Popeye Deformity | Associated Rotator Cuff Pathology | Tenotomy vs Tenodesis
- Popeye deformity is the classic clinical sign (distal migration of muscle belly)
- Minimal functional loss in most patients (supinator strength preserved by short head)
- Associated pathology (rotator cuff tear, SLAP) is common and must be evaluated
- Tenodesis offers better cosmetic outcome and strength but higher complication rate than tenotomy
- Tenotomy is simpler, faster rehab, but leaves deformity and potential cramping
- “Rupture often provides spontaneous pain relief from chronic biceps tendinitis ('autotenotomy')
- “Distal biceps rupture is a DIFFERENT pathology with significant weakness (needs repair)
- “Speed's and Yergason's tests usually positive prior to rupture, negative after
- “Always check the rotator cuff - isolated LHB rupture is rare in older adults
Proximal biceps rupture is a sentinel sign for rotator cuff pathology in patients over 40. Always examine the cuff thoroughly. Isolated rupture is rare in this demographic.
Patients lose minimal elbow flexion strength (approx 20%) and supination strength because the short head remains intact and brachialis is the primary flexor. This justifies non-operative management in low-demand patients.
The "Popeye" deformity is the main complaint. Discuss this explicitly during consent. Tenotomy WILL result in deformity; tenodesis prevents it. Cramping is another potential sequela of tenotomy.
Distal biceps rupture is a completely different injury requiring surgical repair in most active patients due to significant supination strength loss. Do not conflate the two management algorithms.
- Injury Pattern
- Acute/Chronic Rupture
- Treatment
- Non-operative (Benign Neglect)
- Rationale
- Functional deficits minimal, avoids surgical risks
- Injury Pattern
- Rupture + Symptomatic RC Tear
- Treatment
- Tenodesis + RC Repair
- Rationale
- Addresses pathology, restores anatomy/cosmesis
- Injury Pattern
- Acute Traumatic Rupture
- Treatment
- Tenodesis
- Rationale
- Preserves maximal supination strength and endurance
- Injury Pattern
- Failed conservative / Cramping
- Treatment
- Delayed Tenodesis
- Rationale
- To resolve persistent cramping pain (cosmesis harder to fix late)
SCARIndications for Tenodesis
Hook:Tenodesis heals the SCAR of the rupture
Overview and Epidemiology
Proximal biceps tendon rupture predominantly involves the long head of the biceps (LHB). It is frequently a degenerative process associated with chronic shoulder impingement and rotator cuff disease.
Pathophysiology:
- The LHB tendon intra-articular portion is vascularly compromised and subject to shear forces.
- Usually occurs at the proximal bicipital groove entrance or near the supraglenoid tubercle.
- "Autotenotomy": Spontaneous rupture often relieves the deep anterior shoulder pain of chronic biceps tendinitis.
Consider proximal biceps rupture a marker of rotator cuff disease in patients over 40. In younger patients (under 30), it may be isolated trauma (weightlifting, contact sports), but this is much less common.
- Age over 40 (degenerative changes)
- History of rotator cuff tears (supraspinatus/subscapularis)
- Smoking
- Corticosteroid injections (weakens collagen)
- Overuse (overhead sports like tennis, swimming, baseball)
- Anabolic steroid use (in younger weightlifters)
The long head of the biceps often undergoes a process of inflammation (tendinitis) followed by degeneration (tendinosis) and eventual rupture. This "autotenotomy" can be the final stage of a painful process. Once ruptured, the irritating intra-articular portion of the tendon is no longer under tension, often leading to significant pain relief. However, the resulting weakness and deformity must be weighed against the risks of surgical reconstruction. The cosmetic deformity ("Popeye" sign) does not improve with time and is permanent unless surgically addressed.
Anatomy
The LHB originates from the supraglenoid tubercle and superior labrum. It exits the joint through the rotator interval, turning 90 degrees to enter the bicipital groove (intertubercular sulcus). This turn is a site of high stress and degeneration ('pulley lesion').
