Congenital Femoral Deficiency | Aitken Classification | Limb Length Discrepancy | Reconstruction vs Rotationplasty
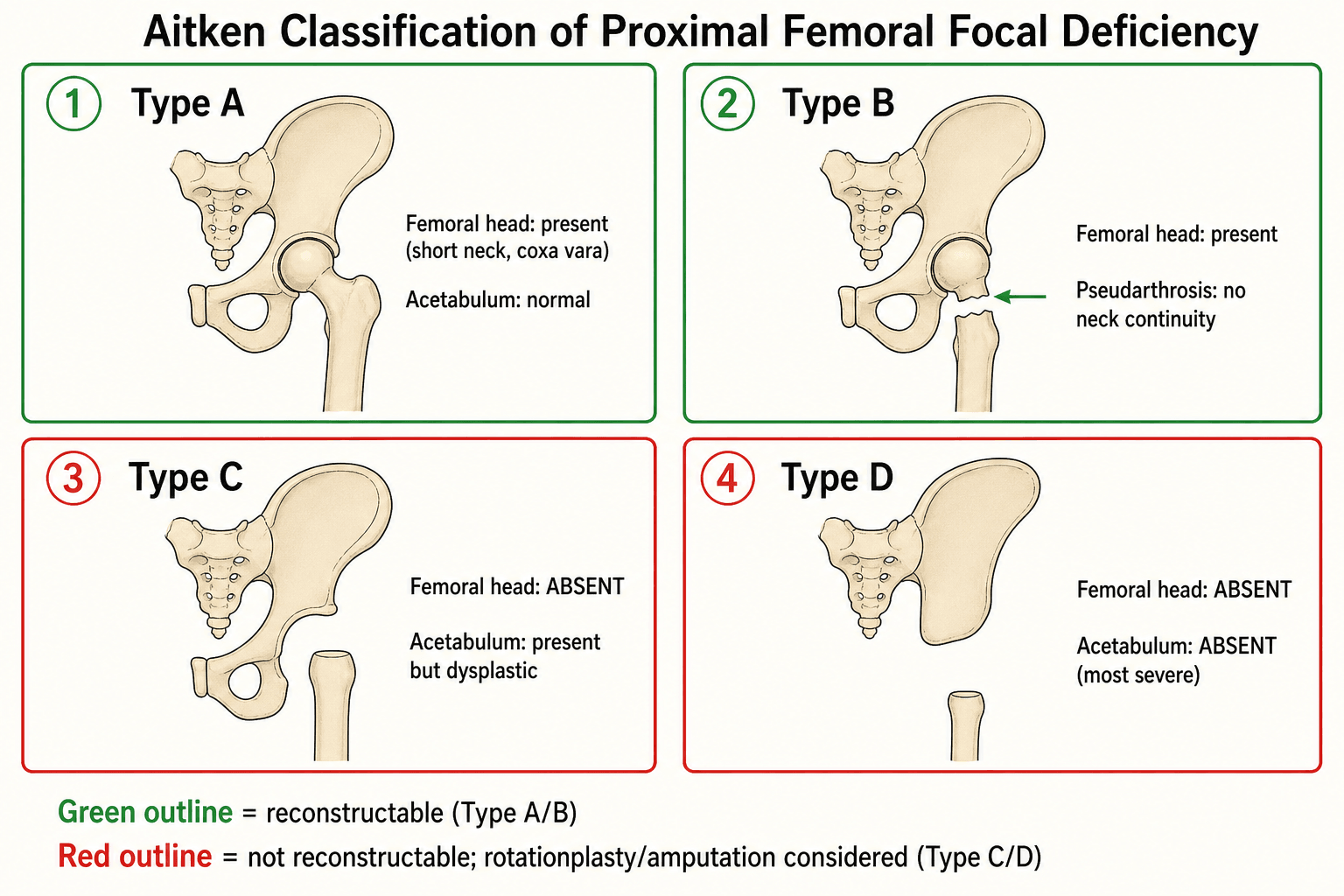
- Aitken classification determines treatment: Type A/B = reconstruction, Type C/D = rotationplasty/amputation
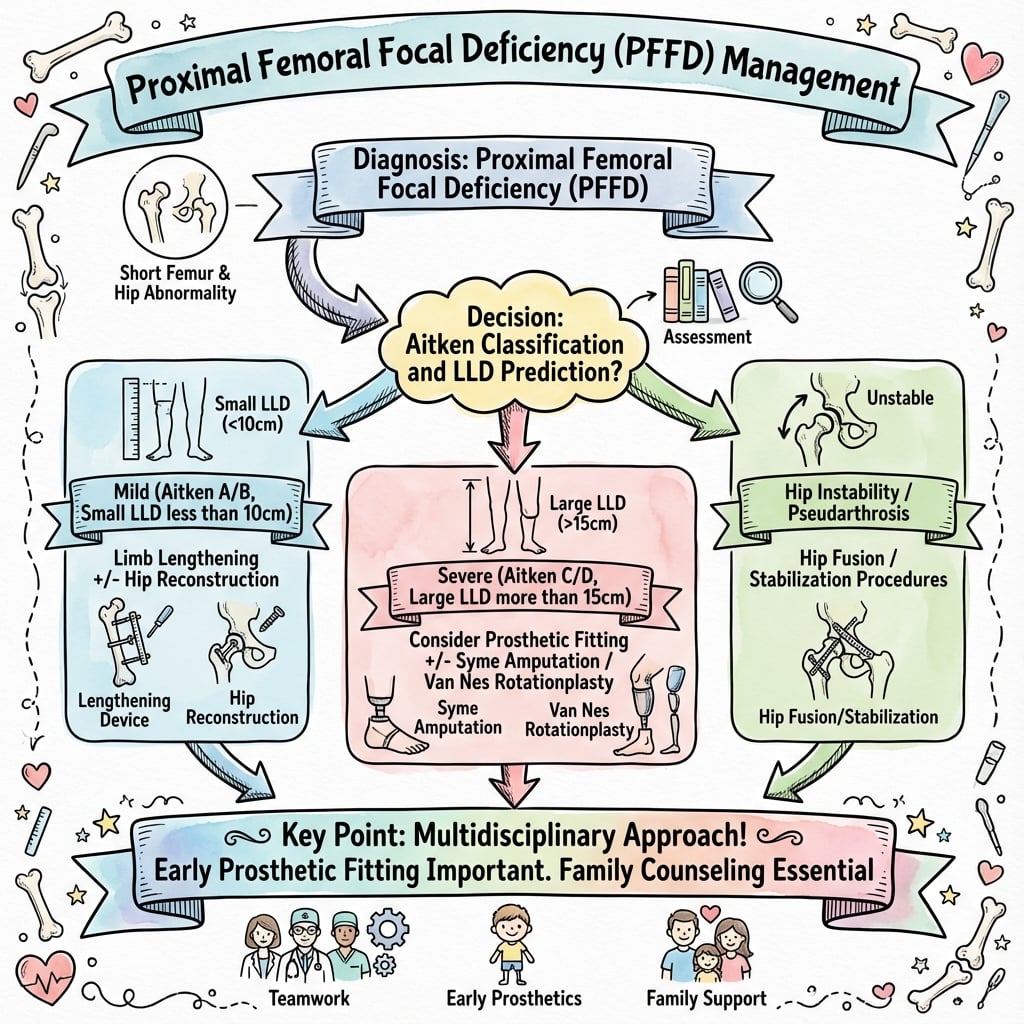
- Limb length discrepancy is the main problem - predict final LLD using multiplier method or Paley method
- Reconstruction options: Pelvic-femoral stabilization, femoral lengthening, hip reconstruction with osteotomy
- Rotationplasty (Van Nes/Winkelmann) converts ankle to knee - preserves an active joint, but contemporary gait/PRO data question its superiority over amputation
- Associated anomalies: Fibular (postaxial) deficiency (~50%), cruciate ligament deficiency, foot anomalies
- “Aitken classification is high-yield - know all 4 types and treatment implications
- “Type A/B have femoral head = reconstruction possible. Type C/D lack femoral head = rotationplasty/amputation
- “Rotationplasty repurposes the ankle as a knee; the JBJS 2021 comparison found no gait/PRO benefit over amputation despite more surgery - decision must be individualised
- “Limb length discrepancy prediction is critical - use the Paley multiplier method
Type A/B have femoral head = reconstruction possible (pelvic-femoral stabilization, lengthening). Type C/D lack femoral head = rotationplasty or amputation. Classification based on presence of femoral head and acetabulum.
LLD increases with growth - predict final discrepancy using multiplier method or Paley method. Severe cases (over 15cm) may need rotationplasty. Reconstruction aims to minimize LLD while maintaining function.
Van Nes/Winkelmann rotationplasty rotates the limb 180 degrees so the ankle drives an active prosthetic knee. Traditionally favoured for an active joint, but a JBJS 2021 comparison found no gait, energy or patient-reported advantage over amputation despite more surgery. Indicated for Type C/D or severe predicted LLD - decision is individualised.
