Scoliosis, Hip Dysplasia & Perioperative Risk
- PRADER-WILLI SYNDROME is a genetic IMPRINTING disorder caused by loss of the PATERNALLY expressed genes at chromosome 15q11-q13 (paternal microdeletion, maternal uniparental disomy, or an imprinting defect), producing neonatal HYPOTONIA and feeding difficulty that evolve into childhood HYPERPHAGIA and OBESITY, with short stature, hypogonadism, developmental delay and behavioural problems.
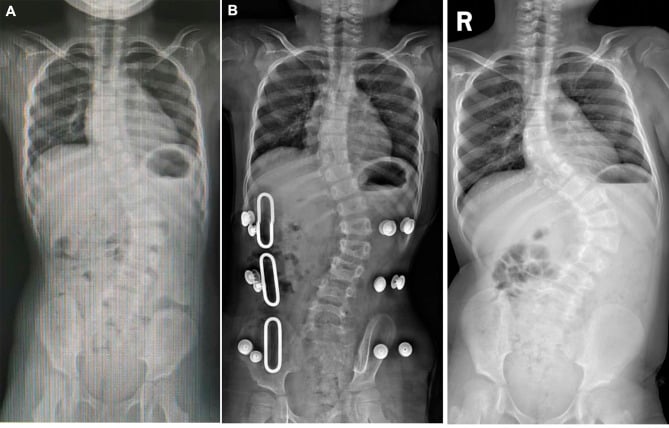
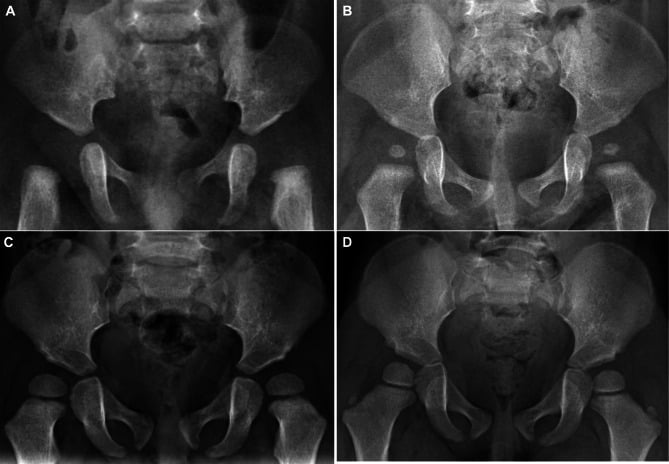
- The two principal ORTHOPAEDIC manifestations are SCOLIOSIS and DEVELOPMENTAL HIP DYSPLASIA, both attributed largely to the underlying HYPOTONIA. In the largest paediatric series (n = 175) scoliosis was present in 43.7% - 78.8% of it MILD, 15.2% moderate, only 6.1% severe - and hip dysplasia in 38.2%. Both are common enough to be actively sought in every child with PWS, but most of the scoliosis found is mild.
- SCOLIOSIS in PWS is variable, presents early (median onset 4.5 years, with prevalence rising sharply at age 5 and again in adolescence) and the mean Cobb angle increases with age - so surveillance must start in the preschool years, not at the usual adolescent screening age. GROWTH HORMONE is widely used in PWS for body composition and stature; consensus is to MONITOR the spine during rhGH rather than reflexively withhold it, but be clear that no trial has shown rhGH causes or accelerates curve progression - the caution is precautionary, not evidence of harm.
- DEVELOPMENTAL HIP DYSPLASIA is common (median detection around 1.8 years) and related to hypotonia; it is screened for and managed along standard DDH lines. Two findings temper how aggressively it is treated: in the largest series only 12.7% of affected children received any orthopaedic treatment, and the mean acetabular index DECREASED (improved) with age across the cohort - which is descriptive, not a licence to observe, but does mean the published PWS hip data describe a largely untreated population.
