DDH, SUFE, Perthes & Growth Plate Assessment
DDH: Hilgenreiner + Perkins lines, acetabular index, Shenton line, Graf USS
SUFE: Klein line, frog lateral (best view), Southwick angle
Perthes: Catterall classification, Herring lateral pillar, Gage sign, head-at-risk
Growth plate: Salter-Harris I-V (SALTR mnemonic)
NAI: Metaphyseal corner fractures, multiple fractures of different ages
Key: The Klein line for SUFE and Perkins/Hilgenreiner for DDH are the most tested paediatric signs
- Klein line: a line drawn along the superior femoral neck on AP radiograph should intersect the lateral epiphysis. Failure = SUFE.
- DDH assessment: Perkins line (vertical from lateral acetabular edge) and Hilgenreiner line (horizontal through triradiate cartilage) create four quadrants — femoral head should be in the inferomedial quadrant.
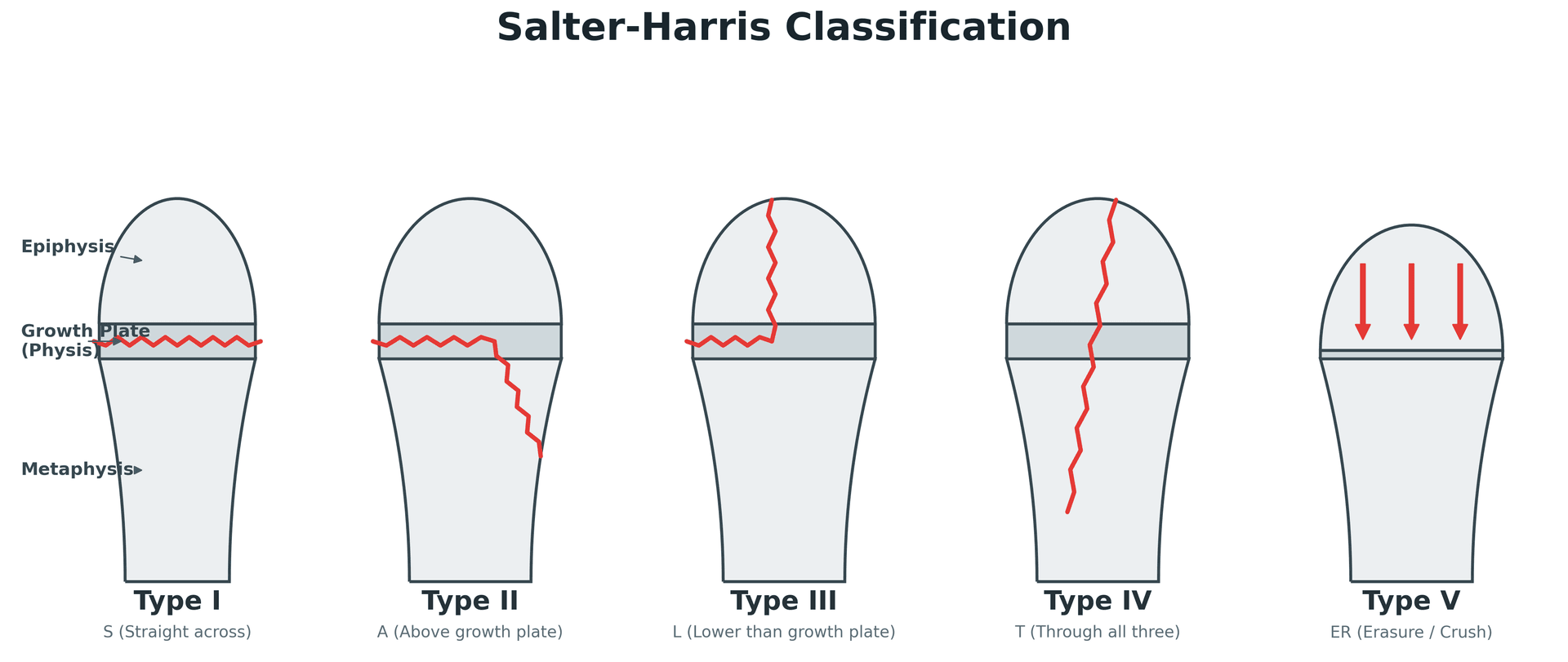
- Salter-Harris classification (SALTR): Slip (I), Above (II), Lower (III), Through (IV), Rammed (V) — describes growth plate fracture pattern.
