Pediatric | O'Brien Classification | Reduction Techniques
- Less than 30° angulation = no reduction needed in children less than 10 years
- Less than 45° angulation = acceptable in children over 10 years
- Closed reduction techniques: supination and valgus, Israeli technique (thumb pressure)
- Patterson technique: percutaneous K-wire joystick reduction
- Avoid open reduction if possible - high rate of stiffness and AVN
- “Radial head does not appear until age 3-5, neck fractures more common in children
- “Posterior interosseous nerve (PIN) at risk - assess finger/thumb extension
- “Open reduction associated with higher complication rates
- “Metaizeau technique: ESIN reduction without opening
Less than 30° angulation = No reduction needed. Aim for less than 30° in young children, less than 45° in adolescents. The radial head has significant remodeling potential.
Open reduction has higher complications. Associated with stiffness, AVN, radioulnar synostosis. Try closed, then percutaneous, then intramedullary (Metaizeau) before opening.
Posterior interosseous nerve at risk. Assess finger and thumb extension before and after any intervention. Usually neurapraxia. Watch for iatrogenic injury during percutaneous methods.
Valgus force with axial load. Fall on outstretched hand with elbow extended. Associated with Monteggia variants and elbow dislocation in 10% of cases.
- Classification
- O'Brien Type I
- Management
- Non-operative - cast
- Classification
- O'Brien Type II
- Management
- Closed reduction attempted
- Classification
- O'Brien Type II-III
- Management
- Closed or percutaneous reduction
- Classification
- O'Brien Type III-IV
- Management
- Percutaneous/Metaizeau/consider open
30-45Angulation Thresholds
Hook:30 for young, 45 for old - both end in fives!
CIPOMReduction Escalation
Hook:Escalate systematically - avoid open if possible!
Overview and Epidemiology
In children, the radial head is largely cartilaginous and the neck is weaker. Force transmission causes neck fractures rather than head fractures seen in adults. The radial head ossification center appears at age 3-5 years.
- 5-10% of pediatric elbow fractures
- Peak age 9-10 years
- Equal male to female ratio
- Usually falls (playground, sports)
- Associated injuries common (50%)
- Elbow dislocation (10%)
- Olecranon fractures
- Ulna fractures (Monteggia variant)
- Medial epicondyle fractures
- Capitellum injuries
Anatomy and Biomechanics
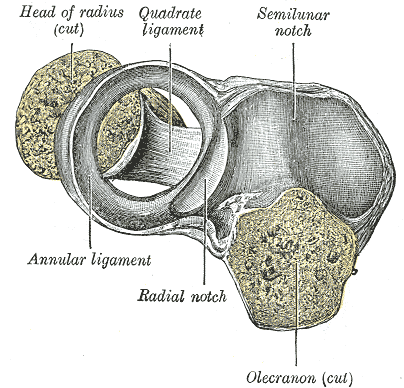
The posterior interosseous nerve (PIN) runs anteriorly around the radial neck. At risk during injury and during percutaneous/open procedures. Enters supinator at arcade of Frohse. Assess finger and thumb extension.
Radial Head Vascularity
Primarily through periosteal vessels around the neck. Intramedullary flow minimal.
Disruption of periosteal vessels during open reduction can cause AVN. Preserve soft tissues if surgery needed.
Excellent potential in children due to physis contribution to growth and robust blood supply.
Classification Systems
O'Brien Classification (By Angulation)
- Angulation
- Less than 30°
- Treatment
- Non-operative
- Angulation
- 30-60°
- Treatment
- Closed reduction
- Angulation
- Greater than 60°
- Treatment
- Percutaneous or open reduction
- Angulation
- 90° (complete displacement)
- Treatment
- Usually requires open reduction
Key point: Angulation measured from shaft axis on lateral X-ray.
Physeal Pattern and Growth Disturbance
The angulation classifications (O'Brien, Judet) describe the deformity, but the examiner also expects the physeal anatomy of the injury and what a growth disturbance would cause.
