Calcium Pyrophosphate Dihydrate | Positively Birefringent | Rhomboid Crystals
- CPP crystals are rhomboid/rod-shaped and positively birefringent (blue parallel to polarizer)
- Chondrocalcinosis on X-ray is pathognomonic but not synonymous with symptomatic disease
- Knee is the most commonly affected joint (50% of cases)
- Associated conditions: Hemochromatosis, hyperparathyroidism, hypomagnesemia, hypothyroidism
- No specific disease-modifying therapy exists unlike gout
- “Positively birefringent = blue when parallel to polarizer axis
- “Chondrocalcinosis on knee X-ray: triangular fibrocartilage, hyaline cartilage
- “Always screen for metabolic causes in patients younger than 55 years
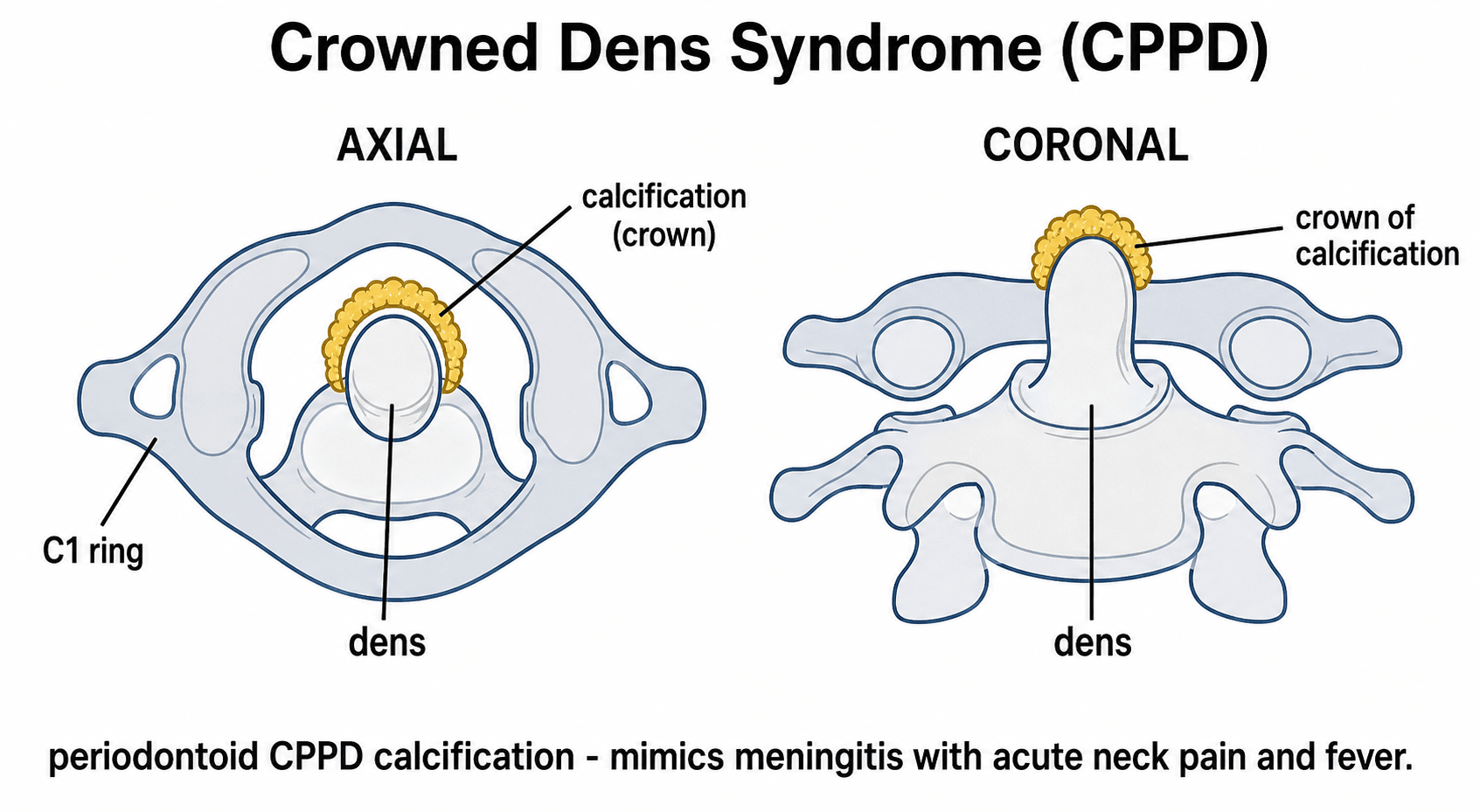
- “Crowned dens syndrome mimics meningitis - look for calcification around odontoid
CPP crystals: Rhomboid or rod-shaped, positively birefringent (blue parallel, yellow perpendicular). MSU crystals (gout): Needle-shaped, negatively birefringent (yellow parallel). This is the fundamental diagnostic distinction tested in exams.
