Posterior Heel Pain | Haglund Association | Two-Finger Squeeze Test
- Two-finger squeeze test - compress bursa anterior to Achilles
- Avoid steroid injection into bursa - Achilles rupture risk
- Parallel pitch lines quantify Haglund deformity on XR
- Preserve at least 30 degree calcaneal pitch during Haglund resection (avoid over-resection)
- Associated with seronegative spondyloarthropathies
- “Differentiate from superficial (retroachilles) bursitis by location
- “Morning stiffness suggests inflammatory arthropathy association
- “MRI shows T2-bright fluid in bursa with surrounding edema
- “Endoscopic vs open approach depends on surgeon expertise
Overview
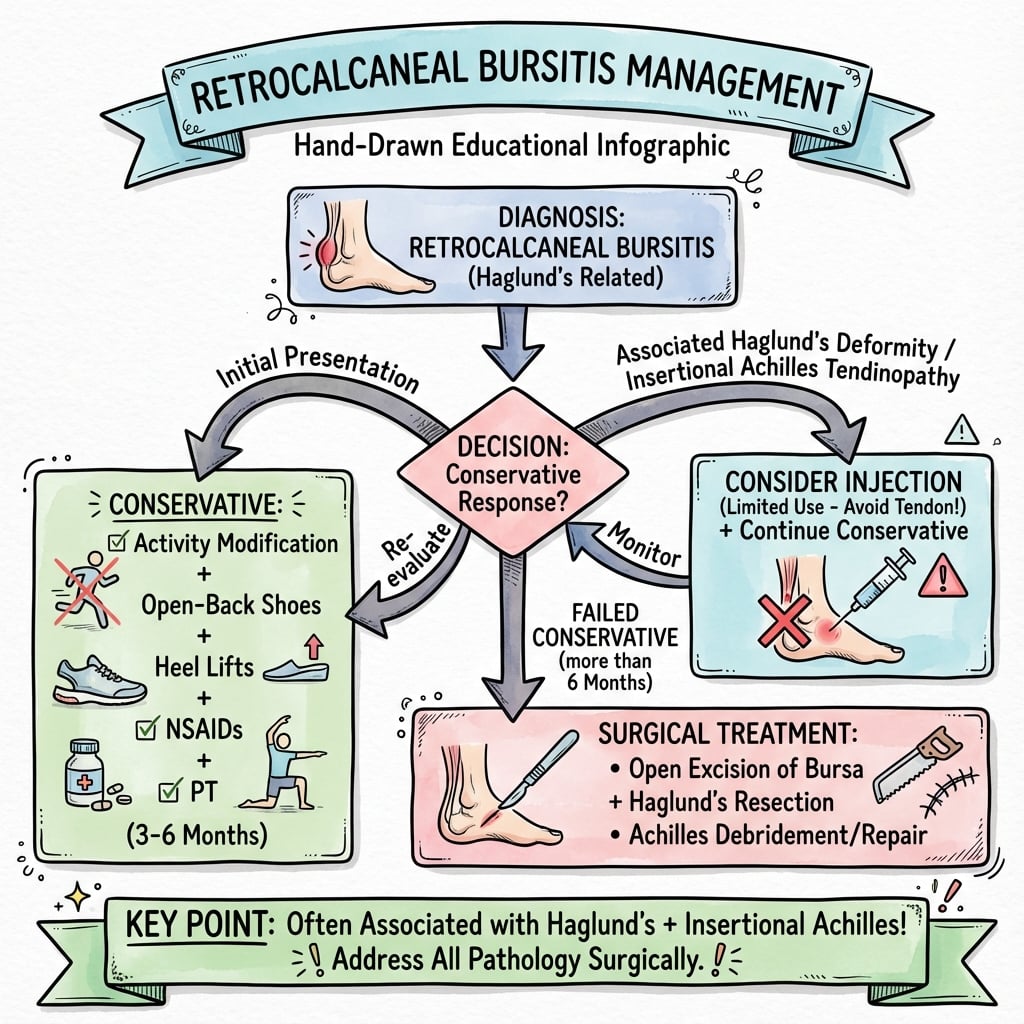
Retrocalcaneal bursitis is inflammation of the bursa between the Achilles tendon and posterosuperior calcaneus, often associated with Haglund's deformity (posterosuperior calcaneal prominence). Key clinical finding is the two-finger squeeze test - compressing the bursa between thumb and index finger anterior to the Achilles. Distinguish from superficial calcaneal bursitis (retroachilles bursa between skin and tendon) and insertional Achilles tendinopathy. Conservative management succeeds in 80-90% (activity modification, NSAIDs, heel lifts). Critical trap: avoid steroid injection directly into bursa due to Achilles rupture risk. Surgery for refractory cases includes bursectomy ± Haglund resection, preserving at least 30° calcaneal pitch.