- In children the injury is usually either a physeal separation (Salter-Harris type I or, more often, type II) through the proximal radial physis, or a purely metaphyseal (subcapital) neck fracture just distal to it.
- The proximal radial physis contributes only about 20 to 25% of the radius's length (the distal radial physis does the bulk), so pure longitudinal growth loss from a proximal injury is usually modest - the remodelling that helps these fractures comes largely from the physis re-orienting the tilted head.
- Severe injury or open reduction can cause premature closure of the proximal radial physis, producing radial-head/neck deformity, relative radial shortening with positive ulnar variance, and altered radiocapitellar congruity.
- Because remodelling depends on remaining growth, the younger child remodels best - which, alongside the excision caveat below, is why a conservative head-preserving strategy is favoured.
Most paediatric radial neck fractures are a Salter-Harris I/II physeal injury or a metaphyseal neck fracture. The proximal radial physis contributes only about 20-25% of radial length, so growth-arrest shortening is usually modest, but premature closure still causes head/neck deformity and positive ulnar variance. The same physis drives the excellent remodelling that justifies accepting modest residual angulation in young children.
Clinical Assessment
- Fall on outstretched hand
- Valgus mechanism
- Lateral elbow pain
- Difficulty with rotation
- Associated dislocation
- Lateral elbow tenderness
- Swelling radiocapitellar region
- Limited pronation/supination
- PIN function (finger/thumb extension)
- Elbow stability
Test BEFORE any intervention. Ask child to extend fingers at MCPs and thumb at IP joint. Compare to other side. PIN injury presents as weak or absent extension. Usually neurapraxia with complete recovery.
50% have associated elbow injuries. Check for olecranon fracture, medial epicondyle fracture, elbow dislocation. Monteggia variant may have associated radial neck injury.
Investigations

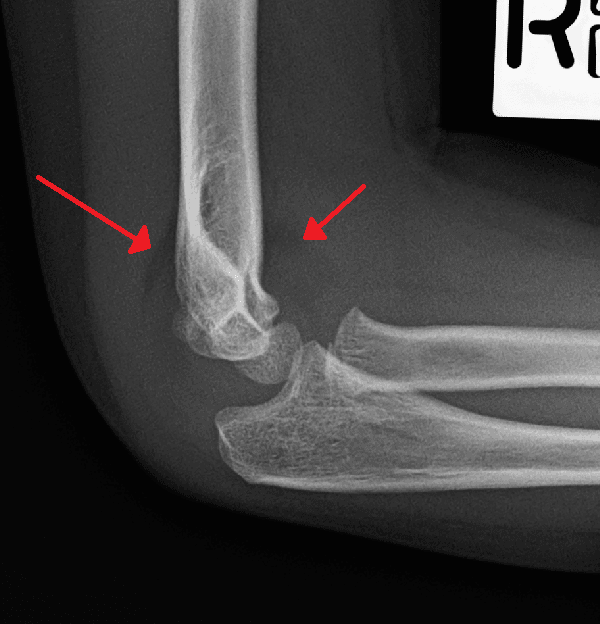
X-ray Protocol
AP and lateral elbow.
Angulation on lateral view - angle between radial shaft and head/neck line.
Check for elbow dislocation, ulna fracture, olecranon fracture.
Differential Diagnosis
The painful, swollen, rotation-restricted child's elbow has several mimics. The radiocapitellar line and the radial neck angle on a true lateral are the discriminators that separate these on plain film.