- KNOW WHAT DOES NOT PREDICT DEFORMITY. In that series, sex, genotype (paternal deletion vs maternal uniparental disomy), BMI and obesity rate showed NO significant association with either scoliosis or hip dysplasia, or with their age of onset. A lean child with PWS is not protected, and a deletion genotype does not warrant different surveillance - every child is screened on the same schedule.
- PERIOPERATIVE RISK is a central orthopaedic concern: OBESITY, obstructive SLEEP APNOEA, hypotonia (and respiratory muscle weakness), altered temperature regulation and pain perception, and behavioural difficulties all increase ANAESTHETIC and respiratory risk - so any surgery, especially scoliosis correction, needs careful multidisciplinary perioperative planning.
- MANAGEMENT is EARLY DIAGNOSIS and SURVEILLANCE within a multidisciplinary team: monitor the SPINE (clinical/radiographic, especially during growth and rhGH therapy) and the HIPS, treat scoliosis on its merits (bracing/surgery for progression, with the perioperative caveats) and DDH along standard lines, and optimise the systemic issues (weight, OSA) before any operation.
- “Prader-Willi = imprinting disorder (loss of PATERNAL 15q11-q13); hypotonia -> hyperphagia/obesity, short stature, hypogonadism, developmental delay.
- “Miao n = 175: scoliosis 43.7% (78.8% mild) median onset 4.5 yrs; hip dysplasia 38.2% median onset 1.8 yrs. Sex, genotype, BMI and obesity predicted NEITHER. Only ~1 in 8 affected children were treated.
- “MONITOR the spine during rhGH rather than withholding it - but know that no trial shows rhGH accelerates curves; the caution is precautionary. PERIOPERATIVE risk = obesity + OSA + hypotonia (anaesthetic/respiratory) - plan carefully, especially for spine surgery. PWS is NOT associated with malignant hyperthermia.
Scoliosis 43.7% (78.8% mild, median onset 4.5 years) and hip dysplasia 38.2% (median 1.8 years), both attributed to hypotonia. Screen from the preschool years, not at adolescence.
Obesity + obstructive sleep apnoea + hypotonia (+ altered temperature/pain) raise anaesthetic and respiratory risk - optimise and plan carefully, especially for scoliosis surgery.
Orthopaedic Manifestations & Perioperative Care
Prader-Willi syndrome is an imprinting disorder (loss of paternal 15q11-q13) with hypotonia, hyperphagia/obesity, short stature and developmental delay. Its orthopaedic footprint is scoliosis (common, often mild, presenting from early childhood and progressing with growth) and developmental hip dysplasia (common), both driven by hypotonia. Scoliosis management interacts with growth-hormone therapy, so the spine is monitored during rhGH rather than treatment withheld reflexively. The major surgical concern is perioperative risk - obesity, obstructive sleep apnoea, hypotonia/respiratory weakness, altered temperature/pain responses and behavioural issues - which must be optimised and planned for, especially before scoliosis correction.
- Surveillance: monitor the spine (clinically/radiographically, especially during growth and rhGH) and the hips (DDH screening/management).
- Scoliosis: treat on its merits (observation/bracing/surgery for progression) - monitor, don't reflexively stop rhGH.
- DDH: manage along standard lines, with awareness of the syndrome.
- Perioperative: optimise weight and OSA, plan anaesthesia/respiratory care; multidisciplinary (endocrine, respiratory, anaesthesia) involvement for any operation.
For the orthopaedic surgeon, the two messages in Prader-Willi syndrome are that the spine and hips need active surveillance, and that the perioperative period is genuinely high-risk. Scoliosis and developmental hip dysplasia are both common and are driven by the underlying hypotonia, so they should be actively sought and monitored, particularly during growth spurts and growth-hormone therapy; the interaction between rhGH and scoliosis means the spine should be monitored during treatment rather than rhGH being reflexively withheld. When surgery is required - especially scoliosis correction - obesity, obstructive sleep apnoea, hypotonia with respiratory muscle weakness, and altered temperature and pain responses combine to raise anaesthetic and respiratory risk, and behavioural issues can complicate care; so weight and OSA should be optimised preoperatively and the operation planned with endocrinology, respiratory medicine and anaesthesia in a multidisciplinary team, with close postoperative respiratory monitoring.
