Posterior Instability | Impression Fracture | McLaughlin Lesion
- Often associated with posterior shoulder dislocation (seizures, electrocution)
- Lightbulb sign on AP X-ray due to internal rotation
- Critical defect size is greater than 25% (some sources say 20%)
- Modified McLaughlin transfers subscapularis/lesser tuberosity into defect
- Chronic locked posterior dislocations are frequently missed
- “Demonstrate the 'Posterior Drawer' and 'Jerk Test' in viva
- “Axillary lateral view is mandatory to confirm diagnosis
- “Distinguish between 'engaging' and 'non-engaging' lesions
- “Review the 3 'E's of posterior dislocation: Epilepsy, Ethanol, Electricity
Posterior dislocations are the most commonly missed major joint dislocation (greater than 50% missed initially). Always check axillary view.
20-25% articular surface. Defects larger than this are unstable and engage with the posterior glenoid rim.
Adduction + Internal Rotation. Seizures and electrocution cause massive muscle contraction (Lat/Pec/Subscap) driving head posterior.
less than 3 weeks = Acute. Over 3 weeks = Chronic. Affects reducibility and viability of the head.
- Defect Size
- Small (under 20%)
- Treatment
- Closed Reduction + Brace
- Key Pearl
- Immobilize in ER (gunslinger)
- Defect Size
- Medium (20-45%)
- Treatment
- Mod. McLaughlin / Allograft
- Key Pearl
- Transfer L.T. into defect
- Defect Size
- Large (over 45%)
- Treatment
- Hemi / Total Shoulder
- Key Pearl
- Head is unsalvageable
LIRThe 3 Signs on X-ray
Hook:Look for LIR (Lighthouse in Rain) - Lightbulb, Impression, Rim!
Overview and Epidemiology
Reverse Hill-Sachs Lesion: An impaction fracture of the anteromedial humeral head. Reverse Bankart Lesion: Injury to the posterior glenoid labrum. Both occur in posterior shoulder instability/dislocation.
Impaction of the anterior humeral head against the posterior glenoid rim during dislocation.
Often present as "Locked Posterior Dislocation". The head is impacted and cannot be reduced closed.
Pathophysiology and Mechanisms
A Reverse Hill-Sachs lesion is considered "engaging" if the defect falls off the posterior glenoid rim when the arm is internally rotated and flexed (functional position). This causes recurrent instability.
Mechanism of Injury
- Axial loading of the adducted and internally rotated arm.
- Violent muscle contraction: The internal rotators (Latissimus Dorsi, Pectoralis Major, Subscapularis) are stronger than external rotators.
- During a seizure, these muscles overpower the external rotators, forcing the humeral head posteriorly.
The Defect
- Location: Anteromedial humeral head.
- Comparison: A reflected image of a standard Hill-Sachs (which is posterolateral).
- Engagement: As the arm internally rotates, the defect engages the posterior glenoid.
- Hill-Sachs
- Anterior
- Reverse Hill-Sachs
- Posterior
- Hill-Sachs
- Posterolateral
- Reverse Hill-Sachs
- Anteromedial
- Hill-Sachs
- Bankart (Anterior)
- Reverse Hill-Sachs
- Reverse Bankart (Posterior)
- Hill-Sachs
- Abduction + Ext Rotation
- Reverse Hill-Sachs
- Adduction + Int Rotation
3 EsCauses of Posterior Dislocation
Hook:The 3 Es force the head out the Back!
The Glenoid Track: Why a Reverse Hill-Sachs Engages
The topic repeatedly relies on "engaging vs non-engaging," the gamma angle, and a viva follow-up explicitly asks "What is the 'Track' concept in posterior instability?" - but the glenoid-track framework that underpins all of this is never explained. It is the modern, examinable way to predict whether a humeral-head defect will engage.
The concept (developed for anterior instability): through range of motion the glenoid maintains a contact zone that sweeps across the humeral head - the glenoid track (classically about 83% of the glenoid width). A humeral-head defect is:
- On-track if it stays within that contact zone throughout motion - the rim never drops into the defect, so the shoulder is stable.
- Off-track if the defect extends beyond the medial margin of the track - the glenoid rim falls into the defect and the head dislocates ("engages").
