Ischial Tuberosity Origin | 2- vs 3-Tendon Tear | Sciatic Proximity
- Biceps femoris (long head) and semitendinosus share a conjoint tendon off the ischial tuberosity
- Semimembranosus has a separate origin (more anterolateral, deeper on the tuberosity)
- Mechanism = forced hip flexion with knee extension (waterskiing, sprinting, hurdling)
- MRI is the gold standard: shows tendon stump location, retraction distance, and sciatic relationship
- Complete 3-tendon avulsion or any avulsion with greater than 2 cm retraction is a surgical indication
- “Surgical repair within 4 weeks gives the best functional outcome
- “Sciatic nerve lies posterior to the hamstring origin - identify first when operating
- “Prone position, knee flexed, transverse or oblique gluteal crease incision
- “Suture anchors (3-5) into the ischial tuberosity, knee flexed to reduce tension
- “Neglected avulsions scar to the sciatic nerve and cause hamstring syndrome
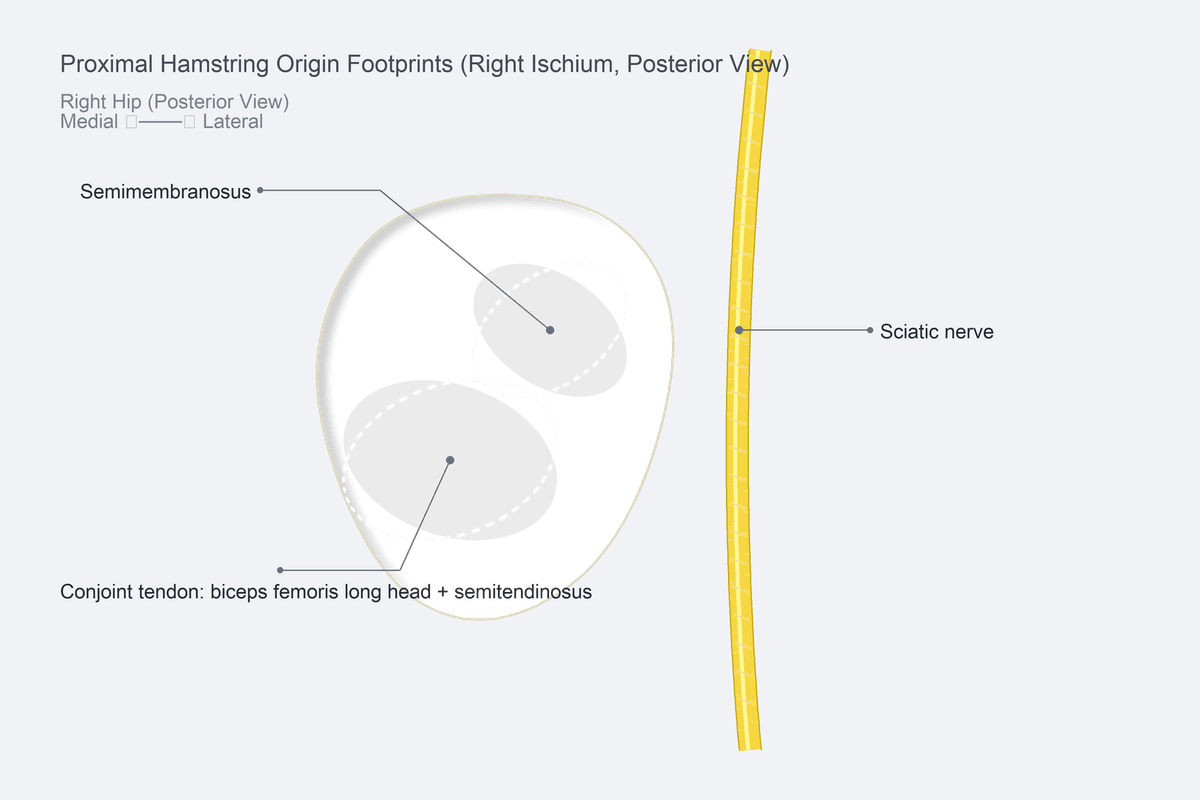
Conjoint tendon = biceps femoris (long head) + semitendinosus, sharing a common footprint on the posteromedial ischial tuberosity. Semimembranosus arises separately from the anterolateral aspect. This anatomy matters: a 2-tendon tear is usually the conjoint; a 3-tendon tear is the full hamstring origin.
