Chordoma | Chondrosarcoma | Osteosarcoma | Ewing Sarcoma
- Chordoma - most common primary malignant spine tumor, arises from notochord remnants, sacrum 50%, skull base 35%
- Chondrosarcoma - second most common, arises from cartilage, ring-and-arc calcifications on CT
- En bloc resection is goal for chordoma/chondrosarcoma (chemotherapy and radiation resistant)
- Ewing sarcoma - pediatric/young adult, highly chemo/radiosensitive, permeative bone destruction
- Osteosarcoma - rare in spine, requires neoadjuvant chemo, osteoid matrix on imaging
- “Chordoma - T2 hyperintense, physaliferous cells (vacuolated), brachyury positive
- “Chondrosarcoma - ring-and-arc calcifications, arises from posterior elements
- “Marginal excision = 50-70% local recurrence vs 20% with wide margins
- “Ewing and osteosarcoma require chemotherapy unlike chordoma/chondrosarcoma
Know the distribution: Sacrococcygeal 50%, skull base (clivus) 35%, mobile spine 15%. In mobile spine, cervical is more common than thoracic/lumbar. Arises from notochord remnants along the neuraxis.
Surgical margin is key - chordoma and chondrosarcoma are resistant to chemotherapy and conventional radiation. Wide en bloc resection (Enneking) is the only chance for cure. Intralesional = 100% recurrence.
Different from chordoma - highly chemosensitive and radiosensitive. Treatment is chemotherapy + surgery or radiation. Peak age 10-25 years. Permeative destruction with soft tissue mass. t(11;22) translocation.
Know distinguishing features: Chordoma = T2 hyperintense, lobulated, midline. Chondrosarcoma = ring-and-arc calcifications. Osteosarcoma = osteoid matrix, sunburst pattern. Ewing = permeative lytic.
- Chordoma
- 40-70 years
- Chondrosarcoma
- 30-70 years
- Osteosarcoma
- 10-30 years
- Ewing Sarcoma
- 10-25 years
- Chordoma
- Midline, sacrum 50%
- Chondrosarcoma
- Posterior elements
- Osteosarcoma
- Variable
- Ewing Sarcoma
- Any location
- Chordoma
- Notochord remnant
- Chondrosarcoma
- Cartilage
- Osteosarcoma
- Osteoblast
- Ewing Sarcoma
- Neural crest
- Chordoma
- T2 hyperintense
- Chondrosarcoma
- Ring-arc calcification
- Osteosarcoma
- Osteoid matrix
- Ewing Sarcoma
- Permeative lytic
- Chordoma
- No/Minimal
- Chondrosarcoma
- No
- Osteosarcoma
- Yes (chemo)
- Ewing Sarcoma
- Yes (both)
- Chordoma
- Wide en bloc
- Chondrosarcoma
- Wide en bloc
- Osteosarcoma
- Neoadjuvant chemo + surgery
- Ewing Sarcoma
- Chemo + surgery/RT
Overview and Epidemiology
Primary malignant bone tumors of the spine are rare, accounting for only 5% of all spinal tumors. The most common types are chordoma, chondrosarcoma, osteosarcoma, and Ewing sarcoma.
Relative Incidence of Primary Spine Tumors:
- % of Primary Spine Tumors
- 40%
- Typical Age
- 40-70 years
- Gender
- M more than F (2:1)
- % of Primary Spine Tumors
- 20%
- Typical Age
- 30-70 years
- Gender
- M=F
- % of Primary Spine Tumors
- 10%
- Typical Age
- 10-30 years
- Gender
- M more than F
- % of Primary Spine Tumors
- 5%
- Typical Age
- 10-25 years
- Gender
- M more than F
- % of Primary Spine Tumors
- 25%
- Typical Age
- Variable
- Gender
- Variable
Key Epidemiological Points:
Chordoma and chondrosarcoma are tumors of adulthood, while Ewing sarcoma and osteosarcoma predominantly affect children and young adults. Understanding age at presentation helps narrow the differential diagnosis.
Primary spine tumors have characteristic locations: Chordoma = midline (sacrum, clivus, vertebral body). Chondrosarcoma = posterior elements. Ewing sarcoma = any location. Osteosarcoma = vertebral body or posterior elements.