50% have fibular hemimelia, cruciate ligament deficiency, foot anomalies. Always assess entire limb. May affect treatment choice (e.g., fibular hemimelia may favor rotationplasty).
- Femoral Head
- Present
- Acetabulum
- Present
- Treatment Options
- Reconstruction: pelvic-femoral stabilization, lengthening
- Femoral Head
- Present
- Acetabulum
- Present
- Treatment Options
- Reconstruction: osteotomy + stabilization, lengthening
- Femoral Head
- Absent
- Acetabulum
- Present
- Treatment Options
- Rotationplasty or amputation
- Femoral Head
- Absent
- Acetabulum
- Absent
- Treatment Options
- Rotationplasty or amputation
FACTSPFFD Associated Anomalies
Hook:FACTS about PFFD: Fibular hemimelia, ACL deficiency, Coxa vara, Tarsal anomalies, and Short femur are all associated findings!
CARSRotationplasty Indications
Hook:CARS drive rotationplasty: C/D type, Ankle function, Residual LLD over 15cm, and Stable knee are key indications!
Overview and Epidemiology
Proximal femoral focal deficiency (PFFD) is a rare congenital condition characterized by partial or complete absence of the proximal femur. It represents a spectrum of femoral deficiency ranging from mild shortening with coxa vara to complete absence of the proximal femur and acetabulum.

- Incidence: 1 in 50,000 live births
- Male to female ratio: 1:1
- Bilateral involvement: 15% of cases
- Left side more commonly affected than right
- No clear genetic inheritance pattern (sporadic)
PFFD results from failure of normal development of the proximal femur during embryogenesis (4-8 weeks gestation). The exact cause is unknown but may involve:
- Vascular insult during development
- Teratogenic exposure
- Genetic factors (rare familial cases reported)
- Failure of mesenchymal condensation
The condition represents a spectrum, with Aitken classification describing the severity based on presence of femoral head and acetabulum.
Pathophysiology and Mechanisms
The proximal femur develops from mesenchymal condensation at 4-6 weeks gestation. The femoral head, neck, and greater trochanter develop from separate ossification centers that fuse during childhood.
In PFFD, there is failure of normal development of the proximal femur, resulting in:
- Shortened or absent proximal femur
- Coxa vara deformity (Type A)
- Pseudarthrosis at neck (Type B)
- Absent femoral head (Type C/D)
- Dysplastic or absent acetabulum (Type D)
- Associated soft tissue deficiencies (muscles, ligaments)
- Fibular hemimelia (50% of cases)
- Cruciate ligament deficiency (common)
- Foot anomalies (tarsal coalition, equinovarus)
- Patellar anomalies
- Tibial shortening (less common than fibular)
Understanding the anatomy helps determine reconstruction feasibility and treatment planning.
Classification Systems
Aitken Classification (1969)
The Aitken classification is the most widely used system, based on radiographic appearance of the femoral head and acetabulum:
- Femoral Head
- Present
- Femoral Neck
- Short, coxa vara
- Acetabulum
- Normal
- Treatment
- Reconstruction
- Femoral Head
- Present
- Femoral Neck
- Absent, pseudarthrosis
- Acetabulum
- Normal
- Treatment
- Reconstruction with osteotomy
- Femoral Head
- Absent
- Femoral Neck
- Absent
- Acetabulum
- Present but dysplastic
- Treatment
- Rotationplasty/amputation
- Femoral Head
- Absent
- Femoral Neck
- Absent
- Acetabulum
- Absent
- Treatment
- Rotationplasty/amputation
Type A: Best prognosis. Femoral head present but delayed ossification. Short neck with coxa vara. Acetabulum normal. Reconstruction possible with pelvic-femoral stabilization and lengthening.
Type B: Femoral head present but no neck continuity (pseudarthrosis). Acetabulum present. Reconstruction requires osteotomy to establish continuity, then lengthening.
Type C: No femoral head. Acetabulum present but dysplastic. Reconstruction not feasible. Rotationplasty or amputation indicated.
Type D: Most severe. No femoral head, no acetabulum. Rotationplasty or amputation only options.
The classification determines treatment options and prognosis.