Forced hip flexion with the knee in extension (eccentric overload of a lengthening hamstring). Classic scenarios: waterskiing fall, sprint start, hurdling, splits, road traffic dashboard injury. A palpable pop is followed by immediate posterior thigh pain and inability to accelerate.
T2 fat-saturated sequences show fluid-filled gap between tendon stump and ischial tuberosity. Axial + coronal + sagittal planes are mandatory. Measure retraction in cm - this drives the operative decision. Look for sciatic nerve tethering or oedema.
Complete 3-tendon avulsion; 2-tendon avulsion with greater than 2 cm retraction; elite or young active patient; sciatic nerve symptoms; failure of conservative care. Acute repair (less than 4 weeks) consistently outperforms delayed repair and conservative care.
- Diagnosis
- MRI: all three tendons off tuberosity
- Treatment
- Operative repair within 4 weeks
- Key Pearl
- Best results - 80-90 percent return to prior sport
- Diagnosis
- MRI retraction 2-5 cm, no scar
- Treatment
- Operative repair (acute) or delayed
- Key Pearl
- Younger, active patients benefit most
- Diagnosis
- MRI shows tendon near tuberosity
- Treatment
- Trial of conservative care
- Key Pearl
- Re-image at 6-12 weeks if no progress
- Diagnosis
- MRI: fluid at footprint, intact conjoint
- Treatment
- Conservative, structured rehab
- Key Pearl
- Most do well without surgery
SCAROperative Repair Sequence
Hook:The repair leaves a SCAR - sciatic first, clear footprint, anchors in, reattach with the knee flexed.
Overview and Epidemiology
Proximal hamstring avulsion is frequently misdiagnosed as a simple hamstring strain, and the window for an excellent operative result is narrow. Acute surgical repair (within 4 weeks) reliably returns high-demand athletes to prior sport; conservative care or delayed repair of complete 3-tendon avulsions is associated with persistent weakness, sitting pain, and sciatic symptoms. A high index of suspicion and a timely MRI are the two exam-favoured actions.
- Sports: Sprinting, hurdling, water skiing, rugby, football, dance, martial arts
- Age: Peak in 30-50 year-old recreational and competitive athletes
- Sex: Slight male predominance (waterskiing and sprint populations)
- Bilateral: Rare, reported in sprinters and waterskiing cohorts
- Strength loss: Knee flexion and hip extension strength drop 20-50 percent if untreated
- Sitting pain: Discomfort on hard chairs (ischial compression of stump)
- Sciatic symptoms: Scar tethering, paraesthesia, dysaesthesia
- Return to sport: 80-90 percent after acute repair; 30-50 percent after conservative care of complete tears
Pathophysiology
The hamstring origin is two footprints, not one. The conjoint tendon of biceps femoris (long head) and semitendinosus shares a common posteromedial insertion on the ischial tuberosity. The semimembranosus arises from a separate, more anterolateral and distal facet. This is why a 2-tendon avulsion is usually the conjoint and a 3-tendon avulsion is the complete origin. Failing to inspect the semimembranosus footprint at surgery is a recognised cause of missed injury.
- Origin
- Posteromedial ischial tuberosity
- Footprint shape
- Single, rounded
- Clinical note
- Most commonly avulsed as a unit
- Origin
- Anterolateral ischial tuberosity
- Footprint shape
- C-shaped / linear, separate facet
- Clinical note
- May avulse independently or with conjoint
- Origin
- Posterior to hamstring origin
- Footprint shape
- Runs distally down the thigh
- Clinical note
- At risk during surgery and from chronic scar
- Origin
- Superior to the hamstring origin
- Footprint shape
- Exits below piriformis
- Clinical note
- Protect during gluteal retraction
Eccentric overload of a contracting hamstring
- Hip flexion + knee extension = lengthening muscle under load
- Waterskiing fall (knee extended, hip flexing)
- Sprint start / acceleration
- Hurdling, splits, kicking sports
- Dashboard injury in road traffic
Risk amplifiers: warm-up deficit, fatigue, hamstring tightness, prior hamstring strain.
