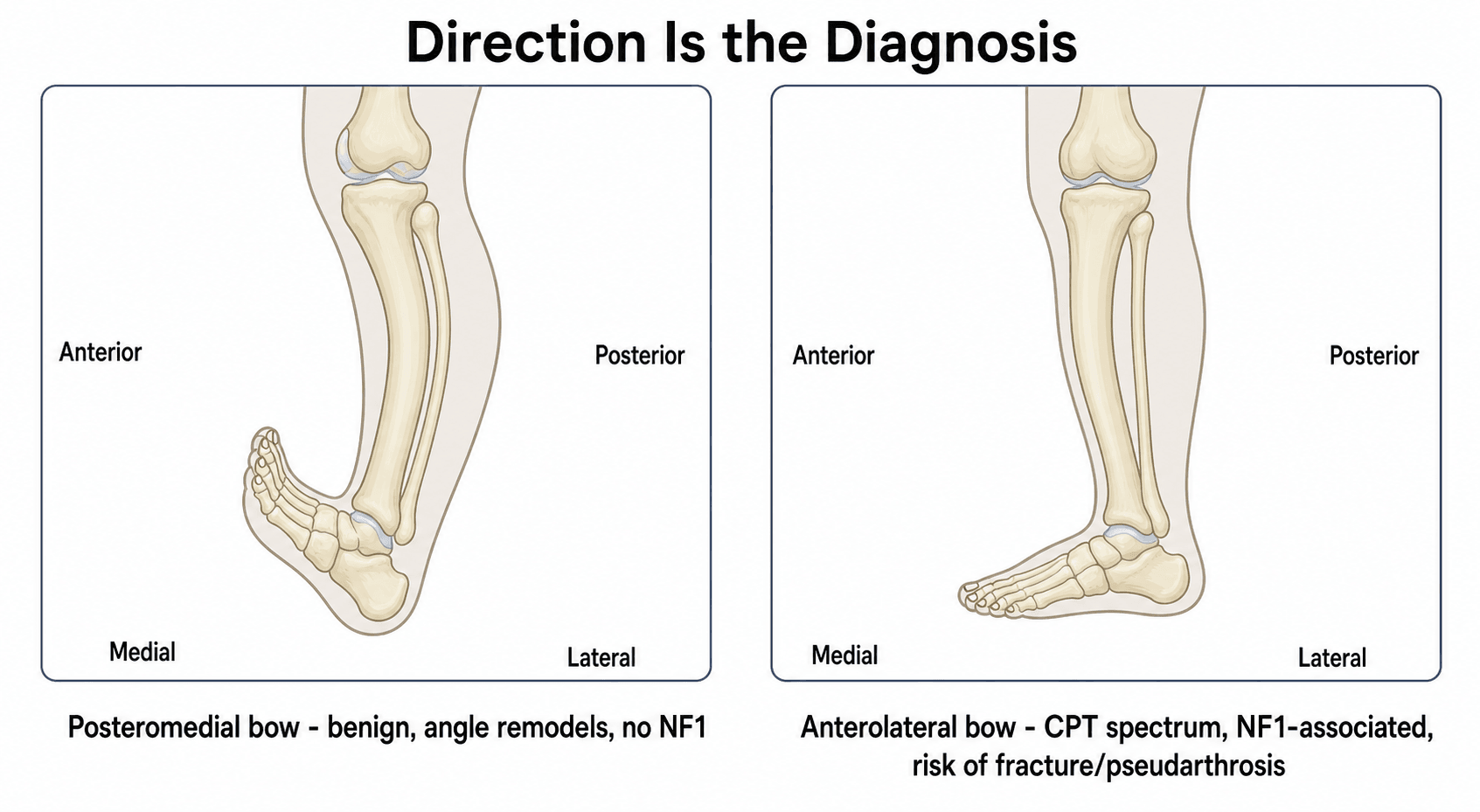
- NOT associated with NF1 — this is what distinguishes it from anterolateral (CPT) bowing; posteromedial bow does NOT fracture or form pseudarthrosis
- Calcaneovalgus foot is almost universal at birth and usually resolves; the tibial shortening does not
- “Trap: posteromedial bow is benign for ANGLE but NOT for LENGTH — predict LLD with the multiplier method and plan equalisation
- “Direction is the diagnosis: posteromedial + calcaneovalgus = benign bow; anterolateral + NF1 = pre-pseudarthrosis (CPT)
- “Discrepancy proportion is stable after ~12 months, allowing reliable prediction of LLD at maturity
- “Surgery is for the discrepancy (epiphysiodesis / lengthening), not usually for the residual angulation
The classic exam trap is calling this "benign and self-resolving". The angular bow does remodel spontaneously (mostly in the first 1-4 years), but the limb-length discrepancy is progressive and is the dominant long-term problem — mean 3-4 cm at maturity, sometimes greater than 5 cm.
