Idiopathic Scaphoid Osteonecrosis | Proximal Pole Disease | Diagnosis of Exclusion
- Diagnosis of exclusion: Preiser is idiopathic AVN with NO acute fracture - rule out occult fracture/nonunion first
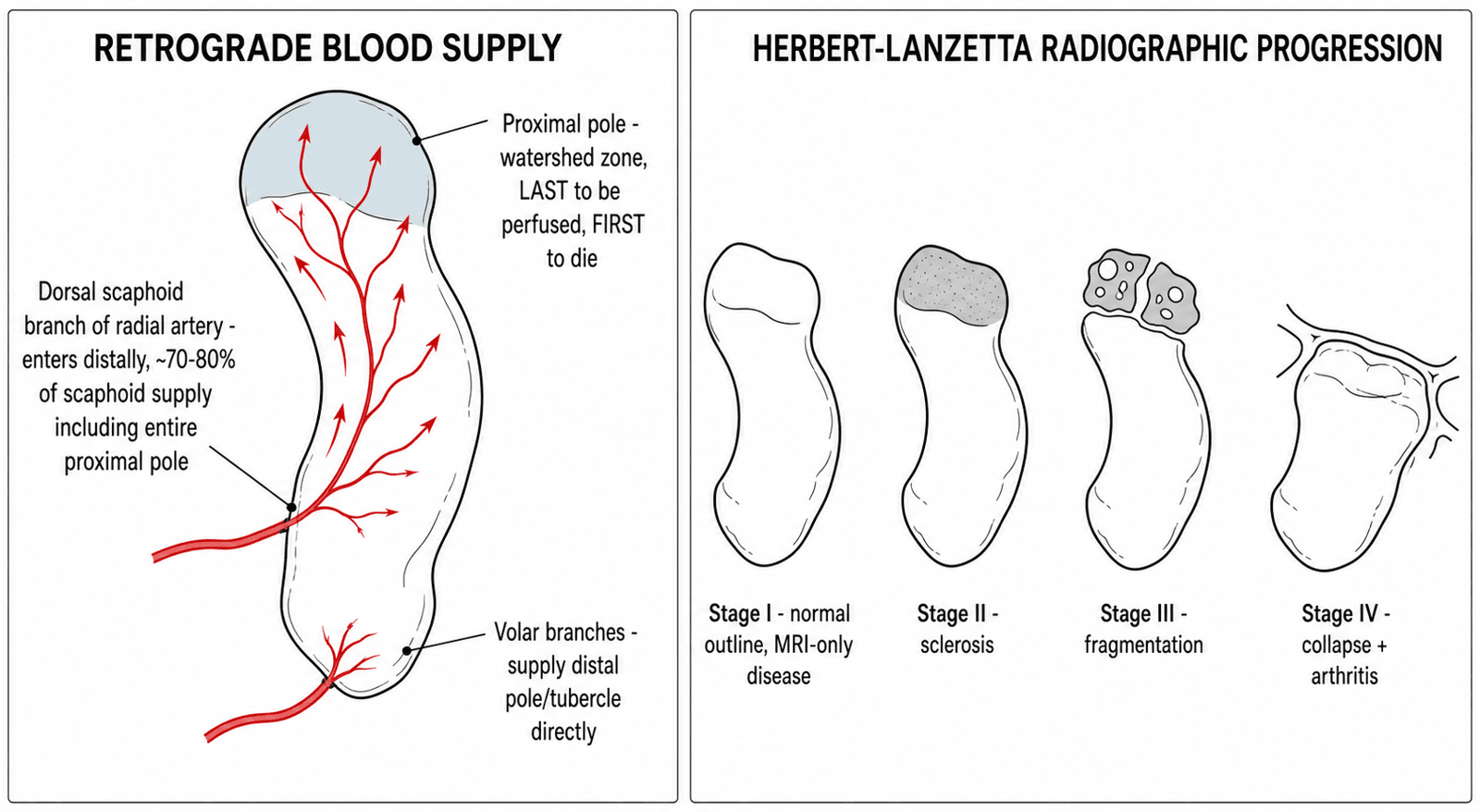
- Retrograde blood supply: dorsal scaphoid branch of the radial artery enters distally, so the PROXIMAL pole is most ischaemic
- MRI is the key test: diffuse low T1 signal of the scaphoid; Stage I is MRI-only with normal radiographs
- Kalainov MRI split: complete (entire scaphoid) vs partial (proximal pole only) necrosis - guides graft suitability
- Salvage when collapsed/arthritic: proximal row carpectomy and four-corner fusion give the most reliable pain relief
- “Scaphoid is the 2nd most common carpal bone for AVN after the lunate
- “Proximal pole disease = retrograde, distally-entering blood supply
- “Normal X-ray does not exclude Preiser - get an MRI
- “No level I evidence and no formal guideline - treatment is staged and individualised
Preiser disease = idiopathic AVN of the scaphoid with NO acute fracture. Before you call it Preiser, exclude an occult fracture or established nonunion (which has its own proximal-pole AVN). The history of insidious pain without significant trauma is the giveaway.
The scaphoid has a retrograde blood supply. The dorsal scaphoid branch of the radial artery enters the dorsal ridge distally and runs proximally, so the proximal pole is the watershed and the first to die - the same reason proximal pole fractures fail to unite.
Plain films can be normal early (Stage I). Diffuse low T1 signal of the scaphoid confirms AVN. MRI also separates complete from partial necrosis (Kalainov), which influences whether a vascularized graft is sensible.
There is no level I evidence and no society guideline. Management is built on small case series: immobilize early disease, graft viable non-arthritic scaphoids, and salvage once the carpus collapses or arthritis appears.
- Imaging
- Normal X-ray, MRI positive
- Preferred treatment
- Immobilization, activity change, observe
- Key pearl
- Some viable scaphoids revascularise without surgery