- Perthes disease staging: Catterall classification (4 groups by extent of head involvement) and Herring lateral pillar classification (A, B, C by lateral pillar height preservation).
- Ultrasound is the primary imaging modality for DDH screening before 6 months (Graf classification). AP pelvis radiograph after 6 months.
- “The Klein line is the single most important radiographic sign for SUFE — always check it on AP views of skeletally immature patients with hip or knee pain.
- “SUFE can present as knee pain (referred via the obturator nerve) — always examine and image the hip when a child presents with knee pain.
- “Perthes: the Herring lateral pillar classification is the best prognostic indicator. Group A (full height) = good prognosis. Group C (less than 50% height) = poor prognosis.
- “Salter-Harris Type II is the MOST COMMON growth plate fracture (commonly quoted as ~75%; 54% in the population-based Olmsted County series). Type V may be radiographically occult — diagnosed retrospectively by growth arrest.
- “The metaphyseal corner fracture (bucket-handle) in an infant is highly specific for non-accidental injury (NAI).
Paediatric radiological signs are among the most frequently tested topics. You must be able to: draw and interpret the Klein line (SUFE), construct Perkins and Hilgenreiner lines for DDH assessment, classify growth plate injuries using Salter-Harris, stage Perthes disease, and recognise the radiographic features of non-accidental injury. Classic traps: missing a mild SUFE by not drawing the Klein line, and not imaging the hips when a child presents with isolated knee pain.
SALTRSalter-Harris Classification
Hook:SALTR: Slip, Above, Lower, Through, Rammed — the five Salter-Harris types in order of increasing severity.
Overview
Radiological signs in paediatric orthopaedics are fundamental examination topics that test pattern recognition, understanding of growth plate anatomy, and knowledge of specific paediatric conditions. The key principle is that the developing skeleton has unique anatomical features (growth plates, ossification centres, developing joint morphology) that create both diagnostic challenges and specific pathological patterns not seen in adults.
The paediatric skeleton differs from the adult in: (1) Growth plates (physes) are cartilaginous and radiolucent — fractures through them may be invisible on radiographs (Salter-Harris I, V). (2) Ossification centres appear sequentially and can be confused with fractures (CRITOE in the elbow). (3) The periosteum is thicker and more metabolically active — greenstick and torus (buckle) fractures are unique to children. (4) Joints are more cartilaginous — ultrasound is needed before ossification occurs (DDH screening). (5) Remodelling potential is greater but depends on direction of angulation and proximity to the growth plate.
The Klein line is the single most important and most commonly tested radiographic sign in paediatric orthopaedics. HOW TO DRAW IT: on the AP pelvis or hip radiograph, draw a line along the superior cortex of the femoral neck and extend it laterally. In NORMAL hips, this line should intersect (cut through) the lateral portion of the femoral head epiphysis. In SUFE: the epiphysis has slipped posteriorly (and often inferiorly), so the Klein line passes ABOVE or TANGENTIAL to the epiphysis without intersecting it. ALWAYS CHECK BOTH SIDES. CRITICAL PITFALL: SUFE can present with isolated KNEE pain (referred pain via the obturator nerve). ALWAYS image the hips when assessing a child with atraumatic knee pain.