- Origin: Supraglenoid tubercle (40-60% from superior labrum).
- Transverse Humeral Ligament: Holds tendon in groove (continuation of subscapularis tendon).
- Bicipital Groove: Between greater and lesser tuberosities.
- Short Head: Originates from coracoid process (remains intact in LHB rupture).
- Insertion: Radial tuberosity (common tendon).
- Anterior circumflex humeral artery branches.
- Proximal intra-articular zone is relatively hypovascular ("watershed zone").
- Elbow Flexion: Secondary to brachialis.
- Forearm Supination: Primary supinator (with supinator muscle).
- Shoulder Stability: Depresses humeral head (minor role), anterior stabilizer.
LBSBiceps Anatomy and Function
Hook:LBS (Pounds) of force - Biceps lifts heavy things
Pathophysiology
The long head of biceps (LHB) tendon fails through a predictable degenerative cascade rather than a single traumatic event in most patients.
- Mechanical environment: The intra-articular LHB makes a near 90-degree turn at the rotator interval to enter the bicipital groove. This turn is a chronic shear and friction point ("pulley" zone).
- Vascular factors: The proximal intra-articular segment lies in a relative hypovascular watershed zone, limiting healing and predisposing to attritional degeneration.
- Degenerative sequence: Tenosynovitis (tendinitis) progresses to tendinosis with collagen disorganisation, then partial and finally complete rupture - typically near the supraglenoid tubercle or groove entrance.
- Impingement linkage: Subacromial impingement and rotator cuff disease accelerate LHB degeneration, which is why proximal rupture is a sentinel sign of cuff pathology over the age of 40.
- Instability mechanism: Because the transverse humeral ligament is reinforced by subscapularis fibres, a subscapularis tear allows the LHB to sublux/dislocate medially before it ruptures.
- "Autotenotomy": Once the tendon ruptures, the inflamed intra-articular pain generator is unloaded, which is why chronic anterior shoulder pain often improves after the rupture event.
Classification
Etiological Classification
- Mechanism
- Chronic wear/impingement
- Demographics
- Older (over 50)
- Associated Injuries
- Rotator cuff tears, Impingement
- Mechanism
- Sudden eccentric load
- Demographics
- Younger (under 40)
- Associated Injuries
- SLAP lesions, Labral tears
The Biceps Pulley and Medial Instability
The pathophysiology and classification refer to the "pulley lesion" and to medial subluxation with subscapularis tears — here is the pulley anatomy and the instability it governs.
- The reflection pulley. At the rotator interval the LHB is held at its turn into the groove by a fibrous sling — the biceps reflection pulley — formed by the superior glenohumeral ligament (SGHL) and coracohumeral ligament (CHL), reinforced anteriorly by fibres of subscapularis and posteriorly by supraspinatus.
- Why instability is (almost always) medial. Because the anterior wall of the pulley and groove is reinforced by the subscapularis, a subscapularis (with SGHL) tear lets the LHB sublux or dislocate medially — riding over or under the torn subscapularis — often before the tendon frankly ruptures. Medial biceps dislocation is therefore a strong indirect sign of a subscapularis tear.
- Classifying the lesion. Pulley lesions are commonly graded by the Habermeyer classification (types I-IV) according to which structures are involved (isolated SGHL, SGHL plus the supraspinatus side, SGHL plus the subscapularis side, or both), which predicts the pattern of biceps instability.
- Management. Address the unstable biceps (tenodesis or tenotomy) AND repair the subscapularis / anterior pulley — leaving the pulley or subscapularis lesion untreated allows persistent pain and re-subluxation. Detailed subscapularis repair is developed in the subscapularis-tears topic.
Q: A biceps tendon is dislocated medially out of the groove — what associated injury must you assume, and why medial? A: A subscapularis tear — the subscapularis reinforces the anterior wall of the biceps reflection pulley (SGHL/CHL sling), so its failure lets the LHB dislocate medially (over or under the subscapularis). Repair the biceps (tenodesis/tenotomy) AND the subscapularis; a medially dislocated biceps is a red flag for an occult subscapularis tear.