- Imaging
- Sclerosis / density change, no fragmentation
- Preferred treatment
- Vascularized bone graft or radial osteotomy (if viable, no arthritis)
- Key pearl
- Best stage for joint-preserving surgery
- Imaging
- Fragmentation / cystic change of proximal pole
- Preferred treatment
- Graft if no arthritis; otherwise salvage
- Key pearl
- Assess cartilage and carpal alignment carefully
- Imaging
- Collapse + peri-scaphoid arthritis
- Preferred treatment
- Salvage: PRC or four-corner fusion
- Key pearl
- Joint-preserving surgery no longer works
SAFCHerbert-Lanzetta Radiographic Stages
Hook:SAFC = Silent, Altered, Fragmented, Collapsed - the radiographic march of an untreated osteonecrotic scaphoid.
PFESalvage Options Once the Scaphoid Is Gone
Hook:PFE = the salvage toolkit for an arthritic or collapsed Preiser wrist - motion-preserving (PRC, four-corner) before motion-sacrificing (total fusion).
Overview and Epidemiology
Preiser disease is rare but a classic exam topic because it forces you to reason from first principles: scaphoid vascular anatomy, the difference between AVN and nonunion, and a staged treatment algorithm where no guideline exists.
Preiser disease is idiopathic avascular necrosis (osteonecrosis) of the scaphoid occurring without an acute fracture. It was first described by Georg Preiser in 1910. The scaphoid is the second most common carpal bone to undergo osteonecrosis after the lunate (Kienbock's disease).
- Age: typically 30-50 years
- Sex: both sexes affected; several surgical series show a female predominance
- Laterality: usually unilateral
- Rarity: only a few hundred cases in the world literature
A pooled literature review of 53 publications captured only around 170 patients in a century.
- Early (I-II): a viable scaphoid may revascularise or remain stable
- Mid (III): fragmentation and proximal-pole volume loss
- Advanced (IV): collapse and peri-scaphoid arthritis (SNAC-like pattern)
- Timeline: months to years
Unlike acute fracture AVN, the necrosis here is primary, not the result of a displaced fragment losing its blood supply.
