Salter-Harris Physeal Fracture Classification
The Salter-Harris classification
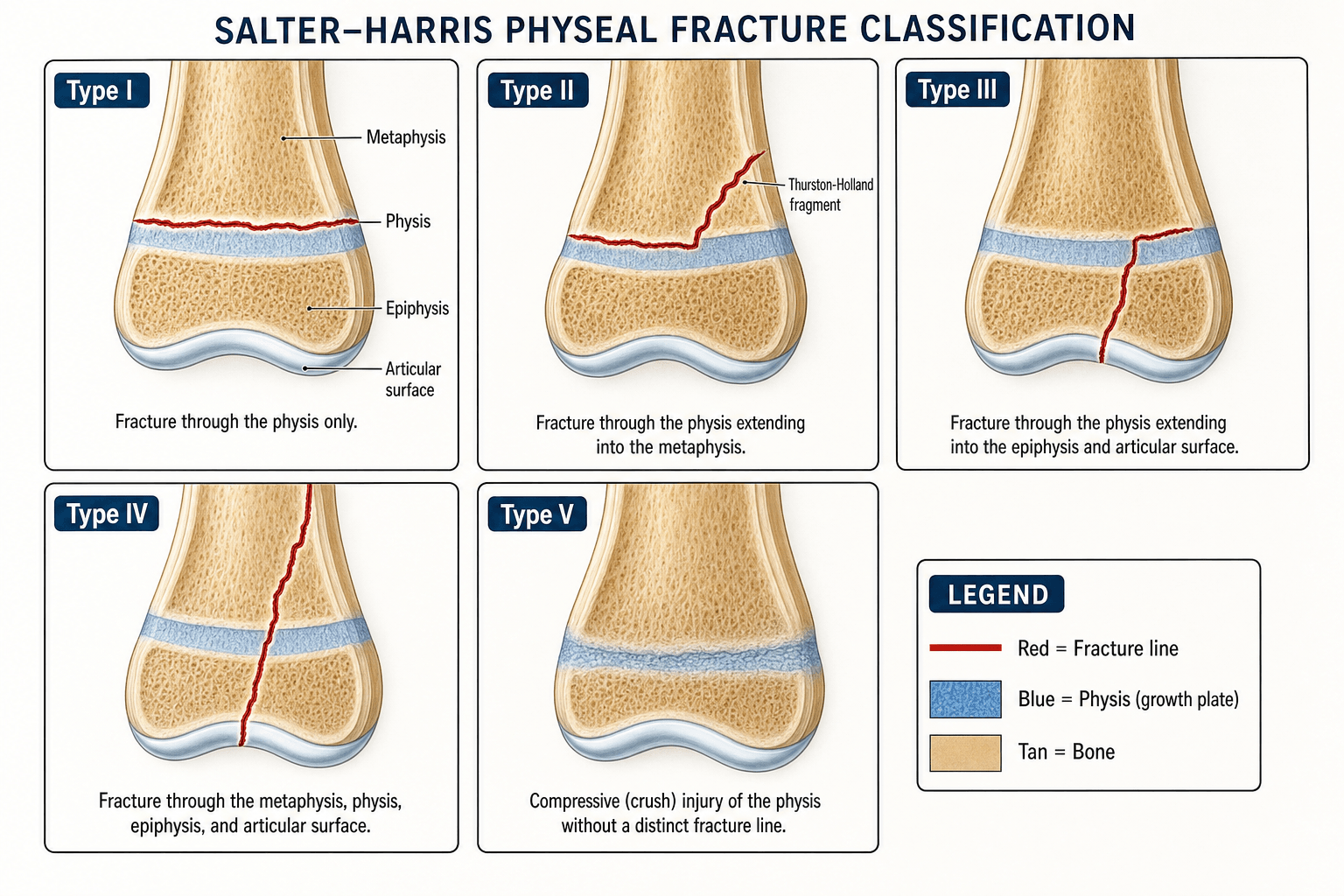
The classification is based on the fracture line's relationship to the physis, epiphysis and metaphysis.