This page covers the primary malignant tumours, but the examiner's first sieve for any primary spinal bone tumour is where in the vertebra it sits and the patient's age - which also flags the common benign primaries. Posterior elements favour osteoid osteoma, osteoblastoma, aneurysmal bone cyst and chondrosarcoma; the vertebral body favours haemangioma, giant cell tumour, chordoma, eosinophilic granuloma (Langerhans cell histiocytosis, classically causing vertebra plana in a child), metastasis and myeloma. For age: under ~30 and benign-looking suggests osteoid osteoma/osteoblastoma/ABC/eosinophilic granuloma (or Ewing if aggressive); under ~30 and aggressive suggests Ewing or osteosarcoma; over ~40 with a destructive lesion is far more likely metastasis or myeloma than a primary sarcoma, with chordoma and chondrosarcoma the leading primary-malignant possibilities. A painful scoliosis with night pain relieved by NSAIDs in a teenager is the classic osteoid osteoma/osteoblastoma story. Place the lesion in this location-plus-age grid before committing to a diagnosis.
Pathophysiology
Cellular Origins
Notochordal Origin
Chordoma arises from remnants of the embryonic notochord - the primordial axial skeleton that guides vertebral development.
- Physaliferous cells - vacuolated cells containing mucin (pathognomonic)
- Lobulated architecture with fibrous septae
- Abundant myxoid matrix
- Brachyury positive (highly specific diagnostic marker)
- Cytokeratin positive (EMA, CK8/18)
- S-100 positive
Three histological subtypes: conventional (most common), chondroid (better prognosis), and dedifferentiated (worst prognosis with high-grade sarcomatous component).
Classification and Staging
Enneking Surgical Staging System
Standard staging for musculoskeletal tumors.
- Grade
- Low (G1)
- Compartment
- Intracompartmental
- Metastases
- M0
- Grade
- Low (G1)
- Compartment
- Extracompartmental
- Metastases
- M0
- Grade
- High (G2)
- Compartment
- Intracompartmental
- Metastases
- M0
- Grade
- High (G2)
- Compartment
- Extracompartmental
- Metastases
- M0
- Grade
- Any
- Compartment
- Any
- Metastases
- M1
Most spine tumors at presentation are Stage IIB (extracompartmental) due to anatomic complexity of spine.
Clinical Presentation
Presenting Symptoms
- Localized back pain, often insidious onset
- Typically progressive over months
- Night pain and rest pain common
- May be mechanical or constant
- Radiculopathy from nerve root compression
- Myelopathy if cord compression
- Cauda equina syndrome with sacral tumors
- Bowel/bladder dysfunction (late)
Tumor-Specific Presentations
- Sacral: Low back pain, sciatica, constipation, urinary symptoms
- May present with palpable presacral mass on rectal examination
- Skull base: Cranial nerve palsies, headache
- Often presents with systemic symptoms
- Fever, weight loss, elevated inflammatory markers
- May mimic infection
- Pain and swelling
- Pathological fracture possible
- Elevated alkaline phosphatase
Red Flags
- Pain worse at night or at rest
- Progressive neurological deficit
- Weight loss, fever
- Mass lesion palpable
- Pathological fracture
Differential Diagnosis of a Destructive Spinal Lesion
A primary malignant bone tumour must be distinguished from far more common mimics. In any adult over 40 with a destructive vertebral lesion, metastasis and myeloma are statistically far more likely than a primary sarcoma - but the management of a primary tumour (en bloc, biopsy-tract excision) is so different that it must be actively excluded before any intervention.
