The Great Extensor Nerve of the Upper Limb
- Originates from Posterior Cord (C5-T1)
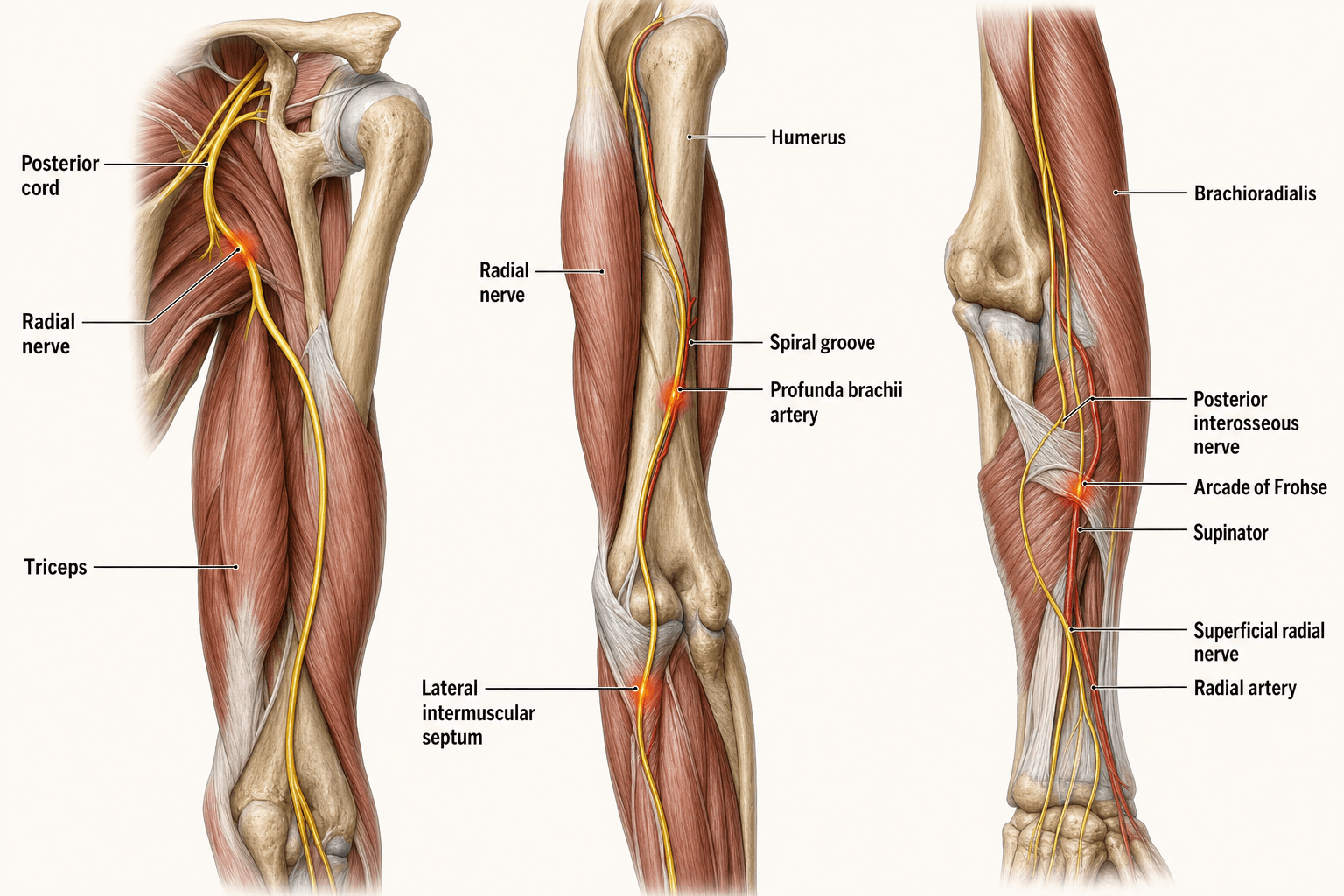
- Passes through Triangular Interval to enter Spiral Groove
- Pierces Lateral Intermuscular Septum 10cm proximal to lateral epicondyle
- Divides into Superficial (Sensory) and Deep (PIN) at lateral epicondyle
- PIN enters Supinator via Arcade of Frohse
- “Triceps is usually SPARED in humeral shaft fractures (innervation is proximal)
- “ECRL is innervated by Radial Nerve proper (before division)
- “ECRB is often innervated by Radial Nerve proper or PIN
- “Mobile Wad = BR, ECRL, ECRB
10cm Rule: The nerve pierces the lateral intermuscular septum approximately 10cm proximal to the lateral epicondyle. This is the danger zone in lateral approaches to the humerus.