Bursal Anatomy
Bursal Anatomy
- Lies between Achilles tendon anteriorly and posterosuperior calcaneal tuberosity posteriorly
- Superior boundary: Achilles tendon substance
- Inferior boundary: superior aspect of calcaneal attachment
- Does NOT communicate with ankle joint
- Normal bursa contains small amount of synovial fluid (less than 1mL)
- Located between Achilles tendon and skin
- Also called retroachilles or subcutaneous calcaneal bursa
- Develops in response to friction from shoe counter
- Often coexists with retrocalcaneal bursitis
- Clinically presents as visible swelling posterior to heel
Detailed Anatomy
Bursal Anatomy
- Lies between Achilles tendon and posterosuperior calcaneal tuberosity
- Normal dimensions: 6mm anterior-posterior, 3mm depth
- Contains less than 1mL synovial fluid normally
- Does NOT communicate with ankle joint
- Located between Achilles tendon and skin
- Often develops secondary to friction from footwear
- May coexist with retrocalcaneal bursitis
- Posterosuperior tuberosity is site of Haglund prominence
- Achilles insertion on posterior calcaneus below bursa
- Fowler-Philip angle measures prominence of posterosuperior corner
Severity Grading
There is no validated severity grading system for retrocalcaneal bursitis. Examiners expect you to state this and instead classify by etiology (mechanical, inflammatory, septic - see Classification) and by associated pathology (isolated bursitis through to full Haglund syndrome with insertional tendinopathy). The presence and extent of associated Achilles and bony pathology, not a numeric grade, drives treatment planning and surgical approach.
Sural Nerve: Hindfoot Anatomy and the Safe Zone
The sural nerve is the structure most at risk in posterolateral hindfoot surgery (about 3% injury rate) and a viva favourite, yet the body only says it "courses posterolateral to the lateral malleolus" without giving the course or how to stay off it.
- Course. The sural nerve forms in the calf from the medial sural cutaneous nerve (from the tibial nerve, between the two heads of gastrocnemius), usually joined by a peroneal communicating branch. It pierces the deep fascia in the mid-calf, runs alongside the small saphenous vein, and passes about 1-1.5cm posterior (and slightly inferior) to the lateral malleolus, then curves forward below the malleolar tip toward the base of the fifth metatarsal, supplying sensation to the posterolateral leg, lateral heel and lateral border of the foot.
- Why it is at risk. In a posterolateral approach to the retrocalcaneal space the nerve lies just anterolateral to the Achilles at the operative level; a too-lateral incision, retractor pressure, or a distal-lateral endoscopic portal can catch it, producing lateral heel/foot numbness or a painful neuroma.
- Staying safe. Keep the incision just lateral to the Achilles midline but posterior to the nerve's course, use blunt dissection straight down to bone, and for endoscopic calcaneoplasty place the lateral portal at the superior calcaneal level with care - the small saphenous vein is the surface marker to respect, since the nerve runs with it.
Q: Describe the sural nerve's course in the hindfoot and how you protect it during retrocalcaneal surgery. A: It arises in the calf (medial sural cutaneous from the tibial nerve, usually joined by a peroneal communicating branch), pierces the deep fascia in the mid-calf and runs with the small saphenous vein about 1-1.5cm posterior to the lateral malleolus, curving forward below the malleolus to the base of the fifth metatarsal and supplying the lateral heel and lateral border of the foot. Protect it by keeping the incision just lateral to the Achilles but posterior to the nerve, using blunt dissection to bone, and respecting the small saphenous vein (its surface marker) when placing a lateral endoscopic portal.
FHL Transfer to Augment the Achilles Insertion
The topic repeatedly states that if more than 50% of the Achilles insertion is detached or debrided the repair should be augmented with an FHL transfer, and a viva followUp asks for the technique - but the operation is never described.