Both can show proximal-pole sclerosis, but Preiser disease has no fracture line - the necrosis is primary and idiopathic. In nonunion, the AVN is a consequence of a fracture that failed to heal. On MRI, Preiser typically shows necrosis confined to the zone of dead bone, whereas a nonunion shows a discrete fracture line. Getting this distinction right changes both the diagnosis and the operation.
Pathophysiology and Anatomy
The scaphoid receives roughly 70-80% of its blood (including the entire proximal pole) from the dorsal scaphoid branch of the radial artery, which enters the dorsal ridge distally and runs retrograde toward the proximal pole. The distal pole and tubercle are supplied by volar branches. Because no vessel enters the proximal pole directly, it is the watershed and dies first - the same anatomy that explains delayed union of proximal pole fractures.
Aetiology is multifactorial and, by definition, often unknown:
Risk Factors and Associations
-
Slender ("type 2") scaphoid morphology
- A narrow scaphoid has a sparser intra-osseous vascular network
- Over-represented in operative Preiser series compared with the wider "type 1" scaphoid
-
Repetitive load and vibration
- Manual labour, drilling, impact sports
- Cumulative microtrauma to a marginally perfused bone
-
Drugs and systemic disease
- Corticosteroids, cytotoxic chemotherapy, alcohol
- Systemic lupus erythematosus, vasculitis, sickle cell disease, gout, renal disease
-
Idiopathic
- In many patients no cause is ever identified - this is the "core" Preiser group
Pathophysiology cascade:
- Compromised perfusion of a marginally vascularised (often slender) scaphoid
- Ischaemia of the proximal pole (the watershed zone)
- Osteocyte death; dead trabecular bone is not resorbed, producing relative sclerosis on X-ray
- Subchondral microfracture and fragmentation
- Loss of scaphoid height, carpal malalignment (DISI) and instability
- Peri-scaphoid radiocarpal and midcarpal arthritis
A radiology study described a three-layered scaphoid in Preiser disease: a proximal zone of osteonecrosis, a middle zone of repair, and a distal zone of viable marrow. Pathological fractures occurred only within the necrotic zone. This maps neatly onto the retrograde, distal-to-proximal blood supply.
Increased density does not mean "more bone". Living bone around the dead segment continues to be remodelled and partly resorbed, while the dead bone is not - so the necrotic area looks relatively dense on radiographs (the same principle as in Kienbock's and femoral head AVN).
The Distal-Pole Variant: Reverse-Pattern Scaphoid Osteonecrosis
The distal pole and tubercle receive a direct, antegrade volar blood supply (palmar and superficial palmar branches of the radial artery entering the distal tubercle), so they are the best-perfused part of the scaphoid. That is precisely why the proximal pole, fed only retrograde, is the watershed that dies first - and why isolated distal-pole necrosis is a genuine rarity worth flagging.