Distal Third Spiral Fracture: High risk of radial nerve entrapment or injury as the nerve is tethered by the septum at this level.
Differentiating Lesions: High lesions (Axilla) affect Triceps. Mid-shaft lesions (Spiral Groove) SPARE Triceps. This distinguishes Crutch Palsy from Saturday Night Palsy.
Tenodesis Effect: Do not be fooled by 'extension' caused by wrist flexion. Isolate the MCP joints to test EDC.
- Key Detail
- Posterior Cord (C5-T1)
- Clinical Significance
- Shoulder dislocation can injure it
- Key Detail
- Spiral Groove of Humerus
- Clinical Significance
- Vulnerable in shaft fractures (10-15%)
- Key Detail
- ALL Extensors of Arm/Forearm
- Clinical Significance
- Loss = Wrist Drop
- Key Detail
- Dorsal Hand (Webspace 1)
- Clinical Significance
- Autonomous zone for testing
- Key Detail
- Anterior to Lateral Epicondyle
- Clinical Significance
- Splits into SRN (Sensory) + PIN (Motor)
BESTBranches in the Arm
Hook:The Radial nerve is the BEST nerve for extension.
PL PSensory Branches (Proximal to Distal)
Hook:People Love Pasta (3 branches before the hand).
Overview and Function
The Radial Nerve is the nerve of extension. It extends the elbow, wrist, and fingers. It also supinates the forearm (when elbow is extended). Loss of function results in the classic "Wrist Drop".
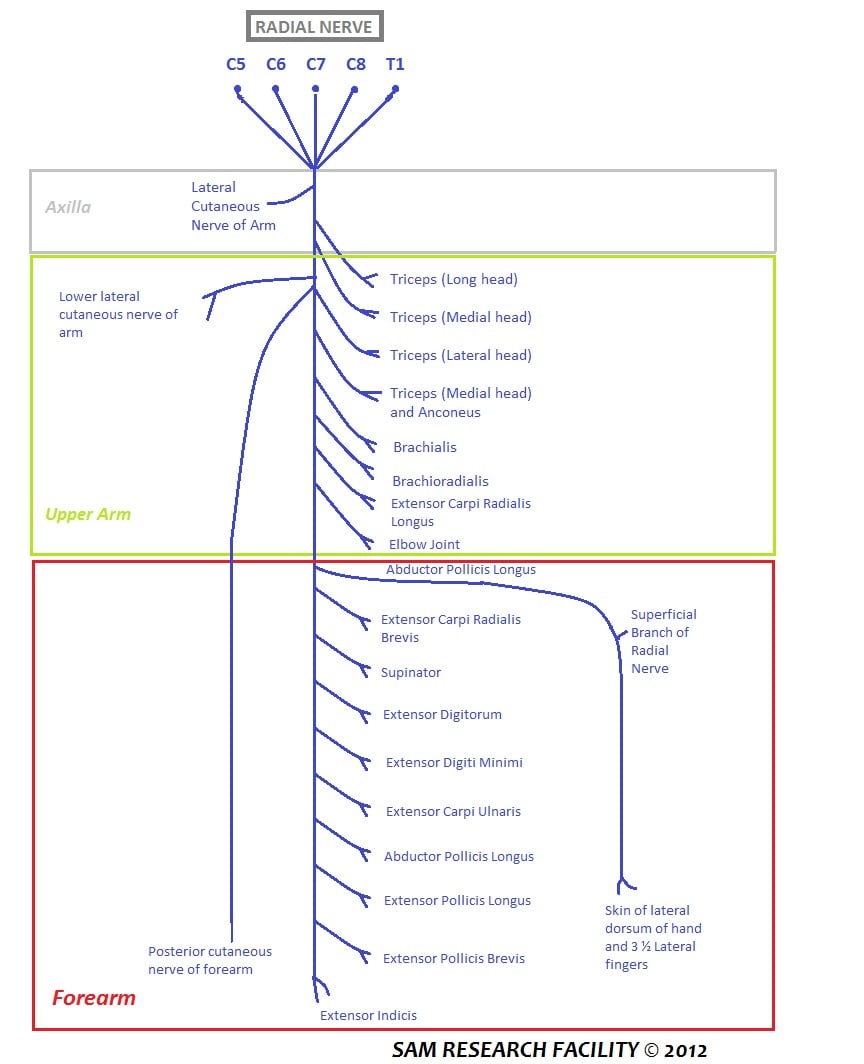
Motor Innervation Summary
- Arm: Triceps (Long, Lateral, Medial heads), Anconeus.