Clinical Assessment

- "Pop" or "snap" reduced pain
- Sharp initial pain, then ache
- Bruising down the arm
- History of prodromal shoulder pain
- Popeye Deformity: Muscle belly retracts distally
- Ecchymosis: Medial arm (tracks down gravity)
- Compare symmetry with uninjured side
Patients often report that their chronic shoulder pain improved after the acute rupture event. This is because the pain generator (the inflamed tendon) is no longer under tension within the joint/groove.
Special Tests (Pre-rupture / Contralateral): Tests are often negative AFTER complete rupture.
- Speed's Test: Pain with forward flexion against resistance (elbow extended, supinated).
- Yergason's Test: Pain with supination against resistance (elbow 90 deg). Specific for groove pathology.
- Ludington's Test: Hands on head, flex biceps. Palpate for absence of tendon (specific for rupture).
Investigations
Diagnostic Workup
- AP, Scapular Y, Axillary Lateral
- Usually normal for biceps
- Rule out underlying OA, fractures
- Look for high-riding humeral head (chronic massive RC tear)
- Excellent for tendons
- "Empty groove" sign
- Can assess dynamic subluxation
- Operator dependent
- Gold Standard for associated pathology
- Confirms empty groove
- Evaluates Rotator Cuff integrity (crucial for management)
- Evaluates Labrum (SLAP)
Look for the "empty groove" sign on axial MRI slices. The LHB tendon should be visualized within the bicipital groove. Absence indicates rupture or dislocation (check medially!).
Differential Diagnosis
The "Popeye" arm and acute anterior shoulder pain have a short but exam-relevant differential. The single most important distinction is proximal vs distal biceps rupture, because their management algorithms are opposite.
- Key Distinguishing Feature
- Older patient, mild pain, intact supination, sentinel for cuff disease
- Deformity Direction
- Belly migrates DISTALLY (low Popeye)
- Default Management
- Usually non-operative
- Key Distinguishing Feature
- Reverse Popeye, weak supination, positive hook test
- Deformity Direction
- Belly migrates PROXIMALLY (high bulge)
- Default Management
- Surgical repair in active patients
- Key Distinguishing Feature
- Tendon still present, groove tenderness, positive Speed/Yergason
- Deformity Direction
- No deformity
- Default Management
- Conservative, then tenodesis if refractory
- Key Distinguishing Feature
- Weak abduction/external rotation, positive lag signs
- Deformity Direction
- No biceps deformity (may coexist)
- Default Management
- Address cuff per tear pattern
- Key Distinguishing Feature
- Younger overhead athlete, deep clicking, positive O'Brien
- Deformity Direction
- No deformity
- Default Management
- Rehab; debridement/repair/tenodesis
The hook test differentiates distal biceps rupture: with the elbow flexed to 90 degrees and the forearm supinated, the examiner cannot hook a finger under an intact distal biceps tendon from the lateral side if it is ruptured. This is the bedside test that protects against missing a distal rupture, which needs surgery.