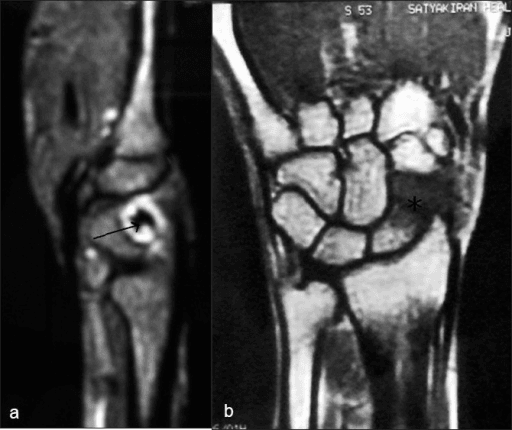
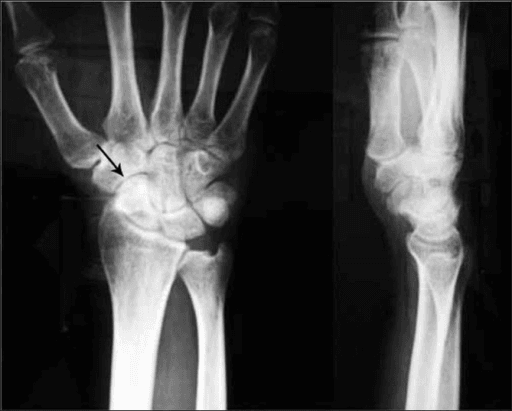
Almost all Preiser disease affects the proximal pole or the whole scaphoid, because the proximal pole is the retrograde watershed. Nontraumatic osteonecrosis confined to the distal pole is a recognised but very rare "reverse-pattern" variant - and it is the pattern captured in this topic's imaging panels (a drill operator whose distal-pole necrosis revascularised with rest and a change of occupation). It matters for three reasons:
The distal pole is normally well perfused, so idiopathic necrosis there is exceptional. When it does occur it implies an unusual insult acting on a marginally perfused (often slender) scaphoid rather than a simple watershed failure.
The distal pole is not the structural keystone of carpal alignment, so distal-pole necrosis is less likely to drive the DISI and collapse cascade. As in the illustrated case, an early, viable distal pole may revascularise over one to two years with immobilization and load reduction alone.
A dense distal pole must still be separated from an old tubercle fracture, an accessory ossicle, or degenerative sclerosis of the scaphotrapeziotrapezoid (STT) joint - all of which can mimic focal distal-pole osteonecrosis on plain films.
Because the term Preiser was coined for proximal or whole-scaphoid disease, a distal-pole case sits at the edge of the definition. Describe the necrosis by its actual location rather than forcing every dense scaphoid into the proximal-pole box.
Scaphoid Morphology: the Slender (Type 2) Scaphoid and the Contralateral Wrist
The most consistent constitutional risk factor for idiopathic scaphoid necrosis is a slender scaphoid shape. Scaphoid morphology is broadly divided into a wide (type 1) and a slender (type 2) form; the slender scaphoid carries a sparser intra-osseous vascular network, leaving its already-marginal proximal pole even more vulnerable when perfusion is challenged by load, drugs or systemic disease.
In the Mayo series of 39 operated wrists, Amundsen and colleagues assessed the unaffected contralateral wrist in patients with unilateral disease and found a slender scaphoid shape in half of the wrists that could be evaluated (four of eight) - supporting a constitutional predisposition rather than a purely acquired insult, since the shape is present in the healthy wrist too.
Because Preiser disease is usually unilateral, the contralateral scaphoid is a free control: image it to establish the patient's baseline morphology, to exclude asymptomatic bilateral disease, and as an anatomical template for reconstruction planning.
The classic Preiser vignette is a constitutional-plus-mechanical two-hit: a slender, marginally perfused scaphoid (the predisposition) in someone who loads it hard - the vibrating drill, the impact sport - or who carries a systemic insult (corticosteroids, chemotherapy, connective-tissue disease). Neither hit alone reliably kills the bone; together they do, which is why so many cases remain labelled idiopathic.
Classification Systems
Herbert-Lanzetta Classification (Radiographic)
The original and most widely used staging system, based on plain radiographs and treatment implications.
- Radiographic findings
- Normal radiograph; MRI shows AVN
- Scaphoid status
- Structurally intact
- Treatment approach
- Immobilization, observation
- Radiographic findings
- Sclerosis / density change, normal shape
- Scaphoid status
- Intact, no fragmentation
- Treatment approach
- Vascularized graft or radial osteotomy
- Radiographic findings
- Fragmentation / cystic change
- Scaphoid status
- Proximal pole losing volume
- Treatment approach
- Graft if no arthritis, else salvage
- Radiographic findings
- Collapse with peri-scaphoid arthritis
- Scaphoid status
- Fragmented, arthritic carpus
- Treatment approach
- Salvage (PRC, four-corner fusion)
Stage IV is the prognostic watershed: once peri-scaphoid arthritis is established, joint-preserving surgery is no longer effective and salvage is required.