- Why the FHL. The flexor hallucis longus is the ideal donor: it is the strongest expendable posterior-compartment tendon, its muscle belly is low-lying and vascularised (bringing blood supply to a poorly-vascular insertional zone), it is in-phase with the gastroc-soleus (both plantarflex), and it lies immediately deep to the Achilles so it is harvested through the same wound.
- Harvest. The FHL is identified deep to the Achilles through the posteromedial part of the exposure; a single-incision harvest divides it as far distally as can be reached behind the ankle, while a two-incision technique adds a medial midfoot incision for extra length - protecting the medial and lateral plantar nerves at the master knot of Henry, where the FHL crosses the FDL.
- Fixation. After the bursectomy, Haglund resection and tendon debridement, the FHL is passed into a calcaneal bone tunnel or fixed with an interference screw/anchor just anterior to the debrided Achilles footprint and tensioned with the ankle in slight plantarflexion; the residual Achilles insertion is then reattached over it with suture anchors.
- Consequence. Loss of independent hallux interphalangeal flexion is well tolerated (the FDL and intrinsics compensate); the trade buys a vascularised, strong reconstruction that guards against post-debridement rupture. (The FHL transfer for chronic Achilles rupture is developed in the Achilles-rupture topic.)
Q: When and how do you augment the Achilles with an FHL transfer during Haglund/insertional surgery? A: Augment when more than 50% of the Achilles insertion is detached or debrided. The FHL is chosen because it is the strongest expendable, in-phase donor with a low vascular muscle belly lying just deep to the Achilles. Harvest it through the same posteromedial exposure (single-incision, or two-incision for extra length while protecting the plantar nerves at Henry's knot), fix it into a calcaneal bone tunnel or with an interference screw/anchor anterior to the Achilles footprint, tension in slight plantarflexion, and reattach the residual Achilles over it. Loss of hallux IP flexion is well tolerated.
Pathophysiology
The retrocalcaneal bursa functions to reduce friction between the Achilles tendon and calcaneus during ankle dorsiflexion. Repetitive compression during activities leads to inflammatory response within the bursal sac.
Haglund Deformity Components:
The classic triad consists of:
- Posterosuperior calcaneal prominence (pump bump)
- Retrocalcaneal bursitis
- Insertional Achilles tendinopathy
Geometric assessment on lateral radiograph includes parallel pitch lines, posterior calcaneal angle, and Fowler-Philip angle to quantify bony prominence.
HAGLUNDHAGLUND - Deformity Features
Hook:Named after Swedish orthopedic surgeon Patrick Haglund (1928)
Risk Factors
Risk Factor Categories
Classification
Retrocalcaneal bursitis is classified by underlying cause:
- Mechanical / Primary: associated with Haglund deformity and biomechanical overload (most common)
- Inflammatory: associated with seronegative spondyloarthropathies (bilateral, morning stiffness, often HLA-B27 positive)
- Septic: rare bacterial infection of the bursa (acute, erythema, fever)
Clinical Presentation
History
- Gradual onset posterior heel pain
- Pain worse with activity, especially running and jumping
- Aggravation with shoe wear, particularly rigid heel counters
- Morning stiffness that improves with initial activity
- Pain with direct pressure on posterosuperior heel
- May report visible swelling or prominence
- Acute onset suggests Achilles rupture
- Night pain suggests infection or tumor
- Bilateral symmetric involvement suggests inflammatory arthropathy
- Fever or constitutional symptoms suggest septic bursitis
Physical Examination
- Observe hindfoot alignment (varus predisposes to lateral impingement)
- Assess for visible posterosuperior prominence (Haglund deformity)
- Look for erythema suggesting superficial bursitis
- Check for swelling anterior to Achilles tendon insertion
- Antalgic gait with shortened stance phase
- Reduced push-off power
- May adopt toe-walking pattern to avoid dorsiflexion
- Assess for limb length discrepancy
The visual appearance can help differentiate superficial from deep bursitis. Superficial bursitis presents with obvious posterior swelling that is fluctuant and superficial to the Achilles. Retrocalcaneal bursitis shows subtle fullness on either side of the Achilles when viewed from posterior aspect.