- Key clinical clue
- Lateral tenderness, painful pronation/supination
- Radiographic discriminator
- Angulation/translation of head on neck; radiocapitellar line intact through head
- Why it matters
- Remodels well; reduction only if over threshold
- Key clinical clue
- Toddler, axial traction history, arm held pronated, no swelling
- Radiographic discriminator
- Normal radiographs (often reduced by positioning for the film)
- Why it matters
- No fracture; supination-flexion manoeuvre cures it, do not over-investigate
- Key clinical clue
- Ulnar deformity or tenderness with elbow injury
- Radiographic discriminator
- Radiocapitellar line does NOT pass through capitellum; ulna bowed or fractured
- Why it matters
- Missed dislocation if you fixate on the radius; reduce the ulna first
- Key clinical clue
- Lateral tenderness, fat pad sign
- Radiographic discriminator
- Metaphyseal fragment lateral distal humerus, NOT radial neck
- Why it matters
- Intra-articular, Salter-Harris IV, often needs fixation; high non-union risk if missed
- Key clinical clue
- Mechanical block, effusion in older child
- Radiographic discriminator
- Defect or loose body at capitellum; radial head intact
- Why it matters
- Different operative plan; MRI often needed
- Key clinical clue
- Painless, chronic, often bilateral, found incidentally
- Radiographic discriminator
- Dome-shaped/hypoplastic radial head, convex articular surface, no acute fracture line
- Why it matters
- Do not attempt acute reduction of a chronic/congenital head
Always trace the radiocapitellar line on EVERY paediatric elbow film: a line through the centre of the radial neck must point at the capitellum in all views. If it does not, you are looking at a Monteggia-equivalent, not an isolated radial neck fracture. Second, a normal-looking film in a toddler with a classic traction history is a pulled elbow, not an occult fracture.
Management
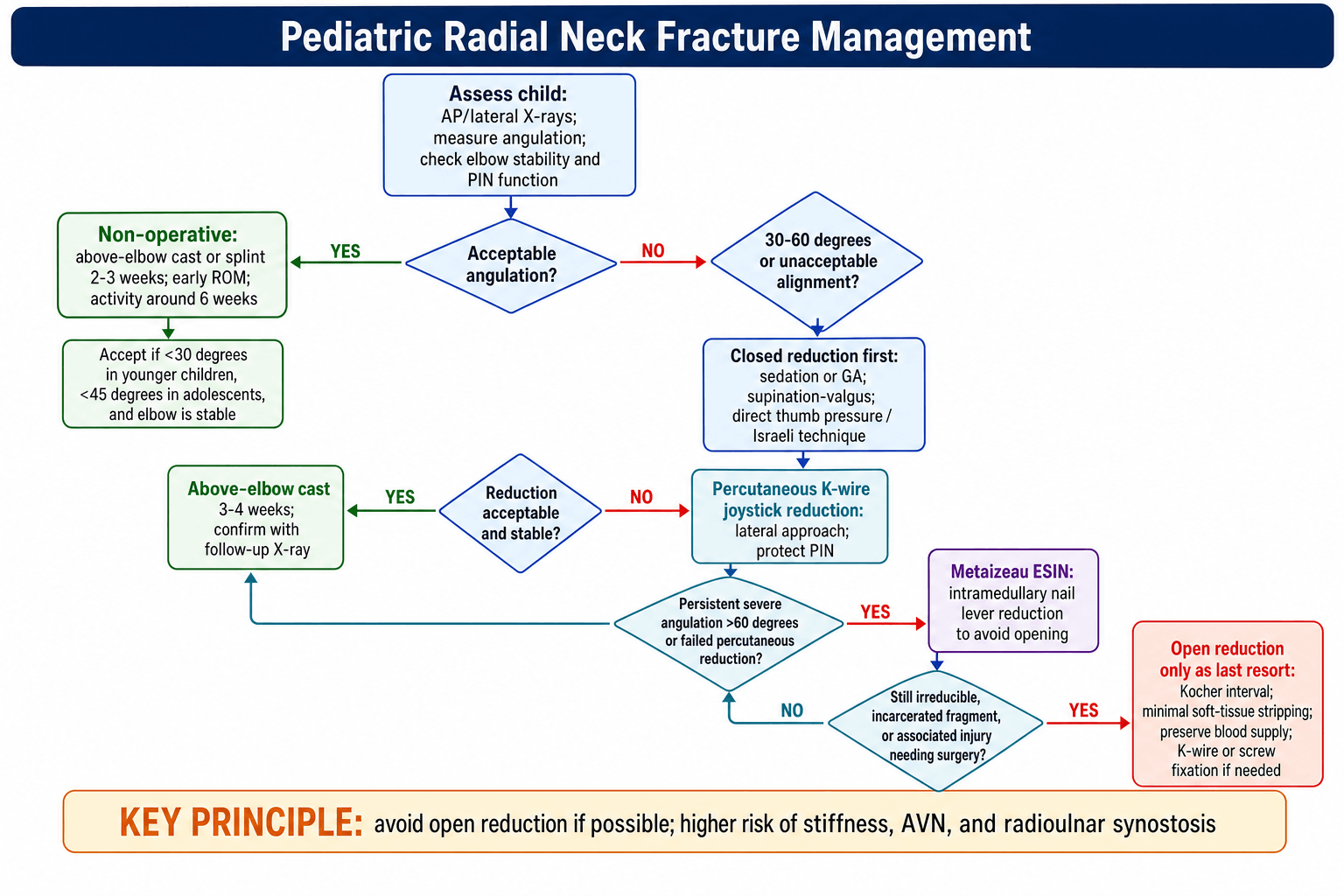
Avoid open reduction if possible. Open reduction has significantly higher rates of stiffness, AVN, and synostosis. Escalate through closed, then percutaneous, then intramedullary techniques before considering open.
Non-Operative Management
Angulation less than 30° in younger children (under 10 years). Angulation less than 45° in adolescents. Stable elbow.
Above-elbow cast or splint for 2-3 weeks. Early ROM exercises after. Full activity at 6 weeks.
Excellent. These fractures remodel well.