Screen for underlying causes in young patients (less than 55 years): Hemochromatosis (ferritin, transferrin saturation), hyperparathyroidism (calcium, PTH), hypomagnesemia, hypothyroidism (TSH). These are frequently asked in vivas.
Chondrocalcinosis: Linear calcification in fibrocartilage (menisci, TFCC, symphysis pubis) and hyaline cartilage. Pyrophosphate arthropathy: Subchondral cysts, osteophytes, joint space narrowing - often in unusual OA locations.
No urate-lowering equivalent exists for CPPD - treatment is symptomatic only. Joint distribution differs - knee more common than 1st MTP. Chronic form resembles OA rather than erosive arthritis. Attacks often less intense than gout.
- CPPD (Pseudogout)
- Rhomboid/rod-shaped
- Gout (MSU)
- Needle-shaped
- CPPD (Pseudogout)
- Positive (BLUE parallel)
- Gout (MSU)
- Negative (YELLOW parallel)
- CPPD (Pseudogout)
- Knee, wrist
- Gout (MSU)
- 1st MTP (podagra)
- CPPD (Pseudogout)
- Chondrocalcinosis
- Gout (MSU)
- Punched-out erosions
- CPPD (Pseudogout)
- Hemochromatosis, HPT, hypoMg
- Gout (MSU)
- Diet, alcohol, CKD
- CPPD (Pseudogout)
- None available
- Gout (MSU)
- Allopurinol, febuxostat
RHOMBUSCPPD Crystal Features
Hook:RHOMBUS-shaped crystals glow BLUE parallel!
KWISTChondrocalcinosis Locations
Hook:Know Where It Shows on Targeting X-rays!
Overview and Epidemiology
Calcium pyrophosphate deposition (CPPD) disease is a crystal arthropathy caused by the deposition of calcium pyrophosphate dihydrate (CPP) crystals in articular and periarticular tissues. It encompasses a spectrum from asymptomatic chondrocalcinosis to acute pseudogout attacks to chronic pyrophosphate arthropathy.
- Prevalence increases markedly with age: rare before age 50, present in greater than 40% of those over 84 years
- Male to female ratio: approximately equal (slight female predominance in some studies)
- Radiographic chondrocalcinosis: 15% at age 65-74, 44% at age 85 and older
- Only 25% of those with radiographic chondrocalcinosis are symptomatic
- Age: Strongest risk factor - prevalence doubles each decade after 60
- Prior joint injury: Meniscectomy, joint trauma
- Osteoarthritis: Strong association, chicken-and-egg relationship
- Metabolic conditions: Hemochromatosis, hyperparathyroidism, hypomagnesemia, hypothyroidism
- Familial: Rare autosomal dominant forms (ANKH gene mutations)
CPPD in a patient under 55 should trigger investigation for underlying metabolic disease. This is a common exam question - always screen young patients for the 4 H's: Hemochromatosis, Hyperparathyroidism, Hypomagnesemia, Hypothyroidism.
Pathophysiology
Understanding the pathophysiology of CPPD is essential for both diagnosis and management. The disease results from aberrant pyrophosphate metabolism leading to crystal formation in cartilage.