Clinical Assessment
Clinical Assessment Summary
- Duration and onset of symptoms
- Activity relationship (running, sport participation)
- Footwear aggravation
- Prior treatments attempted
- Systemic symptoms (bilateral, morning stiffness suggests inflammatory cause)
- Standing inspection for hindfoot alignment
- Palpation of retrocalcaneal space (two-finger squeeze test)
- Range of motion assessment
- Differential testing (Thompson test for Achilles rupture)
- Two-finger squeeze test positive (85% sensitivity)
- Pain with forced dorsiflexion
- Visible posterosuperior prominence (Haglund)
Investigations
Radiographic Assessment
Plain Radiographs
- Lateral view - primary imaging study for Haglund deformity assessment
- Weight-bearing preferred to assess true calcaneal position
- AP view to rule out other hindfoot pathology
- Calcaneal axial view if indicated
- First line: along plantar aspect of calcaneus
- Second line: from posterior plantar calcaneus to posterosuperior corner
- Third line: from posterior plantar calcaneus to medial tubercle
- Haglund deformity present if posterosuperior corner lies above second line
- Intersection of line parallel to calcaneal undersurface and line from posterior superior corner to medial tubercle
- Normal range: 44-69 degrees
- Angles less than 44 degrees associated with increased risk of retrocalcaneal bursitis
PITCHPITCH - Radiographic Assessment
Hook:PITCH lines help assess calcaneal pitch and prominence on lateral XR
Advanced Imaging
Imaging Modality Comparison
Laboratory Investigations
- Bilateral involvement suggests systemic disease
- Recurrent or refractory cases
- Constitutional symptoms present
- Young patient with no clear mechanical cause
- Inflammatory markers: ESR, CRP (elevated in inflammatory arthropathy)
- Rheumatoid factor and anti-CCP antibodies
- HLA-B27 for seronegative spondyloarthropathy screening
- Uric acid if gout suspected
- Complete blood count if infection concern
- Rarely indicated
- Consider if septic bursitis suspected
- Send for cell count, Gram stain, culture, crystal analysis
- Cloudy fluid with elevated WBC suggests infection
- Crystals may indicate gout or pseudogout
Disease Subtypes
Classification Overview
Retrocalcaneal bursitis is classified based on etiology and associated pathology:
- Mechanical/Primary: Associated with Haglund deformity and biomechanical factors
- Inflammatory: Associated with systemic inflammatory arthropathies
- Septic: Rare bacterial infection of the bursa
- Mild: Bursal inflammation only, minimal functional limitation
- Moderate: Bursal inflammation with Haglund deformity
- Severe: Combined pathology with insertional Achilles tendinopathy
Investigations
Investigation Summary
- Weight-bearing lateral foot radiograph
- Assess for Haglund prominence using parallel pitch lines
- Calculate Fowler-Philip angle (normal 44-69 degrees)
- MRI if diagnosis uncertain or surgical planning needed
- Ultrasound for bursal assessment and guided injection
- Bilateral involvement
- Young patient without mechanical cause
- Features of inflammatory arthropathy
- Tests: ESR, CRP, RF, anti-CCP, HLA-B27, uric acid
Differential Diagnosis
Posterior Heel Pain Differential
Management
Non-Operative Treatment
- Reduce or eliminate aggravating activities
- Avoid hill running and excessive dorsiflexion activities
- Cross-training with low-impact activities (cycling, swimming)
- Gradual return to sport protocol when symptoms resolve
- Shoes with soft heel counter or no heel counter
- Heel lifts 6-12mm to reduce dorsiflexion stress
- Wider heel box to reduce compression
- Avoid new or poorly fitted shoes
- Eccentric Achilles strengthening program
- Gastrocnemius and soleus stretching
- Manual therapy for soft tissue mobilization
- Ultrasound therapy for anti-inflammatory effect
- NSAIDs for 2-4 weeks (if no contraindications)
- Topical NSAIDs as alternative
- Avoid oral corticosteroids (limited evidence)
- Analgesics for pain control
Injection Therapy:
- Limited high-quality evidence supporting steroid injection
- Risk of Achilles rupture outweighs potential benefits in most cases
- PRP or autologous blood injection: insufficient evidence
- If injection performed: must be under imaging guidance, patient counseled on rupture risk
- Low to moderate energy shockwave therapy
