SOX9 Bowing Dysplasia
- CAMPOMELIC (camptomelic) DYSPLASIA is a rare, frequently LETHAL skeletal dysplasia caused by mutation or disruption of SOX9 (autosomal dominant, usually arising de novo); it is one of the recognised skeletal dysplasias of the fetus/infant, and the name means 'bent limb'.
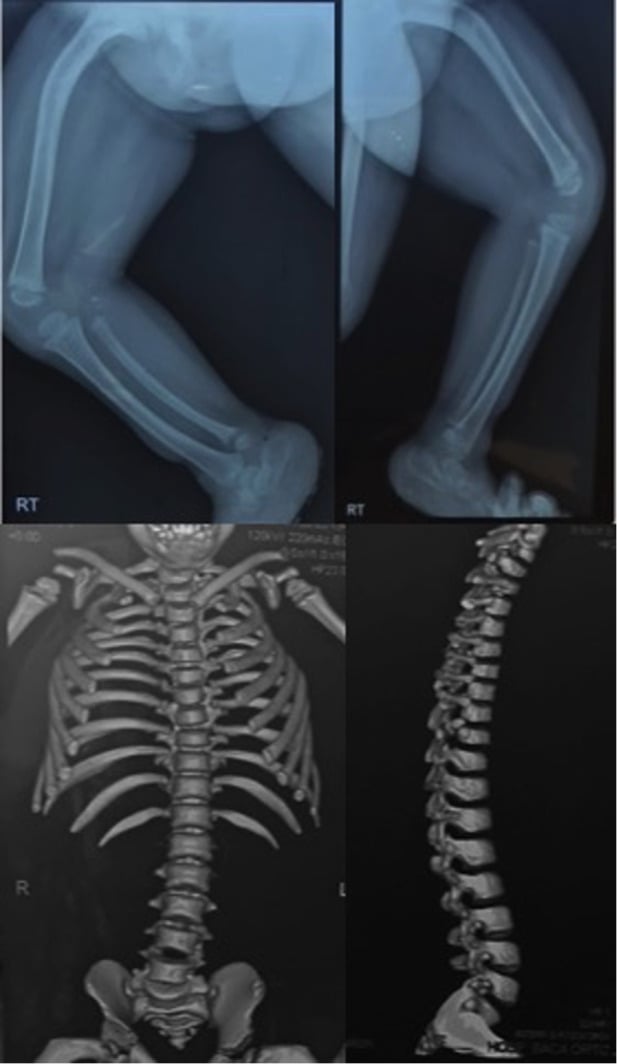
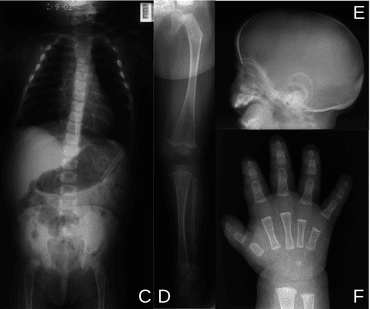
- The SKELETAL HALLMARK is congenital BOWING (camptomelia) of the long bones - characteristically ANTERIOR bowing of the TIBIA (and the femur), often with a SKIN DIMPLE overlying the apex of the bow - together with hypoplastic scapulae, a reduced number of rib pairs, scoliosis, clubfeet and a small/narrow thorax.
- The principal cause of the HIGH MORTALITY is RESPIRATORY COMPROMISE: the small thorax and, importantly, LARYNGOTRACHEOMALACIA (softening of the airway cartilage from the SOX9 chondrogenesis defect) cause airway collapse and restrictive/obstructive respiratory failure, often fatal in the neonatal period - though some milder/longer-surviving cases exist.
- A characteristic NON-skeletal feature is SEX REVERSAL: SOX9 is essential for testis determination, so a large proportion of karyotypically XY (46,XY) individuals have FEMALE or ambiguous external genitalia (XY sex reversal) - a key clue linking the skeletal phenotype to the SOX9 gene.
- OTHER associated anomalies include cleft palate, Pierre Robin sequence (micrognathia/glossoptosis), and cardiac/renal anomalies; the diagnosis is by the clinical/radiographic phenotype (bowed long bones, hypoplastic scapulae) with SOX9 genetic confirmation and karyotype.