Pyrophosphate Metabolism
- Inorganic pyrophosphate (PPi) is produced during ATP hydrolysis
- PPi is normally converted to orthophosphate by pyrophosphatases
- Balance between PPi generation and breakdown maintains normal levels
- Chondrocytes are the primary source of articular PPi
- Excess PPi combines with calcium to form CPP crystals
- Crystals deposit preferentially in fibrocartilage (menisci, TFCC) and hyaline cartilage
- Crystal shedding into joint space triggers acute inflammation
Mechanisms of Crystal Formation
- Increased ANKH transporter activity (exports PPi from cells)
- Decreased tissue non-specific alkaline phosphatase (TNAP) activity
- Chondrocyte senescence with altered metabolism
- Elevated calcium concentrations (hyperparathyroidism)
- Increased PPi (ANKH mutations, hemochromatosis)
- Decreased PPi degradation (hypomagnesemia - Mg is TNAP cofactor)
- Cartilage matrix changes with aging
Inflammatory Response
Crystal-induced inflammation:
- CPP crystals shed from cartilage into joint space
- Crystals phagocytosed by synovial macrophages
- NLRP3 inflammasome activation (similar to gout)
- IL-1beta release triggers neutrophil influx
- Acute synovitis develops
Magnesium is an essential cofactor for pyrophosphatases that break down PPi. Low magnesium leads to PPi accumulation and crystal formation. This explains the association with diuretic use and alcoholism.
Chronic arthropathy:
- Persistent low-grade inflammation damages cartilage
- Crystal deposition alters cartilage biomechanics
- Secondary osteoarthritic changes develop
- Distinctive pattern of joint involvement
HHHHMetabolic Causes of CPPD
Hook:The 4 H's of metabolic CPPD - Hunt for Hidden causes!
Clinical Presentation
Acute CPP Crystal Arthritis (Pseudogout)
- Acute monoarticular arthritis mimicking gout or septic arthritis
- Knee is the most common site (50% of attacks)
- Less severe than gout - can usually weight-bear
- Self-limiting over 1-3 weeks without treatment
- May be triggered by illness, surgery, or trauma
- Knee - 50%
- Wrist - 25%
- Shoulder, ankle, elbow - remaining 25%
- 1st MTP (podagra) - uncommon unlike gout
Chronic CPP Crystal Arthropathy
Features:
- Resembles osteoarthritis clinically and radiographically
- Affects joints atypical for primary OA
- MCP joints, wrists, shoulders, ankles - unusual OA sites
- Progressive joint destruction possible
- Morning stiffness and inflammatory features may be present
Crowned Dens Syndrome
Cervical spine involvement:
- Calcification around the odontoid process
- Acute severe neck pain, fever, elevated inflammatory markers
- Mimics meningitis or retropharyngeal abscess
- Diagnosis: CT showing periodontal calcification
- Treatment: NSAIDs, usually self-limiting
Physical Examination
- Swelling and erythema over affected joint (less marked than gout)
- Joint effusion, particularly at knee
- No tophi (unlike gout)
- Warmth and tenderness over affected joint
- Effusion detectable at knee (ballottement, patellar tap)
- Crepitus in chronic arthropathy
Investigations
Laboratory Studies
- CPP crystal identification under polarized microscopy
- Rhomboid or rod-shaped, positively birefringent crystals
- Blue when parallel to the polarizer (opposite of gout)
- WBC count: 10,000-50,000/microL (predominantly neutrophils)
- Ferritin and transferrin saturation - hemochromatosis
- Calcium, PTH - hyperparathyroidism
- Magnesium - hypomagnesemia
- TSH - hypothyroidism
- ESR, CRP - elevated during acute attack
- Uric acid - may help differentiate from gout
Imaging
- Chondrocalcinosis - linear calcification in cartilage
- Fibrocartilage: Menisci (triangular), TFCC (linear), symphysis pubis
- Hyaline cartilage: Parallel lines within cartilage
- Pyrophosphate arthropathy: Subchondral cysts, osteophytes, joint space narrowing
- Knee: Meniscal calcification, femoral condyle cartilage
- Wrist: TFCC, scapholunate ligament
- Pelvis: Symphysis pubis
- Spine: Intervertebral disc calcification
- Hyperechoic deposits within cartilage
- Distinguishable from gout (cartilage surface vs within cartilage)
- Best for crowned dens syndrome (periodontal calcification)
- Useful for spinal involvement
Differential Diagnosis of an Acute Hot Joint
The single most important step in acute monoarthritis is to exclude infection. Crystals and sepsis can coexist, so positive crystals never fully exclude a septic joint.