- Typical age
- Bimodal
- Key discriminators
- Midline + T2 bright (chordoma); ring-arc Ca (chondrosarcoma); osteoid/sunburst (osteo); permeative + systemic features (Ewing)
- Why it matters
- Needs planned biopsy and en bloc resection - do not curette
- Typical age
- Over 50
- Key discriminators
- Known primary; multiple levels; pedicle erosion; usually spares disc
- Why it matters
- Most common malignant spine lesion - tissue/staging before assuming primary
- Typical age
- 50-70
- Key discriminators
- Diffuse osteopenia; punched-out lytic lesions; paraprotein on electrophoresis
- Why it matters
- Systemic disease - radiosensitive, rarely needs en bloc
- Typical age
- 20-40
- Key discriminators
- Expansile lytic lesion, often sacrum/vertebral body; locally aggressive, benign
- Why it matters
- Denosumab and curettage/resection - different algorithm
- Typical age
- Under 20
- Key discriminators
- Expansile, fluid-fluid levels on MRI, posterior elements
- Why it matters
- Benign - curettage/embolisation, not en bloc
- Typical age
- Any
- Key discriminators
- Disc + adjacent endplate destruction; fever; raised CRP/ESR; mimics Ewing
- Why it matters
- Antimicrobial therapy, not surgery - culture before treating
Investigations
Imaging
Initial Assessment
Often first imaging modality, but sensitivity is limited.
- Lytic vs sclerotic pattern
- Bone destruction
- Matrix mineralization
- Soft tissue mass
- Chordoma: Midline lytic destruction, soft tissue mass
- Chondrosarcoma: Stippled/ring-arc calcifications
- Osteosarcoma: Dense sclerosis, sunburst periosteal reaction
- Ewing: Permeative/moth-eaten destruction
Plain films may be normal in early disease. Advanced imaging always required.
Biopsy
Principles:
- Biopsy tract must be excisable with definitive surgery
- CT-guided preferred for spine
- Avoid contaminating multiple compartments
- Discuss approach with treating surgeon first
Poorly planned biopsy can compromise subsequent en bloc resection. The biopsy tract will need excision, so coordinate with the surgeon who will perform definitive surgery BEFORE biopsy.
Management
Surgical Principles
Gold Standard for Chordoma/Chondrosarcoma
Goal is negative surgical margins without violating tumor capsule.
- Intralesional: Through tumor (contamination)
- Marginal: Through reactive zone
- Wide: Through normal tissue, cuff around tumor
- Radical: Entire compartment (rarely achievable in spine)
- Intralesional: 100% recurrence
- Marginal: 50-70% recurrence
- Wide: 20-30% recurrence
En bloc vertebrectomy is technically demanding and requires experienced spine oncology team.
Treatment Algorithm
- Staging (MRI, CT, PET)
- Biopsy (coordinated with surgeon)
- En bloc resection with wide margins
- Consider proton therapy if margins positive
- Staging
- Neoadjuvant chemotherapy (10-12 weeks)
- Surgical resection
- Adjuvant chemotherapy based on necrosis
- Staging including whole-body PET
- Neoadjuvant chemotherapy
- Surgery or radiation (or both)
- Maintenance chemotherapy
Chordoma and chondrosarcoma are NOT chemosensitive - surgery is primary treatment. Ewing sarcoma and osteosarcoma ARE chemosensitive - chemotherapy is integral to treatment. This fundamental difference determines management approach.
Complications
Surgical Complications
- Wound complications (most common, especially sacral)
- Cerebrospinal fluid leak
- Neurological deficit
- Massive blood loss (average 2-5L for sacral tumors)
- Hardware failure
- Pseudarthrosis
- Adjacent level disease
- Chronic pain
Neurological Deficits
- S1 sacrifice: Ankle plantar flexion weakness
- S2 sacrifice: Bladder/bowel dysfunction likely
- S3 sacrifice: Definite bladder/bowel/sexual dysfunction
- Nerve root sacrifice may be required for clear margins
- Spinal cord injury risk with en bloc techniques
The functional cost of a sacrectomy is set by which S2-S4 roots survive, and the examinable rules are: bilateral preservation of S2 and at least one S3 is generally needed to retain useful bladder, bowel and sexual function; losing both S3 roots (a bilateral cut at or above S3) typically produces neurogenic bladder/bowel and sexual dysfunction. Unilateral sacrifice of even all sacral roots on one side is usually tolerated with preserved continence provided the contralateral S2-S4 are intact. Resection below S3 bilaterally usually preserves continence (with some saddle numbness). Separately from neurology, consider stability: a cut through or above S1 divides the weight-bearing ala and disrupts the pelvic ring, mandating lumbopelvic (spinopelvic) reconstruction, whereas low sacrectomies below S1 usually do not. So counsel and plan on two axes - the roots kept (continence) and the level relative to S1 (stability).
