Medial + Posterior Oblique Ligament Failure | Anteromedial Rotatory Instability | Often with ACL
- Superficial MCL (sMCL) is the primary restraint to valgus at 30 degrees flexion
- Posterior oblique ligament (POL) resists internal rotation and is the key to AMRI
- Semimembranosus has 5-6 insertional arms - main dynamic stabiliser of the PMC
- Isolated PMC injury is uncommon - always assess for ACL, PCL, meniscus
- AMRI is the hallmark instability pattern when PMC is deficient
- Acute repair within 3 weeks gives better results than chronic reconstruction
- “Valgus opening at 0 degrees = PMC plus cruciate injury, not isolated MCL
- “Anterior drawer in external rotation tests the POL and PMC
- “Slocum test with foot in external rotation exposes AMRI from PMC loss
- “MRI shows sMCL oedema, dMCL thickening, POL stripping, semimembranosus oedema
MDPSPMC Static Stabilisers
Hook:MDPS - the four core static PMC structures you must know for the viva!
Overview and Epidemiology
Posteromedial corner injury is frequently under-recognised in acute knee trauma. Up to 70 percent of PMC injuries occur as part of a multi-ligament knee injury, and an isolated grade III sMCL tear should always prompt a careful search for an associated ACL tear (most common), PCL, or meniscal lesion. Missed PMC injury leads to persistent anteromedial rotatory instability, valgus collapse, and accelerated medial compartment osteoarthritis.
- Valgus force: Lateral blow to knee or fixed foot with valgus load (football, rugby)
- External rotation: Foot planted, body rotates medially (skiing, pivoting sports)
- Combined valgus + external rotation + axial load: Classic for PMC plus ACL
- High-energy trauma: Motor vehicle collision, fall from height (multi-ligament)
- Medial pain and swelling: Localised to sMCL and POL
- Anteromedial rotatory instability: Tibial plateau subluxes anteromedially
- Reduced activity: Cutting, pivoting, and stair descent all limited
- Long-term OA: Untreated PMC deficiency leads to medial compartment wear
Pathophysiology
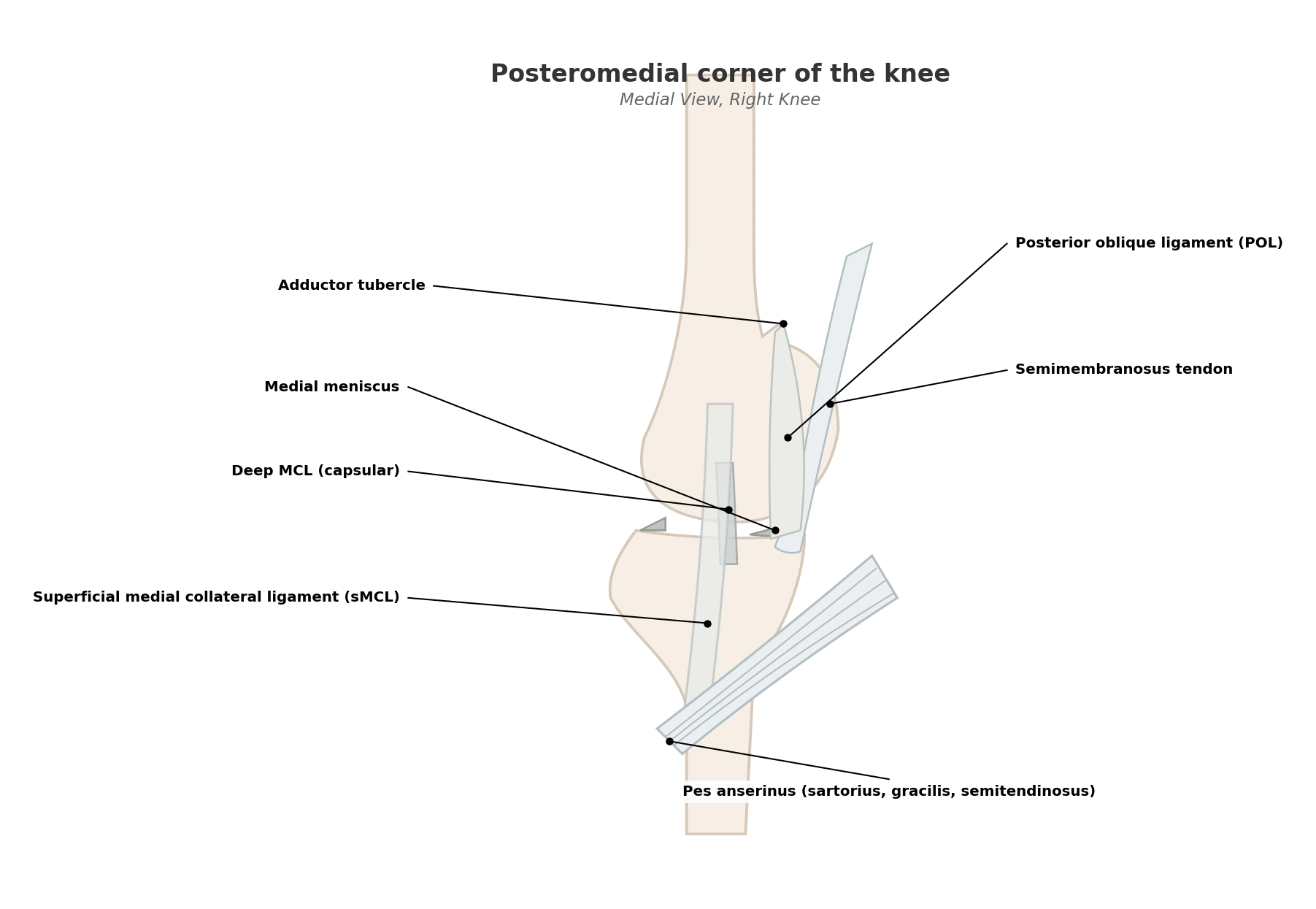
The posteromedial corner is a layered complex of static and dynamic stabilisers on the medial side of the knee. The superficial MCL (sMCL) originates from the medial femoral epicondyle and inserts 5-7 cm below the joint line on the tibia - it is the primary restraint to valgus at 30 degrees flexion. The deep MCL (dMCL) is a thickening of the medial capsule attaching to the meniscus. The posterior oblique ligament (POL) arises from the adductor tubercle and blends with the posteromedial capsule, resisting internal rotation of the tibia. The semimembranosus sends 5-6 insertional arms onto the POL, oblique popliteal ligament, and posterior capsule - it is the primary dynamic PMC stabiliser. Loss of the sMCL alone produces valgus laxity; loss of the POL produces internal rotation laxity; combined loss produces AMRI.