The Genetics: Imprinting, the Three Mechanisms, and Angelman
- Genomic imprinting. Some genes are expressed from only ONE parental allele because the other is epigenetically silenced (methylated) according to its parent of origin. At 15q11-q13 a cluster (including SNRPN and the SNORD116 snoRNA cluster) is normally expressed only from the paternal allele; losing that paternal expression causes PWS.
- Three mechanisms. (1) Paternal 15q11-q13 deletion (~65-75%); (2) maternal uniparental disomy - both chromosome 15s inherited from the mother (~20-30%); (3) an imprinting-centre defect (~1-3%); rarely a paternal translocation.
- The Angelman contrast. The SAME 15q11-q13 region, but loss of the maternally expressed gene (UBE3A) causes Angelman syndrome (maternal deletion / paternal uniparental disomy / UBE3A mutation) - an entirely different phenotype (severe intellectual disability, ataxia, seizures, a happy demeanour). Parent-of-origin decides which syndrome results.
- Diagnosis. DNA methylation analysis of 15q11-q13 is the first-line test - it detects all three mechanisms (an abnormal methylation pattern); FISH/microarray (deletion) and microsatellite/uniparental-disomy studies then define the specific mechanism, which matters for recurrence-risk counselling.
Q: What is the genetic basis of Prader-Willi syndrome, and how does it differ from Angelman syndrome?
A: PWS is a disorder of genomic imprinting: the 15q11-q13 cluster (SNRPN/SNORD116) is normally expressed only from the paternal allele, and loss of that paternal expression causes PWS - by paternal deletion (~65-75%), maternal uniparental disomy (~20-30%), or an imprinting-centre defect (~1-3%). The same region, but loss of the maternally expressed UBE3A, causes Angelman syndrome - parent-of-origin determines the phenotype. First-line diagnosis is DNA methylation analysis (detects all three mechanisms); FISH/microarray and UPD studies then define the mechanism for counselling.
Anaesthetic Considerations (Including the Malignant-Hyperthermia Myth)
- Airway and respiration. Obesity plus OSA plus hypotonia with weak respiratory muscles and a blunted ventilatory response to hypoxia/hypercapnia (plus thick secretions) give a difficult airway and a high risk of postoperative hypoventilation and respiratory failure - so a preoperative sleep study is valuable and extended postoperative respiratory monitoring is required.
- Thermoregulation - NOT malignant hyperthermia. Hypothalamic dysfunction causes altered thermoregulation and intraoperative temperature instability (hyper- or hypothermia), so temperature must be monitored - but, despite the hypotonia, PWS is NOT associated with malignant hyperthermia, and volatile agents/succinylcholine are not contraindicated on MH grounds. This misconception is a common exam trap.
- rhGH and the airway. Before starting recombinant growth hormone, a sleep study / ENT assessment is recommended: rhGH can worsen OSA (adenotonsillar/lymphoid tissue) early in treatment and has been linked with sudden death in children with severe respiratory compromise - so respiratory status is optimised first, and the airway is co-monitored alongside the spine.
- Other. Delayed gastric emptying and hyperphagia raise aspiration risk; pain may be under-reported (altered perception); there is heightened sensitivity to sedatives; and obesity makes IV access and positioning difficult.
Q: What are the key anaesthetic considerations in Prader-Willi syndrome?
A: Obesity, OSA and hypotonia with weak respiratory muscles and a blunted ventilatory drive give a difficult airway and a high risk of postoperative respiratory failure - so a preoperative sleep study and extended postoperative respiratory monitoring are needed. Hypothalamic dysfunction causes altered thermoregulation (monitor temperature), but PWS is NOT associated with malignant hyperthermia despite the hypotonia. Watch for aspiration (delayed gastric emptying/hyperphagia), altered pain reporting, high sedative sensitivity and difficult access; and remember rhGH can worsen OSA, so respiratory status is assessed before starting it.