Clinical Assessment
- Pain: insidious radial-sided / dorsal wrist pain, worse with activity
- No significant trauma: or pain disproportionate to a trivial injury
- Weakness: reduced grip strength
- Stiffness: progressive loss of wrist motion
- Risk factors: steroid use, chemotherapy, connective-tissue disease, vibration exposure
A drill operator or manual worker with months of unexplained radial wrist pain is a classic vignette.
- Tenderness: over the anatomical snuffbox / scaphoid
- Swelling: dorsoradial fullness
- ROM: reduced flexion-extension, painful at extremes
- Grip: weak and painful
- Watson (scaphoid shift) test: may be positive if carpal instability has developed
Findings are non-specific; imaging makes the diagnosis.
Radial-sided wrist pain in an adult has several mimics. MRI is the single best discriminator: Preiser disease shows diffuse low T1 marrow signal of the scaphoid without a fracture line, whereas the alternatives below have characteristic alternative patterns.
- Typical features
- Insidious radial wrist pain, no acute fracture
- Key imaging discriminator
- Diffuse low T1 scaphoid signal, NO fracture line
- Distinguishing point from Preiser
- Primary idiopathic AVN of an intact scaphoid
- Typical features
- Prior wrist injury, snuffbox pain
- Key imaging discriminator
- Discrete fracture line plus proximal-pole sclerosis
- Distinguishing point from Preiser
- AVN is secondary to a fracture that failed to unite
- Typical features
- Acute fall on outstretched hand, focal tenderness
- Key imaging discriminator
- Fracture line on MRI/CT, bone oedema
- Distinguishing point from Preiser
- Acute trauma and a true fracture, not idiopathic AVN
- Typical features
- Trauma, dorsal SL tenderness, positive Watson
- Key imaging discriminator
- SL gap (Terry-Thomas), DISI; scaphoid marrow normal
- Distinguishing point from Preiser
- Ligamentous instability; scaphoid signal is normal
- Typical features
- Radial styloid pain, positive Finkelstein
- Key imaging discriminator
- Tenosynovitis of first dorsal compartment; bone normal
- Distinguishing point from Preiser
- Tendon, not bone, pathology
- Typical features
- Older patient, base-of-thumb / radial pain
- Key imaging discriminator
- Joint-space loss and osteophytes; no diffuse AVN
- Distinguishing point from Preiser
- Degenerative joint disease rather than osteonecrosis
Investigations
Investigation Protocol
PA, lateral and scaphoid (ulnar-deviation) views. Look for scaphoid sclerosis (Stage II), fragmentation/cysts (Stage III), collapse and peri-scaphoid arthritis (Stage IV), and any DISI on the lateral. Films are normal in Stage I, so a normal radiograph never excludes the diagnosis.
T1 and T2 sequences (consider contrast). Diffuse low T1 signal confirms AVN; absence of a fracture line distinguishes Preiser from nonunion. MRI detects Stage I disease, assesses lunate viability, and separates complete vs partial necrosis (Kalainov) to guide graft suitability.
For bony detail and surgical planning. Defines fragmentation, cyst location, collapse and any subtle fracture line. Sagittal-oblique reformats along the scaphoid axis are most useful.
Direct cartilage assessment. Allows grading of articular damage and can be combined with debridement; helps decide between joint-preserving surgery and salvage when imaging is equivocal.
Key Imaging Points
- What it shows
- Sclerosis, fragmentation, collapse, arthritis
- Role in Preiser disease
- Herbert-Lanzetta staging; normal in Stage I
- What it shows
- Diffuse low T1 marrow signal, extent of necrosis
- Role in Preiser disease
- Confirms diagnosis; Kalainov complete vs partial; detects Stage I
- What it shows
- Trabecular detail, cysts, fracture line, collapse
- Role in Preiser disease
- Surgical planning; excludes occult fracture/nonunion

Management Algorithm
Conservative Management
Indications: Stage I disease, viable scaphoid, low-demand or reluctant patient, significant comorbidity.