Systematic Approach
Paediatric Radiological Signs Assessment
- Key Radiological Sign(s)
- USS: Graf classification (alpha/beta angles). AP pelvis (more than 6mo): Perkins + Hilgenreiner lines, acetabular index, Shenton line
- Clinical Significance
- Femoral head in superolateral quadrant = subluxation/dislocation. Acetabular index more than 30 degrees = dysplasia
- Key Radiological Sign(s)
- Klein line fails to intersect epiphysis on AP. Frog lateral: ice cream off cone. Southwick angle for severity
- Clinical Significance
- Any positive Klein line = SUFE. Check BOTH sides (bilateral in 20-40%). Non-weight-bearing until surgical fixation
- Key Radiological Sign(s)
- Catterall: extent of head involvement (groups I-IV). Herring: lateral pillar height (A, B, C). Head-at-risk signs: Gage sign, lateral calcification
- Clinical Significance
- Herring A = good prognosis. Herring C = poor. Head-at-risk signs indicate need for containment treatment
- Key Radiological Sign(s)
- SALTR: I (physis only — may be normal radiograph), II (physis + metaphysis — most common), III (physis + epiphysis), IV (all three), V (crush — retrospective)
- Clinical Significance
- Type I: clinical diagnosis (tenderness at physis). Type III-IV: need anatomical reduction (ORIF). Type V: worst growth outcome
- Key Radiological Sign(s)
- Metaphyseal corner fractures (bucket-handle), multiple fractures of different ages, posterior rib fractures, complex skull fractures
- Clinical Significance
- Metaphyseal corner fractures in infants are HIGHLY SPECIFIC for NAI. Skeletal survey is mandatory
- Key Radiological Sign(s)
- Proximal femoral focal deficiency (PFFD), fibular hemimelia, limb length discrepancy
- Clinical Significance
- Aitken classification for PFFD. Scanogram for limb length. Planning for reconstruction or amputation
Differential Diagnosis of the Limping / Painful Paediatric Hip by Age
- Most likely diagnoses
- DDH, septic arthritis/osteomyelitis, toddler's fracture, NAI
- Discriminating radiological / clinical clue
- DDH: disrupted Shenton line, head superolateral. Septic: effusion on USS, raised inflammatory markers. NAI: metaphyseal corner fracture, fractures of different ages
- Most likely diagnoses
- Transient synovitis, Perthes disease, septic arthritis, JIA
- Discriminating radiological / clinical clue
- Perthes: sclerotic/fragmented epiphysis, lateral pillar collapse. Transient synovitis: normal radiograph, small effusion, well child. Septic: Kocher criteria positive
- Most likely diagnoses
- SUFE, septic arthritis, apophyseal avulsion, JIA, tumour
- Discriminating radiological / clinical clue
- SUFE: positive (modified) Klein line, posterior slip on frog lateral. Avulsion: displaced apophysis (AIIS, ischium). Tumour: aggressive periosteal reaction, soft-tissue mass
- Most likely diagnoses
- Septic arthritis, malignancy (leukaemia, osteosarcoma, Ewing), NAI
- Discriminating radiological / clinical clue
- Fever, night pain, systemic upset, weight loss, refusal to bear weight, raised CRP/ESR — escalate urgently, do not assume benign cause
The two most dangerous misses are SEPTIC ARTHRITIS (a surgical emergency — use the Kocher criteria: non-weight-bearing, fever over 38.5C, ESR over 40, WCC over 12) and SUFE presenting as knee pain. Transient synovitis is a diagnosis of EXCLUSION in a well child with a normal radiograph — never apply it to an unwell or febrile child.
Detailed Condition Assessment
DDH Radiographic and Ultrasound Assessment
Before 6 months (ultrasound): The femoral head has not ossified, making radiographs unreliable. Ultrasound (hip USS) is the primary imaging modality. The Graf classification uses the alpha angle (bony acetabular coverage) and beta angle (cartilaginous coverage): Type I (normal): alpha more than 60 degrees. Type IIa (physiologically immature, under 3 months): alpha 50-59 degrees. Type IIb (delayed ossification, over 3 months — treat): alpha 50-59 degrees. Type III (subluxation): alpha less than 43 degrees. Type IV (dislocation): alpha less than 43 degrees, femoral head displaced.
After 6 months (radiograph): Four key assessments on AP pelvis radiograph (PHAS): (1) Perkins line (vertical from lateral acetabular rim) — femoral head ossification centre should be MEDIAL. (2) Hilgenreiner line (horizontal through triradiate cartilages) — femoral head should be INFERIOR. Together, these create four quadrants — the femoral head should be in the INFEROMEDIAL quadrant (any other location is abnormal). (3) Acetabular index — angle between Hilgenreiner line and the acetabular roof line. Normal: less than 30 degrees (decreases with age). More than 30 degrees = dysplastic. (4) Shenton line — smooth arc disrupted in subluxation/dislocation.