- MANAGEMENT is largely SUPPORTIVE/PALLIATIVE given the high mortality from respiratory failure: neonatal RESPIRATORY support (airway management for laryngotracheomalacia), and for survivors, ORTHOPAEDIC management of the limb bowing, scoliosis and foot deformity, plus management of the sex-reversal/endocrine and other anomalies - within a multidisciplinary team with genetic counselling.
- “Camptomelic dysplasia = rare, often LETHAL SOX9 skeletal dysplasia (usually de novo). Hallmark = congenital BOWING (camptomelia) of long bones - ANTERIOR tibial bow + skin DIMPLE at the apex.
- “High mortality from RESPIRATORY compromise: small thorax + LARYNGOTRACHEOMALACIA (airway cartilage softening).
- “SOX9 = testis determination -> XY SEX REVERSAL (46,XY females/ambiguous genitalia). Also hypoplastic scapulae, scoliosis, clubfeet, cleft palate/Pierre Robin. Management largely supportive/palliative; orthopaedic care for survivors.
Congenital bowing of the long bones (anterior tibial bow + skin dimple), hypoplastic scapulae, small thorax = camptomelic dysplasia (SOX9). Look for XY sex reversal.
Respiratory compromise from the small thorax + laryngotracheomalacia drives the high neonatal mortality. Care is largely supportive/palliative.
Prenatal (Antenatal) Diagnosis
The most severe and lethal skeletal dysplasias are identifiable before birth, and an increasing proportion are confirmed by genetic testing antenatally - so the diagnosis is often first suspected on a scan rather than in the delivery room.
- Antenatal ultrasound features. Shortened and bowed long bones (especially the femora and tibiae), a narrow/small thorax with a reduced chest circumference (predicting the lethal pulmonary hypoplasia that drives mortality), hypoplastic or absent scapulae, and sometimes micrognathia/cleft palate. The bowing plus a small thorax is the key pattern.
- A powerful clue. Discordance between a 46,XY karyotype and female-appearing genitalia on antenatal assessment strongly suggests the SOX9 diagnosis rather than another lethal dysplasia.
- Confirmation. Definitive prenatal diagnosis is molecular - SOX9 sequencing and karyotype on chorionic villus sampling or amniocentesis - particularly where there is a suggestive scan or a family history.
- Why it matters. Recognising a lethal phenotype prenatally allows honest counselling, the option of termination, and planning of delivery and neonatal care (a palliative pathway versus active airway/respiratory support). The differential on antenatal ultrasound includes other lethal dysplasias such as thanatophoric dysplasia and osteogenesis imperfecta type II.
Q: What are the antenatal ultrasound features of campomelic dysplasia?
A: Shortened and bowed long bones (especially femora and tibiae), a narrow/small thorax (predicting lethal pulmonary hypoplasia), hypoplastic or absent scapulae, and sometimes micrognathia/cleft palate. A 46,XY karyotype with female-appearing genitalia is a strong clue. Definitive diagnosis is molecular - SOX9 testing and karyotype on CVS/amniocentesis - and recognising the lethal phenotype allows counselling, the option of termination, and neonatal/delivery planning.
Two Practical Points: the Airway and the Apparently Healthy Parent
Calling the airway problem "laryngotracheomalacia" suggests a single lesion to bypass. In practice many patients have airway obstruction at several levels at once - the SOX9 cartilage defect affects the larynx and trachea together, and the associated micrognathia and glossoptosis of a Pierre Robin sequence add obstruction above them. That is why intubation or a tracheostomy may relieve one level and leave the child still obstructed, and why airway assessment should be by someone who will examine the whole airway rather than treat the first abnormality found. The condition is described as historically lethal, and survival beyond infancy is now reported, so airway planning is not futile.
Most cases are de novo and recurrence risk is usually quoted as low - but germline mosaicism makes it not zero, and there is a molecularly confirmed instance of maternal germinal mosaicism producing two affected siblings. The practical detail is what made it detectable: radiographs of the apparently healthy mother showed mild skeletal changes, and somatic mosaicism was then confirmed. So before counselling a couple that recurrence risk is negligible, examine both parents clinically and image them - a superficially healthy parent can carry the mutation in mosaic form.
