Wells Score | CTPA Gold Standard | Risk Stratify | Anticoagulate or Thrombolyse
- Wells score estimates PE probability - guides need for CTPA
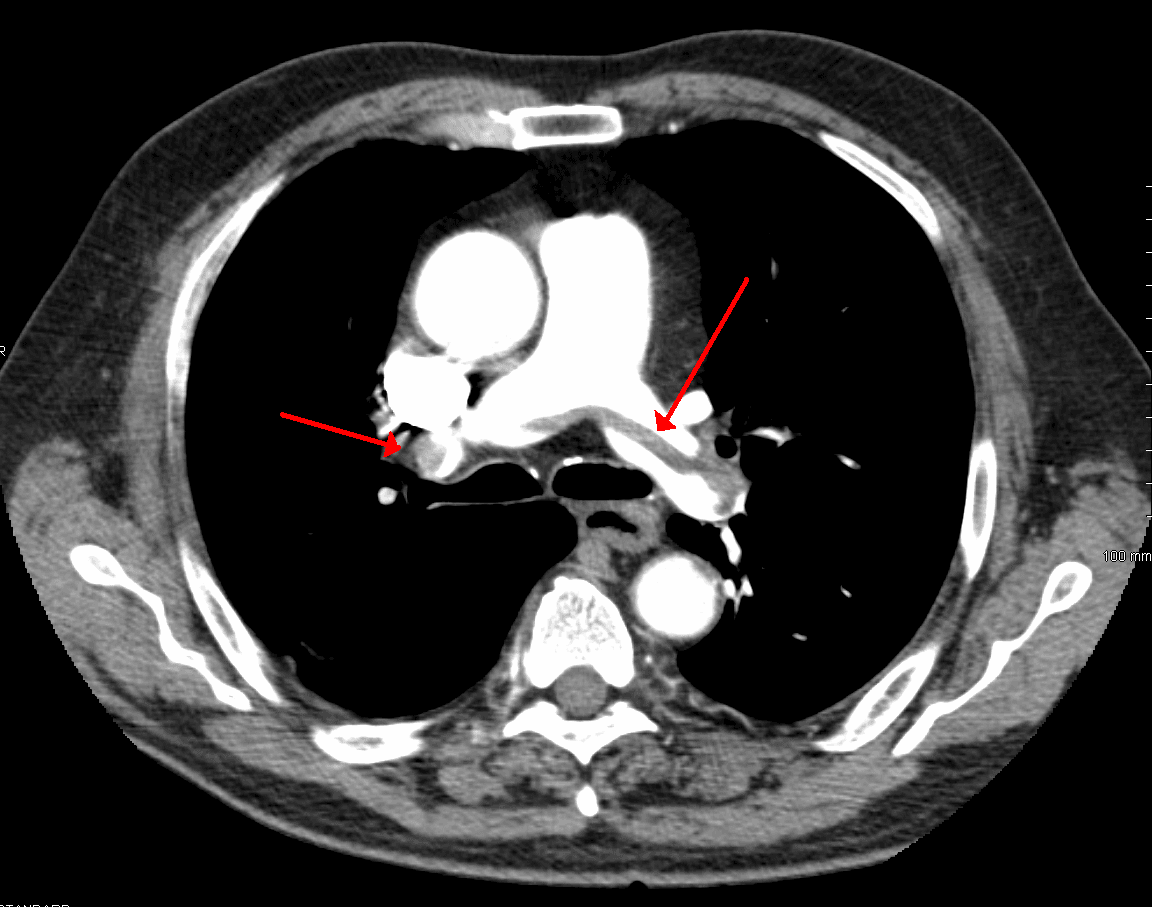
- CTPA is gold standard (95% sensitive) - VQ scan if contrast contraindicated
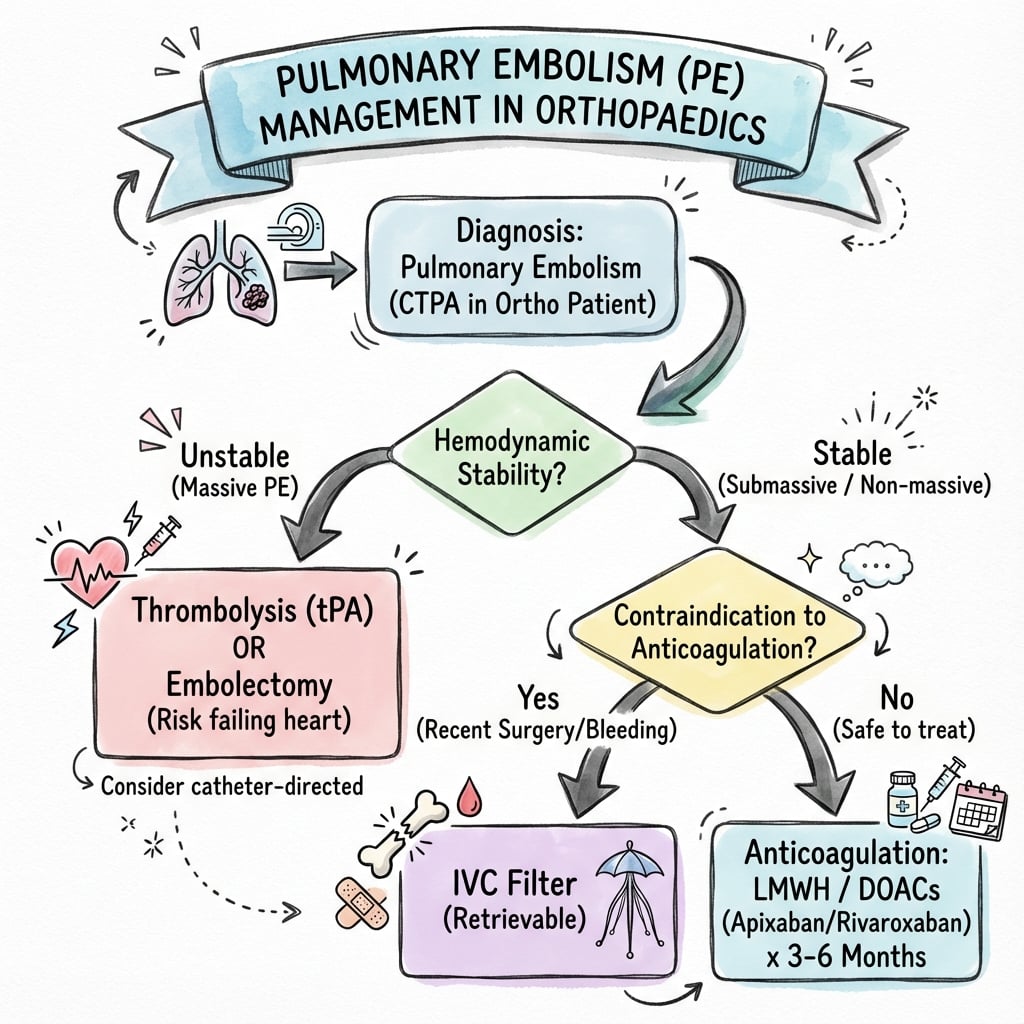
- Risk stratification determines treatment: Massive = thrombolysis, Low-risk = anticoagulation only
- Thrombolysis saves lives in massive PE but 1-5% intracranial bleed risk
- IVC filters ONLY if anticoagulation absolutely contraindicated - NOT routine
- “PERC rule: If ALL 8 criteria negative AND low clinical suspicion, PE excluded (no D-dimer needed)
- “Massive PE = hemodynamic instability (SBP less than 90) - thrombolyse immediately
- “D-dimer negative with low Wells score excludes PE (99% NPV)
- “Postop PE is provoked - anticoagulate 3 months, NOT indefinite
Massive PE = sustained hypotension (SBP less than 90 mmHg) or cardiac arrest. This is an emergency. Give alteplase 50-100mg over 2 hours IMMEDIATELY after confirming on CTPA. Mortality 30% if untreated vs 10% with thrombolysis.
IVC filters do NOT prevent PE or reduce mortality. Only use if absolute contraindication to anticoagulation (active bleeding, recent neurosurgery). PREPIC trial showed filters increase DVT without reducing PE death.
Massive (high-risk): Thrombolysis. Submassive (intermediate): Anticoagulation, watch for deterioration. Low-risk: Anticoagulation, consider outpatient if PESI low risk. Do NOT thrombolyse submassive routinely.
CTPA has 95% sensitivity and 98% specificity for PE. Direct visualization of thrombus in pulmonary arteries. VQ scan only if contrast contraindicated (renal failure, severe allergy). Wells score determines who gets CTPA.
- Wells Score
- Not needed
- Next Step
- No further testing
- Treatment
- PE excluded - no D-dimer needed
- Wells Score
- 0-3 (PE unlikely)
- Next Step
- D-dimer first
- Treatment
- If negative stop. If positive CTPA
- Wells Score
- 4+ (PE likely)
- Next Step
- Skip D-dimer, go to CTPA
- Treatment
- If positive, anticoagulate
- Wells Score
- Not needed
- Next Step
- CTPA if stable, or empiric thrombolysis if crashing
- Treatment
- Alteplase 50-100mg over 2h + anticoagulation
PEACH 3-3-1.5Wells Score for Pulmonary Embolism