- Key Pointers
- Older patient, knee/wrist, post-stress trigger, chondrocalcinosis
- Decisive Test
- SF: rhomboid, positively birefringent crystals
- Key Pointers
- 1st MTP podagra, tophi, hyperuricaemia, punched-out erosions
- Decisive Test
- SF: needle-shaped, negatively birefringent crystals
- Key Pointers
- Systemic sepsis, very high SF WBC, immunosuppression
- Decisive Test
- SF Gram stain and culture (treat as septic if in doubt)
- Key Pointers
- Milwaukee shoulder, rotator-cuff destruction, periarticular calcification
- Decisive Test
- Alizarin red stain; crystals not seen on standard polarised light
- Key Pointers
- Younger patient, preceding infection, enthesitis, extra-articular features
- Decisive Test
- Clinical pattern, serology, SF non-crystalline
- Key Pointers
- Anticoagulation, trauma, frank blood on aspiration
- Decisive Test
- SF macroscopically bloodstained


Pyrophosphate Arthropathy and the Hemochromatosis Pattern
Chronic CPP arthropathy produces a degenerative pattern that is recognisably "OA in the wrong joints" — a key examiner clue that calcium pyrophosphate (or an underlying metabolic driver) is at work.
- Unusual joint distribution — the radiocarpal (wrist), metacarpophalangeal, elbow, shoulder, patellofemoral and talonavicular joints, which typical primary OA tends to spare.
- Patellofemoral-predominant knee OA (isolated, or disproportionate to the tibiofemoral compartments) is a classic CPPD pattern.
- Prominent subchondral cysts and large osteophytes out of proportion to the degree of joint-space loss.
- Frequently superimposed chondrocalcinosis.
- Hereditary haemochromatosis causes a distinctive arthropathy with hook-shaped osteophytes on the radial side of the 2nd and 3rd metacarpal heads — almost a signature sign.
- It typically involves the 2nd–5th MCP joints with squaring and joint-space loss, frequently accompanied by chondrocalcinosis.
- This is why MCP-predominant arthropathy plus chondrocalcinosis should prompt ferritin and transferrin saturation, particularly in a patient under 55.
Degenerative change in the wrist (radiocarpal), MCP joints, elbow, shoulder or patellofemoral joint — sites primary OA usually spares — should make you think CPPD. Hook osteophytes at the 2nd/3rd MCP heads are the classic clue to haemochromatosis, so screen with ferritin and transferrin saturation.
Basic Calcium Phosphate Disease and Milwaukee Shoulder
CPPD must be distinguished from the other common articular calcium crystal, basic calcium phosphate (BCP) — principally carbonated hydroxyapatite. The two frequently coexist in osteoarthritic joints, but they behave and are detected differently.
- CPPD
- Calcium pyrophosphate dihydrate; rhomboid/rod-shaped
- Basic calcium phosphate (BCP)
- Hydroxyapatite; tiny non-crystalline 'clumps'
- CPPD
- Weakly POSITIVELY birefringent (visible)
- Basic calcium phosphate (BCP)
- NOT birefringent — invisible on standard light microscopy
- CPPD
- Synovial-fluid polarised microscopy
- Basic calcium phosphate (BCP)
- Alizarin red S stain, or electron microscopy / spectroscopy
- CPPD
- Pseudogout, chondrocalcinosis, pyrophosphate arthropathy
- Basic calcium phosphate (BCP)
- Calcific tendinitis, Milwaukee shoulder, periarticular calcification
Milwaukee shoulder is the destructive shoulder arthropathy caused by BCP (hydroxyapatite) crystals, classically in elderly women. It produces a large, often blood-stained, non-inflammatory effusion, rotator-cuff destruction with superior migration of the humeral head, and rapid glenohumeral joint destruction. Because the crystals are not birefringent, synovial-fluid microscopy looks "negative" unless alizarin red staining is used. BCP also underlies calcific tendinitis (for example of supraspinatus). Management is largely supportive (aspiration, NSAIDs, activity modification); an irreparably destroyed cuff and joint may ultimately need reverse shoulder arthroplasty.