Applying it to the reverse Hill-Sachs (the posterior analogue):
- Anterior (Hill-Sachs)
- Abduction + external rotation
- Posterior (reverse Hill-Sachs)
- Adduction + internal rotation
- Anterior (Hill-Sachs)
- Anterior glenoid
- Posterior (reverse Hill-Sachs)
- Posterior glenoid
- Anterior (Hill-Sachs)
- Defect clears the anterior track and engages
- Posterior (reverse Hill-Sachs)
- Anteromedial defect clears the posterior track and engages
- Anterior (Hill-Sachs)
- Address bone (remplissage/Latarjet) not labrum alone
- Posterior (reverse Hill-Sachs)
- Address bone (remplissage/McLaughlin/graft) not reverse Bankart alone
an off-track (engaging) reverse Hill-Sachs is exactly the lesion in which an isolated soft-tissue (reverse Bankart) repair fails - the bony defect must be filled or bypassed (reverse remplissage, modified McLaughlin, allograft) or the track effectively widened. An on-track small defect can be stabilised by soft-tissue/non-operative means. This is the biomechanical justification for the size-based algorithm and for the "engaging lesion" warning.
the glenoid-track and gamma-angle numbers are extrapolated from anterior instability and are biomechanically plausible but not yet validated in robust posterior cohorts - so use them as a framework, not a hard cut-off. (The fully validated anterior glenoid-track is developed in the Hill-Sachs and glenoid-bone-loss topics.)
Think on-track vs off-track: a reverse Hill-Sachs that stays within the posterior glenoid contact zone is on-track and stable, but one that clears the medial edge of that track in adduction-internal rotation is off-track and engages. An off-track lesion is why reverse Bankart repair alone fails - you must fill or bypass the bone (remplissage, McLaughlin, allograft). The posterior numbers are extrapolated from anterior data, so treat the track as a concept, not a precise threshold.
Classification Systems
Classification by Articular Surface Involvement
Most clinically useful for decision making.
- % of Head
- under 20%
- Stability
- Stable
- Treatment
- Closed Reduction / Neglect
- % of Head
- 20-45%
- Stability
- Unstable
- Treatment
- Reconstruction (McLaughlin)
- % of Head
- over 45-50%
- Stability
- Grossly Unstable
- Treatment
- Arthroplasty
Clinical Assessment
- Mechanism: Seizure, shock, fall on flexed/adducted arm.
- Symptoms: Pain, "locked" shoulder, inability to externally rotate.
- Missed History: Patient treats it as "frozen shoulder" for months.
- Posture: Arm held in adduction and internal rotation (".gunslinger" position).
- Contour: Flattening of anterior shoulder, prominence of coracoid (posterior fullness).
- ROM: Block to External Rotation (pathognomonic for locked posterior dislocation).
Specific Tests for Posterior Instability
