Fragility Fracture | Assess for Ring Involvement
- Key Question: Is the posterior ring involved? Isolated rami = Stable. Posterior injury = Consider instability.
- Population: Often elderly with fragility fractures (low-energy). Young with high-energy trauma.
- Imaging: CT Pelvis to assess posterior ring (Sacrum, SI joints).
- Treatment: Isolated rami = Conservative (Analgesia, Mobility). Ring involvement = May need fixation.
- Goal: Early mobilization. Prevent immobility complications.
- “Pubic rami fractures are common fragility fractures in the elderly.
- “ALWAYS image the posterior ring (CT) - a ring cannot break in one place only.
- “Lateral Compression Type 1 (LC-1) = Rami + Sacral compression. Usually stable.
- “Focus on early mobilization to prevent immobility complications.
A Ring Breaks in Two Places. If rami are fractured, LOOK for posterior injury. May be subtle on X-ray.
Biggest Risk. Prolonged immobility leads to DVT, PE, Pneumonia, Deconditioning, Death. Mobilize early.
Osteoporosis Workup. Pubic rami fractures in elderly = Osteoporosis. Start treatment.
In Young Patients. High-energy rami fractures may have bladder/urethral injury. Check for hematuria.
- Isolated Rami
- Intact
- With Ring (e.g., LC-1)
- Sacral compression / SI injury
- Isolated Rami
- Stable
- With Ring (e.g., LC-1)
- Usually Stable (LC-1) but assess
- Isolated Rami
- Conservative
- With Ring (e.g., LC-1)
- Conservative or ORIF
- Isolated Rami
- CT to confirm
- With Ring (e.g., LC-1)
- CT shows sacral fracture
- Isolated Rami
- Good
- With Ring (e.g., LC-1)
- May have chronic pain
RING = 2Ring Rule
Hook:A ring breaks in TWO places.
Rami + SacrumLC-1 Pattern
Hook:LC-1 = Rami + Sacral compression.
Overview and Epidemiology
Pubic rami fractures involve the superior and/or inferior pubic rami. They may be isolated (ring intact) or associated with posterior ring injury (sacral fracture, SI joint injury).
- Elderly Fragility Fractures: Most common presentation. Low-energy fall.
- Young High-Energy: MVA, Fall from height. Often part of major pelvic ring injury.
- Incidence: Very common fragility fracture. Often under-recognized.
Anatomy and Pathophysiology
- Superior Pubic Ramus: Connects pubic body to acetabulum (forms anterior column).
- Inferior Pubic Ramus: Connects pubic body to ischium.
- Pubic Symphysis: Fibrocartilaginous joint at midline.
- The pelvic ring is a closed loop: Sacrum, SI joints, Innominate bones (Ilium, Ischium, Pubis), Symphysis.
- A complete ring cannot break in only one place. If rami are fractured, look posteriorly.
- Insufficiency Fractures: Osteoporotic bone can have incomplete or subtle posterior fractures (Sacral insufficiency fractures).
Classification
Simple Classification
- Isolated Rami: Superior and/or Inferior rami only. Posterior ring intact on CT.
- With Ring Involvement: Rami + Sacral fracture (LC-1) or SI injury or Contralateral rami.
CT is essential to determine this.
Clinical Assessment
- Mechanism: Low-energy fall (elderly)? High-energy (young)?
- Pain Location: Groin, anterior pelvis.
- Mobility: Can they walk? Weight-bear?
- Tenderness: Pubic rami (groin/anterior pelvis).
- Deformity: Usually none (isolated stable fractures).
- Compression/Distraction: May elicit pain.
- Gait: Antalgic.
- GU Exam: Blood at meatus? Urethral injury in high-energy (especially males).
- PR/PV Exam: Assess for associated injury.
Lower Urinary Tract Injury with Anterior Pelvic Fractures
The pitfalls box and GU examination both flag "bladder/urethral injury, check for haematuria," but the entity itself deserves development — it is the limb-and-life-relevant association of the anterior ring and the one that changes your very first action at the bedside. It is a young, high-energy problem (straddle injury, fall astride, anteroposterior-compression patterns), not a feature of the elderly low-energy fragility fracture.
- The longer male urethra is the one at risk. The membranous urethra at the urogenital diaphragm is the classic site in pelvic-fracture (anteroposterior) injuries; the bulbar urethra is torn in straddle mechanisms.