Clinical Assessment
- Shortened lower limb noted at birth or early infancy
- Delayed walking (if unilateral, may walk with limp)
- Difficulty with activities requiring equal leg length
- Family history (rare but may be present)
Physical Examination
- Shortened thigh (proximal deficiency)
- Flexed, abducted, externally rotated hip (pseudarthrosis position)
- Knee may be flexed (compensation)
- Foot position (assess for associated anomalies)
- Compare to contralateral side
- Proximal femur may be absent or very short
- Greater trochanter may be palpable (Type A/B) or absent (Type C/D)
- Assess hip stability
- Knee stability (cruciate deficiency common)
- Hip: Limited flexion, abduction
- Knee: May have hyperextension or flexion contracture
- Ankle: Assess for equinus or other deformities
- True leg length: ASIS to medial malleolus
- Apparent leg length: umbilicus to medial malleolus
- Thigh length: greater trochanter to lateral joint line
- Predict final LLD using multiplier method or Paley method
- Usually normal
- Assess femoral nerve function (may be affected in severe cases)
Investigations
- Assess presence of femoral head (may be delayed ossification in Type A)
- Evaluate acetabulum (present, dysplastic, or absent)
- Measure coxa vara angle (Type A)
- Identify pseudarthrosis (Type B)
- Measure limb length discrepancy
- Assess alignment
- Evaluate for associated anomalies (fibular hemimelia, tibial shortening)
- Assess unossified femoral head (Type A - may appear absent on X-ray but present on MRI)
- Evaluate acetabular cartilage
- Assess soft tissue structures (muscles, ligaments)
- May identify unossified femoral head
- Assess hip stability
- Multiplier method: Current LLD × multiplier for age/sex = predicted final LLD
- Paley method: More complex, accounts for growth remaining
- Usually not indicated (sporadic)
- Consider if bilateral or family history present
Differential Diagnosis
The shortened, abnormally positioned thigh of PFFD overlaps with several other causes of a congenitally short femur or limb-length discrepancy. The discriminator is the state of the proximal femur, hip and the rest of the limb.
- Proximal Femur / Hip
- Deficient or absent proximal femur; coxa vara, pseudarthrosis or absent head
- Distinguishing Features
- Short, flexed-abducted-externally rotated thigh; ~50% with fibular deficiency
- Key Clue
- Bulky proximal thigh with very short femoral segment
- Proximal Femur / Hip
- Femur present, hip stable, head present
- Distinguishing Features
- Diffuse mild shortening, may have anterolateral bow, no pseudarthrosis
- Key Clue
- Whole femur short but in continuity
- Proximal Femur / Hip
- Femur often near-normal proximally
- Distinguishing Features
- Lateral foot rays/fibula deficient, ball-and-socket ankle, anteromedial tibial bow
- Key Clue
- Foot/ankle anomaly dominates; coexists with PFFD
- Proximal Femur / Hip
- Femur normal length; dysplastic/dislocated hip
- Distinguishing Features
- Galeazzi positive from hip not femoral deficiency; femoral length symmetric
- Key Clue
- Limb-length difference is apparent, not true femoral loss
- Proximal Femur / Hip
- Acquired, prior history
- Distinguishing Features
- Physeal damage, AVN; no congenital dysmorphism
- Key Clue
- History of sepsis/trauma/AVN
Management Algorithm
Treatment Philosophy
Treatment goals:
- Maximize function and independence
- Minimize limb length discrepancy
- Maintain hip stability
- Optimize prosthetic fitting (if needed)
Treatment options:
- Reconstruction: Pelvic-femoral stabilization, lengthening (Type A/B)
- Rotationplasty: Van Nes procedure (Type C/D or severe LLD)
- Amputation: Knee disarticulation or above-knee (Type C/D, failed reconstruction)
- Prosthetic fitting: For any option with significant LLD
Choice depends on Aitken type, predicted LLD, associated anomalies, and family preference.
ROADPFFD Treatment Options
Hook:ROAD to treatment: Reconstruction for A/B, Osteotomy for B, Amputation for C/D, and Distraction for lengthening!
Surgical Techniques
Pelvic-Femoral Stabilization
Type A/B with unstable hip or need for reconstruction.
- Approach: Anterior iliofemoral or extended Smith-Peterson
- Exposure: Proximal femur and acetabulum
- Preparation:
- Acetabulum: Ream to create socket if needed
- Femur: Prepare proximal end
- Stabilization:
- Create continuity between femur and pelvis
- May use bone graft
- Internal fixation (plates, screws)
- Position: Hip in functional position (flexion, slight abduction)
Spica cast 6-12 weeks, then protected weight-bearing.
The SUPERhip Procedure: Reconstructing the Deficient Proximal Femur
Several parts of this topic assume the deficient hip can be "reconstructed" before lengthening, and the Global Practice table names "SUPERhip-type" strategies - but the operation itself is worth defining, because it is the workhorse that makes reconstruction of a Paley type 1b hip possible.