Acute: Tendon avulses from bone or fails at musculotendinous junction
Early (0-4 weeks): Stump retracts distally; haematoma forms; sciatic nerve initially displaced
Subacute (4-12 weeks): Haematoma organises; stump adheres to sciatic nerve and surrounding fascia
Chronic (greater than 12 weeks): Dense scar, sciatic tethering, muscle atrophy, sitting pain
End stage: Chronic hamstring syndrome, persistent weakness, dysaesthesia.
Classification and Types
MRI / Operative Grading
The most widely used grading system. Drives operative decision-making.
- Description
- Osseous avulsion chip, minimal displacement
- Typical management
- Conservative (often heal with rest and rehab)
- Description
- Musculotendinous junction, less than 2 cm retraction
- Typical management
- Controversial - trial conservative or repair in athletes
- Description
- Complete tendon avulsion, 2-5 cm retraction
- Typical management
- Operative repair (strong indication)
- Description
- Complete avulsion, greater than 5 cm retraction
- Typical management
- Operative repair (urgent referral, can be technically demanding)
Type I and low Type II injuries usually respond to structured rehab. Type III and IV are the surgical core.
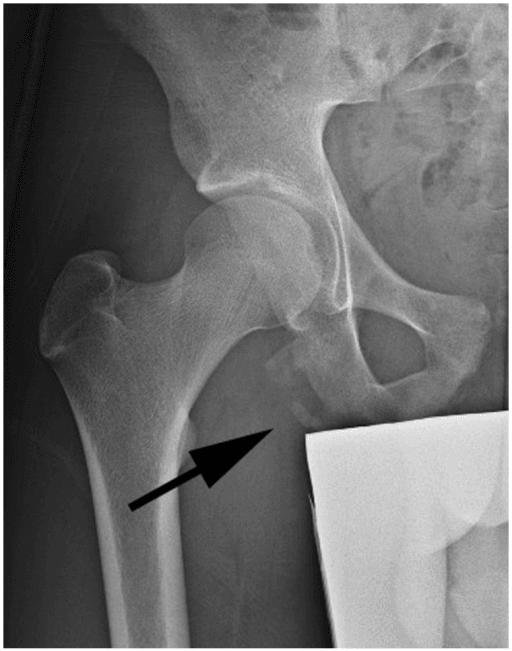
In the skeletally immature athlete (the ischial apophysis is the last pelvic apophysis to fuse, around 20-25 years), the same sprint/hurdle/split mechanism avulses the bony apophysis rather than tearing the tendon - an ischial tuberosity apophyseal avulsion fracture. It is a sprinter/gymnast/footballer injury (typically 14-18 years), presents with a pop and lower-buttock pain, and is diagnosed on a pelvic radiograph (a displaced bony fragment at the ischium) where the adult tendinous avulsion would need MRI. Management is by displacement: minimally displaced fragments (commonly under about 1.5-2 cm) are treated conservatively (rest, protected weight-bearing, graded rehab), while a widely displaced fragment (greater than about 2 cm), a symptomatic non-union, or painful exuberant callus is treated with ORIF (acute) or fragment excision with tendon reattachment (chronic/non-union). The classic trap is mistaking the bony fragment or its hypertrophic healing callus for a tumour or for chronic osteomyelitis. So in the adolescent, X-ray first and treat by fragment displacement, not by the adult tendon-retraction rules.