Mnemonics & Memory Aids
PWS
Hook:PWS: Paternal 15q loss/hyPotonia, Weight+OSA (anaesthetic risk), Scoliosis + hip dysplasia (Surveil, monitor spine on rhGH).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What are the orthopaedic issues in a child with Prader-Willi syndrome, and what would you be cautious about before operating?”
What it is
- Imprinting disorder: loss of paternal genes at 15q11-q13
- Neonatal hypotonia -> hyperphagia/obesity, short stature, hypogonadism, developmental delay
- Hypotonia drives the orthopaedic deformities
Orthopaedic manifestations
- Scoliosis 43.7% - 78.8% mild, 15.2% moderate, 6.1% severe; median onset 4.5 yrs, rising at 5 and in adolescence
- Developmental hip dysplasia 38.2%; median onset 1.8 yrs; acetabular index improved with age
- Sex, genotype, BMI, obesity: NO association with either deformity or its onset
- Only 10.6% / 12.7% received treatment - the published data are largely untreated natural history
- Monitor the spine during rhGH; no trial shows rhGH accelerates curves
Perioperative risk
- Obesity + obstructive sleep apnoea + hypotonia/respiratory weakness
- Altered temperature regulation and pain perception; behavioural issues
- Optimise weight/OSA; multidisciplinary planning; close postoperative respiratory monitoring
Evidence & Key Studies
Orthopedic manifestations in children with Prader-Willi syndrome
- Retrospective single-centre review of 175 children with PWS at a Chinese tertiary children's hospital (Zhejiang), to March 2023. Scoliosis in 66 (43.7%) and hip dysplasia in 47 (38.2%) - note the percentages are calculated on the subsets who had the relevant imaging (roughly 151 and 123 respectively), not on all 175, so they are prevalence among those investigated.
- Scoliosis severity: 52 mild (78.8%), 10 moderate (15.2%), 4 severe (6.1%). Median age at scoliosis 4.5 years, prevalence rising sharply at age 5 and again in adolescence, mean Cobb angle increasing with age. Median age at hip dysplasia 1.8 years, and mean acetabular index DECREASED with age.
- Treatment uptake was strikingly low: only 7 of 66 scoliosis patients (10.6%) and 6 of 47 with hip dysplasia (12.7%) received any orthopaedic treatment - so this cohort describes the largely UNTREATED natural history, not the results of management.
- NEGATIVE findings that matter: no significant difference in sex, genotype (deletion vs uniparental disomy), BMI, or obesity rate in relation to scoliosis or hip dysplasia, or to their age of onset. Obesity and genotype did not predict who developed a deformity.
- Limitations: single centre, retrospective, cross-sectional; no follow-up duration and NO outcome data, so the authors' closing statement that early diagnosis and treatment matter for prognosis is a recommendation, not a result of this study.
The prevalences (scoliosis 43.7%, 78.8% of it mild; hip dysplasia 38.2%), the median onset ages (4.5 and 1.8 years), the Cobb-angle and acetabular-index trends with age, the low treatment uptake (10.6% and 12.7%) and the negative associations with sex, genotype, BMI and obesity all come from the Miao series (DOI) - a single-centre Chinese retrospective study with no follow-up or outcome data. The imprinting genetics (loss of paternal 15q11-q13), the role of hypotonia, and the perioperative risks (obesity, OSA, hypotonia, and the absence of a malignant-hyperthermia association) are standard, well-established teaching.
Be precise about growth hormone. Miao reported only that the prevalence of hip dysplasia among children treated with rhGH was low; that study did not test whether rhGH causes, accelerates or protects against scoliosis. The recommendation to monitor the spine during rhGH rather than withhold it is consensus practice, not a finding of this cohort, and no randomised trial has established a causal effect of rhGH on curve progression in PWS. No validated PWS-specific curve-progression risk score, bracing threshold or surveillance interval has been published; the age-targeted screening described here is extrapolated from the onset ages above.