Hook:PEACH 3-3-1.5: Score less than 4 = PE unlikely (D-dimer), score 4+ = PE likely (CTPA). Remember Prior DVT, Elevated HR, Alternative unlikely, Cancer, Hemoptysis!
PERC 8PERC Rule (PE Rule-Out Criteria)
Hook:If ALL 8 PERC criteria negative AND low clinical suspicion, PE excluded - NO D-dimer needed! Saves unnecessary testing.
Overview and Clinical Significance
Pulmonary embolism is the LEADING cause of preventable perioperative death in orthopaedic surgery. THA and TKA have 10-20% PE risk without prophylaxis. With modern prophylaxis, risk is 0.5-2% but still significant. Early recognition and treatment are life-saving.
- Incidence: 60-100 per 100,000 population annually
- Ortho surgery (with prophylaxis): 0.5-2%
- THA/TKA (without prophylaxis): 10-20%
- Peak: Days 3-7 postoperatively
- Mortality: 2-8% overall, 30% if massive PE untreated
- Fatal PE: Often first presentation (25% sudden death)
- Massive PE: 30% mortality if untreated, 10% with thrombolysis
- Submassive PE: 10-15% deterioration to massive
- Post-PE syndrome: Chronic dyspnea 50% at 1 year
- Chronic thromboembolic pulmonary hypertension (CTEPH): 2-4%
- Recurrent VTE: 10-30% over 5 years if inadequately treated
Pathophysiology
Mechanism of Pulmonary Embolism
PE results from venous thrombus (95% from lower limb DVT) embolizing to pulmonary circulation:
- Venous stasis (immobility, surgery)
- Endothelial injury (surgical trauma, central lines)
- Hypercoagulability (inflammatory response, cancer, thrombophilia)
- Thrombus breaks off from DVT (usually proximal leg veins)
- Travels through IVC and right heart
- Lodges in pulmonary arteries (lobar, segmental, or subsegmental)
- Small PE: Minimal effect, may be asymptomatic
- Moderate PE: Ventilation-perfusion mismatch, hypoxia, tachycardia
- Massive PE: Acute RV failure from sudden afterload increase, cardiogenic shock
- Dead space ventilation (ventilation without perfusion)
- Hypoxemia from V/Q mismatch
- Hyperventilation and hypocapnia (initially)
- Atelectasis from surfactant depletion
Massive PE causes acute RV failure because the thin-walled RV cannot generate sufficient pressure to overcome sudden increase in pulmonary vascular resistance. RV dilatation impairs LV filling (ventricular interdependence), reducing cardiac output and causing cardiogenic shock.