The name is misleading in a minority of cases. An acampomelic (straight-bone) variant is well described, in which the femur, tibia and fibula are not bowed and the diagnosis rests on the rest of the phenotype - hypoplastic scapulae, 11 pairs of ribs, scoliosis with undermineralised thoracic pedicles, short ischia, delayed femoral epiphyseal ossification and a cranial vault large relative to the face. It is more often associated with the upstream regulatory rearrangements than with intragenic SOX9 mutations, and tends to be the milder end of the spectrum. Absence of bowing therefore does not exclude the diagnosis, and a neonate with hypoplastic scapulae and a small thorax deserves SOX9 testing even with straight long bones.
No reliable survival figure for this condition was retrievable, and quoting one would be invented - describe it as historically lethal with death usually from respiratory failure in the neonatal period, while noting that survival into childhood and beyond is reported and that airway obstruction is multi-level. Recurrence is usually low but not zero: image the parents before saying otherwise.
Features & Management
Camptomelic dysplasia is a rare, often lethal skeletal dysplasia from SOX9 mutation (usually de novo). Its hallmark is congenital bowing (camptomelia) of the long bones - characteristically anterior tibial bowing with an overlying skin dimple - plus hypoplastic scapulae, scoliosis, clubfeet and a small/narrow thorax. The high mortality is driven by respiratory compromise from the small thorax and laryngotracheomalacia. Because SOX9 determines testis development, many 46,XY individuals show female/ambiguous genitalia (sex reversal). Other features include cleft palate and Pierre Robin sequence. Management is largely supportive/ palliative (neonatal respiratory/airway support), with orthopaedic care of bowing/scoliosis/feet for survivors, plus endocrine and genetic input.
Two features dominate camptomelic dysplasia clinically. First, the cause of its high mortality is respiratory: the small thorax combined with laryngotracheomalacia - a softening of the airway cartilage that follows directly from the SOX9 chondrogenesis defect - leads to airway collapse and respiratory failure that is frequently fatal in the neonatal period, so neonatal airway and respiratory support is the immediate priority, and the prognosis must be discussed honestly with the family. Second, because SOX9 is essential for testis determination, a large proportion of karyotypically XY infants have female or ambiguous external genitalia (XY sex reversal), so the apparent sex may not match the karyotype - an important point for diagnosis and family counselling. The skeletal hallmark of anterior tibial bowing with a skin dimple, together with hypoplastic scapulae, points to the diagnosis, which is confirmed by SOX9 testing and karyotype. For the minority who survive, orthopaedic management addresses the limb bowing, scoliosis and foot deformity within multidisciplinary care.
The SOX9 Gene: Locus and Mechanism
- The gene. SOX9 (an SRY-box transcription factor) maps to chromosome 17q24.3. It is a master regulator of two processes that explain the whole phenotype: chondrogenesis (cartilage/skeletal and airway development - hence the bowing, small thorax and laryngotracheomalacia) and testis determination (hence the XY sex reversal).
- Two molecular mechanisms. Campomelic dysplasia results from heterozygous loss of SOX9 function by either route:
- Intragenic mutations - point or truncating mutations WITHIN the SOX9 coding region (the majority of cases, usually arising de novo, autosomal dominant).
- Chromosomal rearrangements upstream of SOX9 - translocations, inversions or deletions in the large regulatory region up to about 1 Mb upstream that separate SOX9 from its distant tissue-specific enhancers (a position effect / cis-regulatory disruption). These extragenic rearrangements are more often associated with the milder or acampomelic (straight-bone) phenotypes.
- Inheritance and counselling. Most cases are de novo (low recurrence risk), but germline mosaicism in an apparently unaffected parent means the recurrence risk is not zero - there is a molecularly confirmed family in which maternal germinal mosaicism produced two affected siblings, and the mother's mosaicism was only suspected because radiographs showed mild skeletal changes. Examine and image both parents before quoting a negligible recurrence risk.
Q: What gene causes campomelic dysplasia, where is it, and how does the mutation act?
A: SOX9 (an SRY-box transcription factor) on chromosome 17q24.3. Campomelic dysplasia is caused by heterozygous loss of SOX9 function - either intragenic point/truncating mutations within SOX9 (usually de novo, autosomal dominant) or chromosomal rearrangements in the upstream regulatory region that disrupt SOX9's distant enhancers (a position effect). SOX9 is the master regulator of both chondrogenesis (the skeletal/airway phenotype) and testis determination (the XY sex reversal).