Management Algorithm
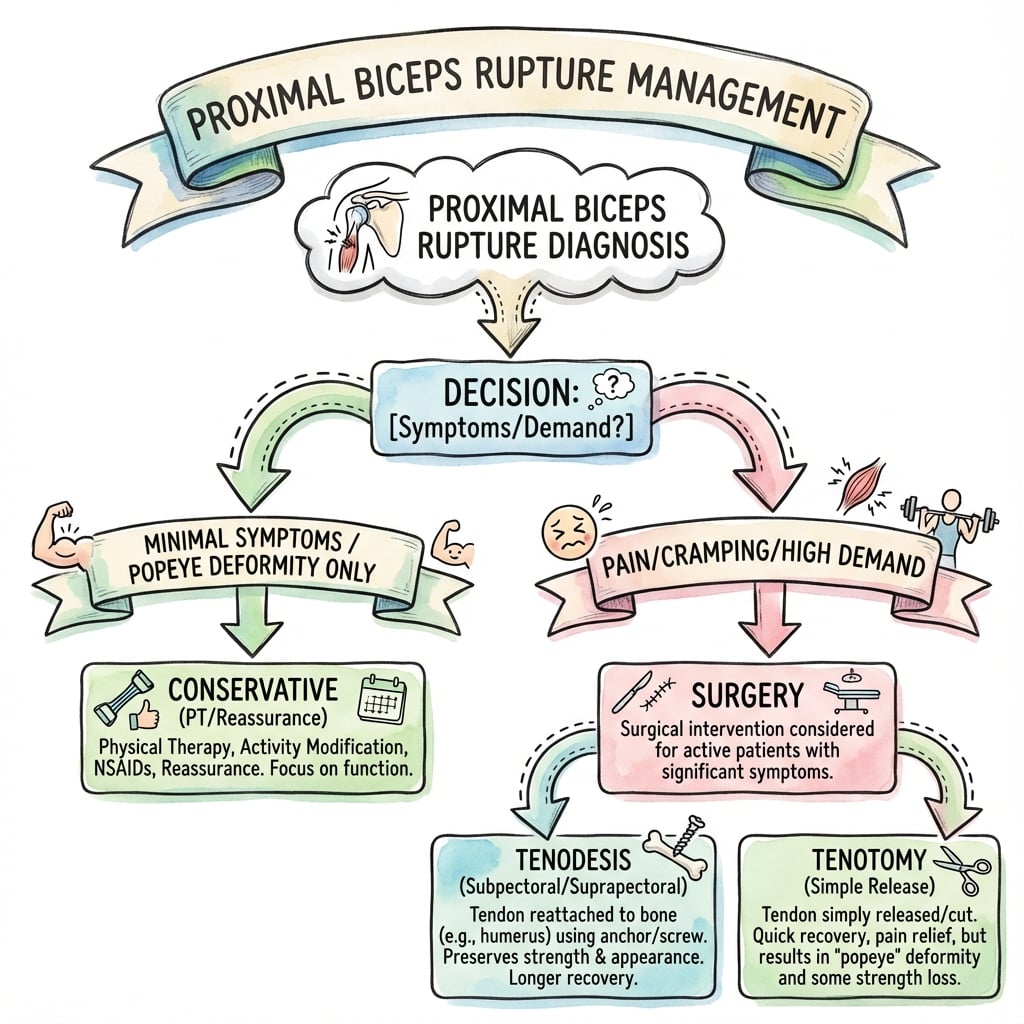
Treatment Selection
- Elderly / Low demand
- Willing to accept cosmetic deformity
- Minimal cramping/pain
- No repairable cuff pathology
- Young / High demand
- Unacceptable cosmesis (Popeye)
- Persistent cramping
- Undergoing surgery for Rotator Cuff anyway
Tenotomy: Cut the tendon. Fast, easy, no hardware. Risk: Deformity, cramping. Good for elderly/low demand. Tenodesis: Reattach tendon to humerus. Better cosmesis/strength. Risk: Failure, humerus fracture, pain. Good for young/active.
Surgical Technique
Tenodesis Approaches
- Supra-pectoral: Arthroscopic or open. High in the groove.
- Sub-pectoral: Open (mini-incision). Distal to groove.
- Position: Beach chair.
- Approach: Small incision in axillary fold, medial to pec major tendon.
- Identify: Locate tendon (often retracted). Retrieve.
- Preparation: Whipstitch distal end of tendon.
- Drilling: Drill hole in humerus (centered, unicortical or bicortical depending on fixator).
- Fixation: Interference screw, suture anchor, or cortical button.
- Tension: Restore physiologic tension (elbow 90, forearm supinated).