Critical distinction: posteromedial bow (benign for angle, never fractures) vs anterolateral bow (the pre-pseudarthrosis stage of CPT, strongly NF1-associated, high fracture/pseudarthrosis risk). Get the direction and the NF1 screen right.
A calcaneovalgus foot is almost universal at birth and usually resolves with stretching. However, reduced ankle dorsiflexion (and sometimes calf/peroneal weakness) frequently persists and does not fully normalise.
Discrepancy proportion is stable after about 12 months, so use the multiplier method to predict LLD at maturity. Most mild bows need only observation, but a substantial minority need epiphysiodesis or lengthening — counsel families about this early.
- Posteromedial Bow
- Posterior + medial (concave anteromedial)
- Anterolateral Bow (CPT spectrum)
- Anterior + lateral (anterolateral)
- Posteromedial Bow
- No
- Anterolateral Bow (CPT spectrum)
- Yes (about 50-90%)
- Posteromedial Bow
- No
- Anterolateral Bow (CPT spectrum)
- High (pre-pseudarthrosis lesion)
- Posteromedial Bow
- Remodels spontaneously (mostly under age 4)
- Anterolateral Bow (CPT spectrum)
- Progresses, does not remodel
- Posteromedial Bow
- Calcaneovalgus
- Anterolateral Bow (CPT spectrum)
- None typical
- Posteromedial Bow
- Progressive limb-length discrepancy (mean 3-4 cm)
- Anterolateral Bow (CPT spectrum)
- Fracture, pseudarthrosis, refractory non-union
- Posteromedial Bow
- Observe bow; equalise length (epiphysiodesis / lengthening)
- Anterolateral Bow (CPT spectrum)
- Bracing, bypass grafting, complex reconstruction
BOWEDPosteromedial Bow - Core Features
Hook:The BOW is BOWED: Bow remodels, One leg short, Without NF1, Equalise length, Dorsiflexion limited.
DIRECTIONDistinguishing the Two Congenital Bows
Hook:DIRECTION decides everything: posteromedial + calcaneovalgus + no NF1 = benign bow with a length problem; anterolateral + NF1 = pre-pseudarthrosis.
PLANManaging the Length Problem
Hook:Have a PLAN for the length: Predict it, treat Length not angle, Approach by size, and often act Near maturity.
Overview and Epidemiology
Congenital posteromedial bowing of the tibia (CPMBT) is a sporadic deformity present at birth in which the tibia (and usually the fibula) is angulated posteriorly and medially, accompanied by tibiofibular shortening and a calcaneovalgus foot. It is almost always unilateral. The deformity is benign in the sense that it does not fracture or form a pseudarthrosis, but it is not simply self-resolving: while the angular bow remodels, the limb-length discrepancy is progressive and frequently requires treatment.
- Rare; reported as roughly 1 per 1,000 to 1 per several thousand live births in older series (exact incidence uncertain — most evidence is small single-centre cohorts)
- Usually unilateral; the left side is more frequently affected in collated case-series data
- A slight male predominance is reported in pooled literature, though individual series vary
- Sporadic — no Mendelian inheritance pattern and no reproducible familial clustering
- An association with firstborn status has been noted, supporting an intrauterine-packaging mechanism
the two components behave oppositely over time. According to PubMed, Pappas (1984) followed 33 patients and showed that the posterior and medial angular components reduce markedly with growth, but tibial shortening persists and is proportional to the initial bow, with absolute discrepancies of 3.3-6.9 cm at maturity (DOI/PMID 6490868).
Pathophysiology and Mechanisms
the tibia is normally straight in both the sagittal and coronal planes, with a triangular cross-section. Bone remodels throughout childhood in response to physeal growth and mechanical (Heuter-Volkmann) forces, which is why a flexible neonatal angular deformity can correct.