Orthopaedic Surgery Risk Factors
- Prolonged immobility: Pre-op, intra-op (anesthesia), post-op
- Direct vascular trauma: Hip and knee surgery near large veins
- Bone marrow embolization: Fat and marrow emboli activate coagulation
- Cement polymerization: Thermal injury, microemboli
- Tourniquet use: Ischemia-reperfusion injury, endothelial damage
- Inflammatory response: Massive cytokine release activates coagulation cascade
- THA: 10-20% symptomatic PE, 0.5-1% fatal PE
- TKA: 10-20% symptomatic PE, 0.3-0.7% fatal PE
- Hip fracture surgery: 10-15% PE
- Spine surgery: 2-5% PE
- Arthroscopy: Less than 1% PE (but still occurs)
Classification
PE Risk Stratification Classification
- Massive (High-Risk): Sustained hypotension (SBP less than 90 mmHg for 15+ minutes), cardiac arrest, or cardiogenic shock
- Submassive (Intermediate-Risk): Normotensive BUT RV dysfunction on echo/CT OR elevated troponin/BNP
- Low-Risk: Normotensive, no RV dysfunction, normal biomarkers
- Saddle PE: Thrombus at bifurcation of main pulmonary artery
- Central PE: Main or lobar pulmonary arteries
- Segmental/Subsegmental PE: Peripheral branches
- Acute PE: New thrombus, fresh clot
- Chronic thromboembolic disease: Organized thrombus, may lead to CTEPH
Clinical Presentation
25% of fatal PE present with sudden death without prior symptoms. Symptoms range from none (incidental finding) to sudden cardiovascular collapse. Maintain high index of suspicion in postoperative orthopaedic patients.
Symptoms (Nonspecific)
- Frequency
- 80-90%
- Clinical Notes
- Most common - often pleuritic
- Frequency
- 50-70%
- Clinical Notes
- Sharp, worse with inspiration (pleural irritation)
- Frequency
- 40-50%
- Clinical Notes
- Dry or productive
- Frequency
- 10-20%
- Clinical Notes
- Blood-streaked sputum (pulmonary infarction)
- Frequency
- 10-15%
- Clinical Notes
- Suggests massive PE with hypotension
- Frequency
- 30-40%
- Clinical Notes
- Concurrent DVT
Classic triad (dyspnea, pleuritic pain, hemoptysis) occurs in less than 20% of cases.
Signs
- Frequency
- 70-80%
- Significance
- Most sensitive sign
- Frequency
- 40-60%
- Significance
- Compensatory response to hypoxia
- Frequency
- 50-70%
- Significance
- V/Q mismatch
- Frequency
- 5-10%
- Significance
- MASSIVE PE - RV failure
- Frequency
- 20-30%
- Significance
- RV dysfunction
- Frequency
- 30-40%
- Significance
- Source of embolus
Clinical Syndromes
Massive (High-Risk) PE
Sustained hypotension (SBP less than 90 mmHg for 15+ minutes) OR requiring inotropes OR cardiac arrest OR cardiogenic shock.
- Severe dyspnea, often unable to speak
- Hypotension, cold peripheries
- Altered mental status (confusion from poor perfusion)
- Cyanosis
- Elevated JVP, RV gallop
- ECG: Sinus tachycardia, S1Q3T3 pattern (25%)
30% if untreated, 10% with thrombolysis.
THROMBOLYSIS (alteplase) + anticoagulation. Surgical embolectomy if thrombolysis contraindicated.
This is a medical emergency requiring immediate action.
Differential Diagnosis
- Discriminating Features
- Sudden dyspnoea, pleuritic pain, hypoxia, tachycardia, often DVT signs; peak postop days 3-7
- Key Investigation
- CTPA (filling defect); risk-stratify with echo, troponin, BNP
- Discriminating Features
- Crushing central/retrosternal pain, diaphoresis, radiation to arm/jaw; cardiac risk factors
- Key Investigation
- ECG (ST changes), serial troponin, coronary angiography
- Discriminating Features
- Fever, productive cough, focal crepitations, leucocytosis; later postop onset
- Key Investigation
- Chest X-ray (consolidation), inflammatory markers, cultures
- Discriminating Features
- Long-bone/pelvic fracture or IM nailing; petechial rash, hypoxia, confusion 24-72h postop
- Key Investigation
- Clinical (Gurd criteria), hypoxia on ABG, CT chest
- Discriminating Features
- Sudden unilateral pleuritic pain, reduced breath sounds; CVC insertion or barotrauma
- Key Investigation
- Chest X-ray / point-of-care ultrasound
- Discriminating Features
- Orthopnoea, bilateral crepitations, raised JVP, fluid overload postop
- Key Investigation
- Chest X-ray, BNP, echocardiography
- Discriminating Features
- Diagnosis of exclusion; normal SpO2, paraesthesiae, respiratory alkalosis
- Key Investigation
- Normal CTPA/D-dimer once PE excluded
Diagnostic Approach
Never order CTPA without first assessing pretest probability. Use PERC rule (very low suspicion) or Wells score (low to high suspicion) to determine who needs D-dimer vs CTPA. This reduces unnecessary radiation and contrast exposure.