- Origin / Insertion
- Medial epicondyle to 5-7 cm below joint line
- Function
- Primary restraint to valgus at 30 deg
- When Injured
- Valgus laxity, medial pain, opens at 30 deg
- Origin / Insertion
- Femur and tibia, attaches to meniscus
- Function
- Secondary valgus restraint, meniscal anchor
- When Injured
- Capsular sign, meniscal tear association
- Origin / Insertion
- Adductor tubercle to posteromedial tibia
- Function
- Resists internal rotation of tibia
- When Injured
- AMRI, increased external rotation at 30 and 90 deg
- Origin / Insertion
- Ischial tuberosity to POL, oblique popliteal ligament
- Function
- Dynamic PMC stabiliser, posterior drawer
- When Injured
- Loss of dynamic restraint, posteromedial pain
Normal: sMCL + POL + semimembranosus restrain anteromedial subluxation
After PMC injury: Combined valgus and external rotation produces anteromedial tibial translation
Hughston axis: POL is the primary restraint to internal rotation at all flexion angles
Result: Tibial plateau subluxes anteromedially under valgus + ER load
Valgus + ER + axial load: Single blow disrupts ACL, sMCL, and POL together
Hyperextension: Disrupts PMC, ACL, and PCL sequentially from posterior to anterior
Posterolateral + PMC: Shares the semimembranosus and oblique popliteal ligament
High-energy knee dislocation: All four corners may be involved
Classification and Types
Anatomical Classification of PMC Injury
- Structures Injured
- sMCL fibres only
- Examination Finding
- Valgus opening at 30 deg only
- Treatment
- Hinged brace 4-6 weeks
- Structures Injured
- Capsular disruption plus meniscus attachment
- Examination Finding
- Valgus opening at 30 deg, meniscal sign
- Treatment
- Bracing, assess meniscus on MRI
- Structures Injured
- sMCL + dMCL + POL + semimembranosus
- Examination Finding
- Valgus at 0 and 30 deg, AMRI, increased ER
- Treatment
- Repair (acute) or reconstruction (chronic)
- Structures Injured
- PMC plus ACL or PCL
- Examination Finding
- Pivot, posterior sag, gross laxity
- Treatment
- Cruciate reconstruction plus PMC repair or recon
The anatomical pattern dictates the surgical plan: isolated sMCL is treated non-operatively, complete PMC needs repair or reconstruction, and PMC plus cruciate requires combined ligament surgery.