Conservative Treatment Steps
Cast or splint for several weeks to months to unload the scaphoid and allow revascularisation. Combine with activity / occupational modification (e.g. moving away from vibration or heavy impact work). Monitor with serial radiographs and MRI.
Avoid heavy load and vibration. NSAIDs for symptom control. Hand therapy to maintain motion.
Repeat MRI to detect revascularisation or progression. Some early, viable scaphoids recover (as in the illustrated case); others progress and need surgery.
Conservative care is most appropriate for genuinely early, viable disease - it is temporizing once fragmentation or arthritis appears.
- Preferred treatment
- Immobilization + activity change
- Alternative
- Observation with serial MRI
- Notes
- Some viable scaphoids revascularise
- Preferred treatment
- Vascularized bone graft
- Alternative
- Closing radial wedge osteotomy
- Notes
- Best window for joint preservation
- Preferred treatment
- VBG if no arthritis
- Alternative
- Salvage if cartilage damaged
- Notes
- Decision hinges on arthritis and necrosis extent
- Preferred treatment
- PRC or four-corner fusion
- Alternative
- Total wrist fusion (end-stage)
- Notes
- Joint-preserving surgery no longer effective
Complications
- Early complications
- Persistent pain
- Late complications
- Progression to collapse / arthritis
- Management
- Convert to surgery
- Early complications
- Pedicle injury, stiffness
- Late complications
- Incomplete revascularisation, ongoing arthritis
- Management
- Salvage procedure
- Early complications
- EPL rupture, hardware irritation, DRUJ symptoms
- Late complications
- Stage progression despite pain relief
- Management
- Tendon reconstruction, revision
- Early complications
- Stiffness, CRPS
- Late complications
- Radiocapitate arthritis over time
- Management
- Convert to fusion
- Early complications
- Nonunion, hardware prominence
- Late complications
- Adjacent-joint arthritis
- Management
- Revision / total fusion
General Complications
- Fragmentation, scaphoid collapse, DISI and peri-scaphoid arthritis
- Some early viable scaphoids instead revascularise and stabilise
- Risk after any wrist surgery; minimise with early motion and good analgesia
- Common after prolonged immobilization or fusion; early hand therapy mitigates it
Clinical Relevance and Outcomes
- Pain relief
- Variable; some full recovery
- Motion
- Often preserved
- Evidence
- Case reports / small series
- Pain relief
- Improved in most
- Motion
- Preserved (around half of normal)
- Evidence
- Level IV series
- Pain relief
- Good pain relief
- Motion
- Largely retained
- Evidence
- Small Level V series
- Pain relief
- Reliable pain relief
- Motion
- Roughly 50% of normal
- Evidence
- Level IV salvage data
Prognostic factors:
- Better outcome
- I-II
- Worse outcome
- III-IV
- Better outcome
- Partial (type 2)
- Worse outcome
- Complete (type 1)
- Better outcome
- Intact
- Worse outcome
- Peri-scaphoid arthritis
- Better outcome
- Stable
- Worse outcome
- DISI / collapse
Bottom line: outcomes are driven by when the disease is caught. Caught early and viable, the scaphoid may be preserved or even revascularise; caught late with collapse and arthritis, salvage gives dependable pain relief but never restores a normal wrist.
Guidelines, Registries & Global Practice
Global epidemiology. Preiser disease is rare worldwide - only a few hundred cases exist in the literature, and most hand surgeons see only one or two in a career. It clusters in adults aged 30-50, with several surgical series reporting a female predominance, and is associated with corticosteroids, chemotherapy, alcohol, connective-tissue disease and a slender scaphoid morphology. There is no population incidence figure and no implant registry, because the operations performed (grafts, osteotomies, carpectomies and fusions) are not arthroplasty.