- Lateral Epicondyle: Brachioradialis, ECRL, ECRB (variable).
- Forearm (PIN): Supinator, EDC, EDM, ECU, APL, EPB, EPL, EIP.
These muscle groups represent the ordered motor recovery.
Neurovascular
Origin and Proximal Course
- Continuation of the Posterior Cord of the Brachial Plexus.
- Roots: C5, C6, C7, C8, (T1).
- Lies posterior to the axillary artery.
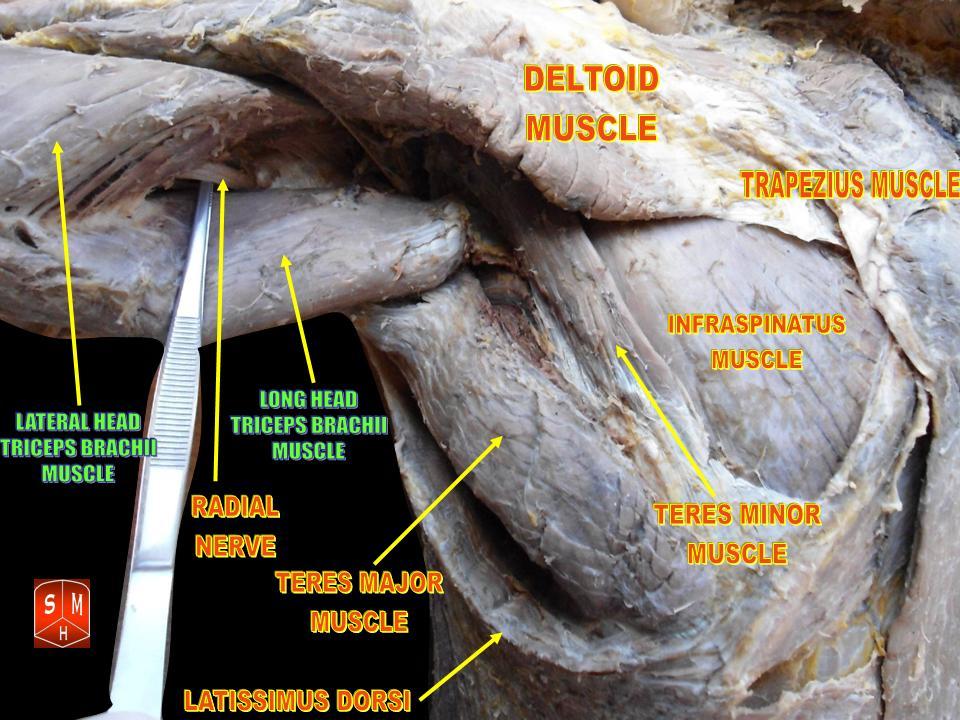
- The nerve exits the axilla entering the posterior compartment through the Triangular Interval.
- Boundaries: Teres Major (superior), Long Head Triceps (medial), Humerus (lateral).
- Contents: Radial Nerve + Profunda Brachii Artery.
- Winds around the humerus in the spiral groove (musculospiral groove) between lateral and medial heads of triceps.
- Passes medial to lateral.
- Innervates: Triceps (Lateral and Medial heads), Anconeus.
The spiral groove is the classic site for "Saturday Night Palsy".