Escalate systematically. Closed reduction first (supination-valgus, Israeli). If failed, percutaneous K-wire (Patterson). If failed, Metaizeau ESIN. Open only as last resort due to complications.
Surgical Technique Considerations
Percutaneous K-Wire Reduction
Patient supine. Fluoroscopy. Sedation or GA.
Insert 1.5-2mm K-wire from lateral side into fracture site adjacent to tilted radial head.
Use wire as joystick. Lever angulated head back into position while applying gentle supination.
Above-elbow cast. Wire removed at 2-3 weeks.
Complications
Complications of Radial Neck Fractures
- Incidence
- 20-50%
- Management
- Usually pronation/supination. Most improve with time.
- Incidence
- 5-10%
- Management
- Usually neurapraxia. Observe. Most recover.
- Incidence
- 5-10%
- Management
- Related to open reduction. May need excision if symptomatic.
- Incidence
- Rare
- Management
- Cross-union. May need excision.
- Incidence
- Variable
- Management
- Accept some angulation. Remodeling helps.
- Incidence
- Rare
- Management
- May limit motion. Excise if mature and symptomatic.
Open reduction has 2-3x higher complication rates. Stiffness rates up to 50% with open vs 10-20% with closed. AVN and synostosis almost exclusively with open procedures. This is why escalation through closed techniques is so important.
SASAComplications of Open Reduction
Hook:SASA remember why to avoid open!
Postoperative Care
Post-Treatment Protocol
Above-elbow cast or splint. Elbow at 90°. Neutral forearm rotation. Non-weight bearing.
Remove cast. Begin active ROM - focus on pronation/supination. Avoid passive stretching.
Progressive strengthening. Return to light activities. Avoid contact sports.
Full return to sports. Monitor for late stiffness. Some ROM loss may persist but often not functional.
Outcomes and Prognosis
Prognosis by Treatment
Excellent prognosis. Full ROM expected. Complete remodeling.
Good outcomes. Some minor ROM loss common but rarely functional.
Intermediate outcomes. Better than open reduction.
Higher complication rates. Significant stiffness in up to 50%. AVN risk.
Guidelines, Registries & Global Practice
Across AAOS, BOA/BSCOS (UK), AO Foundation and EFORT/European paediatric practice, the philosophy is identical and evidence-consistent: accept and remodel modest angulation, reduce closed when over threshold, escalate to intramedullary (Métaizeau/ESIN) for severe displacement, and treat open reduction as a last resort. There is no formal single-society guideline document specific to this fracture, so practice rests on the technique and outcome literature rather than a named protocol.