Clinical Assessment
- Mechanism: Forced hip flexion with knee extended (water ski, sprint, hurdle)
- Pop: Audible or felt "pop" in the buttock
- Acute pain: Posterior thigh / ischial region
- Function: Unable to sprint, sit comfortably, climb stairs with power
- Bruising: Bruising tracks down the posterior thigh over 24-48 hours
- Inspect: Swelling, ecchymosis at the gluteal crease
- Palpate: Tenderness over ischial tuberosity, palpable gap (prone, knee flexed)
- Strength: Knee flexion power reduced (especially at 15-30 degrees)
- Neurovascular: Sciatic symptoms (tingling, dysaesthesia in foot) - if positive, urgent MRI
Puranen test: Active knee flexion against resistance with the patient prone and the hip extended reproduces pain and reveals weakness. Compare to the contralateral side.
Palpable gap: Best felt with the patient prone, hip slightly extended, and the knee flexed to 90 degrees. The defect is at or just distal to the gluteal crease.
Sciatic screen: Always document tibial and peroneal divisions - the sciatic nerve lies within 1 cm of the stump in many cases and may be tethered in chronic injury.
- Technique
- Prone, hip extended, knee flexed to 15-30 degrees, resisted flexion
- Positive finding
- Pain at ischium + weakness
- Sensitivity / Note
- Useful screening test
- Technique
- Prone, knee flexed 90 degrees, palpate gluteal crease
- Positive finding
- Soft tissue gap between ischium and stump
- Sensitivity / Note
- Specific when present
- Technique
- Prone knee flexion against graded resistance
- Positive finding
- Reduced compared with other side
- Sensitivity / Note
- Suggests 2- or 3-tendon tear
- Technique
- Tinel sign over ischial region, foot dysaesthesia
- Positive finding
- Paraesthesia radiating to foot
- Sensitivity / Note
- Suggests scar tethering or acute displacement
Sciatica from lumbar disc: Pain radiates below the knee, positive straight-leg raise, no palpable gap.
Ischiogluteal bursitis: Chronic pain on sitting, no acute event, no weakness.
Hamstring muscle strain (mid-belly): Tender in the posterior thigh, not at the ischium; no gap.
Apophysitis / apophyseal avulsion in adolescents: Similar pain at the ischial tuberosity in skeletally immature athletes (14-25 years); pelvic X-ray shows widened apophysis.
Piriformis syndrome: Buttock pain with sciatic distribution but no ischial defect or post-traumatic onset.
Not every ischial-region complaint is an avulsion. Proximal (high) hamstring tendinopathy is a chronic insertional/overuse tendinopathy of the conjoint origin, classically in distance runners and sprinters, with deep buttock/ischial pain that is worst on sitting and during the acceleration or lengthening phase of running - an insidious onset with no pop, no palpable gap and preserved strength, unlike an acute avulsion. It overlaps with, and must be separated from, ischiogluteal bursitis and deep gluteal (sciatic entrapment) syndrome. MRI or ultrasound shows tendon thickening, intratendinous signal and peritendinous oedema without a retracted stump. Management is non-operative and load-based: relative rest and sitting modification, then a progressive eccentric / heavy-slow-resistance hamstring programme (the mainstay), with extracorporeal shockwave therapy and a carefully placed imaging-guided peritendinous injection (avoiding intratendinous corticosteroid and the sciatic nerve) as adjuncts; surgical debridement or tenotomy is reserved for the refractory minority. This is the answer to "how does it differ from hamstring syndrome and from an avulsion?".
PULSEClinical Presentation of Acute Avulsion
Hook:Feel the PULSE of an acute hamstring avulsion - pop, unable to sprint, lower-glute pain, swelling, examination gap.
Investigations

Imaging Protocol
Views: AP pelvis, frog-leg lateral, and a dedicated ischial tuberosity view
Look for: Osseous avulsion fragment, ischial apophyseal irregularity (in adolescents), pre-existing enthesopathy
Clinical correlation: A bony chip near the ischium in a sprinting athlete is diagnostic of Wood Type I
Sequences: Axial and coronal T2 fat-saturated, sagittal T2, axial T1
Look for: Fluid-filled gap at the ischial tuberosity, retracted tendon stump (measure in cm), sciatic nerve oedema or tethering, muscle oedema (acute) versus atrophy (chronic)
Required measurement: Distance from tuberosity to tendon stump end, in cm, on coronal T2 fat-sat
Indication: Equivocal MRI, claustrophobic patient, or to dynamically assess tendon continuity
Findings: Discontinuity of the tendon, dynamic gapping with knee flexion
Limitations: Operator dependent, deeper sciatic anatomy less well seen
Indication: Bony avulsion with intra-articular extension or large osseous fragment
Findings: Fragment size, displacement, articular involvement
Use: Plan for ORIF versus anchor repair
Three things to write in the MRI report for a proximal hamstring avulsion:
- Which tendons are off - conjoint only, conjoint + semimembranosus, semimembranosus only.