- Fracture path
- Through physis only
- Articular?
- No
- Relative frequency
- ~5–7%
- Growth-arrest risk
- Low
- Fracture path
- Through physis then metaphysis
- Articular?
- No
- Relative frequency
- Commonest (~70–75%)
- Growth-arrest risk
- Low (site-dependent)
- Fracture path
- Through physis then epiphysis
- Articular?
- Yes
- Relative frequency
- ~8–10%
- Growth-arrest risk
- Moderate
- Fracture path
- Through epiphysis, physis and metaphysis
- Articular?
- Yes
- Relative frequency
- ~8–12%
- Growth-arrest risk
- High
- Fracture path
- Crush/compression of physis
- Articular?
- No
- Relative frequency
- Rare (under 1%)
- Growth-arrest risk
- Very high
SALTRSALTR — the five types
Hook:SALTR: Slipped, Above, Lower, Through, Rammed - the letters track where the fracture exits.


In a type II fracture the line exits through the metaphysis, splitting off a triangular metaphyseal corner — the Thurston-Holland fragment — which confirms the type on radiograph. In type III the epiphyseal fragment crosses the articular surface, so the joint may be incongruent and CT is often used for planning. Note that the SALTR letters (Slipped/Above/Lower/Through) describe the direction the fracture exits, which is why "Above" (II) means the metaphyseal side and "Lower" (III) means the epiphyseal side.
The growth plate runs, from the epiphysis to the metaphysis, through the resting (reserve) zone, the proliferative zone (the germinal layer that actually grows the bone, fed by epiphyseal vessels), the hypertrophic zone (cells enlarge and the matrix calcifies - the zone of provisional calcification), and then the metaphyseal primary spongiosa. The hypertrophic zone / zone of provisional calcification is the mechanically weakest layer, so a Salter-Harris fracture characteristically propagates through it - and that is the key to prognosis. In types I and II the cleavage stays in the hypertrophic zone, leaving the proliferative germinal layer and its epiphyseal blood supply intact, so growth usually continues. Types III-IV cross the physis vertically and type V crushes it, damaging the germinal layer and/or its blood supply - which is exactly why the growth-arrest risk climbs with the type number.
Pitfalls & imaging
- Type V is often missed initially. The physis may look normal or only slightly widened; the diagnosis is frequently retrospective when asymmetric growth develops. Suspect it in crush/axial-loading mechanisms.
- MRI detects occult physeal injury and can show acute physeal oedema in a type V when the radiograph is unrevealing.
- CT is preferred for surgical planning in types III and IV — it delineates articular step-off, fragment size and the plane of physeal involvement.
- Growth arrest occurs via physeal bar formation — a bony/fibrous bridge tethering one side, producing angular deformity (partial) or limb-length discrepancy (complete). The distal femoral and distal tibial physes are the highest-stakes lower-limb sites.
- Remaining growth potential changes everything — the same injury is trivial near skeletal maturity but devastating in a young child. Always relate the type to the child's growth remaining.
Management — by type, displacement and site
Management is guided by whether the fracture is intra-articular, the displacement, and the risk of growth arrest (which depends on both the type and the site).
- Reduction
- Closed reduction if displaced
- Fixation
- Rarely needed
- Prognosis
- Excellent — growth disturbance uncommon
- Reduction
- Closed reduction
- Fixation
- Percutaneous K-wires if unstable
- Prognosis
- Generally good — but site-dependent (distal femur worse)
- Reduction
- Open if more than 2 mm displacement
- Fixation
- Internal fixation (screws within the epiphysis, parallel to physis)
- Prognosis
- Good if anatomic reduction achieved
- Reduction
- Open reduction and internal fixation
- Fixation
- Screws in epiphysis and metaphysis, avoiding transphyseal hardware
- Prognosis
- Guarded — significant growth-arrest risk
- Reduction
- N/A — diagnosed retrospectively
- Fixation
- Protected weight-bearing initially
- Prognosis
- Poor — high rate of growth arrest
- 1Classify and assess the jointDetermine the SALTR type and whether it is intra-articular (III/IV). Use CT for articular step-off in types III/IV; consider MRI for an occult or suspected type V.