Local Recurrence
- Intralesional vs en bloc surgery
- Positive surgical margins
- Tumor grade
- Dedifferentiated histology
- Re-resection if feasible
- Radiation therapy (proton/carbon ion)
- Palliative care if unresectable
Postoperative Care
En Bloc Spine Tumor Resection Protocol
Postoperative Rehabilitation Timeline
- Intensive care monitoring for first 24-72 hours
- Hemodynamic monitoring (blood loss often 2-5L for sacral resections)
- Drain management and output monitoring
- Pain management (multimodal, patient-controlled analgesia)
- DVT prophylaxis (mechanical initially, chemical once hemostasis assured)
- Wound assessment for flap viability if soft tissue reconstruction
- Mobilisation with physiotherapy (weight-bearing status per surgeon)
- Wound care and drain removal when output minimal
- Bladder/bowel function monitoring (especially sacral resections)
- Nutritional support for wound healing
- Begin rehabilitation for neurological deficits
- Outpatient wound checks every 1-2 weeks
- Progressive mobilisation and physiotherapy
- Brace if spinal instability concern
- Imaging at 6 weeks to assess instrumentation
- Referral for radiation oncology if margins positive (proton therapy)
- Surveillance imaging every 3-6 months (MRI for local, CT chest for metastases)
- Functional rehabilitation for neurological deficits
- Oncology follow-up for adjuvant therapy if indicated
- Psychological support for adaptation to functional deficits
Outcomes
Survival by Tumor Type
- 5-Year Survival (Wide Excision)
- 65-70%
- 5-Year Survival (Marginal/Intralesional)
- 35-40%
- Key Prognostic Factor
- Surgical margin status
- 5-Year Survival (Wide Excision)
- 90%
- 5-Year Survival (Marginal/Intralesional)
- 70%
- Key Prognostic Factor
- Tumor grade
- 5-Year Survival (Wide Excision)
- 30%
- 5-Year Survival (Marginal/Intralesional)
- 10-15%
- Key Prognostic Factor
- Tumor grade
- 5-Year Survival (Wide Excision)
- 60-70%
- 5-Year Survival (Marginal/Intralesional)
- Similar (chemo-dependent)
- Key Prognostic Factor
- Response to chemotherapy
- 5-Year Survival (Wide Excision)
- 40-50%
- 5-Year Survival (Marginal/Intralesional)
- 20-30%
- Key Prognostic Factor
- Necrosis rate post-chemo
Local Recurrence Rates
- Wide margin: 20-30% local recurrence
- Marginal margin: 50-70% local recurrence
- Intralesional: Approaching 100% local recurrence
For chordoma and chondrosarcoma, surgical margin status is the MOST IMPORTANT prognostic factor. En bloc resection with wide margins is the only chance for long-term disease control. Proton beam therapy can help salvage positive margins.
Guidelines, Registries & Global Practice
Global epidemiology
Primary malignant bone tumours of the spine are rare, accounting for only a small fraction of spinal tumours; the spine is far more commonly affected by metastatic disease. Chordoma is the most frequent primary malignant tumour of the mobile spine and is itself uncommon. The age distribution is bimodal across the group: chordoma and chondrosarcoma predominate in adults (typically 40-70 and 30-70 years respectively), whereas Ewing sarcoma and osteosarcoma cluster in children and young adults. Across reported series there is a modest male predominance for chordoma. The largest contemporary outcome data come from multicentre registries rather than single-country health systems.