- Signs: blood at the external meatus (the cardinal sign), inability to pass urine, a high-riding or boggy / impalpable prostate on rectal examination, and a perineal or scrotal "butterfly" haematoma.
- The rule that wins marks: if a urethral injury is suspected, do NOT pass a urethral catheter. Perform a retrograde urethrogram first — blind catheterisation can convert a partial tear into a complete disruption and worsen later stricture.
- Gross haematuria is the cardinal sign and mandates a CT cystogram (retrograde gravity filling, not just a passively clamped catheter).
- Extraperitoneal rupture is the common pattern with pelvic-ring fractures and is usually managed with catheter drainage alone.
- Intraperitoneal rupture (free leak into the peritoneal cavity, often a dome tear) requires operative repair.
In a young patient with an anterior-ring/rami fracture, blood at the meatus, a high-riding prostate or a perineal haematoma means a suspected urethral injury: retrograde urethrogram before any catheter. Gross haematuria points instead to a bladder injury → CT cystogram, with extraperitoneal tears drained and intraperitoneal tears repaired. Involve urology early.
Investigations
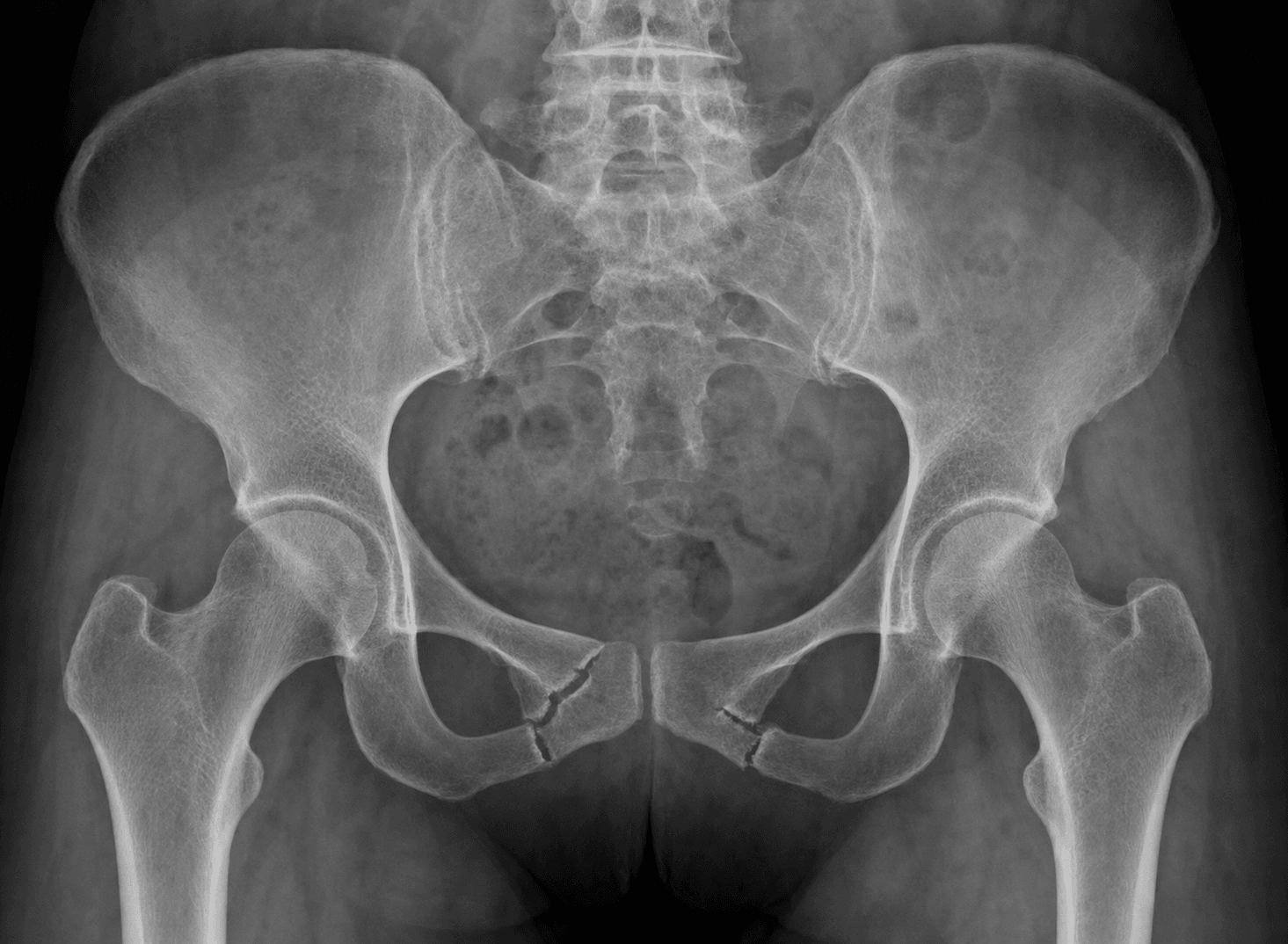
- X-ray (AP Pelvis): Shows rami fractures. May miss posterior injury.