SUPERhip stands for the Systematic Utilitarian Procedure for Extremity Reconstruction of the hip, developed by Paley in 1997 for congenital femoral deficiency with a mobile hip but a severely deformed proximal femur (Paley type 1b: coxa vara with a very low neck-shaft angle, delayed ossification of the femoral neck/subtrochanteric region, and extra-articular hip contractures). It is a single-stage operation performed before any femoral lengthening, and it systematically addresses every component of the deformity:
- Release of the extra-articular contractures (the flexion-abduction-external-rotation posture) to mobilise the hip
- Subtrochanteric valgus and derotation osteotomy to correct the coxa vara and restore the neck-shaft angle toward normal (the Violante 2024 series improved the mean neck-shaft angle from about 72 to 133 degrees)
- Abductor rebalancing / greater-trochanteric advancement to restore the abductor lever arm and reduce a Trendelenburg gait
- Correction of associated acetabular dysplasia where present, to create a stable, congruent hip
The dominant late problems are recurrent coxa vara and persistent delayed ossification of the femoral neck. Paley's series of 72 type 1b hips required revision in nearly half of the early cases; recurrence fell significantly only when a fixed-angle internal-fixation device was used to hold the correction, combined with BMP-2 placed in the un-ossified neck cartilage to induce ossification (a non-fixed rush-rod repeatedly lost correction). Only once a stable, ossified, well-aligned hip is achieved does staged femoral lengthening proceed - reconstruction of the hip is the foundation, not a substitute, for equalising limb length.
The SUPERhip (Systematic Utilitarian Procedure for Extremity Reconstruction of the hip) corrects the proximal-femoral pathoanatomy of Paley type 1b CFD - coxa vara, delayed neck ossification and hip contractures - as a prerequisite to lengthening, not instead of it. Remember its two Achilles heels: recurrent coxa vara (mitigated by a fixed-angle device) and persistent neck non-ossification (mitigated by BMP-2). Detailed rotationplasty and pure distraction-lengthening technique are owned by the dedicated Rotationplasty and Limb Lengthening Principles topics.
The Equinus (Extension) Prosthesis: the Non-Operative Pathway
The management options above - reconstruction, rotationplasty and amputation - are all surgical, yet the landmark gait study underpinning this topic (Floccari 2021) included a distinct non-operative group treated with an equinus prosthesis, an option that is easy to forget in the exam.
In a child whose deficiency is milder, or whose family declines surgery, the intact foot is left in place and held in maximal equinus (plantarflexion) inside a custom extension prosthesis. The plantarflexed foot then behaves like a short, end-bearing Syme-level residual limb: it delivers distal weight-bearing and length, while a prosthetic knee mechanism is built into the socket below the foot. No bone is cut and no growth plate is sacrificed, so it is fully reversible and keeps all reconstructive and ablative options open as the child grows.
The trade-offs are honest ones for a viva:
- The prosthesis is bulky and cosmetically longer than the sound side, and the retained foot sits high, so it cannot drive a slim below-knee-style limb
- A fixed equinus foot is prone to skin/pressure problems, and the socket needs frequent revision with growth
- Crucially, it is not functionally inferior: in Floccari's series the equinus-prosthesis group actually walked the fastest (about 97 percent of normal cadence for age) and had PODCI pain, function and happiness scores no different from the rotationplasty and Syme-amputation groups, while undergoing the fewest operations (mean 0.7 procedures)
Beside reconstruction, rotationplasty and amputation, the equinus (extension) prosthesis is a legitimate non-operative pathway: the plantarflexed foot is retained as an end-bearing "residual limb" inside an extension socket with a built-in prosthetic knee. It avoids all surgery, is reversible, and - per Floccari 2021 - delivered the fastest walking speed with equal patient-reported outcomes despite the fewest operations. It reinforces the topic's central message that management is individualised and family-centred, not a fixed ladder. Generic socket/knee-unit component detail is owned by the Prosthetic Limb Components topic.