- Posterior + medial diaphyseal angulation — apex posteromedial, concavity anteromedial; initial bow at birth ranges from roughly 25 to 70 degrees
- Normal bone architecture — no narrowed/sclerotic canal, no cystic lesion and no hamartomatous fibrous tissue (these are features of the CPT spectrum, not of posteromedial bow)
- Tibial and fibular shortening present from birth and progressive in absolute terms through growth
- Distal tibial changes can develop — wedging of the distal tibial epiphysis, fibular hypoplasia and valgus inclination of the distal articular surface in some children
Two mechanisms of angular correction were described by Shah, Doddabasappa and Joseph (2009): rapid early physeal realignment and slower diaphyseal remodelling. Most correction occurs in the first year, slows markedly thereafter, and may leave residual deformity beyond 4 years of age — so it is incorrect to promise complete resolution by 2-3 years (PMID 19339901).
the leading hypothesis is intrauterine moulding / packaging (fetal constraint of a dorsiflexed, externally rotated foot pressing the leg posteromedially), supported by the firstborn association, the universal calcaneovalgus foot and prenatal ultrasound detection. It is not a positional deformity in the trivial sense, because the shortening is a true growth disturbance, not just a postural curve.
- Calcaneovalgus foot — almost universal at birth, usually resolves
- Reduced ankle dorsiflexion and sometimes calf/peroneal muscle weakness — may persist into later childhood (Pappas described early posterior soft-tissue fullness evolving into relative muscle atrophy)
- Progressive limb-length discrepancy — the dominant long-term issue
Classification Systems
Severity by Initial Bow — and What It Predicts
There is no formal eponymous classification for CPMBT. The clinically useful grading is by the initial angular bow, because — per Hofmann & Wenger and Pappas — the greater the initial bow, the greater the eventual limb-length discrepancy. Severity therefore predicts the length problem, not whether the angle will correct (the angle corrects in nearly all cases).
- Angular outcome
- Remodels well, early
- Anticipated LLD risk
- Lower projected discrepancy
- Implication
- Observe; predict LLD with multiplier
- Angular outcome
- Remodels, residual medial bow may persist
- Anticipated LLD risk
- Moderate projected discrepancy
- Implication
- Monitor; plan equalisation if projection significant
- Angular outcome
- Remodels but may leave residual deformity past age 4
- Anticipated LLD risk
- High projected discrepancy (often over 4-5 cm)
- Implication
- Likely epiphysiodesis or lengthening near maturity
The angle is monitored radiographically using anteroposterior and lateral interphyseal (or diaphyseal) angles; the length is tracked as percentage tibial shortening (affected/normal length).
Clinical Assessment
- Bowing noted at birth or early infancy
- May have calcaneovalgus foot noted
- Usually no pain or functional limitation
- Family history (rare but may be present)
- No history of trauma
Physical Examination
- Posterior and medial bowing of tibia
- May be bilateral (50-60%)
- Calcaneovalgus foot (common association)
- Assess for other deformities
- Bowing is palpable
- No pseudarthrosis site (unlike CPT)
- Normal bone structure
- Ankle: characteristic calcaneovalgus posture at birth (foot dorsiflexed against the shin); later, reduced ankle dorsiflexion may persist
- Test active plantarflexion / toe-walking — calf and peroneal weakness can be present
- Knee and hip: usually normal
- Angular bow (clinical + radiographic interphyseal angles, AP and lateral)
- Limb-length discrepancy — measure clinically (block test, galeazzi) and confirm radiographically; this is the key longitudinal measurement
- Foot position (calcaneovalgus assessment)
Investigations
- Assess posteromedial bowing
- Measure bowing angle
- Evaluate bone structure (should be normal)
- Assess for any cystic changes (should be absent)
- Evaluate medullary canal (should be normal)
- Measure bowing angle accurately
- Assess alignment
- Evaluate for leg length discrepancy
- Assess foot position
- Posteromedial diaphyseal angulation with normal bone architecture — normal cortical thickness, no canal narrowing/sclerosis, no cyst, no pseudarthrosis (these features exclude the CPT spectrum)
- Tibial and fibular shortening, often with fibular hypoplasia distally
- Possible distal tibial epiphyseal wedging and increased lateral distal tibial angle deviation (ankle valgus) over time
- Track the angular bow (AP and lateral interphyseal angles) — expect rapid early correction
- Track the percentage tibial shortening and predict LLD at maturity using the multiplier method — the proportional discrepancy is stable after about 12 months, making prediction reliable
- Follow at 6-12 month intervals in early childhood, then periodically; continue surveillance until skeletal maturity because LLD progresses and ankle deformity can evolve — do NOT discharge once the angle looks better
posteromedial bowing can be detected on antenatal ultrasound (reported from the second trimester); recognising it prenatally allows appropriate parental counselling and avoids misdiagnosis as a skeletal dysplasia or fracture.