- May stimulate healing and reduce inflammation
- Limited evidence specifically for retrocalcaneal bursitis
- More evidence for insertional Achilles tendinopathy
- Typical protocol: 3-5 sessions over 6-12 weeks
Surgical Treatment
Technique: Posterolateral Incision
- Prone or lateral decubitus position
- Tourniquet application optional
- Bump under ipsilateral hip if prone
- Ensure adequate fluoroscopy access
-
Incision: 6-8cm posterolateral incision centered over posterosuperior calcaneus, lateral to Achilles tendon midline to avoid scar contracture
-
Dissection: Identify and protect sural nerve branches, incise deep fascia, identify retrocalcaneal bursa lateral to Achilles
-
Bursal Excision: Complete excision of thickened bursal tissue, visualize insertion of Achilles on posterosuperior calcaneus
-
Haglund Resection: If prominent, use osteotome or sagittal saw to resect posterosuperior prominence parallel to posterior facet of calcaneus
-
Bone Recontouring: Smooth remaining bone with rongeur or burr, ensure no sharp edges, preserve Achilles insertion
-
Achilles Assessment: Inspect for insertional pathology, debride diseased tissue if present, repair insertion if detached
-
Closure: Deep dermal sutures, skin closure with interrupted or continuous suture, sterile dressing, posterior splint in neutral
- Incision must be lateral to avoid wound healing complications
- Preserve minimum 1cm superior calcaneal attachment of Achilles
- Resect prominence but maintain calcaneal pitch greater than 30 degrees
- Aggressive debridement of Achilles risks rupture
The posterolateral approach provides excellent visualization of the retrocalcaneal space and allows complete bursectomy with or without Haglund resection while protecting the Achilles insertion.
- 35 studies, 1260 ankles (1147 patients); overall good results and high satisfaction
- Endoscopic vs open: AOFAS 90.7 vs 87.1, complications 4.1% vs 15.5%, failures 1.2% vs 6.0% (all p less than 0.001)
- Faster return to sport with endoscopic (11.9 vs 20.7 weeks)
Rehabilitation Protocol
Post-Operative Rehabilitation Timeline
Modified Protocol if Achilles Detached:
- Extended period of plantarflexion positioning (4 weeks)
- Delayed active ROM to 4-6 weeks
- More gradual progression of strengthening
- Return to sport typically 6-9 months rather than 3-6 months
Management Algorithm
Surgical Technique
Surgical Technique Summary
- Position: Prone or lateral decubitus
- Incision: 6-8cm posterolateral, lateral to Achilles midline
- Identify and protect sural nerve branches
- Incise deep fascia, identify retrocalcaneal bursa
- Complete bursectomy
- Haglund resection if prominent (parallel to posterior facet)
- Smooth remaining bone with rongeur or burr
- Preserve Achilles insertion
- Layered closure, posterior splint in neutral
- 2-portal technique (medial and lateral)
- Arthroscopic bursectomy and calcaneoplasty
- Smaller incisions, potentially faster recovery
Complications
Surgical Complications
- Delayed healing due to tenuous soft tissue coverage
- Increased risk with midline incisions
- Prevention: lateral incision, meticulous tissue handling
- Treatment: local wound care, delayed closure if needed
- Superficial wound infection most common
- Deep infection rare but serious
- Treatment: antibiotics, surgical debridement if deep
- May require drainage if symptomatic
- Prevention: meticulous hemostasis, drain placement
- Numbness lateral heel and foot
- Painful neuroma formation
- Prevention: identify and protect during lateral dissection
- Treatment: neuroma excision if symptomatic
- Risk increased with aggressive debridement
- Higher risk if greater than 50% insertion debrided
- Prevention: preserve insertion, FHL augmentation if needed
- Treatment: surgical repair with augmentation
- Inadequate Haglund resection most common cause
- Failure to address biomechanical factors
- Treatment: revision surgery with adequate resection
Treatment Complications
Complications
Complication Overview
- Wound healing problems (6%) - especially with midline incisions
- Infection (less than 2%)
- Hematoma
- Sural nerve injury (3%) - numbness lateral foot, neuroma
- Achilles rupture (2%) - higher risk if aggressive debridement
- Recurrence (5-10%) - usually from inadequate resection
- Use lateral incision, not midline