No single global guideline - practice rests on case-series evidence. No society publishes a formal Preiser treatment guideline. Practice converges on a staging-driven algorithm derived from Level IV-V evidence.
- Staging emphasis
- Herbert-Lanzetta + Kalainov MRI
- Early disease (Stage I-II)
- Vascularized bone graft for viable, non-arthritic scaphoids
- Advanced (III-IV)
- PRC favoured; four-corner fusion if capitate arthritic
- Staging emphasis
- Herbert-Lanzetta + MRI necrosis extent
- Early disease (Stage I-II)
- Vascularized graft (Zaidemberg-type) in early stages
- Advanced (III-IV)
- Scaphoidectomy +/- implant, PRC or carpal arthrodesis
- Staging emphasis
- Herbert-Lanzetta + Kalainov + DISI assessment
- Early disease (Stage I-II)
- Closing radial wedge osteotomy as less-invasive option
- Advanced (III-IV)
- Conservative care common in elderly; salvage if disabling
- Staging emphasis
- Plain radiographs (MRI often unavailable)
- Early disease (Stage I-II)
- Immobilization and activity modification
- Advanced (III-IV)
- Total wrist fusion as reliable, low-cost salvage
Registry and high- vs limited-resource practice. Where MRI is freely available, early (Stage I) disease is detected and viable scaphoids can be grafted or simply observed before collapse. Where MRI is scarce, diagnosis is later and total wrist fusion becomes the dependable salvage because it needs no specialist implant and reliably abolishes pain. Vascularized grafting and microsurgical reconstruction are concentrated in specialist hand units.
Consent essentials (universal). For joint-preserving surgery, counsel that proximal-pole revascularisation is often incomplete and arthritis may still progress. For salvage surgery, counsel explicitly on the motion-versus-pain-relief trade-off (PRC and four-corner fusion preserve some motion; total fusion removes motion but most reliably relieves pain), and on progression risk if early disease is managed non-operatively.
Controversies and Areas of Uncertainty
Preiser disease has no level I evidence and no consensus guideline. A strong candidate acknowledges the uncertainty rather than overstating any single procedure.
Preiser's original 1910 description was controversial and some early "cases" were probably unrecognised fractures. Modern authors restrict the term to genuinely idiopathic AVN with no fracture, but the boundary with occult fracture and nonunion remains debated.
A systematic review found surgery gave greater pain relief than conservative treatment in Stages II-III, but the evidence is entirely Level IV case series. Some early, viable scaphoids revascularise with immobilization alone, so not every patient needs an operation.
A large single-centre series found pedicled vascularized bone grafts gave functional outcomes similar to salvage procedures but preserved the scaphoid in about 70% of cases - so the trade-off (preserve a partly dead bone vs remove it) is genuinely unsettled.
Even when grafts improve MRI signal, revascularisation of the proximal pole is frequently incomplete, and arthritis can still progress. This tempers enthusiasm for grafting in wholly necrotic (Kalainov type 1) scaphoids.
Closing radial wedge osteotomy can relieve pain and preserve motion, but in published series radiographic stage still progressed in many patients - suggesting it is symptom-modifying rather than disease-modifying.
As in other end-stage carpal collapse, both salvage options give reliable pain relief with broadly comparable function; choice is driven by cartilage status, demand and surgeon preference rather than high-quality comparative data.
SCAPHOIDWhy the Scaphoid (and the Proximal Pole) Dies
Hook:SCAPHOID spells out both the bone and the reasons its proximal pole is so prone to avascular necrosis.
MCQ Practice Points
Q: Which carpal bone is the second most common site of avascular necrosis after the lunate? A: The scaphoid - idiopathic scaphoid osteonecrosis is termed Preiser disease.