Complications
- Infection (5-10%)
- Wound healing problems
- Neurovascular injury (rare but devastating)
- Fixation failure
- Hip instability (recurrent subluxation/dislocation)
- Stiffness (hip, knee)
- Contractures (flexion, abduction)
- Limb length discrepancy recurrence (growth asymmetry)
- Delayed union/nonunion (osteotomy sites)
- Hardware problems (loosening, breakage)
- Pin site infection (common, usually minor)
- Stiffness (knee most common)
- Contractures (flexion, equinus)
- Delayed union (prolonged consolidation)
- Premature consolidation (stops lengthening)
- Nerve injury (peroneal most common)
- Vascular compromise (rare)
- Refracture after fixator removal
- Wound healing problems
- Neurovascular injury
- Malrotation (incorrect rotation angle)
- Nonunion
- Prosthetic fitting problems
- Careful preoperative planning
- Appropriate patient selection
- Meticulous surgical technique
- Aggressive physical therapy
- Close monitoring during lengthening
Postoperative Care
- Pain management
- Neurovascular monitoring
- Wound care
- Immobilization (cast, splint, external fixator)
- Spica cast 6-12 weeks
- Protected weight-bearing 3-6 months
- Physical therapy for range of motion
- Gradual return to activities
- Pin site care (daily cleaning)
- Distraction protocol (1mm/day)
- Physical therapy (critical for preventing stiffness)
- Regular radiographs (weekly during distraction, monthly during consolidation)
- Monitor for complications
- Cast 6-8 weeks
- Wound monitoring
- Prosthetic fitting after healing
- Gait training
- Annual assessment until skeletal maturity
- Monitor LLD progression
- Assess function and quality of life
- Address complications as they arise
Outcomes and Prognosis
- Reproducible radiographic correction of coxa vara/acetabular dysplasia (neck-shaft angle commonly restored toward normal; Violante 2024)
- Usually requires multiple staged procedures (hip reconstruction then lengthening)
- Final residual LLD often managed with limited lengthening plus shoe raise
- Hip stability achievable in most reconstructable hips
- Complication rates higher in children under 5 years
- Rotationplasty: durable pain-free outdoor ambulation; high appearance acceptance in selected patients (Kowalczyk 2018)
- Contemporary comparison shows no measurable gait/energy/PRO advantage over amputation (Floccari 2021)
- Both pathways need lifelong prosthetic care with revisions as the child grows
- Shared decision-making and family counselling are central
- Most patients adapt well
- Sports participation possible (with modifications)
- Vocational outcomes generally good
- Psychosocial support important
- Severe associated anomalies (fibular hemimelia, foot problems)
- Bilateral involvement
- Multiple complications
- Poor compliance with rehabilitation
- Most patients function independently
- May develop hip or knee arthritis (reconstruction)
- Prosthetic needs may change with growth
Guidelines, Registries & Global Practice
Global Epidemiology:
- PFFD/congenital femoral deficiency is rare, with frequently quoted incidence around 1 in 50,000 to 1 in 200,000 live births
- Mostly sporadic and unilateral; bilateral involvement in roughly 10-15% (more often bilateral when associated with broader limb-deficiency syndromes)
- Strong association with ipsilateral fibular (postaxial) longitudinal deficiency in around half of cases
- Population registry data are scarce: a Finnish national malformation/care registry captured all 185 lower-limb-deficiency live births over 1993-2008, confirming the heavy hospital and surgical burden of long-bone deficiencies relative to the general paediatric population (Syvanen 2018)
Side-by-Side Practice (no single global guideline exists):
- Reconstruction-led centres
- Paley functional classification to plan reconstruction
- Prosthetic/amputation-led centres
- Aitken descriptive grade plus functional assessment
- Common ground
- Both record femoral-head presence and hip stability
- Reconstruction-led centres
- Hip reconstruction + staged lengthening (e.g. SUPERhip-type)
- Prosthetic/amputation-led centres
- Early Syme/knee-disarticulation or rotationplasty + prosthesis
- Common ground
- Stabilise the hip and equalise/manage LLD
- Reconstruction-led centres
- Attempt reconstruction in selected cases
- Prosthetic/amputation-led centres
- Rotationplasty vs amputation, shared decision
- Common ground
- Functional ankle is prerequisite for rotationplasty
- Reconstruction-led centres
- Motorized plate / external fixation (avoid IM nail)
- Prosthetic/amputation-led centres
- Defer lengthening; prosthetic management
- Common ground
- IM nails risk femoral-head AVN before maturity
- No implant-survival registry applies directly to PFFD (it is a reconstruction/prosthetic, not arthroplasty, problem)
- Outcome data come from single-centre series and gait laboratories; there is no level-1 trial comparing reconstruction, rotationplasty and amputation
- Limb Lengthening and Reconstruction Society outcome indices (e.g. the angular-deformity/infection/motion score) are used to standardise lengthening complications
- High-resource settings: MRI for unossified head, motorized internal lengthening implants, formal gait analysis, multidisciplinary limb-deficiency clinics
- Limited-resource settings: reliance on plain radiographs and clinical prediction, external fixation (lower implant cost but higher pin-site burden), earlier prosthetic conversion where staged reconstruction is impractical; prosthetic availability and follow-up for growth-related revisions are the rate-limiting factors
paediatric orthopaedic/limb-reconstruction surgeon, physiotherapist (critical during lengthening), occupational therapist, prosthetist/orthotist, and psychological/social support for child and family. Informed consent must cover the multi-operation, long-term commitment and realistic, evidence-honest expectations.