PE Diagnostic Algorithm
Very low suspicion AND all PERC criteria negative? PE excluded, stop. Otherwise calculate Wells score for PE.
If Wells 0-3 (PE unlikely), check D-dimer. If NEGATIVE - PE excluded (99% NPV). If POSITIVE - proceed to CTPA.
If Wells 4+ (PE likely), skip D-dimer and go directly to CTPA. D-dimer has low utility when pretest probability is high.
CTPA is gold standard (95% sensitive). VQ scan if contrast contraindicated. If positive, risk stratify (massive/submassive/low-risk).
Check BP, echo (RV function), troponin, BNP. Classify as massive (thrombolyse), submassive (anticoagulate + monitor), or low-risk (anticoagulate +/- outpatient).
PERC Rule (PE Rule-Out Criteria)
If ALL 8 criteria are NEGATIVE AND clinical suspicion is LOW, PE is excluded (no D-dimer needed):
- Age less than 50 years
- Heart rate less than 100 bpm
- Oxygen saturation 95% or greater on room air
- No hemoptysis
- No estrogen use (OCP, HRT)
- No prior DVT or PE
- No unilateral leg swelling
- No surgery or trauma requiring hospitalization in past 4 weeks
Only use PERC if suspicion is LOW. If ANY criterion positive OR suspicion moderate/high, proceed to Wells score.
Wells Score for PE
- Points
- +3
- Points
- +3
- Points
- +1.5
- Points
- +1.5
- Points
- +1.5
- Points
- +1
- Points
- +1
Interpretation:
- Score 0-3: PE unlikely (15% prevalence) - check D-dimer
- Score 4+: PE likely (40% prevalence) - skip D-dimer, go to CTPA
Investigations
D-dimer Testing
Principle: D-dimer is fibrin degradation product elevated in VTE. High sensitivity (95-98%) but low specificity (40-60%).
- Low Wells score (less than 4)
- Negative D-dimer = PE excluded
- High negative predictive value (99%)
- Avoids unnecessary CTPA (radiation + contrast)
- High Wells score (4+) - go to CTPA
- Postoperative patients - often elevated
- Cancer, pregnancy, elderly - often elevated
- Positive D-dimer does NOT diagnose PE
- Negative D-dimer + Low Wells: PE excluded, no CTPA needed
- Positive D-dimer: Proceed to CTPA (does NOT confirm PE)
- In postop ortho patients: Often falsely elevated - CTPA may be needed regardless
In patients over 50, use cutoff of (age x 10) instead of 500 ng/mL to improve specificity.

Risk Stratification
ALL confirmed PE patients must be risk stratified to determine if they need thrombolysis (massive), close monitoring (submassive), or standard anticoagulation (low-risk). This is NOT just for prognosis - it directly impacts treatment decisions.
- Hemodynamics
- SBP less than 90 mmHg or shock or arrest
- RV Dysfunction
- Usually present
- Biomarkers
- Usually elevated
- Mortality
- 30% untreated
- Treatment
- THROMBOLYSIS + anticoagulation
- Hemodynamics
- SBP greater than 90 mmHg (normotensive)
- RV Dysfunction
- Present (echo or CT)
- Biomarkers
- Troponin or BNP elevated
- Mortality
- 10-15% deterioration
- Treatment
- Anticoagulation + close monitoring, rescue thrombolysis if deteriorates
- Hemodynamics
- SBP greater than 90 mmHg (stable)
- RV Dysfunction
- Absent
- Biomarkers
- Normal
- Mortality
- Less than 1%
- Treatment
- Anticoagulation, consider outpatient if PESI low
Assessing RV Dysfunction (for Submassive PE)
- RV dilatation: RV/LV diameter ratio greater than 0.9 (apical 4-chamber view)
- RV hypokinesis
- McConnell sign (RV free wall hypokinesis with apical sparing)
- RV/LV diameter ratio greater than 1.0 on axial images
- BNP greater than 90 pg/mL or NT-proBNP greater than 500 pg/mL
- Troponin I greater than 0.4 ng/mL
If ANY of the above present with normotensive patient = submassive PE.
H-R-SMassive vs Submassive vs Low-Risk PE
Hook:H-R-S: High-risk needs thrombolysis, RV dysfunction needs monitoring, Stable can go home!
PESI and Simplified PESI (sPESI)
The risk-stratification and management sections refer to the PESI class and the sPESI to pick out low-risk patients for outpatient care, but the score itself is worth setting out. The Pulmonary Embolism Severity Index predicts 30-day mortality from clinical variables; the simplified version (sPESI) is easier to apply at the bedside.
- Threshold for a Point
- Over 80 years
- Threshold for a Point
- Present
- Threshold for a Point
- Chronic heart failure or chronic lung disease
- Threshold for a Point
- 110 bpm or higher
- Threshold for a Point
- Below 100 mmHg
- Threshold for a Point
- Below 90%
An sPESI of 0 (none of the six present) identifies a low-risk PE with roughly 1% 30-day mortality; combined with no RV dysfunction and adequate social support, these patients are candidates for early discharge or outpatient treatment on a DOAC. Any single point (sPESI 1 or more) marks higher risk warranting admission. The original PESI adds further weighted variables - male sex, respiratory rate 30 or higher, temperature below 36 C, and altered mental status, with age scored per year - to give Classes I to V, of which Classes I-II (85 points or fewer) correspond to low risk.