BRECOrder of Innervation (Mobile Wad)
Hook:Break-fast is the first meal (Brachioradialis first).
The Three Posterior Spaces
Examiners pair the triangular interval (which transmits the radial nerve) with its two neighbours - know all three and their contents.
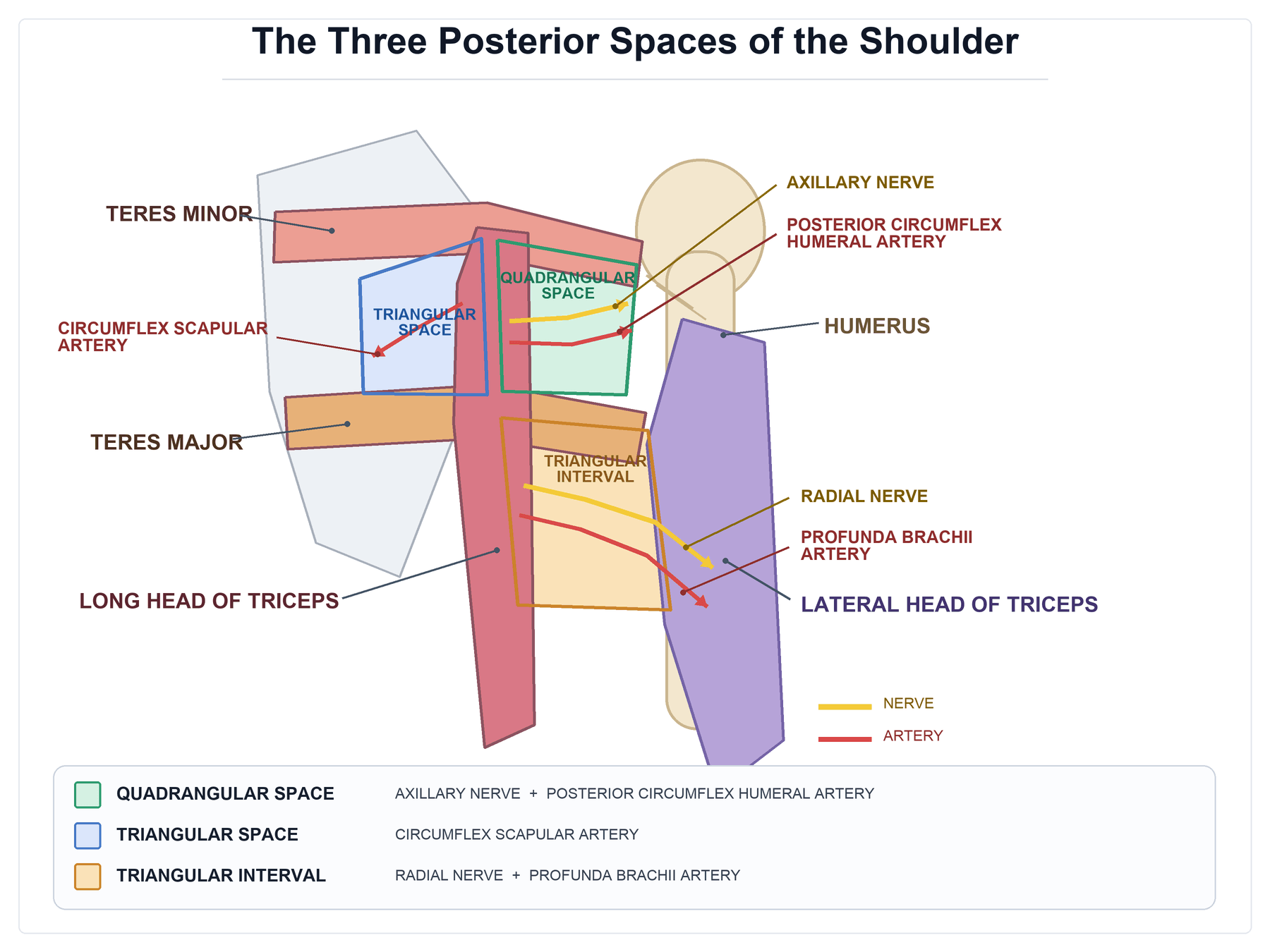
- Boundaries
- Teres minor (above), teres major (below), long head of triceps (medial), surgical neck of humerus (lateral)
- Contents
- AXILLARY nerve + posterior circumflex humeral artery
- Boundaries
- Teres minor (above), teres major (below), long head of triceps (lateral)
- Contents
- Circumflex scapular artery (branch of the subscapular artery)
- Boundaries
- Teres major (above), long head of triceps (medial), shaft/lateral head of humerus (lateral)
- Contents
- RADIAL nerve + profunda brachii (deep brachial) artery
The radial nerve travels with the profunda brachii through the triangular interval (the lowest of the three, bounded above by teres major). Do not confuse it with the quadrangular space, which transmits the axillary nerve and posterior circumflex humeral artery (at risk in shoulder dislocation and proximal humerus fracture). The triangular space between them carries only the circumflex scapular vessels - no nerve.