Controversies & Areas of Uncertainty
PFFD management is one of the more genuinely contested areas in paediatric limb reconstruction. Examiners reward candidates who can hold the uncertainty rather than reciting dogma.
-
Rotationplasty versus amputation. The long-held belief that rotationplasty is functionally superior has been challenged. The JBJS 2021 gait-analysis comparison found no advantage in oxygen cost, gait deviation index or patient-reported outcomes over Syme amputation with a prosthetic knee, despite more operations. The counterpoint is that rotationplasty preserves an active joint with good long-term acceptance (Kowalczyk 2018) and durable, energy-efficient gait at very long follow-up in rotationplasty cohorts overall (Krebbekx 2026). The honest position: individualised, family-centred decision-making.
-
Reconstruction/lengthening versus prosthetic management. With modern hip reconstruction and serial lengthening (SUPERhip-type strategies, motorized implants), some severe deficiencies once destined for amputation are now reconstructed. Critics note the burden of multiple operations, complications and uncertain long-term durability. There is no level-1 evidence comparing a full reconstructive pathway against early prosthetic conversion.
-
Classification: Aitken versus Paley. Aitken is descriptive and widely known but does not directly guide reconstruction feasibility. The Paley classification is function- and reconstruction-oriented and increasingly used in lengthening centres. Candidates should know both and why the field is shifting.
-
Implant choice in the young child. Intramedullary lengthening nails carry a femoral-head AVN risk in skeletally immature children, so external fixation or motorized expandable plates are used instead - but the plate evidence is early (small case series; Georgiadis 2022).
-
Terminology. "Fibular hemimelia" is increasingly regarded as inaccurate; some authors prefer "postaxial/fibular longitudinal deficiency" and group PFFD with associated fibular and midline metatarsal deficiencies as a single dysvascular spectrum.
MCQ Practice Points
Q: Which Aitken type of PFFD has a femoral head present but no femoral neck continuity (pseudarthrosis)? A: Type B - Type B has a femoral head present with a pseudarthrosis at the neck level. Type A has a short neck with coxa vara. Type C and D lack the femoral head entirely.
Q: What is the main indication for rotationplasty in PFFD? A: Aitken Type C or D (no femoral head) or severe predicted limb length discrepancy (over 15-20cm), with a functional ankle. Rotationplasty converts the ankle to an active prosthetic knee. Note that the historical claim of "better function than amputation" is contested - the JBJS 2021 comparison showed no gait, energy or patient-reported advantage over amputation.
Q: What is the most common associated anomaly in PFFD? A: Fibular hemimelia - present in 50% of PFFD cases. Other associated findings include cruciate ligament deficiency, foot anomalies, and patellar anomalies.
Q: What is the most common complication during femoral lengthening for PFFD? A: Knee stiffness and flexion contracture - this is the most common complication and requires aggressive physical therapy from the start of lengthening. Other complications include pin site infection, delayed union, and nerve injury.
Q: Which Aitken types are candidates for reconstruction rather than rotationplasty or amputation? A: Type A and Type B - both have a femoral head present, making reconstruction feasible. Type A requires pelvic-femoral stabilization and lengthening. Type B requires osteotomy to establish neck continuity, then stabilization and lengthening. Type C and D lack the femoral head and require rotationplasty or amputation.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 2-year-old child presents with a shortened right lower limb noted since birth. Parents report the child walks with a limp. On examination, the right thigh is significantly shorter than the left, and the hip is held in flexion and abduction. Radiographs show a short proximal femur with coxa vara, but the femoral head is present. How would you assess and manage this child?”
“A 5-year-old child with known PFFD presents for treatment planning. Radiographs show absence of the femoral head with a dysplastic but present acetabulum (Aitken Type C). The predicted limb length discrepancy at maturity is 18cm. The ankle is functional. What are the treatment options and how would you counsel the family?”
“A 10-year-old child with Type A PFFD underwent femoral lengthening with an external fixator. During the distraction phase, the parents report the child has developed increasing knee stiffness and is unable to fully extend the knee. On examination, there is a 30-degree flexion contracture. The distraction is at 4cm of the planned 6cm. How would you manage this?”