Isolated Subsegmental PE: Anticoagulate or Observe?
Modern multidetector CTPA increasingly detects isolated subsegmental PE - clot confined to subsegmental arteries with no more proximal thrombus. Because some of these are false positives or clinically trivial, whether to anticoagulate is a genuine decision rather than automatic, and it is a recognised modern controversy that the evidence base (CHEST) addresses directly.
- Favours Anticoagulation
- Multiple subsegmental defects
- Favours Anticoagulation
- Concurrent proximal DVT
- Favours Anticoagulation
- Cancer, hospitalised or immobile, poor cardiopulmonary reserve
- Favours Anticoagulation
- Unprovoked or ongoing risk; markedly raised D-dimer
Isolated subsegmental PE has poor interobserver reliability on CTPA, so first satisfy yourself the finding is genuine (scan quality, ideally a second read). Guidelines (ACCP/CHEST, ESC) suggest clinical surveillance with bilateral leg ultrasound over anticoagulation when there is no proximal DVT and recurrence risk is low; anticoagulate if there is proximal DVT, active cancer, immobility, limited cardiopulmonary reserve, or strong patient preference. A post-operative orthopaedic patient with reduced mobility often falls into the higher-risk group despite the transient provocation.
Management Algorithm
Once PE is diagnosed (or strongly suspected while awaiting CTPA), start anticoagulation immediately. Delays increase mortality. Choice of agent depends on hemodynamic status, bleeding risk, and renal function.
- Advantages
- Oral from day 1, no monitoring, no LMWH lead-in
- Disadvantages
- Cost, renal impairment, limited reversal
- Typical Use
- First-line for stable PE
- Advantages
- Cheap, reversible, familiar
- Disadvantages
- LMWH injections, INR monitoring, drug interactions
- Typical Use
- Traditional approach, still used
- Advantages
- Reversible (short half-life), can use in renal failure
- Disadvantages
- IV access needed, monitoring (aPTT), HIT risk
- Typical Use
- Used in massive PE, perioperatively
- Advantages
- No monitoring, predictable
- Disadvantages
- Injections, expensive long-term
- Typical Use
- Cancer-associated PE
Direct Oral Anticoagulants (First-Line for Stable PE)
- 15mg BD for 21 days, then 20mg daily
- No LMWH lead-in needed
- Reduce to 15mg daily if CrCl 30-50
- Avoid if CrCl less than 30
- 10mg BD for 7 days, then 5mg BD
- No LMWH lead-in needed
- Reduce to 2.5mg BD if 2 of: age greater than 80, weight less than 60kg, creatinine greater than 133
- Avoid if CrCl less than 30
Oral from day 1, predictable, no monitoring, easier than warfarin, similar efficacy, lower bleeding risk.
Low-risk and submassive PE (after ruling out need for thrombolysis).
Massive PE (use IV heparin initially), CrCl less than 30, active bleeding, mechanical valve, antiphospholipid syndrome.
Treatment Duration
- Duration
- 3 months
- Rationale
- Transient risk factor removed, low recurrence risk (1-3% annually)
- Duration
- 3-6 months minimum
- Rationale
- Assess bleeding vs recurrence risk. May extend if low bleeding risk
- Duration
- Indefinite
- Rationale
- High recurrence risk (15% annually if stopped)
- Duration
- Indefinite (while active)
- Rationale
- Ongoing hypercoagulable state, high recurrence
PE occurring after orthopaedic surgery is PROVOKED (transient risk factor). Treat for 3 months only. Lower recurrence risk (1-3% annually) vs unprovoked PE. Do NOT anticoagulate indefinitely.
Thrombolysis for Massive PE
Massive PE has 30% mortality if treated with anticoagulation alone vs 10% with thrombolysis. If patient has sustained hypotension (SBP less than 90 mmHg) or cardiogenic shock, give alteplase 50-100mg IV over 2 hours IMMEDIATELY after confirming PE on CTPA.
Indications for Thrombolysis
- Sustained hypotension (SBP less than 90 mmHg for 15+ minutes) AND confirmed PE
- Cardiac arrest due to PE
- Cardiogenic shock
- Normotensive BUT severe RV dysfunction AND deteriorating clinically
- PEITHO trial showed routine thrombolysis in submassive PE reduces hemodynamic collapse (2% vs 5%) but increases major bleeding (11% vs 2%) and stroke (2% vs 0.2%)
- Current recommendation: Anticoagulation for submassive, rescue thrombolysis only if deteriorates
Thrombolytic Agents
- Dose
- 100mg IV over 2 hours OR 50mg bolus (if arrest)
- Notes
- First-line, most evidence
- Dose
- 30-50mg IV bolus (weight-based)
- Notes
- Single bolus, easier administration
- Dose
- 1.5 million units over 2 hours
- Notes
- Rarely used (antigenic, allergic reactions)
Give heparin concurrently (bolus + infusion as per protocol).
Contraindications to Thrombolysis
- Relative
- Recent minor bleeding (less than 10 days)
- Relative
- Recent major surgery (10-14 days)
- Relative
- Ischemic stroke greater than 3 months ago
- Relative
- Major trauma
- Relative
- CPR greater than 10 minutes
- Relative
- Pregnancy, first week postpartum
- Relative
- Uncontrolled hypertension (SBP greater than 180)
If absolute contraindication: Consider surgical embolectomy or catheter-directed thrombolysis.