- CT/MRI — not routinely indicated; reserve for surgical planning or atypical features
- Genetic / NF1 testing — only if NF1 stigmata raise the possibility of an anterolateral (CPT) lesion instead
Prenatal Diagnosis and Antenatal Counselling
The topic's own investigation and aetiology sections note that posteromedial bowing can be recognised on antenatal ultrasound from the second trimester and that this recognition helps avoid misdiagnosis as a skeletal dysplasia or intrauterine fracture — but the prenatal picture and how to counsel expectant parents deserve development, because families are increasingly referred before birth.
What CPMBT looks like on fetal ultrasound:
- An isolated, usually unilateral long-bone bow angulated posteriorly and medially, with the concavity anteromedial
- Normal bone echogenicity and mineralisation — the shaft is not thin, wide, fractured, sclerotic or cystic
- Normal length and morphology of the other long bones, a normal chest circumference and no other skeletal anomaly
- A commonly associated dorsiflexed (calcaneovalgus) foot pressed against the shin — a supportive clue consistent with the intrauterine-moulding hypothesis
- Mild-to-moderate tibial shortening may already be measurable relative to the contralateral side
The fetal differential of a bent or short long bone — the reason the read matters:
- Discriminating features
- Multiple bones affected, bilateral, short/broad or under-mineralised bones, in-utero fractures, small chest, other anomalies
- Discriminating features
- Bow apex anterolateral (opposite direction), may show cortical narrowing; associated NF1 family history
- Discriminating features
- Callus or a discrete fracture line, angulation at a focal point rather than a smooth diaphyseal curve
- Discriminating features
- Circumferential soft-tissue groove, distal lymphoedema, digital amputation
Reassuring combination: an isolated, unilateral, smoothly curved posteromedial bow with normal mineralisation, no fractures, normal other bones and a calcaneovalgus foot is characteristic of CPMBT rather than a lethal or generalised skeletal condition.
Antenatal counselling should mirror the postnatal message and avoid two opposite errors — needless alarm (mistaking a benign bow for a dysplasia) and false reassurance ("it will simply straighten"). Parents should be told that the angular deformity is expected to remodel after birth, that the leg is nonetheless likely to remain somewhat short with a progressive discrepancy requiring surveillance and possibly later equalisation, and that the condition does not fracture or form a pseudarthrosis. Postnatal confirmation with radiographs and clinical examination, plus a review of the newborn for the calcaneovalgus foot and reduced ankle dorsiflexion, completes the assessment.
An isolated, unilateral, smoothly curved posteromedial tibial bow with normal mineralisation, no fractures and normal other bones is CPMBT, not a skeletal dysplasia. The single most useful discriminators are direction (posteromedial, not anterolateral), whether one bone or many are involved, and the presence of fractures or abnormal mineralisation (present in dysplasias, absent here). Counsel that the angle remodels but the length lags — never promise complete resolution.
Differential Diagnosis
The diagnosis is usually clinical, but the direction of the bow and the surrounding features separate it from dangerous mimics. The single most important distinction is from anterolateral bowing (the congenital pseudarthrosis spectrum), which is managed completely differently.
- Direction of bow
- Posterior + medial
- Key associations
- Calcaneovalgus foot, shortening
- Natural history
- Angle remodels; LLD progresses
- Distinguishing point
- Calcaneovalgus + no NF1 + never fractures
- Direction of bow
- Anterior + lateral
- Key associations
- NF1 (50-90%), fibular involvement
- Natural history
- Fractures, pseudarthrosis, no remodelling
- Distinguishing point
- NF1 stigmata, sclerotic/cystic canal — do NOT osteotomy
- Direction of bow
- Varus, symmetrical, bilateral
- Key associations
- Normal toddler, no shortening
- Natural history
- Resolves by age 2-3 years
- Distinguishing point
- Bilateral, symmetric, no posterior component
- Direction of bow
- Proximal tibia varus + internal rotation
- Key associations
- Obesity, early walking
- Natural history
- Progressive metaphyseal change
- Distinguishing point
- Metaphyseal-diaphyseal angle, proximal not diaphyseal
- Direction of bow
- Variable bow + longitudinal deficiency
- Key associations
- Foot/ray deficiency, instability
- Natural history
- Fixed deficiency
- Distinguishing point
- Absent/hypoplastic bone, foot deficiency
- Direction of bow
- Often anterolateral or varus, bilateral
- Key associations
- Metaphyseal cupping/fraying, biochemical changes
- Natural history
- Corrects with medical treatment
- Distinguishing point
- Bilateral, biochemistry abnormal, metaphyseal flaring
The cardinal trap is mistaking an anterolateral bow (pre-pseudarthrosis of CPT) for a posteromedial bow. Performing an osteotomy or biopsy on a CPT-spectrum tibia can precipitate a refractory pseudarthrosis. Always confirm the direction of the bow and screen for NF1 (cafe-au-lait macules, axillary/inguinal freckling, family history) before any surgical decision.