Removes tendon from groove (eliminates groove pain), strong fixation. Cons: Humerus fracture risk (torsion), neurovascular risk (musculocutaneous n.).
- Tenotomy
- Fast
- Tenodesis
- Longer
- Tenotomy
- Popeye Deformity
- Tenodesis
- Restored
- Tenotomy
- Slight Decrease
- Tenodesis
- Near Normal
- Tenotomy
- Immediate
- Tenodesis
- Protected
- Tenotomy
- Low
- Tenodesis
- Implants required
- Tenotomy
- Cramping
- Tenodesis
- Fracture/Fail/Pain
The Hourglass Biceps: A Mechanical Block to Elevation
The tenotomy technique warns about an "hourglass" biceps and the evidence base includes it — the entity deserves developing, because it changes the operation.
- What it is. A hypertrophic intra-articular segment of the long head of biceps that becomes too bulky to slide down into the bicipital groove when the arm is elevated. On elevation the tendon buckles and is squeezed (incarcerated) between the humeral head and glenoid — an intra-articular mechanical block, likened by Boileau to a bucket-handle meniscal tear locking the knee.
- How it presents. Anterior shoulder pain with a 10-20 degree loss of active AND passive elevation (a true mechanical block, not just weakness), usually with coexisting rotator cuff disease.
- How it is confirmed. The intraoperative "hourglass test" — forward elevation with the elbow extended reproduces the buckling and incarceration of the tendon within the joint.
- Why it changes management. Simple tenotomy at the origin does NOT relieve the block — the hypertrophic intra-articular portion is still incarcerated. The bulky intra-articular segment must be excised (a "bipolar" tenotomy) or removed as part of a tenodesis. Recognising it converts an unexplained stiff, painful shoulder into a treatable mechanical lesion.
Q: A patient has anterior shoulder pain and a fixed 10-20 degree loss of elevation from a hypertrophic intra-articular biceps — why is simple tenotomy insufficient? A: This is an hourglass biceps — the bulky intra-articular tendon cannot slide into the groove and incarcerates between the humeral head and glenoid (a mechanical block, like a locked knee). Releasing it at the origin leaves the hypertrophic segment stuck in the joint, so the block persists; the intra-articular portion must be excised (bipolar tenotomy or tenodesis with excision).
Complications
- Risk Factor
- Tenotomy
- Management
- Accept or Tenodesis if symptomatic
- Risk Factor
- Tenotomy
- Management
- Physio, stretching, late tenodesis
- Risk Factor
- Tenodesis (Screw)
- Management
- ORIF
- Risk Factor
- Retractor placement
- Management
- Explore/Repair
- Risk Factor
- Poor bone quality
- Management
- Revision or Conversion to Tenotomy
- Risk Factor
- Prolonged immobilization
- Management
- Physio/MUA
In sub-pectoral tenodesis, vigorous medial retraction can injure the musculocutaneous nerve. The nerve enters the coracobrachialis medial to the operative field.
CCCComplications of Tenotomy
Hook:Tenotomy is simple but has 3 C's
Postoperative Care
Rehab Protocol (Tenodesis)
- Sling for comfort (wean earlier than RC repair)
- Passive elbow flexion
- No active elbow flexion against resistance
- Passive shoulder ROM
- Active assist range of motion
- Begin light active flexion
- No lifting heavier than 1-2 lbs
- Full active ROM
- Progressive resistance training (biceps curls)
- Gradual return to activities
- Unrestricted activity
- Return to sport
Note for Tenotomy: Immediate active ROM is allowed as tolerated. No specific restrictions other than pain.
Outcomes and Prognosis
Evidence summary (consolidated from Level I RCTs and meta-analyses):
- Functional scores equivalent — ASES, WORC and Constant-Murley scores do not differ between tenotomy and tenodesis in pooled Level I data.
- Popeye deformity is the one reproducible difference — roughly 23-33% after tenotomy vs 7-10% after tenodesis.
- Strength — most RCTs show no difference in elbow flexion or supination strength; only isolated trials show marginally higher supination strength after tenodesis (clinical relevance debated).