Complications of Thrombolysis
- Incidence
- 10-15%
- Management
- Stop thrombolytic, transfuse, consider reversal (cryoprecipitate, TXA)
- Incidence
- 1-5%
- Management
- STOP thrombolytic, reverse, neurosurgical consultation
- Incidence
- 20-30%
- Management
- Local pressure, monitor
- Incidence
- 5-10%
- Management
- Antihistamines, steroids, switch to alteplase
Intracranial hemorrhage is the most feared complication - occurs in 1-5%. Risk higher in elderly, uncontrolled HTN, prior stroke.
Management Algorithm
Surgical and Interventional Options
Surgical Pulmonary Embolectomy
Massive PE with absolute contraindication to thrombolysis OR failed thrombolysis.
- Median sternotomy
- Cardiopulmonary bypass
- Direct removal of thrombus from pulmonary arteries via pulmonary arteriotomy
- Mortality 30-50% (very sick patients)
- Success depends on speed of intervention
- Reserved for last resort
Only at tertiary cardiac surgery centers.
VTE Prophylaxis in Orthopaedic Surgery
All orthopaedic surgery patients require VTE prophylaxis unless absolute contraindication. The goal is to reduce VTE risk from 10-20% to 0.5-2%. Use mechanical (TED stockings, intermittent pneumatic compression) PLUS chemical prophylaxis (LMWH, fondaparinux, rivaroxaban, or aspirin).
Risk Assessment
- Total hip arthroplasty (THA): 28-35 days
- Total knee arthroplasty (TKA): 10-14 days
- Hip fracture surgery: 28-35 days
- Spine surgery (multilevel, malignancy): 10-14 days
- Arthroscopy: 7-10 days if other risk factors (age greater than 40, obesity, prior VTE)
- Upper limb surgery: Generally low risk, prophylaxis only if additional risk factors
Prophylaxis Options
- Dose
- 40mg SC daily (20mg if weight less than 50kg or CrCl less than 30)
- Duration
- 28-35d THA, 10-14d TKA
- Role / Notes
- Widely used
- Dose
- 10mg PO daily
- Duration
- 28-35d THA, 10-14d TKA
- Role / Notes
- Oral convenience
- Dose
- 2.5mg PO BD
- Duration
- 28-35d THA, 10-14d TKA
- Role / Notes
- Oral
- Dose
- 2.5mg SC daily
- Duration
- 28-35d
- Role / Notes
- Synthetic pentasaccharide
- Dose
- 100mg PO daily
- Duration
- 28-35d (after initial LMWH)
- Role / Notes
- Cheaper, ASA trial showed non-inferiority after initial LMWH
- Dose
- Target INR 2-3
- Duration
- Rarely used now
- Role / Notes
- Replaced by DOACs
Mechanical prophylaxis:
- TED stockings (graduated compression stockings)
- Intermittent pneumatic compression (IPC) devices
- Early mobilization
Use BOTH mechanical AND chemical unless contraindication.
Timing of Prophylaxis
- LMWH/fondaparinux: 12 hours post-op (NOT pre-op if neuraxial anesthesia planned - epidural hematoma risk)
- Rivaroxaban/apixaban: 6-10 hours post-op (once hemostasis achieved)
- Aspirin: Post-op day 1
- LMWH given pre-op requires 12-24 hour gap before neuraxial
- LMWH given post-op requires 12 hour gap before catheter removal
- DOACs require 24 hour gap before neuraxial
Contraindications to Chemical Prophylaxis
- Active bleeding
- Severe bleeding risk (e.g., bleeding peptic ulcer, recent intracranial hemorrhage)
- HIT with thrombosis (cannot use heparin-based agents)
- Recent neurosurgery or ophthalmologic surgery (balance risk vs benefit)
- Platelets less than 50,000 (relative, depends on bleeding risk)
- Severe renal impairment (avoid LMWH/fondaparinux, use UFH or reduce dose)
Use mechanical prophylaxis alone, consider IVC filter if very high risk (NOT routinely recommended).