- Retraction distance - measure from the ischial footprint to the most distal retracted tendon end on coronal T2 fat-sat.
- Sciatic nerve relationship - displaced, tethered, oedematous, or clear.
These three lines drive the surgical decision more than any other finding.
Management Algorithm
Operative Repair (Type III / IV, 3-Tendon, or Symptomatic 2-Tendon)
Goal: Reattach avulsed tendon(s) to the ischial tuberosity, free the sciatic nerve, and restore hamstring strength and length.
Surgical Protocol
Position: Prone on a standard table with bolsters under the chest and pelvis, both arms abducted
Prep: Wide prep from the lower lumbar spine to the popliteal fossa; the entire leg is draped free to allow knee flexion
Tourniquet: Not required; the dissection is in the buttock
Incision: Transverse or oblique incision in the gluteal crease, centred over the ischial tuberosity (typically 6-10 cm)
Identify sciatic nerve first: Medial to the ischial tuberosity, lying on the short external rotators. Tag with a vessel loop
Mobilise the stump: The tendon end is usually retracted 2-5 cm distally. Gentle blunt dissection frees it from surrounding fascia
Clear the footprint: Remove residual tendon and decorticate the ischial tuberosity to bleeding cancellous bone
Identify each tendon: Conjoint and semimembranosus footprints are separate. Inspect both even if MRI suggested a 2-tendon tear
Suture anchors: Three to five double-loaded anchors along the footprint (5.5 mm titanium or PEEK, with high-strength suture)
Pass and tie: Pass tendon-grasping sutures through the stump; tie with the knee in 60-90 degrees of flexion to offload the repair
Check tension: Confirm solid reattachment; avoid strangulating the tendon
Drain: Closed-suction drain in the buttock for 24-48 hours
Brace: Hip-knee brace locked at 30-60 degrees of knee flexion for 4-6 weeks
Weight-bearing: Non-weight-bearing with crutches for 6 weeks; progressive loading thereafter
Tying the sutures with the knee flexed (60-90 degrees) brings the hamstring muscle closer to the ischial footprint and dramatically reduces the tensile load on the repair. Many early re-ruptures are technical failures from tying in extension under too much tension.
- Indication
- Acute avulsion with mobile stump
- Outcome
- Best functional scores; return to sport in 6-9 months
- Complications
- Re-rupture (less than 5 percent), sciatic dysaesthesia
- Indication
- Subacute injury with sciatic scar
- Outcome
- Good sciatic symptom relief; strength gains
- Complications
- Persistent nerve symptoms, scar recurrence
- Indication
- Chronic (greater than 12 weeks) with stump not reaching
- Outcome
- Restores length; modest strength gains
- Complications
- Graft failure, infection, donor site morbidity
- Indication
- Large osseous fragment (Wood Type I with displacement)
- Outcome
- Anatomic bony healing
- Complications
- Hardware irritation, non-union
FIX ITSurgical Indications - When to Fix
Hook:You FIX IT when the tear is full, retraction is more than 2 cm, the patient is high-demand, you are still in the 4-week window, or the sciatic nerve is trapped.