- CT Pelvis: Essential. Assess posterior ring (Sacrum, SI joints).
- MRI: If CT negative but high clinical suspicion. For occult sacral insufficiency fractures.
- Rami Fractures: Usually visible on X-ray.
- Sacral Compression (LC-1): May be subtle on CT. Look for buckling of sacral ala.
- Sacral Insufficiency Fracture: Classic 'H-sign' (Honda sign) on bone scan / MRI (bilateral sacral ala + transverse fractures).
Differential Diagnosis
The elderly patient with groin or buttock pain and inability to weight-bear is not always a rami fracture. Distinguish:
- Discriminating Feature
- Anterior pelvic / groin tenderness, ring tenderness; often able to lie still
- Key Test
- AP pelvis then CT for posterior ring
- Discriminating Feature
- Pain on log-roll, shortened/externally rotated leg, axial load pain
- Key Test
- MRI hip if radiograph negative
- Discriminating Feature
- Low back / buttock pain, sacral tenderness, may have no rami fracture
- Key Test
- MRI / bone scan: Honda (H) sign
- Discriminating Feature
- Atraumatic or trivial-trauma pain, lytic lesion, weight loss, raised markers
- Key Test
- CT, bloods (Ca, ESR, electrophoresis), bone scan
- Discriminating Feature
- Pain on axial loading through the femur, present in ~29% with rami fractures on CT
- Key Test
- CT pelvis
- Discriminating Feature
- No bony tenderness, normal imaging, mechanical pain
- Key Test
- Clinical, exclude fracture first
An elderly faller who cannot weight-bear with a normal pelvic radiograph may have an occult femoral neck fracture, not just a rami fracture. If pain persists or examination points to the hip, obtain MRI (or CT) before attributing everything to the rami.
Management Algorithm
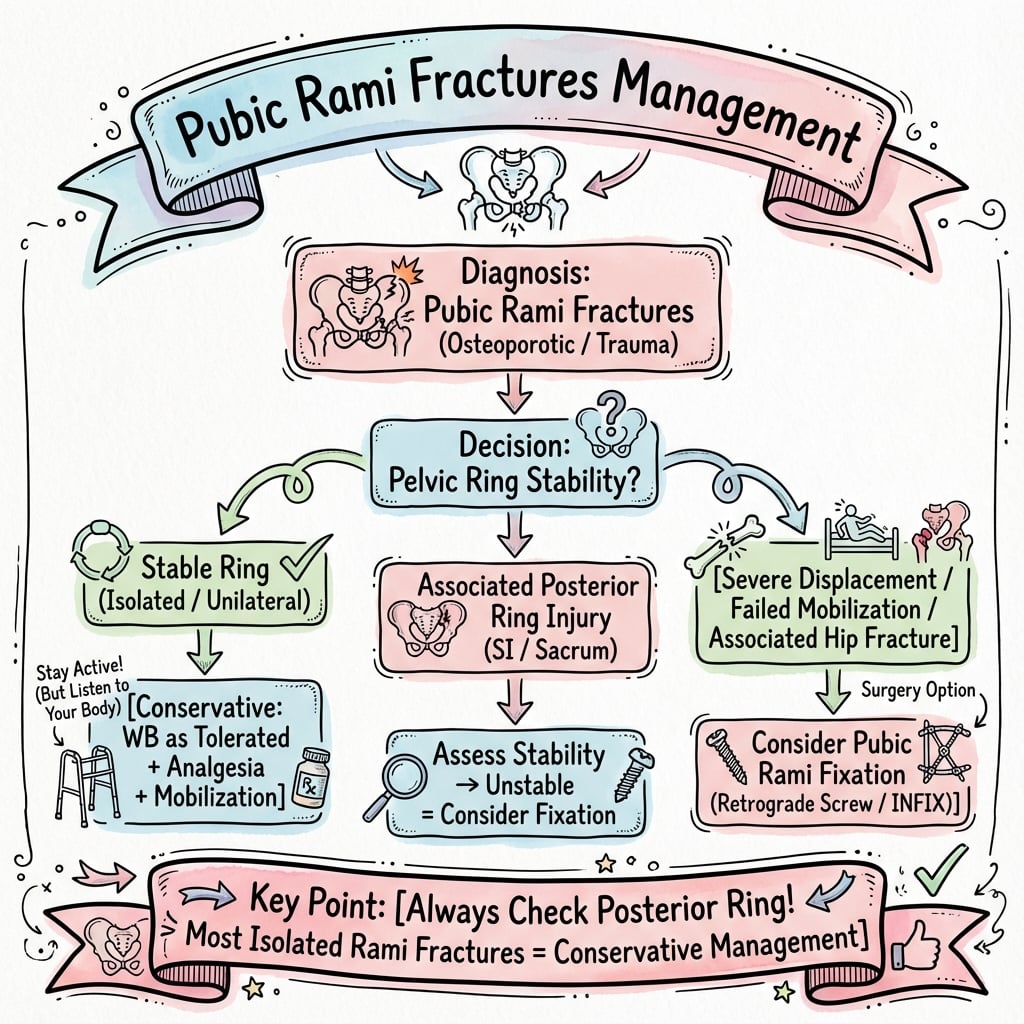
Isolated Rami (Ring Intact)
Conservative Management.
- Analgesia: Multimodal. Paracetamol, NSAIDs (caution in elderly), Opioids PRN.
- Early Mobilization: WBAT with walker/frame. Physio input Day 1.
- DVT Prophylaxis: Chemical + Mechanical.
- Osteoporosis: Start treatment (Calcium, Vitamin D, Bisphosphonate/Denosumab).