- Protect sural nerve throughout dissection
- Preserve Achilles insertion where possible
- Adequate but not excessive Haglund resection
Postoperative Care
Rehabilitation Protocol
Phase 1 (Weeks 0-2): Protection
- Non-weight bearing in posterior splint or CAM boot
- No active dorsiflexion
- Toe range of motion, quad sets, hip strengthening
Phase 2 (Weeks 2-6): Early Motion
- Partial weight bearing in CAM boot
- Gentle passive ROM, progress to active
- Begin pool therapy if available
Phase 3 (Weeks 6-12): Strengthening
- Progress weight bearing as tolerated
- Transition from boot to supportive shoe
- Eccentric Achilles strengthening program
- Proprioceptive training
Phase 4 (Months 3-6): Return to Activity
- Sport-specific training
- Plyometrics when appropriate
- Full return to activity 4-6 months
Prognosis
Expected Outcomes
- Success rate: 80-90% with comprehensive non-operative management
- Average time to resolution: 3-6 months
- Recurrence rate: 10-15% with return to previous activity levels
- Factors predicting success: early intervention, good compliance, modification of risk factors
- Good to excellent results: 85% at 2-5 year follow-up
- Symptom resolution: 90% achieve significant pain improvement
- Return to previous activity level: 75-80%
- Time to full activity: 4-6 months (without detachment), 6-9 months (with Achilles detachment and repair)
- Isolated retrocalcaneal bursitis without Achilles pathology
- Mechanical etiology rather than inflammatory
- Adequate non-operative trial before surgery
- Good surgical technique with complete resection
- Excellent rehabilitation compliance
- Inflammatory arthropathy as underlying cause
- Extensive Achilles pathology requiring detachment
- Workers' compensation claim or litigation
- Smoking or uncontrolled diabetes
- Previous failed surgery
- Inadequate Haglund resection
- Persistent equinus contracture
- Return to high-impact activities too quickly
- Failure to modify footwear
- Underlying systemic inflammatory condition
Long-Term Considerations:
- Most patients maintain good results long-term if activity modifications continued
- Small percentage develop insertional Achilles tendinopathy later
- Importance of ongoing Achilles flexibility and strength maintenance
- Periodic reassessment if symptoms recur
- 47 patients (20 open, 27 endoscopic); no significant difference in any outcome score (VAS, AOFAS, FFI, Tegner, SF-36)
- Extent of bony resection equivalent between techniques
- Sural nerve paraesthesia only in open group (2 patients); endoscopic surgery took longer (65 vs 45 min)
- Endoscopic learning curve plateaued after the fourth case
Outcomes
Treatment Outcomes
- Success rate: 80-90% with comprehensive management
- Time to resolution: 3-6 months
- Recurrence: 10-15% with return to previous activity
- Good to excellent results: 85% at 3-5 year follow-up
- Patient satisfaction: 88-91%
- Return to previous activity level: 75-80%
- Complication rate: 11% overall
- AOFAS hindfoot scores improve from 52 to 88 post-operatively
- Most patients return to sport by 4-6 months
Guidelines, Registries & Global Practice
Global Epidemiology and Practice
- Posterior heel pain (insertional Achilles tendinopathy, retrocalcaneal bursitis and Haglund deformity overlap clinically) accounts for roughly one third of Achilles disorders; the spectrum is most common in adults aged 40-60 and in running/jumping athletes.
- There is no procedure-specific national joint registry for calcaneoplasty or bursectomy (registries capture arthroplasty, not soft-tissue/foot-and-ankle minor procedures), so evidence rests on systematic reviews and cohort series rather than registry survivorship data.
- Universal first principle across all societies: a structured conservative programme for a minimum of 3-6 months before surgical referral.
Imaging access by setting:
- Weight-bearing lateral radiograph is the universally available, low-cost first-line study.
- Ultrasound is the preferred soft-tissue and dynamic tool in most systems (cheap, no radiation).
- MRI is reserved for diagnostic uncertainty or surgical planning and may be rationed in publicly funded or limited-resource settings.
Controversies & Areas of Uncertainty
- No robust conservative-vs-surgical RCT exists; the 6-month conservative threshold is consensus-based, not trial-proven.