Major guidelines, side by side
- Core recommendation for primary malignant spine tumour
- Enneking-appropriate en bloc resection with wide/marginal margins for chordoma, chondrosarcoma, osteosarcoma and (where feasible) Ewing sarcoma; refer to a tumour-board centre before biopsy
- Strength / level
- Multicentre cohort evidence (Level III)
- Core recommendation for primary malignant spine tumour
- Centralise chordoma care; en bloc resection as first-line; high-dose particle (proton/carbon-ion) radiotherapy for residual, recurrent or unresectable disease; systemic options limited
- Strength / level
- Expert consensus position paper
- Core recommendation for primary malignant spine tumour
- All suspected bone sarcomas referred to a specialist sarcoma multidisciplinary team; diagnostic biopsy performed at (or directed by) the treating centre
- Strength / level
- Service-standard guidance
- Core recommendation for primary malignant spine tumour
- Histology-specific algorithms: wide excision for chordoma/chondrosarcoma; neoadjuvant chemotherapy + surgery for osteosarcoma; multiagent chemotherapy ± local therapy for Ewing sarcoma
- Strength / level
- Category 2A consensus
- Core recommendation for primary malignant spine tumour
- Defines diagnostic entities and grading (e.g. brachyury-defined chordoma, fusion-defined Ewing sarcoma, chondrosarcoma grade) that drive treatment
- Strength / level
- Reference standard
A consistent thread across all bodies is that biopsy must be planned by the treating sarcoma team, because a poorly placed tract can render a curative en bloc resection impossible.
Registry and multicentre evidence
Because each centre sees few cases, the strongest evidence is pooled. The AOSpine Knowledge Forum Tumour databases have quantified that Enneking-appropriate en bloc surgery improves survival and local control in spinal Ewing sarcoma and osteosarcoma. For radiotherapy, the Proton Collaborative Group prospective registry and large single-institution proton cohorts demonstrate high local control with low high-grade toxicity. These collaborations function as the de-facto registries for these rare tumours.
Global practice variation
The principal variation worldwide is access to particle therapy. Proton and carbon-ion facilities are concentrated in a limited number of centres in North America, Europe and Asia; carbon-ion therapy in particular is largely confined to dedicated centres (notably in Japan and Europe). In settings without particle therapy, management relies more heavily on achieving a wide en bloc margin and on high-dose photon techniques. Centralisation of these rare tumours to high-volume sarcoma units is recommended in every health system, as surgeon and centre experience correlate with margin achievement and outcome.