Complications
- Incidence
- 5-15 percent dysaesthesia; less than 1 percent motor
- Risk Factors
- Chronic scar, delayed surgery, aggressive retraction
- Management
- Neurolysis at index procedure; late neurolysis for scar
- Incidence
- 3-8 percent in modern series
- Risk Factors
- Tying under tension, premature rehab, anchor pullout
- Management
- Revision repair; consider augmentation
- Incidence
- 1-2 percent
- Risk Factors
- Buttock incision, drain, haematoma
- Management
- Irrigation and debridement; antibiotics
- Incidence
- 1-3 percent
- Risk Factors
- Prone position, hamstring immobility, obesity
- Management
- Mechanical prophylaxis; chemical prophylaxis per local protocol
- Incidence
- 10-20 percent even after repair
- Risk Factors
- Tuberosity prominence, scar tethering
- Management
- Cushion, padding, occasional bursectomy
- Incidence
- Common after missed or conservatively managed complete tears
- Risk Factors
- Scar tethering of sciatic nerve
- Management
- Late neurolysis and repair
Chronic, untreated proximal hamstring avulsions scar the sciatic nerve to the retracted stump. Patients develop sitting pain (ischial compression), posterior thigh tightness, and sciatic-type dysaesthesia in the foot. Treatment is sciatic neurolysis with or without repair, but outcomes are less reliable than acute surgery. This is the single most important reason to MRI early and operate on complete avulsions in active patients.
Outcomes and Prognosis
- Patient
- Complete tear, high demand
- Return to sport
- 80-90 percent
- Strength restoration
- 85-95 percent of contralateral
- Notes
- Best functional scores across series
- Patient
- Subacute, sciatic symptoms
- Return to sport
- 60-75 percent
- Strength restoration
- 75-85 percent of contralateral
- Notes
- Sciatic relief in most; strength gains later
- Patient
- Late presentation, hamstring syndrome
- Return to sport
- 40-60 percent
- Strength restoration
- 60-75 percent of contralateral
- Notes
- Improved but not normal; graft may be required
- Patient
- Partial tear, low retraction
- Return to sport
- 70-85 percent
- Strength restoration
- 80-90 percent of contralateral
- Notes
- Most do well if not complete 3-tendon
- Patient
- Missed or declined surgery
- Return to sport
- 30-50 percent
- Strength restoration
- 50-70 percent of contralateral
- Notes
- Sitting pain, sciatic symptoms common
Favourable: Acute repair (less than 4 weeks), complete tendon off, mobile stump, young active patient, no sciatic involvement, single operation.
Unfavourable: Chronic (greater than 12 weeks), sciatic scar, retracted stump not reaching, re-rupture, multiple prior repairs, age greater than 60, low demand but significant pain.
Key threshold: 4 weeks - outcomes decline measurably beyond this window in most series.
Guidelines, Registries & Global Practice
- Incidence: Proximal hamstring avulsions are uncommon but increasing as participation in sprinting, water sports, and high-intensity training grows worldwide
- Populations at risk: Sprinters (track and field), rugby, football (soccer and American), water skiers, dancers, martial artists
- Mechanism distribution: Eccentric lengthening in sport dominates; dashboard and falls are second-tier causes
- Bilateral avulsions: Reported in sprint and water-ski cohorts; rare but reported
- High-resource: dedicated MRI within 48 hours, sports orthopaedic referral, suture anchor repair, structured sport-specific rehab
- Limited-resource: MRI may be delayed; ultrasound used for screening; conservative care is the default for partial tears; surgical repair is concentrated in tertiary centres
- Universal principle: outcome is determined more by timing of surgery (less than 4 weeks) and accurate MRI grading than by implant choice
- Surgery: most high-volume centres use 3-5 suture anchors to the ischial tuberosity with the knee flexed
- Diagnosis emphasis
- MRI with retraction measurement; classify by Wood
- Operative threshold
- Complete 3-tendon or retraction greater than 2 cm in active patients
- Rehab / return to sport
- Brace at 30-60 degrees flexion, return at 6-9 months
- Diagnosis emphasis
- MRI in elite athletes with suspected avulsion
- Operative threshold
- Operative for complete 2- or 3-tendon in athletes
- Rehab / return to sport
- Eccentric rehab, sport-specific progression, RTS testing
- Diagnosis emphasis
- Clinical exam plus MRI; sciatic assessment
- Operative threshold
- Operative for 3-tendon, 2-tendon with retraction, or sciatic symptoms
- Rehab / return to sport
- MDT-led rehab; phased return to running
- Diagnosis emphasis
- Standardised Wood classification; MRI and operative correlation
- Operative threshold
- Acute operative repair less than 4 weeks when indicated
- Rehab / return to sport
- Eccentric loading, Nordic hamstrings in return phase
There is no dedicated registry for proximal hamstring avulsions, unlike ACL or hip arthroplasty registries. The evidence base is dominated by retrospective case series and small prospective cohorts comparing acute vs delayed repair. Randomised trials are ethically and logistically difficult because the operative indication (complete 3-tendon tear in an active patient) is widely accepted. National joint registries and sports injury databases are gradually including hamstring data, but the field remains principle-based: MRI grading, sciatic assessment, and acute surgery when indicated.