Q: Why is the proximal pole of the scaphoid most affected in Preiser disease? A: The scaphoid has a retrograde blood supply - the dorsal scaphoid branch of the radial artery enters the dorsal ridge distally and runs proximally, so the proximal pole is the watershed and dies first.
Q: What is the key investigation for diagnosing early Preiser disease? A: MRI - it detects diffuse low T1 marrow signal (Stage I) before radiographic changes and distinguishes Preiser from scaphoid nonunion by the absence of a fracture line.
Q: Name the two main classification systems used in Preiser disease. A: The Herbert-Lanzetta radiographic staging (four stages) and the Kalainov MRI classification (complete vs partial necrosis).
Q: When is a vascularized bone graft appropriate in Preiser disease? A: In early disease (Herbert I-II) with a viable scaphoid and no radiocarpal arthritis or carpal instability - ideally a partial (Kalainov type 2) necrosis with viable distal bone.
Q: What is the salvage procedure favoured for advanced (Stage III-IV) Preiser disease in the systematic review evidence? A: Proximal row carpectomy - it gives reliable pain relief and preserves roughly half of wrist motion, provided the capitate head and lunate fossa cartilage are intact.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 36-year-old male drill operator presents with 4 months of insidious radial-sided wrist pain and no clear injury. Snuffbox tenderness is present. Plain radiographs of the wrist are reported as normal. How do you proceed?”
“A 40-year-old woman has 8 months of dorsoradial wrist pain. Radiographs show scaphoid sclerosis without fragmentation. MRI confirms avascular necrosis limited to the proximal pole with viable distal bone, and there is no radiocarpal arthritis or carpal instability. What are her options?”
“A 55-year-old presents late with chronic wrist pain, stiffness and weakness. Radiographs show scaphoid fragmentation and collapse with peri-scaphoid radiocarpal arthritis and a DISI deformity. MRI shows necrosis of the whole scaphoid. How do you manage this, and what does the evidence say?”
Key Concepts
- Idiopathic AVN of the scaphoid with NO acute fracture
- 2nd most common carpal AVN after the lunate (Kienbock's)
- Proximal pole most affected - retrograde, distally-entering blood supply
- Diagnosis of exclusion - rule out occult fracture / nonunion first
Classifications
- Herbert-Lanzetta (radiographic): I normal X-ray, II sclerosis, III fragmentation, IV collapse + arthritis
- Kalainov (MRI): complete (whole scaphoid) vs partial (proximal pole) necrosis
- Schmitt 3-zone model: proximal necrosis, middle repair, distal viable
Investigations
- MRI = key test: diffuse low T1, no fracture line; detects Stage I
- Radiographs: sclerosis, fragmentation, collapse, arthritis (normal in Stage I)
- CT: bony detail, exclude occult fracture, surgical planning
Treatment by Stage
- Stage I: immobilization + activity change, serial MRI
- Stage II: vascularized bone graft (or radial wedge osteotomy)
- Stage III: graft if no arthritis, else salvage
- Stage IV: PRC or four-corner fusion; total fusion for end-stage
Exam Pearls
- Normal X-ray does NOT exclude Preiser - order an MRI
- VBG only for early, viable, non-arthritic scaphoids
- Proximal-pole revascularisation after grafting is often incomplete
- No level I evidence and no formal guideline - staged, individualised care
Evidence Base
- Updated review of 53 publications and 170 patients since Preiser's 1910 description
- Scaphoid is the second most frequent carpal bone for avascular necrosis after the lunate
- Two modern imaging-based classifications now supplement the original Herbert-Lanzetta radiographic system
- Proposes a simple staged treatment algorithm given the absence of formal guidelines
- 10 patients with primary scaphoid osteonecrosis imaged with radiographs, CT and contrast-enhanced MRI
- A three-layered architecture was found: proximal necrosis, middle repair zone, distal viable marrow
- Pathological fractures occurred exclusively within the necrotic zone, unlike scaphoid nonunion
- Three morphological stages described; the initial stage is visible only on MRI