Complications and Long-Term Sequelae
Acute Complications of PE
- Incidence
- 10-30%
- Management
- Thrombolysis reduces to 10%
- Incidence
- 5-10%
- Management
- Thrombolysis, inotropes, consider ECMO
- Incidence
- 2-5%
- Management
- CPR, thrombolysis, consider ECMO
- Incidence
- 5-10% if inadequate anticoagulation
- Management
- Ensure therapeutic anticoagulation, consider IVC filter if recurrent despite therapy
- Incidence
- 1-3% major bleed annually
- Management
- Reversal agents, transfusion
Chronic Complications
- Incidence: 2-4% of PE survivors
- Pathophysiology: Unresolved thrombus causes chronic pulmonary artery obstruction and pulmonary hypertension
- Presentation: Progressive dyspnea, exercise intolerance, right heart failure
- Diagnosis: RV systolic pressure greater than 25 mmHg on echo, confirmed by right heart catheterization + V/Q scan showing perfusion defects
- Treatment: Pulmonary thromboendarterectomy (surgical removal of organized thrombus) OR balloon pulmonary angioplasty OR pulmonary vasodilators (sildenafil, riociguat)
- Screen for CTEPH if persistent dyspnea 3-6 months post-PE
- Chronic dyspnea without pulmonary hypertension
- Incidence: 50% at 1 year
- Cause: Deconditioning, anxiety, subclinical RV dysfunction
- Management: Pulmonary rehabilitation, exercise training
- 10% first year (unprovoked), 1-3% annual (provoked)
- Prevention: Appropriate duration anticoagulation
- Risk factors for recurrence: Unprovoked PE, residual thrombus, thrombophilia, cancer
Postoperative Care
Post-PE Monitoring
- Massive PE: ICU admission, continuous monitoring
- Submassive PE: HDU/step-down for 24-48 hours
- Low-risk PE: Ward care or outpatient if PESI Class I-II
- Vital signs every 4-6 hours
- Oxygen saturation target greater than 94%
- Watch for deterioration (dropping BP, worsening dyspnea)
- DOACs: No routine monitoring required
- Warfarin: INR target 2-3, weekly until stable
- LMWH: Anti-Xa levels if renal impairment or extreme weight
Outcomes
PE Outcomes Summary
- Massive PE untreated: 30%
- Massive PE with thrombolysis: 10%
- Submassive PE: 3-15%
- Low-risk PE: Less than 1%
- Provoked PE (post-surgery): 1-3% annual after stopping anticoagulation
- Unprovoked PE: 10-15% annual if anticoagulation stopped
- CTEPH: 2-4% of PE survivors
- Post-PE syndrome: 50% have persistent dyspnea at 1 year
- Bleeding from anticoagulation: 1-3% major bleed annually
Guidelines, Registries & Global Practice
Side-by-Side Guideline Guidance
- PE diagnosis
- Probability then D-dimer then CTPA; age-adjusted D-dimer (Class I)
- High-risk (massive) PE
- Immediate systemic thrombolysis; embolectomy/catheter therapy if contraindicated (Class I)
- Intermediate (submassive) PE
- Anticoagulate + monitor; rescue reperfusion if decompensation (Class I)
- Anticoagulant of choice
- DOAC first-line (Class I)
- Ortho VTE prophylaxis
- Risk-adapted; defers to surgical guidelines
- PE diagnosis
- Endorses validated algorithms
- High-risk (massive) PE
- Systemic thrombolysis for PE with hypotension (Grade 2B)
- Intermediate (submassive) PE
- Anticoagulation, NOT routine thrombolysis (Grade 2C)
- Anticoagulant of choice
- DOAC over VKA for non-cancer (Grade 2B)
- Ortho VTE prophylaxis
- Covered in AT9/AT10 orthopaedic chapters
- PE diagnosis
- Two-level Wells then D-dimer/CTPA; V/Q-SPECT alternative
- High-risk (massive) PE
- Continuous IV UFH + thrombolysis if haemodynamic instability
- Intermediate (submassive) PE
- Anticoagulate, individualise; no routine thrombolysis
- Anticoagulant of choice
- Apixaban or rivaroxaban first-line
- Ortho VTE prophylaxis
- NG89: mechanical + pharmacological prophylaxis, risk-assessed
- PE diagnosis
- Not a diagnostic guideline
- High-risk (massive) PE
- Per medical/ICU guidance
- Intermediate (submassive) PE
- Per medical/ICU guidance
- Anticoagulant of choice
- Pharmacological agent at surgeon discretion
- Ortho VTE prophylaxis
- Pharmacological +/- mechanical prophylaxis; against routine post-discharge duplex screening
All major bodies (ESC/ERS, ACCP/CHEST, NICE) agree on three points: (1) risk-stratify every confirmed PE; (2) systemic thrombolysis only for high-risk/haemodynamically unstable PE, NOT routinely for intermediate-risk; and (3) DOACs are first-line anticoagulation for most haemodynamically stable patients. Divergence is mainly in prophylaxis duration and agent selection for orthopaedic surgery.
MCQ Practice Points
Q: A patient has Wells score of 2 for PE. What is the next step? A: D-dimer. Wells less than 4 = PE unlikely, check D-dimer. If negative, PE excluded. If positive, CTPA.
Q: What defines massive PE? A: Sustained hypotension (SBP less than 90 mmHg for 15+ minutes) OR cardiac arrest OR cardiogenic shock. Massive PE requires thrombolysis. Submassive PE is normotensive BUT has RV dysfunction.
Q: What is the indication for thrombolysis in PE? A: Massive PE (hemodynamic instability). PEITHO trial showed NO benefit for routine thrombolysis in submassive PE, only increased bleeding.
Q: What did the PREPIC trial show about IVC filters? A: Filters reduce early PE but increase DVT and do NOT reduce mortality. Only use if absolute contraindication to anticoagulation.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 70-year-old woman develops sudden onset dyspnea and pleuritic chest pain on day 5 after total hip arthroplasty. Vitals: BP 130/80, HR 110, RR 24, SpO2 92% on room air. How would you assess and manage?”
“A 65-year-old man collapses 3 days after hip fracture surgery. On arrival to ED, BP 75/40, HR 130, RR 30, SpO2 85% on high-flow oxygen. CTPA shows large bilateral PE with RV/LV ratio of 1.5. He had neurosurgery for subdural hematoma 6 weeks ago. What is your management?”
“A 55-year-old woman has confirmed PE on CTPA 1 week after TKA. She is normotensive (BP 125/75) but echo shows RV/LV ratio 1.1 and troponin is elevated. She was on rivaroxaban 10mg daily for prophylaxis but admits she stopped taking it 3 days ago. How do you manage? Also, what prophylaxis protocol should have been used?”