Classification Systems
Injury Levels & Patterns
- Motor Loss
- Triceps, Wrist Ext, Finger Ext
- Sensory Loss
- Post Arm, Forearm, Dorsal Hand
- Eponym
- Crutch Palsy / Saturday Night (High)
- Motor Loss
- Wrist Ext (Weak), Finger Ext
- Sensory Loss
- Post Forearm, Dorsal Hand (Triceps Sparing)
- Eponym
- Saturday Night Palsy / Humeral #
- Motor Loss
- Finger Ext, Thumb Ext (ECRL preserved → radial deviation)
- Sensory Loss
- None (PIN is motor)
- Eponym
- PIN Syndrome
- Motor Loss
- None
- Sensory Loss
- Dorsal Webspace
- Eponym
- Wartenberg Syndrome
Clinical Assessment
- Triceps: Extend elbow against resistance (abduct shoulder to eliminate gravity).
- Brachioradialis: Flex elbow in neutral rotation.
- ECRL/B: Extend wrist (check for radial deviation).
- EDC: Extend MCP joints (block wrist extension).
- EPL: Retropulsion of thumb (lift thumb off table palm down).
- Autonomous Zone: First dorsal webspace.
- Any loss proximal suggests higher lesion.
Patients with radial nerve palsy can appear to extend the wrist using finger flexion (tenodesis effect). Always isolate the joint being tested.
Investigations
Radiological Assessment
- Plain X-rays: Humeral shaft fracture (Holstein-Lewis), Radial head fracture/dislocation.
- Ultrasound: Can visualize nerve continuity in Holstein-Lewis fractures (nerve entrapped in callus?).
- MRI: For soft tissue masses (lipoma, ganglion) compressing PIN.
Reliable imaging confirms the diagnosis.
Differential Diagnosis of Wrist/Finger Drop
A "wrist drop" is not always a radial nerve lesion, and not every radial nerve lesion is at the same level. Localising the lesion is the high-yield exam skill.
- Triceps
- Weak/absent
- Wrist Extension
- Absent (true wrist drop)
- Finger (MCP) Extension
- Absent
- Sensory Loss
- Dorsal forearm + 1st webspace
- Discriminator
- Triceps involved = lesion above spiral groove
- Triceps
- Spared
- Wrist Extension
- Weak/absent
- Finger (MCP) Extension
- Absent
- Sensory Loss
- Dorsal forearm + 1st webspace
- Discriminator
- Triceps spared, sensory loss present
- Triceps
- Spared
- Wrist Extension
- Present (radial deviation)
- Finger (MCP) Extension
- Absent (finger drop)
- Sensory Loss
- None
- Discriminator
- No sensory loss, ECRL preserved
- Triceps
- Spared
- Wrist Extension
- Present
- Finger (MCP) Extension
- Present
- Sensory Loss
- None
- Discriminator
- Pain only, no motor deficit
- Triceps
- Weak
- Wrist Extension
- Weak
- Finger (MCP) Extension
- Weak
- Sensory Loss
- Dermatomal (middle finger)
- Discriminator
- Neck pain, reflex changes, multi-nerve pattern
- Triceps
- Variable
- Wrist Extension
- Weak
- Finger (MCP) Extension
- Weak
- Sensory Loss
- Cortical pattern
- Discriminator
- Increased tone, brisk reflexes, no autonomous-zone map
- Triceps
- Variable
- Wrist Extension
- Weak (often bilateral)
- Finger (MCP) Extension
- Weak
- Sensory Loss
- Variable
- Discriminator
- Systemic features, often bilateral / multifocal
Answer three questions in order: (1) Is the triceps working? (above vs below spiral groove). (2) Is there sensory loss? (radial nerve proper/SRN vs pure PIN). (3) Does the wrist extend with radial deviation? (ECRL preserved = PIN lesion).