Management Algorithm

Treatment Philosophy
Management separates the angle (treated by patience) from the length (treated by surgery when projected discrepancy is significant).
Goals:
- Confirm the diagnosis and exclude an anterolateral (CPT) lesion
- Allow the angular bow to remodel — avoid osteotomy of a remodelling bow
- Manage the calcaneovalgus foot and any persistent ankle stiffness
- Predict and equalise the limb-length discrepancy — the core long-term task
Treatment options:
- Observation with serial measurement — for the angle in essentially all cases, and for length until the projection is clear
- Foot/ankle care — stretching for calcaneovalgus; guided growth for symptomatic ankle valgus
- Contralateral epiphysiodesis — for moderate predicted discrepancy, timed by growth-remaining
- Tibial lengthening (circular/hexapod external fixator, or lengthening over/with a nail) — for large discrepancies, with simultaneous residual deformity correction
- Tibial osteotomy — uncommon, for residual symptomatic angular/ankle deformity, usually combined with a length procedure
Surgery is therefore not rare in the way "benign and self-resolving" implies — across published series a substantial minority of children undergo limb reconstruction. Wright et al (2018) reported limb reconstruction in 20 of 38 patients (53%); Di Gennaro/Trisolino et al (2020) operated on 26 of 44 (PMID 29707059; PMID 32620101).
Surgical Techniques
Tibial Lengthening with Deformity Correction
significant predicted limb-length discrepancy, especially with residual angular/ankle deformity.
- Plan the corticotomy level, lengthening target and any acute/gradual angular correction from full-length standing films
- Frame — a circular or hexapod external fixator allows gradual lengthening plus multiplanar correction; uniplanar rails need adequate Schanz-screw spread to avoid valgus drift of the distracting segment
- Lengthening over/with a nail or a magnetic internal lengthening nail can shorten external-fixator time in suitable children
- Distract at roughly 1 mm/day (titrated), monitoring regenerate and ankle
- Protect the ankle — anticipate equinus/valgus tendencies; physiotherapy and sometimes temporary foot-frame extension
good/excellent bone results in modern series, with mean length gains around 4-5 cm per episode and residual LLD typically under 1.5 cm; complications include ankle stiffness, tibial valgus, pin-tract infection and regenerate fracture (Johari & Anjum 2024) (PMID 38594586).
Complications
- Progressive limb-length discrepancy — the dominant problem; mean 3-4 cm, frequently over 2.5 cm, occasionally over 5 cm. NOT a trivial sub-centimetre difference
- Residual angular deformity — uncommon but may persist beyond age 4 if the initial bow was severe
- Persistent reduced ankle dorsiflexion and calf/peroneal weakness
- Ankle valgus from distal tibial wedging / fibular hypoplasia
- Pin-tract infection
- Premature/delayed consolidation, regenerate problems
- Neurovascular irritation, joint subluxation during distraction
- Regenerate fracture and tibial valgus malalignment
- Ankle stiffness/equinus
- Recurrence of discrepancy after early lengthening (higher when lengthening is done young — recurrence rates are significantly higher in children lengthened under age 10)
- Need for repeat lengthening if performed far from maturity
- Accurate prediction (multiplier method) and correct timing of equalisation
- Circular/hexapod fixation or internal lengthening with adequate stability
- Proactive ankle protection and physiotherapy during distraction
the untreated complication that matters is the progressive discrepancy, not fracture (this condition does not pseudarthrose); the treatment-related complications are those of limb reconstruction.
Follow-up and Postoperative Care
- At diagnosis — baseline clinical exam, radiographs, document angle, percentage shortening, foot/ankle posture
- 6-12 monthly through early childhood, then periodic review until skeletal maturity
- Each visit: re-measure interphyseal angles and LLD, re-run the multiplier prediction, reassess ankle dorsiflexion
- Do not discharge once the angle improves — the discrepancy and ankle deformity evolve over years
- External fixator until regenerate consolidation (healing index roughly 30-50 days/cm); protect against valgus drift
- Aggressive ankle and knee physiotherapy throughout distraction and consolidation to prevent stiffness/equinus
- Staged weight-bearing as regenerate matures; remove fixator after radiographic union of all cortices
- Continue follow-up for recurrence of discrepancy (especially after early lengthening) and for regenerate fracture after frame removal
- Brief recovery, early mobilisation
- Monitor to confirm the predicted equalisation is achieved at maturity
Outcomes and Prognosis
prognosis is excellent — the posteromedial bow remodels spontaneously and substantially, with most correction in the first year and the majority of children needing no angular surgery. A mild residual medial component may remain.