- Cramping — historically attributed to tenotomy, but high-level RCTs found cramping rates similar between groups.
- Trade-offs — tenotomy is faster with simpler rehab; tenodesis better preserves cosmesis at the cost of operative time, implant cost and the specific risks below.
Guidelines, Registries & Global Practice
Global epidemiology
- Long head of biceps (LHB) pathology is found in a high proportion of rotator cuff tears at surgery; isolated LHB rupture in patients over 40 is widely regarded as a sentinel sign of cuff disease.
- Peak incidence is the 5th-6th decade, predominantly in men and manual or overhead workers.
- Distal ruptures are far rarer than proximal and occur in younger, often muscular men with sudden eccentric load.
Side-by-side guidance
- Imaging stance
- MRI/US to define associated cuff and labral pathology, not for an obvious clinical Popeye
- Treatment emphasis
- Shared decision-making; tenotomy and tenodesis both acceptable
- Imaging stance
- Reserve advanced imaging for surgical planning or diagnostic doubt
- Treatment emphasis
- Non-operative default in low-demand; tenodesis for cosmesis/strength concerns
- Imaging stance
- Focus on concomitant cuff/instability rather than the LHB in isolation
- Treatment emphasis
- Address the LHB at the time of cuff or instability surgery
- Imaging stance
- US first-line in many centres (cheaper, dynamic), MRI for full work-up
- Treatment emphasis
- Procedure choice driven by patient demand and deformity tolerance
Practice variation by resource setting
- High-resource settings: ready MRI access, arthroscopic suprapectoral or open subpectoral tenodesis with implants, formal physiotherapy pathways.
- Limited-resource settings: ultrasound or clinical diagnosis predominate; non-operative management and, when surgery is indicated, arthroscopic tenotomy (no implant cost, immediate rehab) are favoured. The functional equivalence shown in RCTs makes tenotomy a defensible, cost-effective default where implants are scarce.
Controversies & Areas of Uncertainty
Level I RCTs agree function is equivalent; the only consistent difference is Popeye deformity. The unresolved question is whether the small supination-strength and cramping signals are clinically meaningful. Most surgeons reserve tenodesis for younger, leaner, high-demand or cosmesis-conscious patients.
Older series attributed disabling cramping to tenotomy, but blinded RCTs (MacDonald 2020) found no difference in cramping between groups. Cramping may be less procedure-specific than classically taught.
No clear functional winner. Subpectoral fixation moves the tenodesis distal to the groove (theoretically eliminating residual groove pain) but adds a second incision and neurovascular exposure. Suprapectoral arthroscopic fixation is associated with more postoperative stiffness in some series (Werner, Arthroscopy 2014).
Interference screws create a torsional stress riser - cadaveric torsion testing fractured 100% of screw-tunnel specimens (Frank 2019). Suture anchors and the smallest adequate screw reduce this risk, but no high-level clinical trial proves one construct superior in vivo.
MCQ Practice Points
Q: Which nerve is most at risk during open sub-pectoral biceps tenodesis? A: The Musculocutaneous Nerve. It enters the coracobrachialis muscle medial to the operative field and is vulnerable to vigorous medial retraction.
Q: What is the expected functional deficit after non-operative management of a proximal biceps rupture? A: Approximately 10-20% loss of supination strength and endurance. Elbow flexion strength is largely preserved due to the intact brachialis.
Q: What does a positive Yergason's test indicate? A: It indicates pathology of the LHB in the bicipital groove or instability of the transverse humeral ligament. It is performed by resisting supination with the elbow at 90 degrees.
Q: A patient presents with a 'Popeye' deformity. Where has the tendon likely ruptured? A: Proximal Long Head of Biceps. The muscle belly retracts distally, creating a prominent bulge in the lower arm. Distal biceps ruptures cause the muscle to retract proximally.