- Discharge Planning: Home vs Rehabilitation.
Goal: Get them moving. Prevent immobility complications.
Surgical Technique
Sacroplasty for Sacral Insufficiency Fractures
- Painful sacral insufficiency fracture
- Failed conservative management (still unable to mobilize)
- No neurological deficit
- Position: Prone on radiolucent table
- Guidance: Fluoroscopy or CT-guided
- Access: Trocar needles placed into sacral ala bilaterally
- Cement: PMMA injected into fracture site under live imaging
- Volume: Usually 2-4ml per side
- Significant pain relief in 80-90%
- Allows earlier mobilization
Reserved for fractures not responding to conservative care.
Complications
- Risk Factor
- Immobility
- Prevention/Management
- Early mobilization + Prophylaxis
- Risk Factor
- Bed rest
- Prevention/Management
- Early mobilization + Resp physio
- Risk Factor
- Bed rest
- Prevention/Management
- Early mobilization
- Risk Factor
- Immobility
- Prevention/Management
- Pressure care
- Risk Factor
- Sacral involvement
- Prevention/Management
- Analgesia / Sacroplasty
- Risk Factor
- Frailty, Immobility
- Prevention/Management
- Orthogeriatric care
Mortality:
- 1-year mortality for elderly pelvic fragility fractures is significant (10-20%).
- Similar to hip fractures.
- Orthogeriatric model of care improves outcomes.
The Orthogeriatric / Fragility-Fracture Care Pathway
The topic repeatedly tells you to "treat it like a hip fracture" and invokes the "orthogeriatric model," but never says what that pathway actually delivers — yet that pathway, not the fracture pattern, is what determines the elderly outcome. Because one-year mortality and loss of independence after a fragility pelvic fracture approach those of a hip fracture, the modern standard is to manage these patients on the same hip-fracture pathway, with shared orthopaedic and geriatric-medicine care from admission.
- Prompt, opioid-sparing analgesia — multimodal, with consideration of regional blocks — so the patient can actually move; pain that prevents mobilisation is itself a driver of mortality.