Additional DDH signs: Centre-edge angle of Wiberg (used in older children and adolescents): normal more than 25 degrees. Less than 20 degrees = dysplasia. Tonnis classification for acetabular coverage and subluxation grading in older patients.
PHASDDH Radiographic Assessment Lines
Hook:PHAS: Perkins, Hilgenreiner, Acetabular index, Shenton — the four lines/measurements for DDH assessment on AP pelvis.
KISSSUFE Radiographic Assessment
Hook:KISS: Klein line, Ice cream sign, Southwick angle, Symmetry — the four components of SUFE radiographic assessment.
CRITOE: Elbow Ossification Order
The paediatric elbow has six secondary ossification centres that appear in a predictable order, and knowing it is essential to avoid mistaking a normal centre for a fracture (or a fracture for a normal centre). The mnemonic is CRITOE, and the centres appear roughly at the odd ages 1, 3, 5, 7, 9, 11 (the "rule of odds"; girls ossify earlier than boys, so the ages are approximate).
- Centre
- Capitellum
- Approximate age (years)
- ~1
- Centre
- Radial head
- Approximate age (years)
- ~3
- Centre
- Internal (medial) epicondyle
- Approximate age (years)
- ~5
- Centre
- Trochlea
- Approximate age (years)
- ~7
- Centre
- Olecranon
- Approximate age (years)
- ~9
- Centre
- External (lateral) epicondyle
- Approximate age (years)
- ~11
The order itself is the exam trap. Because the internal (medial) epicondyle (I) always ossifies BEFORE the trochlea (T), you should never see a trochlear ossification centre without first seeing the medial epicondyle. If an ossific centre appears to be in the trochlear position but no medial epicondyle centre is visible in its normal location, suspect an avulsed and entrapped medial epicondyle that has been pulled into the joint (e.g. after an elbow dislocation) and is masquerading as the trochlea. Always confirm the medial epicondyle is present and correctly sited before accepting any later centre as normal.
Guidelines, Registries & Global Practice
Paediatric radiological signs are interpreted within national screening and child-protection frameworks that differ in detail but share the same imaging principles worldwide.
Global Epidemiology
- DDH: clinically significant dysplasia in roughly 1-3 per 1,000 live births, but sonographic immaturity/instability is far more common (Graf type IIa in ~14% of neonates). Risk factors: female sex, breech presentation, family history, firstborn, oligohydramnios, swaddling practices.
- SUFE: incidence ~10 per 100,000 children, rising with the global increase in childhood obesity; peak age 10-16 years; more common in boys and in some Pacific Islander, African and Hispanic populations; bilateral in 20-40%.
- Perthes: incidence varies markedly by region (roughly 1-20 per 100,000 children under 15), higher in Northern Europe and lower in some Asian and Black populations; boys affected 4-5 times more than girls.
- Physeal fractures: account for ~18-30% of paediatric long-bone fractures, peaking around the adolescent growth spurt (Olmsted County incidence 279/100,000 person-years).
Side-by-Side Guideline Comparison
- DDH screening stance
- Clinical exam for all newborns; selective ultrasound (6 weeks to 6 months) for risk factors or abnormal exam, rather than universal USS
- Imaging emphasis
- USS before femoral head ossifies; AP pelvis once ossific nucleus present
- DDH screening stance
- Universal newborn and 6-8 week clinical examination; selective USS by ~6 weeks for risk factors (breech, family history) or abnormal exam
- Imaging emphasis
- Graf/Harcke USS; radiograph reserved for older infants
- DDH screening stance
- Universal sonographic screening of all newborns (Graf method)
- Imaging emphasis
- Static Graf alpha/beta angles in a standardised coronal plane
- DDH screening stance
- Concludes evidence is insufficient to recommend FOR or AGAINST routine screening (I statement) — reflecting over-treatment concern
- Imaging emphasis
- Highlights high spontaneous resolution of immature hips
- DDH screening stance
- Not a screening body; standardises physeal fracture description and management
- Imaging emphasis
- Salter-Harris classification; CRITOE for elbow ossification
Registry and Practice Variation
- Registries: dedicated paediatric registries are fewer than adult arthroplasty registries, but regional DDH and Perthes datasets (e.g. UK BSCOS studies and Nordic/Australasian DDH cohorts) inform screening policy and late-presentation rates. The debate between universal (Graf, German-speaking Europe) and selective (US/UK) ultrasound screening turns on cost, over-treatment of self-resolving immature hips, and late-diagnosis rates.