BCP (hydroxyapatite) crystals are NOT birefringent — a synovial sample full of them can look acellular/negative under standard polarised light. Suspect BCP when there is calcific tendinitis, or a destructive Milwaukee shoulder in an elderly woman, and confirm with alizarin red staining rather than ordinary polarised microscopy.
Management
Acute Attack Management
- NSAIDs: Indomethacin 50mg TDS, naproxen 500mg BD
- Colchicine: 0.5mg BD-TDS - less effective than in gout but still useful
- Corticosteroids: Intra-articular (preferred for monoarticular) or oral prednisolone
- Therapeutic as well as diagnostic
- Large effusion aspiration provides significant relief
- Send for crystals and culture (exclude sepsis)
Acute pseudogout can mimic septic arthritis. Always send synovial fluid for Gram stain and culture. If any doubt, treat as septic until proven otherwise. Crystals and infection can coexist.
Refractory cases:
- IL-1 inhibitors (anakinra) for patients unresponsive to conventional therapy
- Systemic corticosteroids if polyarticular
This section covers the acute management of pseudogout attacks.
Surgical Management
Indications for Surgery
- End-stage arthropathy: Joint destruction requiring arthroplasty
- Mechanical symptoms: Loose bodies, meniscal pathology
- Carpal tunnel syndrome: From crystal deposition
- Crowned dens syndrome: Rarely requires surgical decompression
Joint Arthroplasty in CPPD
- CPPD arthropathy is an indication for joint replacement
- Outcomes generally good but some studies show higher complication rates
- Ensure acute attack is not present at time of surgery
- Screen for metabolic conditions
- Assess other joints for involvement
- Consider prophylactic colchicine perioperatively
- Total knee arthroplasty: Good outcomes reported
- Total hip arthroplasty: Comparable to primary OA
- Shoulder arthroplasty: Higher complication rates in some series
- Crystal disease does not preclude arthroplasty
- May have higher manipulation rates post-TKA
- Consider perioperative colchicine for flare prophylaxis
This section covers arthroplasty considerations in CPPD.
Complications
Disease Complications
- Chronic erosive arthropathy: Progressive joint destruction
- Spinal stenosis: From disc calcification and hypertrophy
- Tendon rupture: Rare but reported with periarticular deposits
- Neurological compression: Carpal tunnel, cervical myelopathy
Surgical Complications
- Acute flare: Perioperative pseudogout attack
- Stiffness: May be more common after TKA
- Wound healing: Generally not affected unlike gout with tophi
- Recurrent symptoms: Crystal deposition continues
Guidelines, Registries & Global Practice
CPPD is a global disease of the ageing joint. Because no therapy dissolves CPP crystals anywhere in the world, international guidance converges on the same two pillars: confident diagnosis (crystal identification plus imaging) and control of inflammation, while excluding sepsis and treating any underlying metabolic driver.
Global epidemiology
- Radiographic chondrocalcinosis is strongly age-dependent and varies by population: knee chondrocalcinosis in adults aged 60 and over is around 6-8% in US white cohorts (Framingham) but under 3% in Beijing Chinese cohorts using identical protocols.
- CPPD may be the commonest inflammatory arthritis in people over 60 years; most radiographic chondrocalcinosis is asymptomatic.
- Familial autosomal-dominant forms (ANKH mutations) are rare but cause young, often polyarticular, onset.