- Posterior Drawer Test: Supine. Axial load + posterior force.
- Jerk Test: Seated. Flexion to 90 + Adduction + Axial Load. "Clunk" as head subluxes posteriorly.
- Kim Test: Variation of Jerk test for inferior-posterior, labral pathology.
- Load and Shift: Assess translation grading (Grade I-III).
ALWAYS compare to the contralateral side.
Investigations
Imaging Protocol
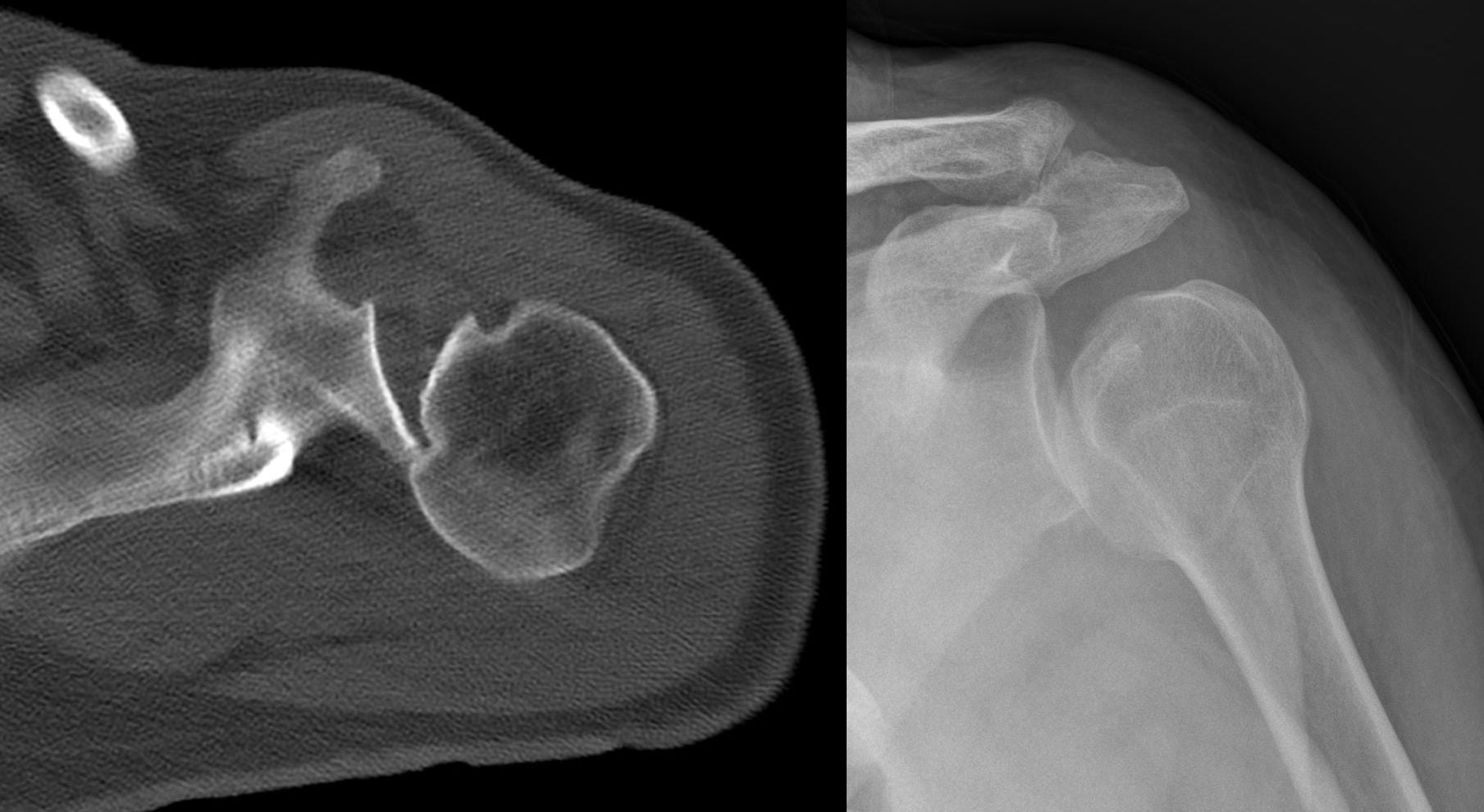
- AP: "Lightbulb sign" (head internally rotated, looks symmetrical). Loss of half-moon overlap.
- Axillary Lateral: GOLD STANDARD. Shows head posterior to glenoid.
- Scapular Y: Head posterior to intersection of Y.
- Mandatory for operative planning.
- Quantify defect size (% of articular surface).
- Assess glenoid bone loss (Reverse Bony Bankart).
- Assess posterior labrum (Reverse Bankart).
- Assess cuff integrity (subscapularis).
- Often done if diagnosis unclear or for chronic pain.
On AP X-ray, the humeral head is fixed in internal rotation. The greater tuberosity rotates anteriorly, making the head look perfectly round (like a lightbulb) rather than its normal walking-stick appearance.
Differential Diagnosis
A patient with a painful, stiff, internally-rotated shoulder after a seizure or fall is easily mislabelled. The differentials below are the classic exam traps.
- Discriminating Feature
- Fixed internal rotation, block to external rotation, lightbulb sign
- Key Investigation
- Axillary lateral / CT
- Pitfall
- Missed as 'frozen shoulder'
- Discriminating Feature
- Global loss of passive AND active ROM, normal joint congruity
- Key Investigation
- Normal radiographs
- Pitfall
- Both block ER, but capsulitis has a congruent joint
- Discriminating Feature
- Discrete fracture lines, crepitus, ecchymosis
- Key Investigation
- AP + axillary; CT for comminution
- Pitfall
- Fracture-dislocation may coexist
- Discriminating Feature
- Arm in abduction/ER, posterolateral head defect
- Key Investigation
- AP + axillary
- Pitfall
- Opposite engaging position (Abd+ER)
- Discriminating Feature
- Recurrent positional subluxation, no impaction defect
- Key Investigation
- MR arthrogram
- Pitfall
- Soft-tissue repair alone fails if a bony defect is present
Management Algorithm

Acute Management
Goal: Reduce and maintain stability.
- Closed Reduction: Under conscious sedation/GA.
- Traction + gentle anterior pressure. Avoid force (fracture risk).
- Assess Stability:
- Stable: Immobilize in External Rotation (gunslinger brace) for 4-6 weeks.
- Unstable: If redislocates or engages in functional ROM to Surgery.
Early reduction minimizes cartilage damage.
SMATreatment Algorithm by Size
Hook:Small, Medium, All-gone (Arthroplasty)
Surgical Technique
The Concept
Transferring the Subscapularis tendon (original McLaughlin) or Lesser Tuberosity (modified) into the defect.