- High-resource settings: ready access to ultrasound, MRI for occult physeal/Perthes assessment, and arthrography-guided reduction.
- Limited-resource settings: reliance on clinical examination and plain radiographs; DDH and SUFE often present late, increasing rates of open reduction, osteotomy, and established avascular necrosis. The same radiographic signs (Klein, Perkins/Hilgenreiner, Shenton, Salter-Harris) remain the diagnostic backbone everywhere because they require only a plain film.
- Child protection: suspected non-accidental injury triggers a standardised skeletal survey worldwide; mandatory reporting and exact survey protocols vary by jurisdiction, but the metaphyseal corner fracture, posterior rib fractures and fractures of differing ages are universally recognised red flags.
Controversies & Areas of Uncertainty
The biggest unresolved debate. Universal sonographic screening (Graf model, German-speaking Europe) detects more dysplasia but treats many hips that would resolve spontaneously (~89% of type IIa hips mature without intervention), risking over-treatment and Pavlik-related AVN. Selective screening (US/UK) targets risk factors but misses some late-presenting dysplasia. The USPSTF issued an "insufficient evidence" (I) statement. There is no internationally agreed gold-standard policy.
The classic Klein line misses up to 60% of slips (sensitivity ~40%). Over-reliance on a single AP sign is a recognised cause of missed/delayed SUFE diagnosis. The modified Klein line (interhip epiphyseal-width comparison) and routine frog-leg lateral views improve detection, but no single radiographic measurement is both highly sensitive and specific for mild slips.
Whether to pin the asymptomatic contralateral hip is contested. Arguments for: 20-40% become bilateral, sequential slip can be silent, and second slips can be unstable. Arguments against: morbidity of a second procedure in hips that may never slip. Prophylactic fixation is more widely favoured in younger children, those with open triradiate cartilage, and underlying endocrine/metabolic disease.
The Herring multicentre data show benefit from containment surgery only in a specific subgroup (lateral pillar B/B-C border, onset over 8 years); group A does well regardless and group C does poorly regardless. The optimal procedure (femoral varus vs innominate osteotomy) showed no significant difference, leaving surgeon and patient preference to guide choice.


Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 12-year-old obese boy presents with a 3-week history of left knee pain. He walks with an antalgic gait. There is no history of trauma.”
“A 6-month-old infant is brought for DDH assessment. The paediatrician has noted asymmetric skin folds and limited left hip abduction.”
“An examiner asks you to describe the Salter-Harris classification and its clinical implications.”
“A 7-year-old boy presents with a 4-month history of a painless limp and reduced left hip abduction and internal rotation. Radiographs show a fragmented, partially flattened left femoral head.”