Beyond grade and timing, the location of an sMCL tear predicts healing. Proximal (femoral-sided) tears heal reliably with bracing because the ends stay apposed. Distal (tibial-sided) tears heal less predictably and are more likely to leave residual valgus laxity — and they carry a specific surgical indication: the Stener-like lesion of the knee, in which the avulsed distal sMCL retracts and flips superficial to the pes anserinus (sartorius, gracilis, semitendinosus), so the ligament end no longer contacts its tibial footprint and cannot heal with bracing. The analogy is the thumb UCL Stener lesion displaced over the adductor aponeurosis. A distal sMCL tear that is displaced/entrapped, or one with a large bony tibial avulsion, therefore favours acute surgical repair over a non-operative trial. MRI showing the distal sMCL stump lying superficial to the pes tendons is the radiographic clue.
Clinical Assessment
- Mechanism: Valgus force, external rotation, contact sport, motor vehicle collision
- Pain location: Medial joint line, posteromedial corner, proximal tibia
- Instability: Sensation of knee giving way into valgus, especially with pivoting
- Swelling: Localised medial bruising, often less than ACL injury haemarthrosis
- Inspect: Medial ecchymosis, effusion, deformity, gait
- Palpate: sMCL femoral and tibial attachments, POL at adductor tubercle, semimembranosus
- Range of motion: Often preserved unless extension block from displaced meniscus
- Neurovascular: Always check before and after reduction; peroneal nerve, popliteal vessels
Valgus stress at 30 degrees: Primary test for sMCL. Grade I = pain only, Grade II = 5-10 mm opening with firm endpoint, Grade III = greater than 10 mm opening with soft endpoint.
Valgus stress at 0 degrees (full extension): Positive only when the PMC plus cruciate ligaments are both injured. Isolated sMCL injury does not open in full extension because the cruciates and posterior capsule act as secondary restraints.
Anterior drawer in external rotation: The foot is externally rotated 15 degrees and the tibia drawn forward. Increased anterior translation compared to the uninvolved knee indicates POL and PMC injury.
Slocum test: With the knee at 90 degrees and the foot fixed in external rotation, the tibia is allowed to rotate back into neutral. The lateral tibial plateau reduces from an anteriorly subluxed position - this is the pathognomonic sign of AMRI from PMC deficiency.