Given the rarity and complexity of these tumours, referral to a specialist sarcoma service is strongly recommended for all patients with a suspected primary malignant spine tumour before any biopsy is performed.
MCQ Practice Points
Q: What is the most common primary malignant bone tumor of the spine? A: Chordoma. It arises from notochordal remnants and occurs predominantly in the sacrum (50%), skull base (35%), and mobile spine (15%). It is a slow-growing, locally aggressive tumor with high recurrence rates.
Q: What histological finding is pathognomonic for chordoma? A: Physaliphorous cells (bubbly vacuolated cells) arranged in lobules within a myxoid matrix. These cells are positive for brachyury immunostaining, which is the most specific marker for chordoma.
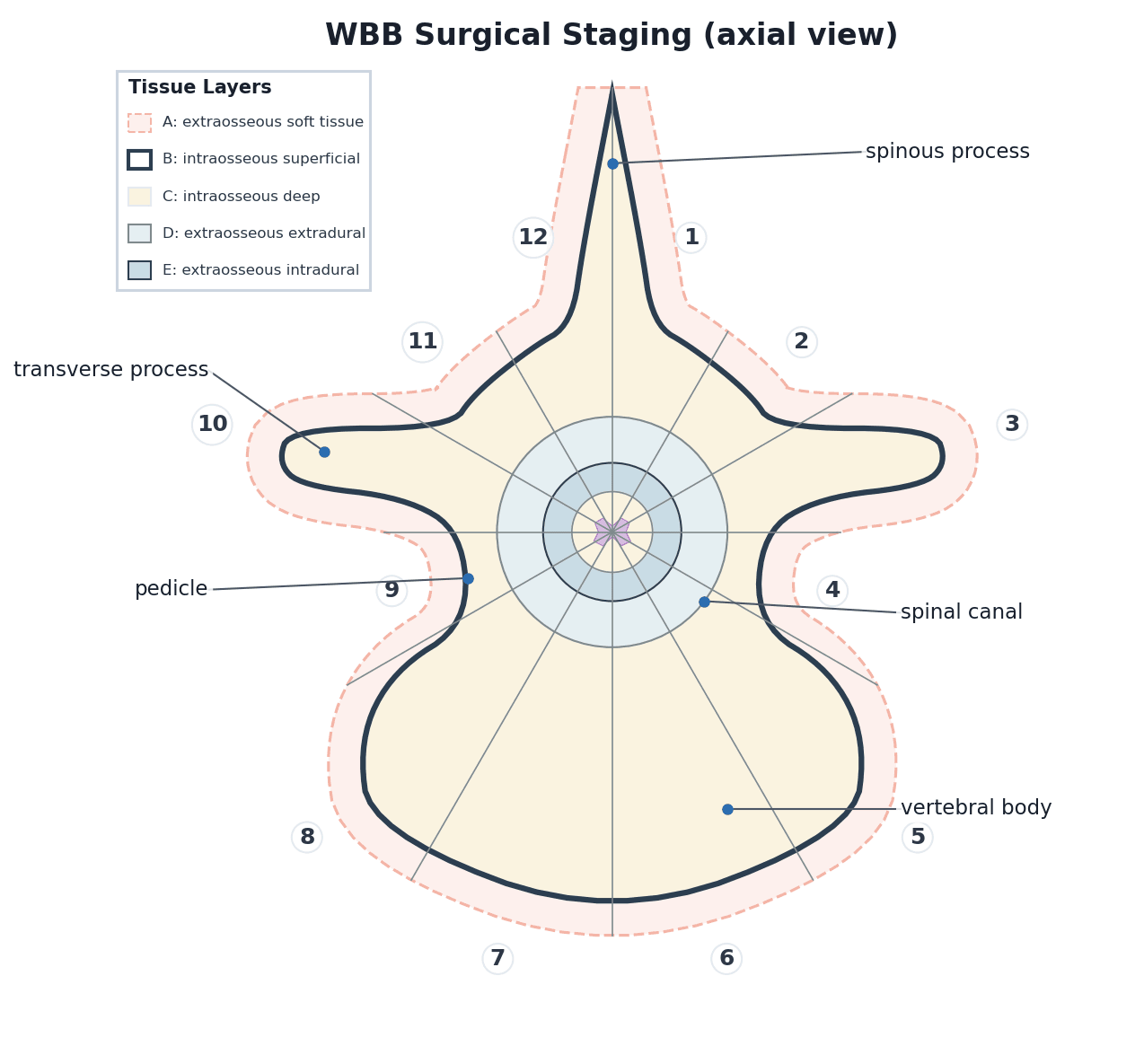
Q: What is the Enneking staging system for spinal tumors and how does it guide surgery? A: The WBB (Weinstein-Boriani-Biagini) system adapted for spine divides the vertebra into 12 sectors and 5 layers (A-E). It determines surgical margin possibilities - wide excision (en bloc) is possible when tumor is contained within sectors/layers that can be resected together.
Q: What radiation modality is preferred for chordoma and chondrosarcoma of the spine? A: Proton beam therapy or carbon ion therapy. These tumors are relatively radioresistant to conventional photon therapy but respond to particle therapy which delivers higher doses with sharp dose fall-off protecting the spinal cord.
At a Glance
Primary bone tumors of the spine represent only 5% of all spine tumors but require distinct management from metastases. Chordoma is the most common primary malignant spine tumor, arising from notochord remnants with 50% in the sacrococcygeal region—characterized by physaliferous cells, brachyury positivity, and T2 hyperintensity on MRI. Chondrosarcoma shows ring-and-arc calcifications and arises from posterior elements. Both chordoma and chondrosarcoma are resistant to chemotherapy and radiation, making en bloc resection with wide margins the only curative option—marginal excision results in 50-70% local recurrence. In contrast, Ewing sarcoma (pediatric, t(11;22) translocation) is highly chemosensitive and radiosensitive.
CEOSPrimary Spine Tumors - CEOS
Hook:CEOS tumors - Chordoma and Chondrosarcoma need En bloc, Others (Ewing, Osteo) Sensitive to chemo
PBSTNChordoma Key Features
Hook:PBSTN - Physaliferous cells with Brachyury positivity in Sacral tumors that are T2 bright from Notochord
IIIIIIEnneking Staging System
Hook:I-II-III: Low-High-Mets. Stage IIB is most common surgical presentation
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old man presents with 12 months of progressive low back and buttock pain. MRI shows a large destructive sacral mass that is very bright on T2-weighted imaging. The mass extends presacrally.”