- Optimal extent of Haglund resection is undefined; over-resection risks calcaneal fracture or Achilles avulsion, under-resection risks recurrence.
- Radiographic thresholds are contested - Fowler-Philip angle and parallel pitch lines correlate poorly with symptoms (Tang 2022); newer bump-based ratios may be better but are not validated prospectively.
- Adjunctive ESWT did not improve insertional disease over eccentrics alone in a Level I RCT (Mansur 2021), challenging routine use.
- Zadek (dorsal closing-wedge) osteotomy is gaining favour as a tendon-sparing alternative that reduces posterior impingement without touching the insertion.
- Minimally invasive / percutaneous osteotomy shows lower reported complication rates but limited case numbers.
- Distinguishing the pain generator (bursa vs insertion vs bone) remains imprecise; asymptomatic bursal fluid is common on MRI, so imaging must be correlated clinically.
- 9 RCTs, 464 participants; very low overall certainty of evidence
- Eccentric exercise plus soft-tissue therapy ranked highest for short-term pain (SUCRA 84.8)
- No single non-surgical modality could be definitively recommended over others
- 17 studies, 611 subjects, 625 Zadek osteotomy procedures
- Both open and percutaneous improved AOFAS, FFI, VISA-A and VAS scores
- Reported complication rate 5.8% percutaneous vs 10.2% open
- Percutaneous data still limited (only 11% of cases)
- 14 trials, 452 procedures in 433 patients; surgical satisfaction high across techniques (mean 89%)
- ESWT superior to both wait-and-see and eccentric training for non-calcified disease
- Eccentric exercises reduced VAS but full-range protocols had high dissatisfaction
- Insufficient evidence to recommend any single surgical technique
- 119 patients randomised to eccentrics plus radial ESWT versus eccentrics plus sham
- No between-group difference in VISA-A at 24 weeks (63.2 vs 62.3, p=0.876)
- ESWT group had higher failure (38.3% vs 11.5%) but lower recurrence (17.0% vs 34.6%)
- No complications in either group
- 43 operatively treated Haglund patients versus 41 asymptomatic controls
- Traditional Fowler-Philip angle and parallel pitch lines did NOT differ between groups
- Bump height (cut-off 4mm or more) and bump-calcaneus ratio (7.5% or more) distinguished symptomatic deformity
- Bump-calcaneus ratio had the highest reliability (inter-observer ICC 0.889)
Essential Mnemonics
BURSABURSA - Anatomic Boundaries
Hook:Bursa is sandwiched between bone and tendon, distinct from superficial bursa
MCQ Practice Points
Q: What is the difference between retrocalcaneal bursitis and superficial (Achilles) bursitis?
A: Retrocalcaneal bursitis: Inflammation of bursa deep to Achilles tendon, between tendon and calcaneus. Associated with Haglund's deformity (posterosuperior calcaneal prominence). Pain anterior to Achilles insertion, worsened by dorsiflexion (compresses bursa). Superficial (retroachilles/Achilles) bursitis: Inflammation of bursa superficial to Achilles insertion, between skin and tendon. Often from shoe friction ("pump bump"). Visible swelling posterior to tendon insertion. Both may coexist. Distinction important for treatment planning.
Q: What is Haglund's deformity and how does it cause retrocalcaneal bursitis?
A: Haglund's deformity is a prominent posterosuperior calcaneal tuberosity that impinges on the Achilles tendon and retrocalcaneal bursa during dorsiflexion. Causes: Congenital bone prominence, high-arched (cavus) foot, tight Achilles. Mechanism: Repetitive dorsiflexion causes bursa and anterior tendon surface to be compressed against the bony prominence, leading to bursitis and insertional tendinopathy. Radiographic measurement: Parallel pitch lines or Fowler-Philip angle (greater than 75 degrees indicates prominent tuberosity). Often bilateral.
Q: What imaging findings are seen in retrocalcaneal bursitis and Haglund's syndrome?
A: Radiographs: Lateral view shows posterosuperior calcaneal prominence (Haglund's), loss of normal retrocalcaneal recess (soft tissue swelling), may show calcification at Achilles insertion (insertional tendinopathy). MRI: Distended retrocalcaneal bursa (high T2 signal), Achilles tendon thickening and degeneration at insertion, bone marrow edema in calcaneus, intrasubstance tendon signal changes. Ultrasound: Bursal fluid collection, tendon changes, can guide aspiration/injection. Imaging helps differentiate from isolated insertional tendinopathy or intratendinous pathology.