Record in every suspected proximal hamstring avulsion:
- Mechanism (eccentric lengthening during hip flexion + knee extension)
- Examination findings (palpable gap, strength deficit, sciatic Tinel)
- MRI report including which tendons off and retraction in cm
- Sciatic nerve symptoms (subjective and objective)
- Patient demand (elite, recreational, low demand)
- Operative plan and timing (within 4 weeks window if indicated)
Delayed diagnosis and missed operative windows are the most common medicolegal issues in this injury worldwide. Document the assessment and the discussion with the patient explicitly.
Controversies & Areas of Uncertainty
Some centres report acceptable outcomes from structured rehab for 2-tendon avulsions with less than 2 cm retraction in non-elite patients, but most sports orthopaedic groups now favour repair in any active patient, citing faster return to sport and lower chronic pain. The exact threshold is debated.
Three to five anchors along the footprint is conventional, but there is no head-to-head trial of 2-anchor vs 5-anchor constructs. Biomechanical cadaveric studies favour wider anchor spread, but clinical correlation is limited.
Bracing at 30-60 degrees of knee flexion is widely accepted, but the optimum angle, duration, and weight-bearing status vary between centres. Early protected weight-bearing in some protocols appears safe but is not yet supported by high-level evidence.
In chronic avulsions with gap greater than 5 cm, allograft (Achilles or hamstring) interposition is the standard off-the-shelf option, but synthetic tapes and other biologics are emerging. Long-term outcome data are lacking.
MCQ Practice Points
Q: Which two tendons share the conjoint origin at the ischial tuberosity? A: Biceps femoris (long head) and semitendinosus. They share a common footprint on the posteromedial ischial tuberosity. The semimembranosus has a separate, more anterolateral origin. This anatomy explains why a 2-tendon avulsion is usually the conjoint and a 3-tendon avulsion is the complete origin.
Q: What is the classic mechanism of a proximal hamstring avulsion? A: Forced hip flexion with the knee in extension - eccentric overload of a contracting hamstring. Common in water skiing (fall with knee extended), sprint starts, hurdling, and dashboard injuries. A pop is typically felt in the buttock, followed by immediate pain and weakness.
Q: In the Wood classification, what retraction distance indicates a surgical repair? A: Greater than 2 cm of retraction (Type III or Type IV). Type I (osseous avulsion, minimal displacement) and Type II (less than 2 cm retraction) may be treated conservatively depending on patient demand. Type III (2-5 cm) and Type IV (greater than 5 cm) are operative indications.
Q: What is the ideal timing for surgical repair of an acute proximal hamstring avulsion? A: Within 4 weeks of injury (acute window). Acute repair produces better strength recovery, higher return-to-sport rates, and lower complication rates than delayed repair. Beyond 12 weeks, the stump retracts and may not reach the ischium, sometimes requiring allograft.
Q: What is the relationship of the sciatic nerve to the proximal hamstring origin, and why does it matter? A: The sciatic nerve lies posterior to the ischial tuberosity and the hamstring origin, passing distally into the thigh. It is at risk during surgical repair (must be identified first) and can become tethered by scar tissue in chronic avulsions (causing hamstring syndrome with sitting pain and sciatic dysaesthesia).