- Mobilisation from day 1 with physiotherapy, weight-bearing as tolerated, and an aid (frame/walker); the explicit aim is to break the immobility cascade (DVT/PE, pneumonia, deconditioning, pressure injury).
- Delirium prevention and screening (e.g. the 4AT), with reorientation, sensory aids, hydration, sleep hygiene, and avoidance of precipitating drugs.
- Pressure-area, continence, nutrition and hydration care, plus review and deprescribing of falls-risk and sedating medications.
- Venous thromboembolism risk assessment and appropriate prophylaxis.
- Enrol the patient in a fracture liaison service, arrange bone-density assessment, and start the osteoporosis work-up; this fragility fracture is a sentinel event signalling high future fracture risk. (Specific drug selection — anti-resorptive vs anabolic agents — is developed in the osteoporosis topic.)
- Undertake a multifactorial falls assessment (gait/balance, vision, postural blood pressure, home hazards) to prevent the next fracture.
- National hip-fracture programmes and their best-practice standards (early surgery where relevant, orthogeriatric review, bone-health and falls assessment) increasingly bring pelvic fragility fractures onto the same audited pathway, recognising them as an equivalent frailty event rather than a benign isolated injury.
A fragility pelvic/rami fracture carries hip-fracture-level mortality and loss of independence, so it earns hip-fracture-level care: orthogeriatric co-management, day-1 mobilisation, delirium and pressure-care bundles, a fracture liaison service for bone health, and a falls assessment. The pathway, not the fracture line, decides the outcome.
MOBILEFragility Fracture Protocol
Hook:MOBILE for fragility rami fractures.
Postoperative Care
- Mobilize Day 1.
- Walker/Frame.
- Physio daily.
- Discharge when safe (Home vs Rehab).
- Mobilize same day or next day.
- Weight-bear as tolerated.
- Follow-up X-ray.
Outcomes
- Isolated Rami: Good outcomes if mobilized early.
- With Ring/Sacral: May have chronic pain. Sacroplasty can help.
- Elderly Frailty: High morbidity/mortality from immobility.
Guidelines, Registries & Global Practice
Global epidemiology:
- Fragility fractures of the pelvis are rising rapidly with population ageing; the typical patient is a woman in her 80s after a low-energy fall.
- Women are affected roughly 5-6 times more often than men, reflecting postmenopausal bone loss.
- One-year mortality (around 15-20%) and loss of independence approach those of hip fracture, making this a sentinel frailty event rather than a benign injury.
Side-by-side guidance:
- Core Recommendation
- Classify by posterior instability (FFP I-IV); image the whole ring with CT; reserve surgery for higher grades or failed mobilization.
- Core Recommendation
- Manage as a fragility fracture on an orthogeriatric pathway: early mobilization, bone-health assessment, falls prevention.
- Core Recommendation
- Treat the underlying osteoporosis after any fragility fracture; close the post-fracture care gap with anti-resorptive or anabolic therapy.
- Core Recommendation
- Increasing use of minimally invasive posterior fixation (sacroiliac/transsacral screws) for unstable FFP III-IV in fit elderly patients.
- No dedicated pelvic-fragility registry exists; data come from national hip-fracture registries and trauma databases, which increasingly capture pelvic fragility fractures under the same frailty pathways.
- Bone-health drugs (bisphosphonates, denosumab, and anabolic agents such as teriparatide/romosozumab) are standard secondary prevention after a fragility fracture; agent choice and access vary by region and fracture risk.
- High-resource settings: routine CT, orthogeriatric co-management, fracture liaison services, and percutaneous fixation/sacroplasty for refractory pain.
- Limited-resource settings: diagnosis often rests on plain radiographs (risking missed posterior injury), with conservative analgesia and mobilization the mainstay and surgery reserved for clear instability.
Controversies & Areas of Uncertainty
The dominant pattern (rami + non-displaced unilateral sacral fracture) sits in a grey zone. A randomized pilot found no functional, pain or mortality advantage for surgery at 1 year, but it was small and underpowered. Most centres start conservatively and fix only those who fail to mobilize.
CT uncovers a posterior lesion in the large majority, yet most are still treated conservatively. The debate is whether universal CT changes management enough to justify the dose/cost, or whether it should be reserved for persistent pain or inability to mobilize.