- Technique
- Knee flexed 30 deg, apply valgus force
- Positive Finding
- Greater than 3 mm side-to-side difference, no endpoint
- What it Tests
- Superficial MCL integrity
- Technique
- Knee in full extension, apply valgus force
- Positive Finding
- Medial opening with knee straight
- What it Tests
- PMC plus cruciate injury (not isolated sMCL)
- Technique
- Foot in 15 deg ER, draw tibia forward
- Positive Finding
- Increased anterior translation vs normal knee
- What it Tests
- POL and PMC integrity
- Technique
- Foot in ER, knee at 90 deg, release
- Positive Finding
- Lateral plateau reduces from anterior subluxation
- What it Tests
- AMRI - pathognomonic for PMC deficiency
- Key Finding
- Valgus opening at 30 deg, AMRI
- Discriminating Sign
- Increased ER, Slocum test positive
- Imaging
- MRI sMCL oedema, POL stripping
- Key Finding
- Joint line tenderness, locking, catching
- Discriminating Sign
- McMurray positive, pain on flexion
- Imaging
- MRI meniscal signal extending to surface
- Key Finding
- Pain 5 cm below joint line, medial tibia
- Discriminating Sign
- No laxity, tenderness localised to bursa
- Imaging
- MRI localised fluid in pes bursa
- Key Finding
- Pivot shift, giving way, haemarthrosis
- Discriminating Sign
- Lachman positive, anterior drawer positive
- Imaging
- MRI ACL discontinuity, lateral femoral condyle bone bruise
- Key Finding
- Lateral or medial plateau depression
- Discriminating Sign
- Tenderness over plateau, possible valgus laxity
- Imaging
- CT or MRI confirms fracture
- Key Finding
- Medial patellar instability, lateral patellar tilt
- Discriminating Sign
- Patellar apprehension, lateral translation
- Imaging
- MRI MPFL oedema, patellar tilt
Isolated PMC injury is uncommon. In any patient with a grade III sMCL tear, always perform Lachman, posterior drawer, pivot shift, dial test, and reverse pivot shift to exclude associated cruciate or posterolateral injury. Up to 70 percent of PMC injuries have another ligament involved, and missing a concurrent ACL rupture is the most common reason for failed conservative treatment of an apparent isolated MCL injury.
VASPExamination Sequence for PMC
Hook:VASP - the four bedside tests to confirm PMC injury and exclude cruciate involvement!
Investigations
Imaging Protocol
Views: AP, lateral, skyline, tunnel views of the knee
Look for: Avulsion fracture of the medial femoral epicondyle (sMCL origin), avulsion of the adductor tubercle (POL origin), Segond equivalent, tibial plateau fracture, Pellegrini-Stieda ossification (chronic sMCL)
Stress views: Bilateral valgus stress radiographs quantify side-to-side medial opening in millimetres - useful for grade III assessment
Indication: All suspected PMC injuries, especially with suspected multi-ligament involvement
Coronal: Best for sMCL origin, midsubstance, and insertion; look for periligamentous oedema, fibre discontinuity, wavy or stripped ligament
Axial: Best for POL at adductor tubercle, semimembranosus tendon and its 5-6 arms, posteromedial capsule
Sagittal: Assesses cruciate ligaments, menisci, and posterior capsule
Bone marrow oedema pattern: Medial femoral condyle and lateral tibial plateau bruise suggests combined ACL/PMC injury
CT: Bony avulsion assessment, tibial plateau depression, fragment size for ORIF planning
CT angiogram or ankle-brachial index: Mandatory in any multi-ligament or high-energy knee injury to exclude popliteal artery injury
Stress radiographs under anaesthesia: Quantify valgus opening and external rotation before surgical planning
The diagnosis of PMC injury is clinical and MRI-confirmed. Plain radiographs exclude bony avulsion and tibial plateau fracture. MRI with corner-specific sequences (coronal for sMCL, axial for POL and semimembranosus) is the gold standard for surgical planning. Pellegrini-Stieda ossification along the proximal sMCL is a chronic finding - if you see it on a plain film, think chronic MCL insufficiency.