- Effect: Fills the defects and acts as a check-rein preventing internal rotation.
Steps
- Approach: Deltopectoral approach.
- Identify Defect: Locate the anteromedial impression fracture.
- Osteotomy: Lesser tuberosity osteotomy (with subscapularis attached).
- Reduction: Reduce the humeral head into the glenoid.
- Preparation: Prepare the defect bed (curette/burr) to encourage healing.
- Fixation: Secure the lesser tuberosity bone block into the defect using screws or suture anchors.
- Result: The bony plug fills the hole and the subscapularis tightens, preventing internal rotation.
Careful protection of the axillary nerve is required.
Complications
- Risk Factors
- Undersized graft, Missed engaging lesion
- Prevention/Management
- Ensure defect is filled/bypassed
- Risk Factors
- Damage to cartilage, hardware penetration
- Prevention/Management
- Countersink screws, accurate reduction
- Risk Factors
- Poor fixation of osteotomy
- Prevention/Management
- Protect range of motion (ER) post-op
- Risk Factors
- Screw heads prominent
- Prevention/Management
- Use headless screws
Postoperative Care
Rehab Protocol (Modified McLaughlin)
- Sling: Gun-slinger brace (neutral to external rotation).
- Restrictions: NO Internal Rotation (protects subscap transfer).
- ROM: Passive ER allowed.
- Wean sling.
- Active assist ROM.
- Begin gentle Internal Rotation stretching.
- Rotator cuff strengthening.
- Scapular stabilizers.
- Return to sport/work assessment.
Outcomes and Prognosis
Good to Excellent results in 75-85% of patients. Low recurrence rate if sized correctly.
Technical procedure but shows good survival at 10 years. Risk of graft resorption/necrosis.
Associated with poor functional outcomes and rapid progression to OA if left unreduced.
Arthroscopic "Reverse Remplissage" involves filling defect with subscapularis via suture anchors. Good for small/medium defects.
Guidelines, Registries & Global Practice
Posterior dislocation accounts for roughly 2-5% of all shoulder dislocations. Population-based data (Edinburgh cohort) give a prevalence of about 1.1 per 100,000 per year, with peaks in men aged 20-49 and in the elderly; roughly two-thirds are traumatic and most of the remainder seizure-related.
There is no single dedicated guideline; AAOS (US), BOA/BESS (UK), AO Foundation and EFORT teaching converge on the same principles — mandatory axillary/CT imaging, treat by defect size, and prefer joint preservation in young patients.
- Emphasis
- Anatomy of impaction & fixation principles
- Practical Point
- Restore head sphericity; countersunk/headless fixation
- Emphasis
- Avoiding missed diagnosis; specialist referral
- Practical Point
- Three radiographic views mandatory after seizure/electrocution
- Emphasis
- Joint preservation in the young
- Practical Point
- Reconstruct rather than replace where the head is viable
Arthroplasty registries (NJR, AJRR, AOANJRR, Swedish/Norwegian) do not isolate reverse Hill-Sachs as an indication, but they inform implant choice when arthroplasty is required: reverse total shoulder is increasingly preferred over hemiarthroplasty in older patients with cuff compromise or unreconstructable bone loss.
Where CT and allograft banking are available, defect quantification and osteochondral allograft expand head-preserving options. In limited-resource settings, autograft modified McLaughlin (no implant dependency) and rotational osteotomy are favoured, and late presentation of neglected locked dislocations is more common.
Controversies & Areas of Uncertainty
Quoted cut-offs (20%, 25%, 40%, 50%) come from small heterogeneous series, not prospective comparisons. Most authors reconstruct intermediate defects (~25-50%) and reserve arthroplasty for over ~45-50% with head collapse, but the exact threshold for any individual head remains judgement-based.
Arthroscopic transfer / capsular fill techniques are increasingly described for small-to-intermediate engaging lesions, but comparative evidence against open modified McLaughlin is limited to case series. Open transfer remains the most validated approach for larger defects.
Some advocate elevating the impacted articular fragment with subchondral bone grafting to restore native cartilage, versus filling/bypassing the defect (McLaughlin, allograft). No high-level data favour one strategy.
The glenoid-track and "gamma angle" concepts are extrapolated from anterior instability; their predictive value for posterior engagement is biomechanically plausible but not yet validated in robust clinical cohorts.
MCQ Practice Points
Q: What is the most common nerve injury associated with posterior shoulder dislocation? A: While the Axillary nerve is most common in anterior dislocations, checking it is still mandatory. However, posterior dislocations have a lower rate of nerve injury overall compared to anterior.