Cohort data show rapid pain relief, but there is no high-quality randomized comparison against optimized conservative care, so its true added benefit and patient selection remain debated.
Interobserver agreement on the FFP grade is only moderate, worst exactly where it matters most — complete vs incomplete sacral fractures that swing the operative decision.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is your assessment and management?”
“Explain the 'Ring Rule'.”
“Discuss the mortality risk.”
MCQ Practice Points
Q: Why must you image the posterior pelvis if pubic rami are fractured? A: A ring cannot break in only one place. If the anterior ring (rami) is broken, there is likely a posterior injury (sacral fracture, SI injury).
Q: What is the classic LC-1 injury pattern? A: Ipsilateral pubic rami fractures (anterior) + Ipsilateral sacral compression (posterior).
Q: What is the treatment for isolated pubic rami fractures? A: Conservative - Analgesia, Early Mobilization (WBAT), DVT Prophylaxis, Osteoporosis Treatment.
Q: What is sacroplasty? A: Percutaneous cement injection into a symptomatic sacral insufficiency fracture to provide pain relief and allow mobilization.
Q: What is the 1-year mortality for elderly patients with pelvic fragility fractures? A: 10-20%, similar to hip fractures. Immobility is the main risk factor.
Key Points
- Ring breaks in 2 places
- CT to assess posterior
- LC-1 = Rami + Sacrum
- Mobilize early
Treatment
- Conservative most cases
- Analgesia + Mobilize
- DVT prophylaxis
- Osteoporosis treatment
Sacroplasty
- For painful sacral insufficiency fractures
- Cement injection (PMMA)
- Pain relief + Earlier Mobility
- Consider for non-union sacral fractures
Mortality
- 10-20% at 1 year (elderly)
- Similar mortality to hip fractures
- Immobility is the killer
- Fragility fracture = fall risk protocol
Evidence Base
FFP Classification (Landmark)
- Comprehensive classification of Fragility Fractures of the Pelvis (FFP) from 245 consecutive patients.
- Graded I to IV by increasing instability (anterior only, non-displaced posterior, displaced unilateral posterior, bilateral/displaced posterior).
- Most FFP are minimally displaced and managed conservatively; higher grades and progressive displacement favour surgical stabilization.
Occult Posterior Ring Injury on CT
- 177 patients with pubic rami fractures and a CT at admission.
- A posterior pelvic ring injury was present on CT in 96.8% of patients who had no obvious posterior injury on the AP radiograph.
- A coexisting acetabular fracture was found in 28.8%; 30% of those with dorsal injury ultimately required operative treatment.
Mortality & Loss of Independence
- 132 patients aged over 65 with low-energy pubic rami fractures; mean age 84 years, women affected 6x more often.
- One-year mortality was 18.5% and almost 30% permanently lost their prior independence.
- A concomitant posterior ring lesion was found on CT in 54%; only 4% required secondary fixation.
Operative vs Conservative FFP II (RCT)
- Randomized pilot of 39 patients over 60 with FFP II (rami + non-displaced unilateral sacral fracture): 17 operative vs 22 conservative.
- No significant difference at 12 months in Barthel index, pain (VAS), quality of life (EQ-5D) or Tinetti gait, and no mortality difference.
- Two conservative patients crossed over to surgery for persistent pain/immobility.
Sacroplasty for Sacral Insufficiency Fractures
- Prospective multicentre cohort of 52 osteoporotic patients undergoing percutaneous sacroplasty.
- Mean VAS pain fell from 8.1 at baseline to 3.4 within 30 minutes and 0.8 at 52 weeks.
- One transient S1 radiculitis was the only significant complication.
FFP: From Eminence to Evidence (Review)
- Synthesis of the evidence accumulated since the 2013 FFP classification.
- Mortality exceeds the reference population and is lower after operative treatment, at the cost of surgical complications.
- Mobility, independence and quality of life remain worse than pre-injury regardless of FFP grade or treatment type.
FFP Classification Reliability
- 100 CT scans of low-energy pelvic ring injuries classified by 4 observers.
- Interobserver reliability was only moderate (kappa 0.42-0.59); intraobserver substantial (0.68-0.72).
- Reliability was poorest for FFP IIc/IIIc/IVb subtypes involving a complete sacral fracture.