Management Algorithm
Isolated Low-Grade sMCL Injury (Grade I-II)
Goal: Protect healing sMCL, restore range of motion, prevent stiffness
Non-operative Protocol
Brace: Hinged knee brace locked in extension for ambulation; unlock for passive ROM 0-90 degrees
Weight-bearing: Weight-bearing as tolerated with crutches, brace locked in extension
Ice, elevation, NSAIDs: Reduce swelling and pain
Isometrics: Quadriceps sets, hamstring sets, straight leg raises
Brace: Continue for ambulation, wean when stable
ROM: Achieve full extension and 90 degrees flexion
Strengthening: Closed chain quadriceps, hamstring curls, hip abductors
Proprioception: Single-leg balance, wobble board
Brace: Discontinue by 6 weeks if asymptomatic
Strengthening: Progress to sport-specific drills
Running: Linear running at 6 weeks if full ROM and strength
Return to sport: 8-12 weeks for non-pivoting, 12-16 weeks for pivoting
Hinged bracing does NOT need to lock the knee in extension full-time. Allowing protected early ROM (0-90 degrees) prevents arthrofibrosis and is the modern standard for grade I-II sMCL injury. The sMCL heals by secondary intention and benefits from controlled motion to align collagen fibres.
The everyday combined injury — an ACL tear with a grade III sMCL/PMC tear (distinct from the gross knee-dislocation pattern) — has a characteristic staged approach that examiners look for. Because the medial side heals well, the usual sequence is to treat the MCL first in a hinged brace, regain full range of motion, and let the medial side heal, then reconstruct the ACL at around 6 weeks once the knee is supple. Reconstructing the ACL acutely alongside a healing medial side risks arthrofibrosis and stiffness, and many grade III MCLs that are clinically stable at 6 weeks need no medial surgery at all. The exceptions that justify acute medial repair/reconstruction at the time of ACL surgery are: persistent gross valgus laxity after a brace trial, a distal/displaced (Stener-like) tear, a large bony avulsion, valgus opening in full extension, or a true multi-ligament/dislocation pattern. The principle: restore the central pivot (ACL) but let a healing medial side declare itself first.
BARSTreatment by Injury Pattern
Hook:BARS - the four treatment principles for PMC injury based on grade and timing!
Complications
- Incidence
- 10-20 percent after repair
- Risk Factors
- Chronic injury, poor tissue quality, missed POL
- Management
- Bracing trial, revision reconstruction
- Incidence
- 10-15 percent after isolated sMCL repair
- Risk Factors
- Untreated POL injury, missed associated cruciate
- Management
- POL reconstruction, address cruciate if missed
- Incidence
- 15-25 percent after multi-ligament surgery
- Risk Factors
- Prolonged immobilisation, combined procedures
- Management
- MUA, arthroscopic release, aggressive rehab
- Incidence
- Rare in isolated PMC, more in dislocation
- Risk Factors
- High-energy mechanism, missed vascular injury
- Management
- CT angiogram, vascular surgery consult
- Incidence
- Less than 5 percent
- Risk Factors
- Multi-ligament injury, varus component
- Management
- Ankle-foot orthosis, nerve recovery 3-6 months
- Incidence
- 5-10 percent with medial approach
- Risk Factors
- Direct injury or traction during exposure
- Management
- Neuropathic pain management, neuroma excision
- Incidence
- 5-10 percent after reconstruction
- Risk Factors
- Early return to sport, poor tunnel placement
- Management
- Revision reconstruction, prolonged rehab
Any knee with PMC plus another ligament injury, or any high-energy mechanism, requires formal vascular assessment. Ankle-brachial index under 0.9, expanding haematoma, absent pulses, or limb ischaemia mandates immediate CT angiogram and vascular surgery consultation. A missed popliteal artery injury can cost the limb.