Side-by-side guidance
- Region
- Europe
- Emphasis
- 'CPPD' umbrella terminology; SF crystal ID is definitive; ultrasound preferred imaging (LR 24.2)
- Region
- International
- Emphasis
- Standardised classification for research; integrates clinical, SF and imaging (including CT for axial disease)
- Region
- International
- Emphasis
- Reproducible US scoring of CPP deposits in cartilage and fibrocartilage
- Region
- International
- Emphasis
- Crystal arthropathy is not a contraindication to arthroplasty; always exclude periprosthetic infection first
Registry and arthroplasty evidence
- Large arthroplasty registries (NJR, AOANJRR, AJRR, Swedish/Norwegian) do not list CPPD as a distinct indication, but cohort data (e.g. 1500-knee CORR series) show chondrocalcinosis does not increase TKA revision risk and yields comparable Knee Society scores.
- Implication: standard implant and bearing selection applies; CPPD changes perioperative flare prophylaxis, not prosthesis choice.
High- vs limited-resource practice variation
- Well-resourced settings: routine polarised microscopy and high-frequency ultrasound enable confident crystal/imaging diagnosis; IL-1 blockade (anakinra/canakinumab) available for refractory attacks.
- Limited-resource settings: diagnosis often rests on plain radiographs and clinical pattern; management relies on NSAIDs, colchicine and intra-articular or oral corticosteroids, with aspiration to exclude sepsis remaining the universal safety step.
- Everywhere: screen young or polyarticular patients for haemochromatosis, hyperparathyroidism, hypomagnesaemia and hypothyroidism, and refer for definitive metabolic treatment.
Controversies & Areas of Uncertainty
CPPD remains under-researched relative to gout, and several questions are unresolved - useful material for higher-order viva discussion.
- Causality with osteoarthritis: CPPD and OA are tightly linked but the direction is unclear. CPP crystals may accelerate cartilage degradation, or degenerate cartilage may simply favour crystal nucleation. The association is also joint-specific (associates with knee OA, not hip OA).
- No crystal-dissolving therapy: Unlike urate-lowering therapy in gout, nothing reliably reduces CPP crystal burden. Drugs targeting pyrophosphate metabolism (e.g. probenecid, magnesium, phosphocitrate) remain experimental or unproven.
- Prophylaxis evidence is weak: Low-dose colchicine and hydroxychloroquine are used for recurrent flares largely by extrapolation from gout and small studies; randomised data are limited. Methotrexate was not confirmed to be effective in recent trials.
- Role of IL-1 blockade: Anakinra and canakinumab help refractory attacks mechanistically (NLRP3/IL-1beta pathway) but evidence is limited to case series; they are not formally licensed for CPPD.
- Imaging thresholds: Ultrasound (and the OMERACT definitions) and dual-energy/conventional CT are increasingly used, but the optimal diagnostic algorithm and how to grade subclinical deposition are still being standardised.
- Whom to screen metabolically: There is consensus to screen young (under ~55-60) or polyarticular patients, but the yield in older sporadic disease is low and the exact age cut-off and panel vary between guidelines.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 72-year-old woman presents with acute onset pain and swelling of her right knee. She had a hip replacement 3 days ago. Examination shows a warm, swollen knee with an effusion. She is afebrile.”
“A 48-year-old man presents with recurrent episodes of knee pain and swelling. X-rays show chondrocalcinosis. His father had similar problems. He also reports fatigue and impotence.”
“You are shown a polarized microscopy image of synovial fluid showing rhomboid crystals that appear blue when aligned parallel to the polarizer. What is your diagnosis?”
“An 80-year-old woman presents with acute severe neck pain, fever, and neck stiffness. She is being investigated for possible meningitis. CT cervical spine shows calcification around the odontoid process.”