Q: What is the post-operative bracing protocol after proximal hamstring avulsion repair? A: Hip-knee brace locked at 30-60 degrees of knee flexion for 4-6 weeks, non-weight-bearing with crutches for 6 weeks, then progressive loading. The knee is flexed at brace application to offload the repair, since tying was performed with the knee flexed. Eccentric strengthening starts at 6-8 weeks; return to sport typically at 6-9 months.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old professional rugby player describes a pop in his left buttock while sprinting to catch a kick 6 days ago. He has bruising tracking down the posterior thigh, weakness with knee flexion, and pain on sitting. MRI shows a complete avulsion of the biceps femoris long head, semitendinosus, and semimembranosus with 3 cm of retraction. The sciatic nerve is displaced but not oedematous. What is your management plan?”
“A 47-year-old recreational marathon runner presents 9 months after a hamstring injury misdiagnosed as a strain. He has persistent buttock pain, sitting discomfort, and intermittent tingling on the lateral border of his foot. Examination reveals a palpable gap at the ischium, reduced hamstring strength, and a positive Tinel sign posteriorly. MRI confirms a complete 3-tendon avulsion with 4 cm of retraction and sciatic nerve tethering. He wants to return to running. How would you manage this?”
Key Anatomy
- Conjoint tendon (biceps long head + semitendinosus) and semimembranosus arise separately from the ischial tuberosity
- Sciatic nerve lies posterior to the hamstring origin - at risk in chronic scar and during surgery
- Mechanism = forced hip flexion with the knee in extension (eccentric lengthening)
Diagnosis
- Mechanism, pop, buttock pain, ecchymosis tracking down the posterior thigh
- Palpable gap at the ischium with the patient prone and the knee flexed
- Reduced knee flexion strength; Puranen test positive
- MRI is gold standard - measure retraction in cm, identify which tendons are off, check sciatic nerve
Classification (Wood)
- Type I = osseous avulsion, minimal displacement (often conservative)
- Type II = musculotendinous, retraction less than 2 cm (contested)
- Type III = complete tendon avulsion, retraction 2-5 cm (operative)
- Type IV = complete avulsion, retraction greater than 5 cm (operative, urgent)
Operative Indications
- Complete 3-tendon avulsion
- 2-tendon avulsion with retraction greater than 2 cm in active patients
- Sciatic nerve symptoms or MRI tethering
- Failed conservative care of partial avulsions
Surgical Pearls
- Prone position, transverse or oblique gluteal crease incision
- Identify and protect the sciatic nerve first
- 3-5 suture anchors to the ischial tuberosity; reattach conjoint and semimembranosus separately
- Tie sutures with the knee flexed to 60-90 degrees to offload the repair
- Acute repair (less than 4 weeks) is best; chronic cases may need allograft
Complications
- Sciatic nerve dysaesthesia (5-15 percent) - identify nerve first
- Re-rupture (3-8 percent) - tied under tension is the usual cause
- Hamstring syndrome in chronic missed injuries - scar tethering of sciatic
- DVT, infection, persistent sitting pain from tuberosity prominence
Evidence Base and Key Trials
Functional outcome after repair of proximal hamstring avulsions
- Acute repair produced higher subjective and objective outcome scores than delayed repair
- Most patients returned to sport after acute repair, with strength restored to near-baseline
Complete proximal hamstring avulsions: a series of 41 patients with operative treatment
- Surgical repair with suture anchors achieved good pain relief and strength in 41 patients
- Sciatic neurolysis was frequently required in chronic cases
Hamstring injuries in professional football players: magnetic resonance imaging correlation with return to play
- Proximal avulsions with greater retraction on MRI were associated with longer return-to-play times
- MRI is valuable for predicting recovery timeline in elite athletes
Outcomes following adolescent athlete proximal hamstring apophyseal avulsion bone fragment excision and direct tendon-ischial tuberosity reattachment
- Direct reattachment after bone fragment excision in adolescent athletes yielded good outcomes
- Return to sport was achieved in the majority with low complication rates