Outcomes and Prognosis
- Indication
- Isolated low-grade sMCL
- Expected Outcome
- Over 95 percent return to sport at 3 months
- Long-term Function
- Excellent, no residual laxity
- Indication
- Low-demand patient, no multi-ligament
- Expected Outcome
- 80-90 percent stable, mild residual laxity common
- Long-term Function
- Good for ADL, may struggle with pivoting sport
- Indication
- Bony avulsion, midsubstance tear, athlete
- Expected Outcome
- 85-95 percent good-to-excellent
- Long-term Function
- Best long-term stability, fastest return
- Indication
- Failed bracing, chronic AMRI, high demand
- Expected Outcome
- 80-90 percent good-to-excellent
- Long-term Function
- Good stability, slower return, graft donor morbidity
- Indication
- Multi-ligament knee
- Expected Outcome
- 75-90 percent good-to-excellent
- Long-term Function
- Good, but stiffness and residual laxity common
Best prognosis: Acute presentation under 3 weeks, isolated injury, no associated cruciate, compliant patient, hamstring autograft or primary repair.
Poor prognosis: Chronic injury over 6 weeks, multi-ligament pattern, knee dislocation, severe chondral damage seen at arthroscopy, prior surgery, smoker, diabetic, obese.
Key threshold: 3 weeks from injury - outcomes decline significantly after this window because the sMCL and POL retract and become difficult to mobilise for primary repair.
Guidelines, Registries & Global Practice
- Isolated grade III sMCL tears are uncommon as surgical cases - the majority of MCL injuries worldwide are low-grade and managed non-operatively
- PMC plus cruciate injuries dominate operative practice, especially in high-energy sport and road traffic collisions
- High-volume centres report multi-ligament knee injuries at 0.02 to 0.2 percent of all orthopaedic trauma admissions globally
- Male predominance in the third and fourth decades, reflecting contact sport and motor vehicle exposure
- High-resource: dedicated knee ligament surgeons, anatomic reconstruction techniques, allograft availability, structured multi-ligament rehabilitation pathways
- Limited-resource: bracing-first approach for most PMC injuries, primary repair of avulsions where feasible, delayed reconstruction reserved for high-demand patients
- Universal principle: the sMCL heals well with non-operative care in isolated injuries; the surgical decision is driven by multi-ligament involvement and patient demand
- Rehabilitation access: outcomes depend on supervised physiotherapy, which is unevenly available across regions
- Diagnosis emphasis
- Lachman, pivot shift, valgus stress, MRI
- Isolated MCL
- Brace and rehab for grade I-II, repair for grade III in athletes
- Multi-ligament PMC
- Single-stage reconstruction of all injured ligaments
- Diagnosis emphasis
- MRI-based classification, anatomic reconstruction
- Isolated MCL
- Functional bracing, structured rehab
- Multi-ligament PMC
- Anatomic sMCL and POL reconstruction, anatomic tunnels
- Diagnosis emphasis
- Clinical examination, MRI, vascular assessment in dislocation
- Isolated MCL
- Brace and rehab as first line for isolated injuries
- Multi-ligament PMC
- Multi-ligament reconstruction in specialist centres
- Diagnosis emphasis
- Multiligament knee classification, treatment algorithm
- Isolated MCL
- Brace-led for isolated low-grade, repair for avulsion
- Multi-ligament PMC
- Single or staged multi-ligament reconstruction, anatomic principles
There is no dedicated PMC injury registry. Multi-ligament knee registries exist in some regions (including the UK and the US) and provide the best population-level data on outcomes, but PMC-specific outcome data is largely from case series and systematic reviews. Surgical decision-making is therefore guided by anatomic and biomechanical principles (LaPrade, Sims, Hughston) and the patient's functional demand.
Record in every PMC injury:
- Valgus opening in millimetres at 0 and 30 degrees
- Anterior drawer in external rotation (side-to-side comparison)
- Lachman, posterior drawer, pivot shift, dial test (to exclude multi-ligament)
- Vascular examination: pulses, capillary refill, ankle-brachial index
- Peroneal nerve and saphenous nerve function
- MRI findings for sMCL, dMCL, POL, semimembranosus, and cruciates
A missed popliteal artery injury is the most catastrophic complication of multi-ligament knee injury. Always document vascular status before and after any reduction.
Controversies & Areas of Uncertainty
Modern series suggest that bracing can restore valgus stability in 80-90 percent of isolated grade III sMCL injuries, with return to sport comparable to surgical repair in non-elite patients. Acute repair is favoured for elite pivoting athletes, but the evidence for universal operative treatment is weak.