prognosis is guarded without planning — the discrepancy is progressive and proportional to the initial bow:
- Hofmann & Wenger (1981): mean LLD 3.1 cm at follow-up, with 9 of 13 children over 2.5 cm and usually progressing
- Pappas (1984): absolute tibial discrepancy 3.3-6.9 cm at maturity, greater with greater initial bow
- Modern series confirm progressive shortening and frequent need for equalisation (epiphysiodesis or lengthening)
the calcaneovalgus foot resolves, but reduced ankle dorsiflexion may persist and ankle valgus can develop from distal tibial changes.
- Greater initial angular bow (the single best predictor)
- Greater early percentage shortening
- Distal tibial epiphyseal wedging / fibular hypoplasia (predict ankle valgus)
generally good. With appropriate prediction and timely, well-executed equalisation, most patients reach maturity with near-equal leg lengths, neutral alignment and good function; outcomes after lengthening are good in modern series, though at the cost of the morbidity of reconstruction. The key message is that good outcomes depend on surveillance and planning, not on assuming the condition disappears on its own.
The Posterior Soft-Tissue Mass, Calf Atrophy and the Persistent Ankle Dorsiflexion Deficit
The topic repeatedly names a calf/peroneal weakness, a persistent reduction in ankle dorsiflexion, and (in the pathophysiology section) "posterior soft-tissue fullness evolving into relative muscle atrophy" — and the controversies section flags a debated neuromuscular contribution — yet the soft-tissue and muscle natural history is never developed as a coherent entity. It matters because it is the part of CPMBT that does not reliably improve, unlike the angular bow.
According to PubMed, Pappas described enlargement of the posterior soft tissues of the affected leg in early life that evolves into a relative muscle atrophy in later years, together with an initial calcaneovalgus foot and a decrease in ankle motion that does not improve with age (DOI is for the related Shah series; Pappas is PMID 6490868, no DOI indexed). Shah, Doddabasappa and Joseph (2009) likewise recommended following all children to maturity specifically to detect residual muscle weakness alongside limb-length inequality and ankle deformity (DOI).
- At birth the foot sits in calcaneovalgus (dorsiflexed against the shin); this posture resolves, but the underlying posterior-compartment weakness and a fixed reduction in ankle dorsiflexion frequently persist
- The functional consequence is weak plantarflexion / push-off — the child may have difficulty with toe-walking and heel-rise, and a subtly weaker calf on the affected side
- This is distinct from the calcaneovalgus foot itself (a flexible neonatal foot posture that is comprehensively covered as its own entity); here the concern is the leg's posterior musculature and the ankle's motion arc, which are CPMBT-specific and long-lasting
- Compare calf girth side to side; document active and passive ankle dorsiflexion/plantarflexion and single-leg heel-rise as the child matures
- Note that reduced dorsiflexion here is a motion/strength deficit, separate from the later ankle valgus produced by distal tibial wedging and fibular hypoplasia — the two can coexist and should be recorded separately
- Physiotherapy and stretching for the ankle motion arc and calf strength; this is the mainstay and surgery is rarely needed
- A fixed equinus/limited-dorsiflexion contribution should be recognised before any lengthening, because distraction tends to aggravate equinus and valgus — the ankle must be protected (physiotherapy, sometimes temporary foot-frame extension) during reconstruction
- True operative soft-tissue correction (tendo-Achilles or posterior release) is reserved for the rare rigid or functionally limiting deformity
In CPMBT the angle remodels and the calcaneovalgus foot resolves, but the posterior soft-tissue mass evolves to relative calf atrophy and the reduced ankle dorsiflexion tends to persist (Pappas: ankle motion "does not improve with age"). Examine calf girth, dorsiflexion arc and heel-rise at every review, keep this deficit separate from later distal-tibial ankle valgus, and remember that any lengthening will worsen equinus/valgus unless the ankle is actively protected.
Guidelines, Registries & Global Practice
Global epidemiology: congenital posteromedial bowing is rare and sporadic worldwide, reported across all populations without a clear geographic or ethnic predilection. Evidence is dominated by small single-centre cohorts (typically 13-51 patients) from Europe, North America, the Middle East and South Asia — there is no large population registry specific to this deformity, and no dedicated society guideline. International multicentre work is now emerging through limb-difference outcome programmes (e.g. the LIMB-Q Kids patient-reported outcome measure, validated across 16 sites in 7 countries; Chhina et al 2025).