- 2Reduce — anatomic if intra-articularTypes I/II: gentle closed reduction, accept the constraints of physeal remodelling. Types III/IV: anatomic reduction (usually open) — do not accept more than 2 mm of articular step-off.
- 3Fix without crossing the physisUse smooth K-wires across the physis if unavoidable, but place definitive screws parallel to and within one side of the physis (epiphysis or metaphysis) — transphyseal threaded hardware can itself create a growth bar.
- 4Monitor for growth arrestSerial radiographs for 12–18 months (especially III–V and the distal femur/tibia); watch for Park-Harris lines, physeal bar, angular deformity or limb-length discrepancy, comparing with the other side.
Types III and IV are intra-articular fractures. Accepting more than 2 mm of displacement risks post-traumatic arthritis and growth arrest, so anatomic reduction — usually open — is the standard of care. And do not assume a type II is automatically benign: at the distal femur, growth disturbance occurs in over half of all physeal fractures regardless of type.
A physeal bar is a bony/fibrous bridge tethering part of the plate, causing progressive angular deformity (an eccentric/peripheral bar) or limb-length discrepancy (a central/large bar). First map it - MRI or fine-cut CT (a physeal map) defines the bar's size, location and the growth remaining. Management then hinges on those:
- A small bar (roughly under 50% of the physis) with significant growth remaining (generally at least 2 years or 2 cm) → resection with interposition of a material to stop it reforming (autologous fat, bone cement/PMMA, or Silastic) - the Langenskiöld procedure - to let the rest of the physis resume growth.
- A large bar (over ~50%) or a child near skeletal maturity → resection is futile; instead complete the epiphysiodesis of the remaining physis ± a contralateral epiphysiodesis to equalise leg lengths.
- Established angular deformity → corrective osteotomy; a significant final limb-length discrepancy → lengthening or an appropriately-timed contralateral epiphysiodesis.
This is what makes the 12-18-month surveillance worthwhile - catching a bar early, while it is still small and resectable.
Exam & revision
Everything below condenses the classification for revision and viva practice.
- SALTR: I Slipped (physis), II Above (metaphysis), III Lower (epiphysis), IV Through (all), V Rammed (crush).
- Type II is the commonest; types III/IV are intra-articular and need anatomic (open) reduction.
- Higher type = higher growth-arrest risk — but site matters too (distal femur is the highest-stakes physis).
- Thurston-Holland fragment = type II (metaphyseal corner).
- Fix parallel to the physis — avoid transphyseal threaded hardware.
- Monitor 12–18 months for physeal bar/Park-Harris lines, especially types III–V.
Higher type, higher arrest riskThree exam rules
Hook:Higher type, higher arrest risk; III/IV intra-articular; V is a crush - but site matters too.
Frequently asked questions
What are the five Salter-Harris types?
The SALTR mnemonic maps the fracture path through the physis. Type I (Slipped): through the physis only. Type II (Above): through the physis and out through the metaphysis, leaving a Thurston-Holland fragment. Type III (Lower): through the physis and out through the epiphysis to the joint surface. Type IV (Through): through metaphysis, physis and epiphysis in one line. Type V (Rammed): a crush injury of the physis with no distinct fracture line.
Which Salter-Harris type is commonest, and which has the worst prognosis?
Type II is by far the commonest (about 70-75 percent) and usually benign because the germinal layer stays with the epiphysis. Type V has the worst outlook - physeal crush injures the germinal cells directly, and the injury is often only recognised when growth arrest appears months later. In general, the higher the type number, the higher the risk of growth disturbance.
Why must Salter-Harris types III and IV be reduced anatomically?