Anatomic reconstruction (LaPrade) restores the sMCL to its native femoral and tibial footprints and gives reliable valgus stability. Isometric reconstruction places the femoral tunnel slightly anterior to the anatomic centre to reduce graft length change through range of motion. The two techniques have not been directly compared in a randomised trial.
The original Lind and LaPrade techniques used a single hamstring graft with sMCL and POL limbs. Some surgeons add an internal brace or suture tape augmentation. There is no high-quality trial showing that one construct is superior for AMRI control.
Most surgeons operate within 3 weeks of injury to allow primary repair and to avoid the stiff, fibrotic knee of delayed surgery. Some recent series report acceptable outcomes with delayed (3-6 weeks) reconstruction after initial spanning external fixation. The optimal window remains debated.
MCQ Practice Points
Q: Name the four core static stabilisers of the posteromedial corner. A: Superficial MCL (sMCL), deep MCL (dMCL), posterior oblique ligament (POL), and posteromedial capsule, with the semimembranosus expansion acting as the dynamic stabiliser. The sMCL is the primary restraint to valgus at 30 degrees flexion, while the POL is the primary restraint to internal rotation of the tibia.
Q: What examination finding confirms anteromedial rotatory instability (AMRI)? A: The Slocum test (or Hughston anterior drawer in external rotation). With the knee flexed to 90 degrees and the foot fixed in 15 degrees of external rotation, the tibia is allowed to rotate back into neutral. The lateral tibial plateau reduces from an anteriorly subluxed position - this reduction is pathognomonic for AMRI from PMC deficiency.
Q: A patient has valgus opening at 0 degrees (full extension). What does this tell you? A: It is not isolated sMCL injury. Valgus opening in full extension implies the PMC plus the cruciate ligaments (typically ACL) are both injured, because the cruciates and posterior capsule act as secondary valgus restraints in extension. Always examine the ACL, PCL, and posterolateral corner when there is medial opening in full extension.
Q: What is the optimal management of an isolated grade II sMCL injury? A: Hinged knee brace for 4-6 weeks with early protected range of motion. The sMCL has excellent healing potential. Weight-bearing as tolerated, progressive ROM, and a structured rehabilitation programme. Return to sport at 8-12 weeks for non-pivoting activities and 12-16 weeks for pivoting. Surgery is rarely required.
Q: What is the optimal window for acute primary repair of the PMC? A: Within 3 weeks of injury. After this window, the sMCL and POL retract, become scarred, and the tissue quality is too poor for primary repair - staged or chronic reconstruction with autograft or allograft is then required. Outcomes after acute repair are consistently superior to outcomes after delayed reconstruction.
Q: A chronic PMC deficiency with AMRI is being reconstructed. What two structures must be addressed? A: The sMCL and the POL. The sMCL limb controls valgus; a separate POL limb (often a second limb of the same hamstring graft) controls internal rotation and AMRI. Reconstructing the sMCL alone leaves residual AMRI - this is the most common technical error in PMC reconstruction.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old professional footballer presents 2 days after a valgus injury to his right knee during a tackle. On examination, he has medial pain, 8 mm of valgus opening at 30 degrees with a soft endpoint, and a positive anterior drawer in external rotation. Lachman and pivot shift are normal. MRI shows isolated sMCL rupture with periligamentous oedema and oedema at the POL insertion. How would you manage this?”
“A 35-year-old motorcyclist presents 5 days after a high-speed collision. He has gross medial laxity with valgus opening at 0 and 30 degrees, increased external rotation at 30 and 90 degrees, a 3+ Lachman, and a positive posterior drawer. CT angiogram is normal. MRI confirms complete sMCL and POL rupture, ACL rupture, and a high-grade partial PCL injury. How do you stage and perform the surgery?”