Wells Score for PE (PEACH 3-3-1.5)
- Prior DVT/PE +1.5, Elevated HR (greater than 100) +1.5
- Alternative diagnosis unlikely +3, Cancer active +1, Hemoptysis +1
- Clinical DVT signs +3, Surgery/immobilization (4 weeks) +1.5
- Score less than 4 = PE unlikely (D-dimer), score 4+ = PE likely (CTPA)
Diagnostic Algorithm
- PERC rule: If ALL 8 negative + low suspicion, PE excluded (no D-dimer)
- Low Wells (less than 4): D-dimer - if negative stop, if positive CTPA
- High Wells (4+): Skip D-dimer, go to CTPA
- CTPA gold standard (95% sensitive), VQ scan if contrast contraindicated
Risk Stratification
- Massive (High-Risk): SBP less than 90 or shock or arrest - THROMBOLYSE
- Submassive (Intermediate): Normotensive BUT RV dysfunction (echo/CT) or elevated troponin/BNP - Anticoagulate + monitor
- Low-Risk: Normotensive, no RV dysfunction - Anticoagulate, consider outpatient if PESI low
- RV dysfunction: RV/LV ratio greater than 0.9 (echo) or greater than 1.0 (CT)
Treatment - Anticoagulation
- First-line: DOACs (rivaroxaban 15mg BD x21d then 20mg OR apixaban 10mg BD x7d then 5mg BD)
- No LMWH lead-in with rivaroxaban/apixaban
- Massive PE: IV heparin initially (UFH bolus 80 units/kg, infusion 18 units/kg/h)
- Duration: Provoked (surgery) = 3 months, Unprovoked = 3-6 months minimum
Thrombolysis
- Indication: Massive PE ONLY (SBP less than 90 or shock)
- Agent: Alteplase 100mg IV over 2h (or 50mg bolus if arrest)
- Reduces mortality from 30% to 10% in massive PE
- Complications: Major bleed 10-15%, intracranial hemorrhage 1-5%
- PEITHO trial: Do NOT routinely thrombolyse submassive PE (more bleeding, no mortality benefit)
IVC Filters and VTE Prophylaxis
- IVC filter ONLY if absolute contraindication to anticoagulation (NOT routine)
- PREPIC trial: Filters reduce early PE but increase DVT, NO mortality benefit
- THA prophylaxis: Rivaroxaban 10mg daily OR enoxaparin 40mg daily for 28-35 days
- TKA prophylaxis: Rivaroxaban 10mg daily OR enoxaparin 40mg daily for 10-14 days
IVC Filters - Evidence and Indications
The PREPIC trial clearly showed IVC filters do NOT reduce PE mortality. They prevent recurrent PE in the first 2 weeks but INCREASE the risk of DVT long-term. Only use if absolute contraindication to anticoagulation.
Indications for IVC Filter
- Acute VTE with absolute contraindication to anticoagulation (active bleeding, recent intracranial hemorrhage, recent neurosurgery)
- Recurrent VTE despite therapeutic anticoagulation (documented compliance + therapeutic levels)
- Free-floating IVC or iliofemoral thrombus (no good evidence)
- Very limited cardiopulmonary reserve where any PE would be fatal (debated)
- Primary prophylaxis in high-risk patients (ortho surgery, trauma) - use chemical prophylaxis instead
- PE with contraindication to thrombolysis (can still anticoagulate)
Evidence Against Routine IVC Filters
- RCT of IVC filter + anticoagulation vs anticoagulation alone in DVT patients
- Filter group: Lower PE at 12 days (1.1% vs 4.8%)
- BUT: Increased DVT at 2 years (21% vs 12%)
- NO difference in mortality at 2 years or 8 years
Filters prevent early PE but cause more DVT. Net benefit is ZERO. Only use if cannot anticoagulate at all.
Types of IVC Filters
- Indication
- Temporary contraindication to anticoagulation
- Notes
- Should be removed within 2-4 weeks once anticoagulation starts
- Indication
- Permanent contraindication to anticoagulation
- Notes
- Rarely needed
Always use retrievable filters and set removal date. Many are left in permanently by mistake.
Evidence Base
PEITHO Trial - Thrombolysis in Intermediate-Risk PE
- Double-blind RCT of 1005 normotensive intermediate-risk PE patients (RV dysfunction PLUS positive troponin)
- Tenecteplase plus heparin vs placebo plus heparin
- Death or haemodynamic decompensation by day 7: 2.6% vs 5.6% (OR 0.44, 95% CI 0.23-0.87, P=0.02)
- BUT extracranial major bleeding 6.3% vs 1.2% (P less than 0.001) and stroke 2.4% vs 0.2% (P=0.003, mostly haemorrhagic)
- No difference in 7-day or 30-day mortality (2.4% vs 3.2% at day 30)
PREPIC Trial - IVC Filters in Proximal DVT
- RCT of 400 proximal-DVT patients at risk of PE: IVC filter plus anticoagulation vs anticoagulation alone
- Filter reduced symptomatic or asymptomatic PE at day 12 (1.1% vs 4.8%, OR 0.22, 95% CI 0.05-0.90)
- BUT increased recurrent DVT at 2 years (20.8% vs 11.6%, OR 1.87, 95% CI 1.10-3.20)
- NO significant difference in mortality at 2 years
- (NEJM 1998;338:409-15; long-term PREPIC follow-up confirmed no mortality benefit)
EINSTEIN-PE Trial - Rivaroxaban vs Enoxaparin/VKA
- Open-label noninferiority RCT of 4832 patients with acute symptomatic PE
- Single-drug rivaroxaban (15mg BD for 3 weeks then 20mg daily) vs enoxaparin followed by a vitamin K antagonist
- Noninferior for recurrent VTE (2.1% vs 1.8%, HR 1.12, 95% CI 0.75-1.68, P=0.003 for noninferiority)
- Major bleeding halved with rivaroxaban (1.1% vs 2.2%, HR 0.49, 95% CI 0.31-0.79, P=0.003)
- Effective oral therapy from day 1 without parenteral lead-in