- Acceptable angulation
- ~30° young, up to ~45° adolescent
- Preferred operative escalation
- Closed → percutaneous joystick → ESIN; open last
- Emphasis
- Remodelling potential, avoid arthrotomy stiffness
- Acceptable angulation
- Conservative bias for moderate angulation
- Preferred operative escalation
- ESIN (Métaizeau) for severe displacement
- Emphasis
- Minimally invasive, day-case where possible
- Acceptable angulation
- Threshold ~30-45° by age
- Preferred operative escalation
- Intramedullary reduction/stabilisation favoured
- Emphasis
- Soft-tissue and vascular preservation
- Acceptable angulation
- Up to ~50° may remodel in young
- Preferred operative escalation
- Métaizeau ESIN as standard for displaced
- Emphasis
- Originator-driven technique adoption
- Roughly 5-10% of paediatric elbow fractures and about 1% of all paediatric fractures
- Peak age 9-10 years; near-equal sex distribution
- Mechanism is consistent worldwide: fall on an outstretched hand with a valgus, axially loaded extended elbow
- Associated injuries in up to ~50% (elbow dislocation ~10%, olecranon, medial epicondyle, ulna)
- No dedicated arthroplasty/implant registry captures this paediatric fracture (registries focus on adult joint replacement)
- Evidence base is retrospective series plus one systematic review/meta-analysis, not registry or trial data
- This evidence gap is itself an exam discussion point: management is consensus- and technique-driven
- Image intensifier and elastic nails readily available, enabling closed Métaizeau/ESIN as the default for severe displacement
- Paediatric anaesthesia and day-surgery pathways support early closed intervention
- Ready access to nerve conduction studies for non-recovering PIN palsy
- Without fluoroscopy or elastic nails, more reliance on closed manipulation and casting, with open reduction used earlier when closed fails
- Strong remodelling potential makes a conservative-first strategy both pragmatic and evidence-supported where implants are scarce
- Threshold for acceptance of residual angulation may be pushed higher when surgical capacity is limited
Special Considerations
Radial Neck with Elbow Dislocation
10% of radial neck fractures associated with dislocation.
Reduce dislocation first. Assess radial head position after.
May need fixation if radial head unstable after dislocation reduced.
Radial Head Excision: Contraindicated in Children
A high-yield distinction from adult practice: in the skeletally immature child, excising the radial head is contraindicated (or a true last resort), whereas in adults it is an accepted option for an unreconstructable head. Preserve the radial head in children whenever possible.
Why excision harms the growing elbow:
- Mechanism
- Loss of the radiocapitellar buttress lets the radius migrate proximally
- Mechanism
- Valgus drift of the elbow stretches the ulnar nerve over time
- Mechanism
- Relative radial shortening makes the ulna ride long at the wrist and overload the DRUJ
- Mechanism
- The radial head normally stabilises the PRUJ, so excision destabilises the whole forearm unit
If the head is genuinely unreconstructable (severe avascular necrosis or fragmentation), delay any excision until skeletal maturity if at all possible.
Radial head excision is an adult option, NOT a paediatric one. In the growing child it causes proximal radial migration, cubitus valgus (with tardy ulnar palsy), positive ulnar variance with wrist pain, and radioulnar instability - so preserve the head, and if excision is truly unavoidable, defer it to skeletal maturity. This is a classic adult-versus-child examiner discriminator.
Controversies and Areas of Uncertainty
The classic teaching of 30° (young) / 45° (older) is a convention, not trial-derived. Vocke and Von Laer documented spontaneous correction of angulation up to 50° in conservatively treated children, prompting some surgeons to accept higher residual angulation in patients with substantial remodelling potential. There is no consensus threshold and no randomised data to anchor it.
Most thresholds quote angulation, but translation (the Judet axis) may matter as much. A markedly translated but only moderately angulated head can still impede rotation. Decisions should integrate both, plus the child's age and remaining growth.