Where guidance converges (society/textbook level):
- Practice position on CPMBT
- Distinguish posteromedial (benign angle, progressive LLD) from anterolateral (CPT); observe angle, predict and equalise length
- Practice position on CPMBT
- Surveillance to maturity; hexapod external-fixator reconstruction for significant LLD/residual deformity (Wright et al, GOSH/RNOH)
- Practice position on CPMBT
- Staged, individualised reconstruction — lengthening plus targeted ankle/length procedures (Di Gennaro/Trisolino)
- Practice position on CPMBT
- Multiplanar correction with circular/hexapod frames; multiplier-method LLD prediction (Paley)
All converge on the same core message: do not osteotomy the remodelling bow, and do plan for the progressive length discrepancy.
High- vs limited-resource practice variation:
- Well-resourced settings: magnetic internal lengthening nails, hexapod fixators and guided-growth implants reduce external-fixator burden; serial scanograms / EOS imaging and routine multiplier prediction.
- Limited-resource settings: reliance on clinical block-test measurement and plain radiographs; Ilizarov / circular external fixators remain the workhorse for lengthening (large Indian and Middle-Eastern series), with epiphysiodesis as a low-cost option for moderate discrepancies; longer follow-up logistics and counselling are the main constraints.
Controversies and Areas of Uncertainty
The biggest practical debate. Lengthening near skeletal maturity avoids repeat procedures and reduces recurrence (Johari & Anjum 2024; Wright et al 2018 showed higher recurrence under age 10). Yet experienced centres report that younger children with very large projected discrepancies can be lengthened safely with shorter fixator time and fewer complications (Sagade/Chaudhary 2021). No randomised data exist; decisions are individualised.
For moderate predicted discrepancies, contralateral epiphysiodesis is simpler and lower-morbidity but sacrifices height; lengthening preserves height and corrects deformity but carries reconstruction morbidity. The threshold between the two is not standardised and depends on projected LLD, family preference and stature.
Older teaching implied the leg would 'catch up'. Contemporary prospective data (Kamath/Shah 2025) show only partial resolution of percentage shortening (20% to 13% by age 6) with persistent absolute discrepancy — so true catch-up is limited and prediction, not optimism, should guide planning.
Intrauterine moulding is the leading hypothesis (firstborn association, calcaneovalgus foot, prenatal detection), but the cause of the growth disturbance producing progressive shortening — as opposed to the postural bow — remains unexplained. A rare neuromuscular/local contribution (the persistent ankle weakness) is debated.
MCQ Practice Points
Q: What is the natural history of congenital posteromedial bow of the tibia? A: The angular bow remodels spontaneously, but the limb-length discrepancy is progressive. Most angular correction occurs in the first 1-4 years; the tibial shortening, however, increases through growth (mean about 3-4 cm at maturity; Hofmann & Wenger 1981, Pappas 1984) and is proportional to the initial bow. It is benign in that it never fractures or pseudarthroses.
Q: What is the key difference between posteromedial bow and anterolateral bow (the CPT spectrum)? A: Direction and NF1. Posteromedial bow is posterior + medial, has a normal canal, is NOT NF1-associated, never fractures, and its angle remodels (length progresses). Anterolateral bow is the pre-pseudarthrosis lesion: NF1-associated (50-90%), abnormal canal, and prone to fracture and pseudarthrosis - it must not be osteotomised.
Q: How do you predict the limb-length discrepancy at maturity? A: The multiplier method. The proportional discrepancy is stable after about 12 months of age, so the discrepancy at maturity can be predicted reliably and used to time equalisation (epiphysiodesis or lengthening).
Q: What foot/ankle features accompany posteromedial bow of tibia? A: A calcaneovalgus foot (almost universal at birth, usually resolves with stretching) and often persistently reduced ankle dorsiflexion, which may not normalise. Distal tibial wedging can cause ankle valgus later.
Q: What treatment does posteromedial bow of tibia require? A: Observe the angle; treat the length. The bow is observed (no osteotomy of a remodelling deformity), but the progressive discrepancy frequently needs contralateral epiphysiodesis (moderate) or tibial lengthening (large), with over half of patients in some tertiary series undergoing limb reconstruction (Wright et al 2018).
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 6-month-old infant is referred with posteromedial bowing of one tibia noted since birth, with a calcaneovalgus foot. Radiographs show posteromedial bowing with normal bone architecture and a normal medullary canal. How would you assess and counsel this family?”
“A 2-year-old presents with tibial bowing. The parents are worried because a child they know has congenital pseudarthrosis of the tibia. How would you differentiate posteromedial bow from anterolateral bow (CPT spectrum)?”