Crystal Identification
- CPP: Rhomboid/rod-shaped, positively birefringent (BLUE parallel)
- MSU: Needle-shaped, negatively birefringent (YELLOW parallel)
- Mnemonic: 'Blue Parallel Pseudogout' vs 'Yellow Parallel Gout'
Classic Presentation
- Acute knee arthritis most common (50%)
- Less severe than gout - can often weight-bear
- May be triggered by surgery, illness, trauma
Radiographic Signs
- Chondrocalcinosis: Linear calcification in cartilage
- Meniscal triangular calcification on knee AP
- TFCC calcification on wrist PA
- Symphysis pubis calcification on pelvis AP
Metabolic Screen (The 4 H's)
- Hemochromatosis: Ferritin, transferrin saturation
- Hyperparathyroidism: Calcium, PTH
- Hypomagnesemia: Serum magnesium
- Hypothyroidism: TSH
Treatment
- NSAIDs, colchicine, or steroids for acute attacks
- No disease-modifying therapy (unlike gout)
- Treat underlying metabolic conditions
- Arthroplasty for end-stage arthropathy
Exam Traps
- Always exclude septic arthritis in acute presentation
- Screen for metabolic causes if under 55 years
- Crowned dens syndrome mimics meningitis
- Crystals and infection can coexist
Evidence Base
EULAR Recommendations for CPPD (Part I: Terminology and Diagnosis)
- 'CPPD' is the umbrella term (acute CPP crystal arthritis, OA with CPPD, chronic CPP inflammatory arthritis)
- Definitive diagnosis requires synovial fluid CPP crystal identification
- Ultrasound positive likelihood ratio 24.2 (95% CI 3.51-168) for peripheral joints, superior to radiography
- Recognised risk factors: ageing, OA, primary hyperparathyroidism, haemochromatosis, hypomagnesaemia
Ethnic Variation in Chondrocalcinosis Prevalence (Beijing vs Framingham)
- Knee chondrocalcinosis much lower in Beijing Chinese (1.8% men, 2.7% women) than US white subjects (6.2% men, 7.7% women)
- Age-standardised prevalence ratio approximately 0.34-0.43 for knee in Chinese subjects
- Wrist chondrocalcinosis rare in Chinese subjects (0.3-1.0%)
- Highlights genetic and environmental contributions to deposition
ANKH Mutations Cause Autosomal-Dominant Familial CPPD
- Identical P5T missense mutation at the amino terminus of ANKH in both families
- All affected members heterozygous; mutation absent in 204 control alleles
- Position 5 of ANKH is a mutational hot spot in dominant CPPD
- Supports excess extracellular pyrophosphate transport as a core mechanism
Pathophysiology of Chondrocalcinosis - Role of ANKH
- Extracellular PPi derives from NTP breakdown (PC-1/ENPP1) and ANK-mediated transport
- Elevated synovial PPi promotes CPP crystal nucleation
- ANKH mutations cause familial CPPD
- No therapy currently dissolves established CPP crystal deposits
Chondrocalcinosis and TKA: Knee Society Scores, ROM and Revision
- Chondrocalcinosis common at TKA (34% of men, 24% of women)
- Knee Society knee and function scores similar with or without chondrocalcinosis
- Revision rates not different (3.6% vs 2.2%, p=0.2)
- Severe synovitis with visible CPPD undergoing synovectomy had lower final ROM and scores
Anakinra for Refractory Acute CPP Crystal Arthritis
- Five patients (4 male) treated with anakinra 100 mg/day subcutaneously for 3 days
- Four showed rapid clinical and biochemical response at a mean of 3 days
- Pain (VAS) fell from 60 to 10 mm; CRP fell from 58 to 5 mg/L
- Well tolerated; one injection-site reaction, no infection
Epidemiology of CPP and Basic Calcium Phosphate Crystal Arthritis
- CPPD prevalence rises steeply with age and associates strongly with OA
- May reflect a generalised articular predisposition and low cortical bone mineral density
- CPP and basic calcium phosphate crystals frequently coexist in OA joints
- Direction of causality between CPPD and OA remains uncertain
Modern CPPD Disease Review (incl. 2023 ACR/EULAR Classification)
- Likely the commonest inflammatory arthritis in people over 60 years
- Crystals activate the NLRP3 inflammasome; no agent dissolves CPP crystals
- Prednisone offers a favourable benefit-risk ratio for acute attacks; low-dose colchicine is also effective
- Colchicine, low-dose methotrexate and hydroxychloroquine may help prophylaxis; IL-1/IL-6 blockade for refractory disease