Q: What is the most appropriate imaging to rule out associated pathology in a 60-year-old? A: MRI of the Shoulder. This is the gold standard to evaluate the rotator cuff (supraspinatus/subscapularis), which is torn in a high percentage of elderly patients with biceps rupture ("Sentinel Sign").
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 72-year-old male presents with sudden arm pain and bruising 2 weeks ago while gardening. Now pain has settled, but he notices a bulge in his arm. He has full range of motion. Examination reveals a Popeye deformity. How do you manage him?”
“A 28-year-old bodybuilder feels a snap doing heavy deadlifts. Acute pain anterior shoulder. MRI shows complete LHB rupture and superior labral tear. He is worried about appearance and strength.”
“You performed a rotator cuff repair and biceps tenotomy on a 55-year-old carpenter 6 months ago. He is happy with the shoulder, but complains of painful cramping in the biceps muscle belly after repetitive hammering. It is affecting his work.”
“A 35-year-old weightlifter had a subpectoral biceps tenodesis 6 weeks ago. While doing a heavy eccentric curl against advice, he felt a painful 'pop' and noticed the muscle belly retract distally again. He is distraught about the appearance. What happened and how do you manage it?”
Key Anatomy
- Origin: Supraglenoid tubercle
- Groove: Intertubercular sulcus
- Function: Supinator dominant vs Flexor
- Nerve: Musculocutaneous (C5-6)
Clinical Signs
- Popeye Deformity (distal bunching)
- Ecchymosis (medial arm)
- Ludington's test positive
- Usually painless after acute phase
Management Rules
- Elderly/Low Demand to Non-operative
- Young/High Demand to Tenodesis
- Cuff Repair to Tenotomy or Tenodesis
- Cosmetic concern to Tenodesis
Tenotomy vs Tenodesis
- Tenotomy: Fast, easy, safe, but deformity/cramps
- Tenodesis: Strong, cosmetic, but longer rehab/risks
- Evidence: Equal functional scores
- Rehab: Immediate (Tenotomy) vs Protected (Tenodesis)
Surgical Risks
- Deformity (Tenotomy)
- Cramping (Tenotomy)
- Humerus Fracture (Tenodesis)
- Musculocutaneous Nerve Injury
Key Exam Pearls
- Always check Rotator Cuff - sentinel sign of cuff disease
- Distal rupture DIFFERENT - needs surgical repair
- Minimal functional loss - short head compensates
- Cosmesis main concern - counsel pre-op
Evidence Base
- Prospective double-blind RCT, 114 patients (mean age 57.7), LHB lesions at arthroscopy.
- ASES and WORC scores improved equally; no difference between groups at 24 months.
- Popeye deformity 33% (tenotomy) vs 10% (tenodesis); relative risk 3.5 (95% CI 1.26-9.70).
- No difference in elbow flexion or supination strength; cramping equivalent; all tenodeses intact on 1-year MRI.
- Systematic review of 5 Level I RCTs: 236 tenodesis vs 232 tenotomy patients, mean follow-up 23 months.
- Cosmetic deformity 6.8% (tenodesis) vs 23.3% (tenotomy), P less than 0.001.
- No difference in ASES, VAS pain, or Constant-Murley scores; only one RCT showed greater supination strength after tenodesis.
- No difference in overall complication rates at latest follow-up.
- Meta-analysis of 7 studies, 622 subjects.
- Tenodesis: higher Constant score (P=0.02), lower Popeye rate (P less than 0.001), less cramp pain (P=0.04).
- Tenotomy: shorter surgical time (P less than 0.001).
- Overall complication rate lower with tenodesis in this cohort.
- Systematic review of 16 studies (Level II-IV): 433 tenodesis and 699 tenotomy procedures.
- Excellent/good outcome 74% (tenodesis) vs 77% (tenotomy) - clinically comparable.
- Cosmetic deformity 8% (tenodesis) vs 43% (tenotomy).
- Postoperative bicipital pain 24% (tenodesis) vs 19% (tenotomy).