Q: What is the non-operative management of retrocalcaneal bursitis?
A: Activity modification: Avoid aggravating activities (hills, stairs). Footwear: Open-backed shoes or soft heel counters, heel lifts (reduce dorsiflexion). Physical therapy: Achilles stretching, eccentric strengthening (limited evidence for insertional disease compared to mid-portion). Anti-inflammatory: NSAIDs, ice. Injections: AVOID corticosteroid injection into the retrocalcaneal bursa - the Achilles lies immediately adjacent and steroid weakens the tendon, risking rupture; this is the high-yield trap. Heel pad/cushioning: Reduce pressure on posterior heel. Trial of 3-6 months conservative treatment before surgery.
Q: What are the surgical options for refractory retrocalcaneal bursitis with Haglund's deformity?
A: Endoscopic bursectomy and calcaneal ostectomy: Minimally invasive, faster recovery; removes bursa and resects posterosuperior calcaneal prominence; avoid excessive bone removal (detaches Achilles). Open surgery: For severe cases or combined insertional tendinopathy; bursectomy + calcaneal exostectomy + debridement of degenerative tendon + possible tendon augmentation (FHL transfer) if greater than 50% tendon detachment required. Postoperative: Protected weight-bearing 2-6 weeks, gradual return to activity 3-6 months. Complications: Wound healing problems (posterior heel), Achilles detachment, persistent pain.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old recreational runner presents with 8 months of posterior heel pain that has failed to improve with rest, physiotherapy, and NSAIDs. Clinical examination reveals tenderness anterior to the Achilles insertion bilaterally. MRI demonstrates retrocalcaneal bursitis with Haglund deformity. How would you manage this patient?”
“You are reviewing a patient 4 weeks after open bursectomy and Haglund resection. The patient complains of numbness over the lateral border of the foot and painful hypersensitivity in that region. What has happened and how would you manage this complication?”
Definition
- Inflammation of the retrocalcaneal bursa between Achilles tendon and posterosuperior calcaneus
- Often associated with Haglund deformity (pump bump)
Clinical Diagnosis
- Posterior heel pain worse with activity and dorsiflexion
- Tenderness ANTERIOR to Achilles insertion
- Positive two-finger squeeze test
- Painful arc with ankle dorsiflexion
Investigation Sequence
- Lateral radiograph with parallel pitch lines and Fowler-Philip angle
- MRI shows high T2 signal in bursa
- Screen for inflammatory arthropathy if bilateral (ESR, CRP, RF, HLA-B27)
Conservative Treatment
- 80-90% success rate
- Activity modification, heel lifts 6-12mm, soft heel counter shoes
- NSAIDs, eccentric Achilles exercises, ESWT
- Minimum 12 week trial
- AVOID direct bursal steroid injection
Surgical Indications
- Failure of 6 months conservative treatment
- Functional impairment
- MRI-confirmed pathology
- Posterolateral approach for bursectomy and Haglund resection preserving Achilles insertion
Complications
- Wound healing 6%
- Sural nerve injury 3%
- Achilles rupture 2%
- Recurrence 5-10%
- FHL augmentation if greater than 50% Achilles debridement needed
Outcomes
- 85% good-excellent results at 3 years post-surgery
- Return to sport 4-6 months
- Worse outcomes with inflammatory arthropathy, extensive Achilles pathology, smoking
Differential Diagnosis
- Insertional Achilles tendinopathy (pain AT insertion)
- Superficial bursitis (visible swelling)
- Paratendinitis (mid-substance)
- Posterior impingement (plantarflexion pain)
Evidence Base
Key Evidence
- Conservative management successful in 80-90% of cases
- Surgery reserved for failure of 6+ months conservative treatment
- No significant difference in long-term satisfaction between approaches
- Open vs endoscopic: Similar satisfaction rates (91% vs 88%)
- Endoscopic may have faster return to work
- Complication rates similar between approaches
- Limited high-quality evidence
- Risk of Achilles rupture outweighs potential benefit
- Not routinely recommended