With ESIN/Métaizeau there is no agreement on retention time. Leaving the nail stabilises the epiphysis against secondary displacement, but adds a second anaesthetic for removal and a small risk of nail-end skin irritation. Practice ranges from a few weeks to several months.
Post-intervention nerve palsy rates (up to ~15% in operative series) blur injury-related and treatment-related causes. Whether percutaneous joystick or lateral elastic nailing genuinely raises iatrogenic PIN risk over the injury itself is unresolved, which is why baseline neurological documentation is mandatory.
MCQ Practice Points
Q: What angulation threshold is acceptable for non-operative management in a 7-year-old? A: Less than 30°. Younger children have greater remodeling potential. Older children (over 10) = 45° threshold.
Q: Which nerve is at risk in radial neck fractures? A: Posterior interosseous nerve (PIN). Motor branch of radial nerve. Test finger and thumb extension.
Q: What technique uses a K-wire as a joystick for radial neck reduction? A: Patterson technique. Percutaneous K-wire inserted adjacent to radial head, used to lever head into position.
Q: Why should open reduction be avoided in radial neck fractures? A: Higher complication rates. Stiffness (up to 50%), AVN, and radioulnar synostosis all more common with open reduction.
Q: What is O'Brien Type III radial neck fracture? A: Greater than 60° angulation. Usually requires percutaneous or open reduction.
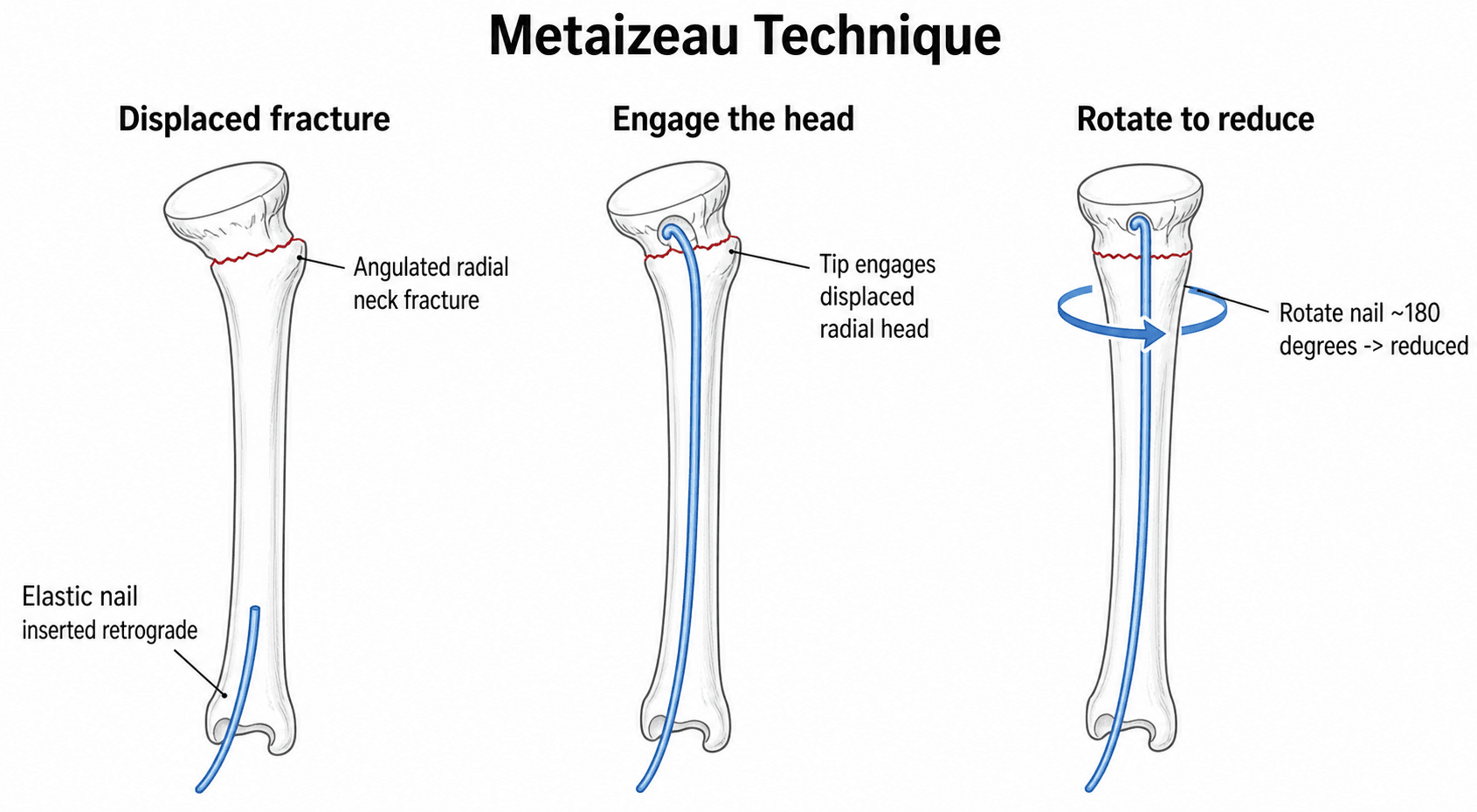
Q: What is the Metaizeau technique? A: ESIN reduction. Flexible nail inserted through distal radius, used to lever radial head from below without opening.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 9-year-old girl falls on an outstretched hand. X-ray shows a radial neck fracture with 40° angulation. Finger and thumb extension are normal. How would you manage this?”
“An 8-year-old boy has a radial neck fracture with 70° angulation and moderate translation. Closed reduction under sedation failed to improve angulation beyond 50°. What are your next steps?”
“You perform closed reduction of a radial neck fracture. Post-reduction, the child cannot extend their fingers at the MCPs or their thumb at the IP joint. What is your assessment and management?”