Key Anatomy
- sMCL = primary valgus restraint at 30 deg, inserts 5-7 cm below joint line on tibia
- POL = primary restraint to internal rotation, arises from adductor tubercle
- Semimembranosus = dynamic PMC stabiliser, 5-6 insertional arms onto POL and capsule
- Deep MCL = capsular thickening, attaches to meniscus (secondary restraint)
Diagnosis
- Valgus stress at 30 deg grades sMCL injury (0 mm = grade 0, 3-5 mm = I, 5-10 mm = II, greater than 10 mm = III)
- Valgus opening at 0 deg = PMC plus cruciate injury, not isolated sMCL
- Anterior drawer in external rotation (Hughston) and Slocum test detect AMRI
- Always examine ACL, PCL, meniscus, LCL - 70 percent of PMC injuries are multi-ligament
Imaging
- MRI with corner-specific sequences is the gold standard for surgical planning
- Coronal views for sMCL, axial for POL and semimembranosus
- CT angiogram or ankle-brachial index mandatory in any multi-ligament knee
- Pellegrini-Stieda ossification on plain film = chronic sMCL injury
Treatment Algorithm
- Isolated grade I-II = hinged brace 4-6 weeks with protected early ROM
- Isolated grade III = brace trial in low-demand patients, repair in athletes under 3 weeks
- PMC plus cruciate = single-stage multi-ligament reconstruction within 3 weeks
- Chronic PMC deficiency = anatomic sMCL plus POL reconstruction, autograft or allograft
Complications
- Residual valgus laxity 10-20 percent, persistent AMRI if POL not addressed
- Stiffness / arthrofibrosis 15-25 percent after multi-ligament reconstruction
- Popliteal artery injury is the most catastrophic - always obtain vascular studies
- Peroneal and saphenous nerve injury with medial approach (5-10 percent)
Evidence Base and Key Trials
Classification of knee ligament instabilities. Part I. The medial compartment and cruciate ligaments
- Original description of anteromedial rotatory instability (AMRI) and its link to the medial and posteromedial structures
- Established the importance of the posterior oblique ligament as a distinct restraint to internal rotation
- Anterior drawer in external rotation (the Hughston test) introduced as the bedside test for AMRI
- Anatomic and biomechanical basis for treating AMRI by addressing the PMC plus cruciate as a unit
The anatomy of the medial part of the knee
- Quantitative anatomic study of the sMCL, POL, and posteromedial capsule in cadaveric knees
- sMCL femoral insertion 3.2 mm proximal and 4.8 mm posterior to the medial epicondyle
- sMCL tibial insertion 6 cm distal to the joint line, on the posteromedial tibia
- POL origin at the adductor tubercle, blending with the posteromedial capsule and semimembranosus expansion
The posteromedial corner of the knee: medial-sided injury patterns revisited
- Review of the three medial structures: sMCL, dMCL (middle third capsular ligament), and POL
- POL and semimembranosus expansion are the prime restraints to internal rotation, not the sMCL
- Failure to address the POL at the time of sMCL repair is a common cause of residual AMRI
- Combined sMCL plus POL reconstruction gives superior rotational stability to sMCL alone
Surgical treatment of acute medial collateral ligament and posteromedial corner injuries of the knee
- Acute grade III PMC injuries treated with primary repair of the sMCL, POL, and semimembranosus expansion
- Cruciate reconstruction (ACL, PCL) performed in the same sitting for multi-ligament knees
- Mean side-to-side medial opening on valgus stress restored to within 2 mm of the contralateral knee
- Over 80 percent of multi-ligament patients returned to pre-injury activity level
Surgical techniques for the reconstruction of medial collateral ligament and posteromedial corner injuries of the knee: a systematic review
- Systematic review of PMC reconstruction techniques in chronic and multi-ligament settings
- Anatomic sMCL reconstruction restores valgus stability but does not consistently control AMRI
- Adding a dedicated POL reconstruction limb reduces residual internal rotation and AMRI
- No consensus on the ideal graft choice (hamstring autograft, tibialis anterior or peroneus allograft)