Q: Which fracture is pathognomonic for a posterior shoulder dislocation? A: A Lesser Tuberosity fracture (avulsion by the subscapularis tendon) is pathognomonic and indicates a posterior dislocation mechanism.
Q: What is the 'Rim Sign' on an AP shoulder X-ray? A: The Rim Sign is a widening of the glenohumeral joint space greater than 6mm on the AP view, indicating posterior displacement of the head.
Q: What is the 'Trough Line Sign'? A: It appears as two parallel lines of dense cortical bone on the AP X-ray, representing the impaction fracture (Reverse Hill-Sachs) of the anteromedial humeral head.
Q: Which muscle group is responsible for posterior dislocation during a seizure? A: The massive internal rotators (Latissimus Dorsi, Pectoralis Major, Subscapularis) overpower the weaker external rotators, driving the head posteriorly.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old male presents with a 'frozen shoulder' for 3 months after a seizure. He cannot externally rotate past neutral. Show me the X-rays you would order and describe the findings.”
“You confirm a locked posterior dislocation. A CT scan shows a Reverse Hill-Sachs lesion involving 35% of the articular surface. The head is viable. How do you manage this?”
“Explain the concept of an 'Engaging' Reverse Hill-Sachs lesion and how it differs from an engaging anterior Hill-Sachs.”
Anatomy
- Impaction of Anteromedial Head
- Engages in Adduction + IR
- Posterior dislocation association
- Subscapularis tendon involvement
Classification (Size)
- Small (under 20%) = Stable
- Medium (20-45%) = Unstable/Recon
- Large (over 45%) = Arthroplasty
- Gamma angle greater than 90 deg = Unstable
Clinical Signs
- Locked in Internal Rotation
- Prominent Coracoid
- Flattened anterior shoulder
- Posterior fullness (humeral head)
Imaging
- Lightbulb Sign (AP)
- Trough Line Sign (Impaction)
- Axillary Lateral = Diagnostic
- Rim Sign: Widened joint space greater than 6mm
Treatment
- Acute less than 3wks + Small = Reduction + Brace
- Chronic/Med = Mod. McLaughlin
- Large/Collapse = Hemi/Total
- Remplissage for small engaging lesions
Complications
- Missed diagnosis (common)
- Recurrent instability
- AVN (late collapse)
- Arthritis
Evidence Base
Locked Posterior Dislocation — the Landmark Series
- Diagnosis had been missed by the initial physician in the majority of cases; mean injury-to-diagnosis interval was 1 year
- Causes: motor-vehicle accident, seizure, alcohol-related injury, or electroshock therapy
- An axillary radiograph confirmed the diagnosis in all 41 shoulders and showed the defect size
- Lesser-tuberosity transfer succeeded in all 4 shoulders treated; subscapularis transfer succeeded in 4 of 9
Defect-Size Treatment Algorithm
- Small impression defects are usually stable after closed reduction
- Intermediate defects (roughly 25-50%) require reconstruction (McLaughlin / bone graft)
- Defects over ~50% with head collapse require prosthetic replacement
- CT quantification of the defect is central to the decision
Epidemiology & Risk of Recurrence
- Prevalence of posterior dislocation 1.1 per 100,000 population per year
- 67% caused by trauma, most of the remainder by seizures
- 17.7% of shoulders developed recurrent instability within the first year
- Age under 40, seizure mechanism, and large reverse Hill-Sachs (over 1.5 cm3) predicted recurrence
Head-Preserving Surgery for Chronic Dislocation
- For chronic posterior dislocation, the two dominant techniques were McLaughlin / modified McLaughlin and bone-graft reconstruction
- Both consistently produced good functional outcomes with few complications
- Chronic anterior dislocation techniques were far more variable with high resubluxation and early arthrosis
- Conservative neglect of chronic dislocation produced poor functional results
Osteochondral Allograft in the Shoulder
- Reverse Hill-Sachs lesions were the single most common indication for shoulder OCA (33 of 83 shoulders)
- 68 of 83 shoulders had favourable outcomes (graft incorporation, pain, function, satisfaction)
- Mean follow-up 45.7 months
- Unfavourable results clustered in concomitant surgery and pain-pump chondrolysis cases
Modified McLaughlin — Functional Outcomes
- Lesser-tuberosity transfer plus artificial bone fixed with lag screws and sutures for 30-40% defects
- Constant-Murley score improved from 46.0 to 85.8 at mean 19.8 months (p=0.001)
- No residual instability and full return to daily activity in all 5 patients
- Reinforces the modified McLaughlin as a reliable joint-preserving option for intermediate defects