Angulation Thresholds
- Less than 30° = non-operative (under 10 years)
- Less than 45° = non-operative (over 10 years)
- Greater than 30-45° = reduction indicated
- Greater than 60° = percutaneous or ESIN/open
O'Brien Classification
- Type I: less than 30° (non-operative)
- Type II: 30-60° (closed reduction)
- Type III: greater than 60° (perc/open)
- Type IV: 90°/complete (usually open)
Reduction Escalation
- Closed first (Patterson supination-valgus)
- Then percutaneous K-wire joystick
- Then Metaizeau ESIN
- Open reduction LAST resort
Avoid Open Because
- Stiffness up to 50%
- AVN of radial head
- Radioulnar synostosis
- Higher overall complication rate
PIN Injury
- 5-10% incidence
- Test finger/thumb extension
- Usually neurapraxia
- Recovery expected 3-6 months
Evidence Base and Key Studies
There are no randomised controlled trials in paediatric radial neck fractures. The literature is built on retrospective series, a systematic review/meta-analysis, and the original technique-describing papers. The consistent signal across all of them: closed/intramedullary reduction outperforms open reduction, and open surgery is the strongest independent predictor of a poor functional result. O'Brien (1965) and Judet (1962) are the classic classification papers and predate PubMed indexing — they are cited here as historical primary sources without a PMID.
Conservative Treatment: Long-Term Results and Remodeling
- 38 children with displaced radial neck fractures reviewed 2-20 years after injury
- Radial head deformity present in 83%, but functional disorder in only 11% (4 children)
- All conservatively treated fractures with angulation up to 50° corrected spontaneously
- Functional problems clustered in children treated with open reduction or with secondary growth disturbance (one radioulnar synostosis)
Centromedullary (ESIN/Metaizeau) Pinning — Technique by the Originator
- Describes the leverage/derotation manoeuvre using a single retrograde elastic nail to reduce and stabilise the displaced epiphysis
- Achieves complete reduction without opening the radiocapitellar joint
- The nail is left in situ to stabilise the epiphysis and prevent secondary displacement
- Reported very low complication rate vs open reduction (AVN, intra-articular calcification, stiffness)