Management of Palsy
Treatment Algorithm
Management Algorithm for Humeral Shaft Palsy
Closed injury? Open? Check nerve function. Most are neurapraxia (85-90% recovery).
If no clinical recovery. Look for fibrillation potentials (denervation).
If no recovery by 3-4 months (and no advancing Tinel's), consider exploration + nerve graft OR tendon transfers.
Jones transfer (PT to ECRB, FCU to EDC, PL to EPL).
The classic Jones Transfer for radial nerve palsy:
- Pronator Teres → ECRB (Restore Wrist Ext)
- FCU (or FCR) → EDC (Restore Finger Ext)
- Palmaris Longus → EPL (Restore Thumb Ext)
Surgical Approaches
Posterior Approach to Humerus
Distal 1/3 fractures, Exploration of Radial Nerve.
- Midline posterior incision.
- Identify interval between Long and Lateral heads of Triceps (proximal).
- Or split Triceps midline (distal).
- Identify Nerve: In spiral groove with Profunda Brachii artery.
- Trace distally through lateral intermuscular septum.
Careful dissection preserves the nerve.
Complications
- Cause
- Injury to SRN
- Prevention
- Protect Wartenberg's point
- Management
- Bury nerve end
- Cause
- Plate fixation (humerus/radius)
- Prevention
- Identify and protect
- Management
- Explore/Repair
- Cause
- Neurotmesis
- Prevention
- Early exploration if open
- Management
- Tendon transfers
- Cause
- Dynamic compression
- Prevention
- Release arcade
- Management
- Decompression
Recovery and Rehab
Dynamic Splinting: Use a dynamic extension splint (outrigger) to prevent flexor contractures and assist function while waiting for nerve recovery.
Maintain passive ROM of all joints. Prevent stiffness. Strengthen substitute muscles.
Outcomes and Prognosis
- Humeral Shaft Compressive Palsy: 90% spontaneous recovery.
- Holstein-Lewis: High rate of recovery, but some advocate early exploration if caused by spiral distal fracture (nerve may be encased).
- Post-operative Palsy: If nerve was seen intact, observation. If nerve integrity unknown, consider exploration.
Guidelines, Registries & Global Practice
Global Epidemiology
- Humeral shaft fractures: incidence approximately 14.5 per 100,000 per year in a European population, rising to nearly 60 per 100,000 per year in the ninth decade, with a bimodal pattern (young men, high energy; older women, low-energy falls) (Ekholm 2006).
- Radial nerve palsy complicates roughly 8-12% of humeral shaft fractures overall, highest in middle/distal-third transverse and spiral patterns (Shao 2005; Ekholm 2006).
- Holstein-Lewis (distal-third spiral) fractures account for around 7.5% of shaft fractures but carry approximately 22% palsy risk (Ekholm 2008).
- Spontaneous recovery of closed traumatic palsy is around 71% with observation and approximately 88% overall including those explored (Shao 2005).
Side-by-Side Guidance
- Position on closed radial nerve palsy
- Observation first-line; surgery for low-recovery scenarios or patient preference
- Emphasis
- Decision-analysis and systematic-review driven (Bishop & Ring; Shao)
- Position on closed radial nerve palsy
- Expectant management for closed palsy; document neurovascular status, image to plan
- Emphasis
- Early neurovascular documentation, structured follow-up
- Position on closed radial nerve palsy
- Inspect/protect the nerve during any planned humeral fixation; explore in open injuries
- Emphasis
- Surgical technique, iatrogenic-injury avoidance, fixation planning
- Position on closed radial nerve palsy
- Aligns with conservative-first approach; ultrasound increasingly used to triage
- Emphasis
- Imaging-led triage, nerve continuity assessment
Ready access to high-resolution ultrasound and electrodiagnostics allows early triage of nerve continuity, MRI for compressive masses around the PIN, and microsurgical repair/grafting or tendon transfer when recovery fails.