“A 4-year-old with known posteromedial bow attends follow-up. The angular bow has largely remodelled, but the affected tibia is now clearly short - a 2.5 cm discrepancy clinically, with the multiplier method projecting around 5 cm at maturity. The parents were previously told the condition would 'resolve on its own'. How do you proceed and counsel them?”
Key Facts
- Sporadic congenital deformity, usually unilateral, present at birth
- Posteromedial diaphyseal bow + tibiofibular shortening + calcaneovalgus foot
- Angle remodels spontaneously; limb-length discrepancy is progressive
- NOT NF1-associated and never fractures/pseudarthroses
Distinctions from Anterolateral (CPT) Bow
- Direction: Posteromedial vs Anterolateral
- Bone canal: Normal vs Narrowed/sclerotic/cystic
- NF1: No vs 50-90%; Fracture risk: No vs High
- Never osteotomy/biopsy a suspected CPT lesion
Management Algorithm
- Observe the angle - do not osteotomy a remodelling bow
- Predict LLD with the multiplier method (stable proportion after ~12 months)
- Moderate LLD: contralateral epiphysiodesis; Large LLD: tibial lengthening
- Circular/hexapod frame for simultaneous lengthening + deformity correction
- Address ankle valgus (medial distal tibial guided growth) when present
Natural History (verified)
- Angular bow: most correction in year 1, limited remodelling after age 4
- LLD: mean 3-4 cm at maturity, proportional to initial bow (Hofmann & Wenger; Pappas)
- Over half needed limb reconstruction in some tertiary series (Wright et al)
- Reduced ankle dorsiflexion may persist; calcaneovalgus foot usually resolves
Complications
- Untreated: progressive LLD (the main morbidity), ankle valgus, ankle stiffness
- Lengthening: pin-tract infection, regenerate fracture, tibial valgus, stiffness
- Recurrence of LLD higher when lengthening done under age 10
- No fracture/pseudarthrosis risk (this is NOT the CPT spectrum)
Evidence Base
According to PubMed, the evidence below has been verified against the primary sources.
Progression of Leg-Length Discrepancy (Landmark)
- 13 children followed a mean of 4 years from diagnosis
- Discrepancy at follow-up 1.9-5.6 cm (mean 3.1 cm), usually progressive
- 9 of 13 had a discrepancy greater than 2.5 cm
- Direct relationship between initial tibial bow and eventual leg-length discrepancy
Growth Pattern and Predictability (Landmark)
- 33 patients with congenital posteromedial bowing of tibia and fibula
- Bow 25-70 degrees at birth; absolute tibial discrepancy 3.3-6.9 cm at maturity
- Proportional length difference stable after 12 months, allowing prediction at maturity
- Initial calcaneovalgus foot and reduced ankle motion that does not improve with age
Mechanisms of Correction and Distal Tibial Changes
- 20 children; two mechanisms of correction - physeal realignment and diaphyseal remodelling
- Rapid angular resolution in year one, then markedly slower; residual deformity can persist beyond age 4
- Shortening proportional to severity (up to 40% in one case)
- Distal tibial epiphyseal wedging and fibular hypoplasia with ankle valgus in some
A Benign Condition or a Case for Limb Reconstruction?
- 38 patients; greatest deformity correction in the first year, limited remodelling after age 4
- Absolute LLD increased throughout growth (mean 14.3% tibial discrepancy)
- 20 of 38 (53%) required limb reconstruction for residual deformity and/or worsening LLD
- Higher LLD recurrence when lengthening performed under age 10
Deformity Progression in a Large Series
- 44 children - one of the largest single-institution series
- Progressive spontaneous correction of angular deformity but progressive increase in LLD
- 26 of 44 underwent surgery (mostly limb lengthening; also epiphysiodesis, osteotomy, distal tibial hemiepiphysiodesis)
- Final lateral distal tibial angle ankle valgus correlated with residual lateral interphyseal angle
Timing of Lengthening - Early vs Late
- 28 tibial lengthenings in 23 patients with circular fixators
- Mean initial LLD 3.4-4.1 cm; projected LLD at maturity often greater than previously reported (up to about 9.5 cm)
- Younger children (5 years or under) had larger deformities but shorter fixator duration/index and fewer complications
- Good/excellent bone results in both age groups
Triplanar Remodelling and Resolution of Shortening (Recent)
- 51 children prospectively followed (median 48 months)
- Posterior diaphyseal bow remodels fastest; remodelling minimal after 4-6 years of age
- Shortening partially resolves (20% at presentation to 13% at age 6 years) but persists
- Multiplier-method prediction of shortening at maturity is reliable after age 2 years