Types III and IV are intra-articular: the fracture crosses the epiphysis to the joint surface. A residual step-off both damages the articular surface and lets a bone bridge form across the physis, causing partial growth arrest and angular deformity. Displaced type III and IV fractures therefore need open or percutaneous anatomic reduction and fixation, with less than 2 mm of articular step accepted.
What is the Thurston-Holland fragment?
The Thurston-Holland fragment is the corner of metaphysis that stays attached to the epiphysis in type II (and type IV) injuries - the metaphyseal flake on the compression side of the fracture. It confirms the fracture path, tells you the periosteum is intact on that side (which helps reduction), and is a classic exam identification point.
Which growth plate is the highest-stakes site for physeal injury?
The distal femur. Site matters as much as Salter-Harris type: the distal femoral physis contributes roughly 37 percent of limb length and has an undulating, multiplanar architecture, so even low-type injuries there carry a disproportionate risk of growth arrest and leg-length discrepancy, and all distal femoral physeal injuries need close radiographic follow-up.
Exam viva
Practise clinical reasoning and management decisions out loud
“A 12-year-old boy falls on an outstretched hand and presents with a painful, swollen wrist. Radiographs show a fracture through the distal radial physis with a small metaphyseal spike on the volar side. Classify this fracture and outline your management.”
“A 10-year-old girl sustains a twisting injury to her ankle. CT shows a fracture extending from the medial malleolar articular surface through the epiphysis, across the physis, and into the metaphysis. The articular step-off is 3 mm. Classify the fracture, explain the prognosis, and describe your operative plan.”
Classification (SALTR)
- Type I: through physis only (Slipped) — rare, good prognosis
- Type II: through physis and metaphysis (Above) — commonest, Thurston-Holland fragment
- Type III: through physis and epiphysis (Lower) — intra-articular, anatomic reduction
- Type IV: through epiphysis, physis and metaphysis (Through) — intra-articular, high risk
- Type V: crush of physis (Rammed) — rarest, worst prognosis, often retrospective
Management principles
- Types I/II: closed reduction; fix only if unstable
- Types III/IV: open reduction + internal fixation for more than 2 mm displacement
- Type V: protected weight-bearing; monitor for growth arrest
- Fixation parallel to the physis — avoid transphyseal threaded hardware
High-yield exam points
- Higher type number = higher growth-arrest risk — but SITE matters too
- Thurston-Holland fragment = type II
- Distal femur = highest-stakes physis (growth disturbance in over half of fractures)
- Monitor at least 12–18 months with serial radiographs after any physeal fracture
Evidence
Distribution of physeal and nonphyseal fractures in 2,650 long-bone fractures in children aged 0-16 years
- Of 2,650 long-bone fractures in children (humerus, radius, ulna, femur, tibia, fibula), growth-plate injuries accounted for 30%.
- Nonphyseal fractures occurred twice as often in the upper extremity as in the lower extremity.
- Girls with physeal fractures were on average 1.5 years younger than boys with the same fracture type and location (reflecting earlier skeletal maturation).
Physeal fractures: Part 1. Epidemiology in Olmsted County, Minnesota, 1979-1988
- Population-based study: 850 children sustained 951 physeal fractures (male:female 2:1; overall incidence 279 per 100,000 person-years).
- The most common site was the phalanges of the fingers (37%); Salter-Harris type II was the most common type (54%).
- 16% of fractures did not fit the Salter-Harris scheme, prompting Peterson to add two new types and propose a revised classification (Parts 2 and 3).
According to PubMed, the frequency of physeal injuries among childhood fractures comes from Mann & Rajmaira 1990 (DOI) and Mizuta et al. 1987 (DOI), whose key message is that prognosis depends more on site than Salter-Harris type; the population epidemiology and the origin of the Peterson modification from Peterson et al. 1994 (DOI); the distal-femoral growth-disturbance rates from Basener et al. 2009 (DOI); and the residual-physeal-gap predictor for distal tibial fractures from Barmada et al. 2003 (DOI). The widely-quoted "~75% are type II" figure comes from the broader literature; Peterson's population study reported 54% (with 16% unclassifiable).