“A 45-year-old woman presents with thoracic back pain. CT shows a mass arising from the posterior elements of T7 with characteristic ring-and-arc calcifications. There is extension into the spinal canal.”
“A 14-year-old boy presents with 6 weeks of back pain, fever, and weight loss. MRI shows a destructive lumbar vertebral body lesion with large paraspinal soft tissue mass. WCC and ESR are elevated.”
“A 60-year-old man who had sacral chordoma resection 3 years ago presents with increasing sacral pain. MRI shows a 4cm presacral mass consistent with local recurrence. There is no distant disease on PET-CT.”
Tumor Types
- Chordoma: Notochord origin, sacrum 50%, T2 bright, brachyury+
- Chondrosarcoma: Cartilage origin, posterior elements, ring-arc calcifications
- Osteosarcoma: Bone-forming, osteoid matrix, sunburst pattern
- Ewing: Neural crest, pediatric, t(11;22), permeative lytic
Treatment Differences
- Chordoma/Chondrosarcoma: En bloc resection (chemo/RT resistant)
- Osteosarcoma: Neoadjuvant chemo + surgery + adjuvant chemo
- Ewing: Chemo + surgery or radiation + chemo
- Margin status is critical for chordoma/chondrosarcoma
Enneking Staging
- Stage I: Low grade (G1), A=intra, B=extra compartmental
- Stage II: High grade (G2), A=intra, B=extra compartmental
- Stage III: Any grade with metastases
- Most spine tumors present as Stage IIB
Surgical Margins
- Intralesional: Through tumor = 100% recurrence
- Marginal: Through reactive zone = 50-70% recurrence
- Wide: Cuff of normal tissue = 20-30% recurrence
- Radical: Entire compartment (rarely achievable in spine)
Sacral Chordoma
- Combined anterior-posterior approach
- Level of resection determines function
- Above S2-S3: Bladder/bowel dysfunction
- Preoperative embolization essential
- Proton therapy if margins positive
Exam Pearls
- Ring-arc calcification = chondrosarcoma
- T2 hyperintense sacral mass = chordoma until proven otherwise
- Pediatric + systemic symptoms + spine mass = Ewing
- Biopsy tract must be excisable - coordinate with surgeon
Evidence Base
Chordoma of the Mobile Spine: Margin-Free En Bloc Resection
- Consecutive series of 52 chordomas of the mobile spine over 50 years
- Intralesional extracapsular excision plus radiotherapy: recurrence in 12 of 16 (mean 30 months)
- En bloc resection: 12 of 18 continuously disease-free at mean 8 years follow-up
- All recurrences after en bloc occurred where margins were contaminated or the tumour had been previously treated
Operative Management of Sacral Chordoma: Margin Predicts Survival
- 52 sacrococcygeal chordomas treated surgically (Mayo Clinic, 1980-2001)
- Overall local recurrence 44%; recurrence-free survival 59% at 5 years and 46% at 10 years
- Overall survival 74%, 52% and 47% at 5, 10 and 15 years
- A wide margin was the single most important predictor of survival - all wide-margin patients survived (p = 0.0001); a combined anteroposterior approach made a wide margin more likely (81% of wide-margin cases)
Ewing Sarcoma of the Mobile Spine
- 13 patients with non-metastatic mobile-spine Ewing sarcoma treated with multiagent chemotherapy plus radiotherapy for local control
- Disease-free survival 49% at 5 years and 36% at 10 years; local recurrence in 3 (23%)
- Pain control improved in 92% and motor function maintained or improved in most
- Post-laminectomy progressive kyphosis in 4 of 10 (40%), underscoring the need for reconstruction
WBB Surgical Staging of Primary Spine Tumours
- Defining paper introducing the Weinstein-Boriani-Biagini (WBB) surgical staging system
- Vertebra divided into 12 radiating zones (clock-face) and 5 tissue layers (A-E)
- Applies Enneking oncological principles to the unique anatomy of the spine
- Standardises terminology for tumour extent and surgical margins to enable planning and comparison across centres