Key Facts
- Incidence: 1 in 50,000 live births
- Aitken classification: Type A-D based on femoral head and acetabulum
- 50% have associated fibular hemimelia
- Limb length discrepancy is main problem
Aitken Classification
- Type A: Femoral head present, short neck, coxa vara = Reconstruction
- Type B: Femoral head present, no neck, pseudarthrosis = Reconstruction with osteotomy
- Type C: No femoral head, acetabulum present = Rotationplasty/amputation
- Type D: No femoral head, no acetabulum = Rotationplasty/amputation
Treatment Algorithm
- Type A/B: Reconstruction (pelvic-femoral stabilization, lengthening)
- Type C/D: Rotationplasty or amputation
- Severe LLD (over 15cm): Consider rotationplasty even in Type A/B
- Predict final LLD using multiplier or Paley method
Surgical Pearls
- Rotationplasty preserves proprioception - better than amputation
- Femoral lengthening: 1mm/day distraction, aggressive PT critical
- Knee stiffness is most common lengthening complication
- Multiple lengthenings may be needed for severe LLD
Complications
- Lengthening: Knee stiffness (most common), pin site infection, delayed union
- Reconstruction: Hip instability, contractures, hardware problems
- Rotationplasty: Wound healing, malrotation, prosthetic fitting issues
- Prevention: Aggressive PT, careful patient selection, close monitoring
Evidence Base
Aitken Classification of PFFD
- Original description of the four-grade Aitken classification (Types A to D)
- Stratifies severity by presence of the femoral head and the adequacy of the acetabulum
- Type A/B retain a femoral head (reconstructable hip); Type C/D lack a femoral head
- Remains the most widely cited descriptive system for PFFD worldwide
Reconstruction Strategy and Gait/PRO Outcomes (Landmark Comparison)
- 23 unilateral PFFD patients: equinus prosthesis (7), rotationplasty (6), Syme amputation with above-knee prosthesis (10)
- Oxygen cost did not differ between groups; all required greater energy than normal (rotationplasty 144%, Syme 159%, equinus 170%)
- No difference in PODCI pain, sport/physical function, happiness, or global function across groups
- Rotationplasty patients had undergone more procedures (mean 3.3 vs 1.8 Syme vs 0.7 equinus, p=0.001)
Rotationplasty: Long-Term Function and Patient Acceptance
- 8 adolescents with unilateral PFFD treated by rotationplasty; mean follow-up 9.25 years
- All patients were pain-free and able to ambulate outdoors at follow-up
- Foot derotation occurred in 5 of 8, requiring re-rotation osteotomy in 2 (recurrence is a recognised pitfall)
- All patients accepted their appearance and considered the procedure beneficial to function
Proximal Femoral Reconstruction (Paley Type 1b)
- 26 patients with Paley type 1b congenital femoral deficiency, mean age 7 years
- Neck-shaft angle improved from 72.3 to 133.1 degrees; acetabular index improved from 27.8 to 16.4 degrees
- Significant radiographic correction of coxa vara and acetabular dysplasia before lengthening
- Complication rate 15.4%, predominantly in children under 5 years
SUPERhip Procedure for Paley Type 1b CFD
- 72 SUPERhip procedures for Paley type 1b congenital femoral deficiency (1997-2012); 34 revisions performed, 106 procedures analysed
- SUPERhip = Systematic Utilitarian Procedure for Extremity Reconstruction of the hip, developed 1997 to correct proximal-femoral pathoanatomy before lengthening
- Very high risk of recurrent coxa vara and persistent delayed ossification of the femoral neck
- Fixed-angle internal fixation reduced recurrent varus; adding BMP-2 to the un-ossified neck reduced persistent delayed ossification
Multiplier Method for Limb-Length Prediction
- Congenital LLD increases proportionally with growth, so a single measurement times an age/sex multiplier predicts maturity discrepancy
- Validated against limb-lengthening and epiphysiodesis cohorts; comparable or superior to the Moseley straight-line graph
- Multipliers independent of height, race, ethnicity, generation and socioeconomic class
- Requires as few as one or two measurements (no serial scanograms or graph plotting)
Lengthening Nails versus External Fixation in Young Patients
- Systematic review of femoral lengthening comparing motorized intramedullary nails with external fixation (91 femora across 2 comparative studies)
- Both devices reliably achieved target length
- Adverse-event prevalence lower with nails (60-73%) than external fixation (81-100%)
- Nails were used in older patients (15-21 years) than external fixation (9-15 years); no PROs reported
Motorized Plate Lengthening in Young Children
- 7 skeletally immature children (ages 2.7 to 9.7 years) with congenital femoral deficiency
- Mean lengthening 4.1 cm (18% of segment); weight-bearing at mean 13 weeks
- Avoids the femoral-head AVN risk of intramedullary nails in young children
- Complication rate comparable to other femoral lengthening methods (patellar instability, transient hip subluxation, mild regenerate varus)