Where nerve imaging and electrophysiology are scarce, management leans on serial clinical examination (advancing Tinel's sign), dynamic extension splinting to prevent contracture, and tendon transfers - which are reliable, equipment-light and durable.
Radial nerve injury during humeral or radial plating is a recognised complication worldwide - document pre-operative nerve status, identify and protect the nerve, and beware the segment 10cm proximal to the lateral epicondyle. The nerve is also vulnerable to prolonged tourniquet or arm-board pressure (Saturday-night-type compression).
Special Topics and Variants
Wartenberg's Syndrome
Compression of Superficial Radial Nerve (SRN).
- Site: Between Brachioradialis and ECRL tendons during pronation (scissoring effect).
- Symptoms: Pain/Paresthesia in dorsal thumb/webspace. +ve Tinel's.
- DDx: De Quervain's (Finkelstein test distinguishes).
Surgical release is rarely needed but effective.
The Five Compression Sites of the Radial Tunnel
The radial tunnel runs from the radiocapitellar joint to the distal edge of supinator, and the PIN can be compressed at five classic points along it - a favourite enumeration in vivas.
- Fibrous bands at the front of the radiocapitellar joint (tethering the nerve to the capsule).
- The leash of Henry - the radial recurrent vessels crossing the nerve.
- The medial (tendinous) edge of ECRB.
- The arcade of Frohse - the thickened proximal edge of the superficial head of supinator (the commonest site).
- The distal edge of the supinator.
These five sites are shared by radial tunnel syndrome (a PAIN syndrome with no motor deficit) and PIN syndrome (a motor palsy - finger drop with radially-deviated wrist extension). The arcade of Frohse is the commonest culprit in both. When decompressing, remember that no single surgical window exposes all five sites, so the approach is matched to the suspected level and complete release may need more than one window.
Controversies & Areas of Uncertainty
The dominant evidence (Shao 2005; Bishop & Ring 2009) supports observation for closed palsy, with around 71% spontaneous recovery and decision-analysis favouring waiting. Debate persists for high-energy mechanisms and for palsy that develops after fracture manipulation (secondary palsy), where some argue the threshold for exploration should be lower.
Many authors recommend nerve inspection at the time of open-fracture debridement/fixation, since a lacerated or interposed nerve is more likely. Others argue a clean low-energy open wound does not in itself mandate routine exploration. No high-level trial settles this.
The diagnosis remains contentious: it is a pain syndrome with no objective motor or sensory deficit and no reliable electrodiagnostic confirmation. Overlap with lateral epicondylitis and inconsistent surgical results fuel scepticism. Decompression outcomes are variable.
Baseline EMG/NCS immediately after injury is of limited value because Wallerian changes take roughly 3-4 weeks to appear. The optimal first study timing (and whether ultrasound should pre-empt it) is debated, with imaging increasingly used to triage early.
MCQ Practice Points
Q: What is the primary root value of the Radial Nerve? A: C5-T1. It is the largest branch of the brachial plexus and receives fibers from all roots (continuation of posterior cord).
Q: Where does the radial nerve pierce the lateral intermuscular septum? A: 10cm proximal to the lateral epicondyle. This is a critical landmark for the anterolateral approach.
Q: Which muscle is used to restore wrist extension in a radial nerve palsy? A: Pronator Teres. It is transferred to the ECRB tendon (PT → ECRB).
Q: What anatomical structure forms the Arcade of Frohse? A: The proximal fibrotendinous edge of the Supinator muscle.
Q: Which three muscles make up the Mobile Wad of Henry? A: Brachioradialis, ECRL, and ECRB.
Anatomy Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A patient presents with a mid-shaft humeral fracture and a wrist drop. Describe the anatomy of the radial nerve relevant to this injury.”
“Describe the course of the Posterior Interosseous Nerve and the potential sites of compression.”
“A patient has paresthesia over the dorsal thumb and index finger. Differentiate Wartenberg's Syndrome from De Quervain's Tenosynovitis.”