DDH Assessment (PHAS)
- Perkins: vertical line from lateral acetabular edge
- Hilgenreiner: horizontal line through triradiate cartilages
- Together create 4 quadrants — femoral head should be INFEROMEDIAL
- Acetabular index: normal less than 30 degrees. More = dysplasia
- USS: before 6 months (Graf). Radiograph: after 6 months
SUFE Assessment (KISS)
- Klein line: along superior femoral neck — fails to intersect lateral epiphysis = SUFE
- Frog lateral: best view. Ice cream falling off cone appearance
- Southwick: mild (less than 30), mod (30-50), severe (more than 50 degrees)
- ALWAYS image hips for isolated knee pain in children
- Bilateral in 20-40%. Unstable = 47% AVN risk
Salter-Harris (SALTR)
- I (Slip): physis only — may be normal radiograph. Clinical diagnosis
- II (Above): physis + metaphysis — MOST COMMON (75%). Thurston-Holland fragment
- III (Lower): physis + epiphysis — intra-articular. ORIF for anatomical reduction
- IV (Through): all three zones — highest bone bridge risk. ORIF essential
- V (Rammed): crush — WORST prognosis. Diagnosed RETROSPECTIVELY
Perthes and NAI
- Herring lateral pillar: A (good), B (moderate), C (poor prognosis)
- Head-at-risk signs: Gage sign, lateral subluxation, lateral calcification
- NAI: metaphyseal corner fractures, posterior ribs, multiple ages
- NAI: skeletal survey MANDATORY. Mandatory reporting
Evidence Base
Herring Lateral Pillar Classification for Perthes
- Prospective multicentre study of 438 patients (451 hips), 345 hips followed to skeletal maturity across five treatment groups.
- The modified lateral pillar classification and age at onset were both strong, independent predictors of outcome (p less than 0.0001 and p = 0.0001).
- Lateral pillar group B (and B/C border) hips in children over 8 years at onset did significantly better with surgery than non-operative care; group C hips did poorly regardless of treatment.
- Group B hips in children 8 years or younger did equally well with operative and non-operative treatment.
Loder Stability Classification for SUFE
- 55 hips (in 54 patients) that would classically be labelled 'acute' were reclassified by physeal stability: 30 unstable, 25 stable.
- Avascular necrosis developed in 14 of 30 unstable hips (47%) and in NONE of the 25 stable hips (0%).
- Satisfactory outcome was reached in 47% of unstable versus 96% of stable hips.
- No association could be demonstrated between early reduction and the development of AVN.
Graf Sonographic Hip Screening — Prospective Validation
- Prospective study of 6,548 neonates examined both clinically and sonographically using Graf's technique.
- 84.6% of hips were mature (Graf type I), 14.3% physiologically immature (type IIa), and 1.1% dysplastic; 63% of sonographically dysplastic hips were clinically normal.
- 89% of type IIa hips matured spontaneously, while 11% required abduction treatment.
- All 68 dysplastic hips normalised (alpha and acetabular index angles) after a maximum of 80 days of abduction, though six hips deteriorated again by 1 year.
Modified Klein Line Improves SCFE Sensitivity
- Five observers assessed 30 AP and 30 frog-leg lateral radiographs of unilateral SCFE on two occasions.
- The CLASSIC Klein line (failure of the line to intersect the epiphysis) identified only 40.3% of slips — missing roughly 60%.
- A MODIFIED method (measuring the width of epiphysis lateral to Klein's line, with a 2 mm side-to-side difference indicating a slip) improved sensitivity to 79%.
- Head/shaft (Southwick) angle and percent epiphyseal displacement on the frog-leg lateral were reliable and reproducible, clearly separating slipped from control hips (p less than 0.001).
Physeal Fracture Epidemiology (Olmsted County)
- Population-based study identifying every physeal fracture in Olmsted County, Minnesota over 1979-1988: 850 children sustained 951 physeal fractures.
- Age- and sex-adjusted incidence was 279 per 100,000 person-years; boys outnumbered girls 2:1, with peaks at 11-12 years (girls) and 14 years (boys).
- The phalanges of the fingers were the most common site (37% of all physeal fractures).
- Salter-Harris type II was the commonest pattern (54%), but 16% of fractures did not fit the Salter-Harris scheme, prompting Peterson's expanded classification.
Metaphyseal Corner Fractures in NAI — Radiologic-Histopathologic Basis
- Combined pre- and post-mortem radiographs with histology of metaphyses from four abused infants explained the classic metaphyseal lesion.
- The underlying injury is a subepiphyseal planar series of microfractures through the most immature metaphyseal bone, isolating a mineralised disc.
- Depending on size, peripheral involvement and projection, the SAME lesion appears as a 'bucket-handle' fracture, a 'corner' fracture, or a metaphyseal lucency.
- Some radiographs were normal despite significant histologic injury, and the germinal cartilage layers were spared in the specimens examined.