Mnemonics & Memory Aids
BENT
Hook:BENT: Bowed bones (camptomelia), Endocrine sex reversal (SOX9), Narrow thorax (laryngotracheomalacia), Testis gene SOX9.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A neonate has congenital bowing of the long bones with anterior tibial bowing and a skin dimple, hypoplastic scapulae and respiratory distress; the karyotype is 46,XY but the genitalia appear female. What is the diagnosis?”
What it is
- Rare, often lethal skeletal dysplasia; SOX9 mutation (usually de novo)
- 'Camptomelic' = bent-limbed
- Recognised among lethal fetal/neonatal dysplasias
Features
- Congenital long-bone bowing (anterior tibial bow + overlying skin dimple)
- Hypoplastic scapulae, reduced rib pairs, scoliosis, clubfeet, small thorax
- Cleft palate / Pierre Robin sequence; XY sex reversal (SOX9)
Mortality & management
- High mortality from respiratory compromise (small thorax + laryngotracheomalacia)
- Largely supportive/palliative; neonatal airway/respiratory support
- Survivors: orthopaedic care of bowing/scoliosis/feet; endocrine + genetic input
Evidence & Key Studies
Skeletal dysplasias of the fetus and infant (including campomelic dysplasia)
- Campomelic (camptomelic) dysplasia is among the recognised genetic skeletal disorders identified in the fetal/neonatal period; the most severe/lethal phenotypes are identifiable prenatally.
- Perinatal autopsy and post-mortem radiographs are crucial for definitive diagnosis, and an increasing number of cases are confirmed by genetic testing.
- Campomelic dysplasia is listed alongside thanatophoric dysplasia, osteogenesis imperfecta, achondroplasia and chondrodysplasia punctata among the dysplasias encountered.
Airway management: obstruction occurs at multiple levels
- Two illustrative children meeting diagnostic criteria, with a review of clinical-molecular correlations in the head and neck - so a case-based review, not a cohort.
- Describes campomelic dysplasia as a rare and HISTORICALLY lethal skeletal dysplasia with a variable but recognisable phenotype - the wording matters, since survival beyond infancy is now described.
- MANY patients have airway obstruction at MULTIPLE LEVELS, so relieving one level may leave the child obstructed.
- Mutations in or around SOX9 account for most patients, with the head and neck anomalies following from the same cartilage defect.
- Two patients: it informs airway strategy and cannot quantify how often multi-level obstruction occurs.
Familial recurrence from maternal germinal mosaicism - and how it was detected
- Most cases are sporadic and de novo; familial campomelic dysplasia is very rare.
- Two siblings with the classic phenotype shared a novel SOX9 frameshift mutation.
- Radiological examination of the apparently healthy MOTHER showed mild skeletal changes, and her somatic mosaicism for the mutation was then confirmed - the first molecularly confirmed maternal germinal mosaicism for SOX9.
- The authors conclude that meticulous clinical examination of superficially healthy parents is needed to avoid overlooking germinal mosaicism.
- A single family: it establishes that mosaic transmission occurs and cannot give a recurrence risk.
The recognition of campomelic dysplasia among the lethal/severe genetic skeletal dysplasias of the fetus/infant (identifiable prenatally, confirmed by radiographs/genetic testing) comes from the cited Jezova review. The SOX9 genetic basis, the skeletal hallmark (congenital long-bone bowing/camptomelia with anterior tibial bow and skin dimple, hypoplastic scapulae), the respiratory compromise from the small thorax and laryngotracheomalacia driving high mortality, the SOX9-related XY sex reversal, the associated anomalies (cleft palate/Pierre Robin), and the supportive/palliative-and-orthopaedic management are standard, well-established teaching. That airway obstruction occurs at multiple levels, and the description of the condition as historically rather than uniformly lethal, come from the cited Nelson review of two patients. The maternal germinal mosaicism, and the point that radiographs of an apparently healthy parent revealed mild skeletal changes, come from the cited Higeta report of a single family. No reliable figure for neonatal mortality, overall survival or the proportion of 46,XY individuals with sex reversal was retrieved, so none is quoted here - the phenotype is described qualitatively rather than with an invented percentage. See also skeletal dysplasias and, for the differential of a bowed tibia in a neonate, congenital pseudarthrosis of the tibia. The library has no dedicated congenital tibial bowing or disorders-of-sex-development topic.