Key Anatomy
- Posterior Cord (C5-T1)
- Triangular Interval (with Profunda Brachii)
- Lateral Intermuscular Septum (pierces 10cm proximal to elbow)
- Arcade of Frohse (Supinator edge) - PIN compression site
- Wartenberg's Point (Distal radius) - SRN emergence
- Lister's Tubercle - EPL turns around it (supplied by PIN)
Branches (Motor)
- Axilla: Long/Medial Triceps
- Spiral Groove: Lateral/Medial Triceps, Anconeus
- Elbow: Brachioradialis, ECRL, ECRB
- PIN: Supinator, EDC, EDM, ECU, APL, EPB, EPL, EIP
Clinical Signs
- Wrist Drop (High lesion)
- Finger Drop + Radial Deviation (PIN lesion)
- Triceps Sparing (Spiral Groove lesion)
- First Dorsal Webspace Numbness (Radial Nerve proper/SRN)
- Tinel's at Wartenberg's point (Wartenberg Syndrome)
Surgical Pearls
- Find nerve in interval between Brachialis and Brachioradialis (Anterior)
- Ligate 'Leash of Henry' (Radial Recurrent vessels)
- Supinate forearm to move PIN away from incision (Henry approach)
- Beware nerve 10cm proximal to lateral epicondyle in lateral plating
Evidence Base
Radial Nerve Palsy in Humeral Shaft Fractures - Landmark Systematic Review
- 35 studies, 1045 patients with radial nerve palsy after humeral shaft fracture
- Overall prevalence of palsy 11.8% (532 palsies in 4517 fractures)
- Overall recovery 88.1%; spontaneous recovery 70.7% in conservatively treated patients
- No significant difference in final result between expectant management and early exploration
- Middle and middle-distal shaft, transverse and spiral patterns carried highest risk
The Holstein-Lewis Fracture and Radial Nerve Risk
- Holstein-Lewis fractures were 7.5% of all humeral shaft fractures (27 of 361)
- Associated with significantly higher acute radial nerve palsy than other patterns: 22% vs 8% (statistically significant)
- All 6 radial nerve palsies recovered regardless of operative or non-operative treatment
- Functional outcome (SMFA) good and similar between treatment groups
Ultrasound Evaluation of the Radial Nerve in Humeral Fractures
- Prospective study of 11 patients with sensorimotor radial deficit after humeral fracture
- In all 5 operated patients, US findings of a severely damaged nerve were confirmed at surgery (entrapment, dissection, laceration, riding on a fragment, buried in callus)
- In the 6 patients treated conservatively, US demonstrated nerve continuity
- US can distinguish a nerve in continuity from an interrupted or entrapped nerve
Observation vs Early Surgery - Decision Analysis
- Expected-value decision analysis using literature-derived probabilities and patient utilities (82 subjects)
- Observation (value 8.4) outperformed early surgery (value 6.7) as the optimal strategy
- Early surgery becomes preferred only if expected spontaneous recovery falls below 40%
- Early surgery also favoured when an informed patient places very high utility on a successful early result
Fingerbreadth Safe-Zone Rule for the Radial Nerve and PIN
- Anatomic study of 10 fresh-frozen cadaveric elbows
- Four fingerbreadths defines a safe zone between the lateral epicondyle and the radial nerve proximally
- Two fingerbreadths defines a safe zone for the PIN from the radiocapitellar joint - only with the forearm pronated
- Radial head diameter and capitellar width correlated with PIN distance
Surgical Approaches to the Radial Tunnel - Anatomic Comparison
- 30 fresh-frozen cadaveric specimens, 10 each of anterior, anterolateral and posterior approaches
- Anterior and anterolateral approaches best visualised the radial head bands, leash of Henry, ECRB origin and arcade of Frohse
- The posterior approach best exposed the distal border of supinator
- No single approach adequately visualised all five compression sites
Tendon Transfers for Irrecoverable Radial Nerve Palsy
- Pronator teres to ECRB restores wrist extension
- FCU (or FCR) to EDC restores finger MCP extension
- Palmaris longus to EPL restores independent thumb extension
- FCR-based (Boyes) variants preserve wrist flexion-extension balance