AOSpine: En Bloc Resection in Spinal Ewing Sarcoma
- Multicentre AOSpine Knowledge Forum Tumour series of 58 surgically treated primary spinal Ewing sarcomas
- Enneking-appropriate (en bloc, wide/marginal) surgery was associated with significantly better survival (p = 0.034)
- Neoadjuvant plus postoperative chemotherapy significantly improved survival (p = 0.008)
- Intralesional margins and previous spine tumour surgery were associated with increased local recurrence
AOSpine: Prognostic Factors in Primary Spinal Osteosarcoma
- Multicentre AOSpine ambispective series of 58 primary spinal osteosarcomas (1987-2012)
- Enneking-appropriate (en bloc) resection gave longer median survival than Enneking-inappropriate surgery (6.8 vs 3.7 years, p = 0.048)
- Enneking-inappropriate surgery carried a significantly higher local recurrence rate (p = 0.001)
- 30% suffered local recurrence and 59% of those died; most patients die despite aggressive surgery
Adjuvant High-Dose Proton-Based Radiotherapy for Spinal Chordoma
- 76 primary spinal/sacral chordomas with en bloc resection and minimum 5-year follow-up (median 9.3 years)
- Completing the goal 70 Gy proton-based dose (C70) gave better 5-year overall survival than incomplete dosing (82% vs 63%, p = .001)
- 5-year local-recurrence-free interval was higher with complete dosing (93% vs 78%, p = .017)
- Local control rates fall with longer follow-up, so mid-term figures may overstate durability
Proton Therapy for Chordoma: Multicentre Prospective Registry
- 100 chordoma patients on the Proton Collaborative Group prospective registry (61% skull base, 23% spine, 16% sacrum)
- 85% had surgical resection; median proton dose 74 Gy (RBE)
- 2-/3-year local control 97%/94%, overall survival 89%/83%
- Very low high-grade toxicity - no grade 4 acute and no grade 3 or higher late toxicity; CNS necrosis under 1%
References
- Boriani S, Bandiera S, Biagini R, et al. Chordoma of the mobile spine: fifty years of experience. Spine (Phila Pa 1976). 2006;31(4):493-503. PMID: 16481964.
- Fuchs B, Dickey ID, Yaszemski MJ, et al. Operative management of sacral chordoma. J Bone Joint Surg Am. 2005;87(10):2211-6. PMID: 16203885.
- Boriani S, Weinstein JN, Biagini R. Primary bone tumors of the spine. Terminology and surgical staging. Spine (Phila Pa 1976). 1997;22(9):1036-44. PMID: 9152458.
- Marco RA, Gentry JB, Rhines LD, et al. Ewing's sarcoma of the mobile spine. Spine (Phila Pa 1976). 2005;30(7):769-73. PMID: 15803079.
- Stacchiotti S, Sommer J; Chordoma Global Consensus Group. Building a global consensus approach to chordoma: a position paper from the medical and patient community. Lancet Oncol. 2015;16(2):e71-83. PMID: 25638683.
- Charest-Morin R, Dirks MS, Patel S, et al. Ewing sarcoma of the spine: prognostic variables for survival and local control in surgically treated patients. Spine (Phila Pa 1976). 2018;43(9):622-629. PMID: 28837533.
- Dekutoski MB, Clarke MJ, Rose P, et al. Osteosarcoma of the spine: prognostic variables for local recurrence and overall survival, a multicenter ambispective study. J Neurosurg Spine. 2016;25(1):59-68. PMID: 26943248.
- Tobert DG, Kelly SP, Xiong GX, et al. The impact of radiotherapy on survival after surgical resection of chordoma with minimum five-year follow-up. Spine J. 2022;23(1):34-41. PMID: 35470086.
- Chhabra AM, Rice SR, Holtzman A, et al. Clinical outcomes and toxicities of 100 patients treated with proton therapy for chordoma on the proton collaborative group prospective registry. Radiother Oncol. 2023;183:109551. PMID: 36813169.
- Beddok A, Saint-Martin C, Mammar H, et al. High-dose proton therapy and tomotherapy for the treatment of sacral chordoma: a retrospective monocentric study. Acta Oncol. 2020;60(2):245-251. PMID: 33095672.