Retrograde Blood Supply | High Nonunion Risk | Anatomic Snuffbox Tenderness
- Retrograde blood supply - enters distally, proximal pole at risk
- Waist fractures are most common (70%) and highest AVN risk
- Proximal pole fractures have highest nonunion and AVN rates
- Anatomic snuffbox tenderness is key clinical finding
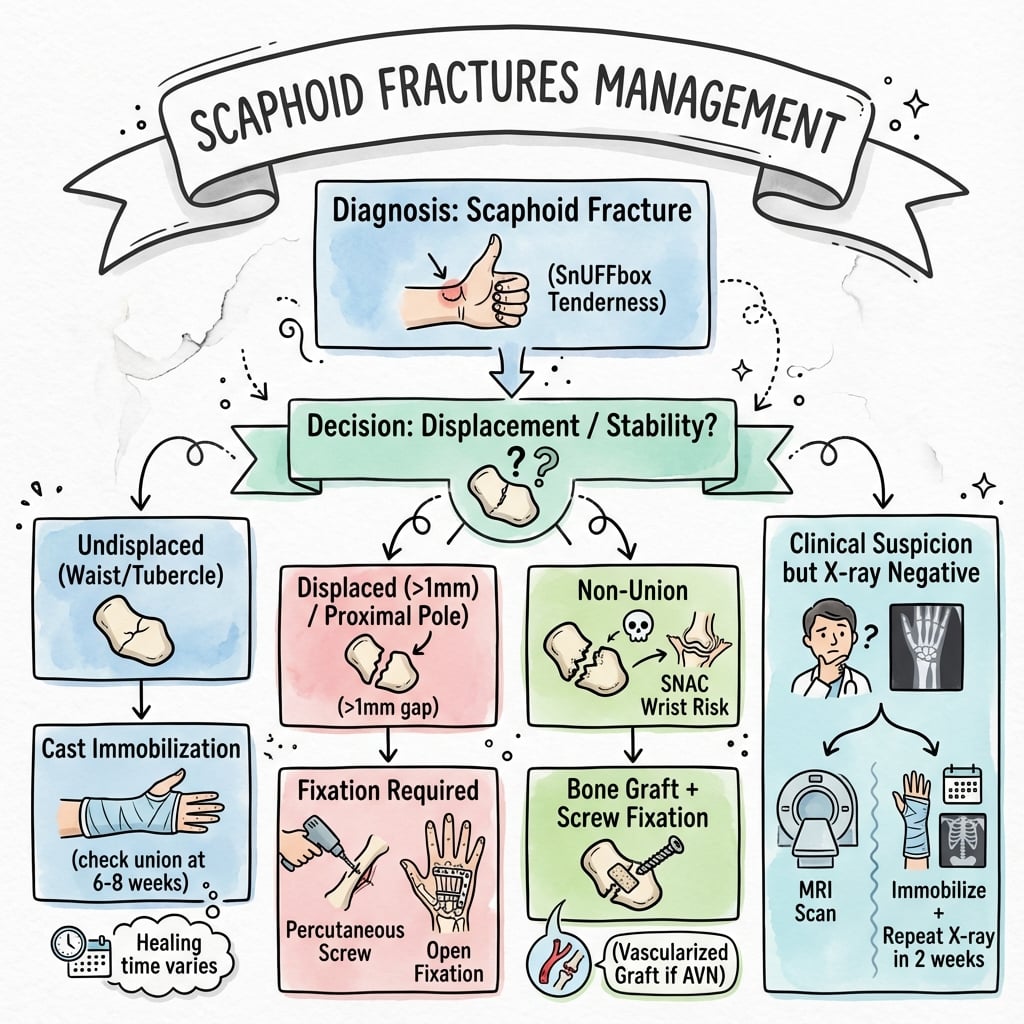
- If suspected but X-ray negative - treat as fracture or get MRI
- “Blood supply via dorsal carpal branch of radial artery - enters distally
- “Proximal pole has no direct blood supply - depends on intraosseous flow
- “Displacement over 1mm, angulation over 15°, or comminution = unstable = surgery
- “Herbert screw allows early motion without cast
Retrograde blood supply via dorsal carpal branch of radial artery. Blood enters at the distal pole, flows proximally. Proximal pole fractures have highest AVN risk because they are distal to the blood entry.
10-20% of scaphoid fractures not visible on initial X-ray. If clinical suspicion high (snuffbox tenderness), either treat as fracture with cast/splint or MRI (most sensitive) to confirm. Don't dismiss.
Proximal pole location, displacement greater than 1mm, delay in treatment greater than 4 weeks, smoking, and comminution increase nonunion risk. These factors guide operative vs conservative decision.
Type A (stable) = cast. Type B (unstable) = surgery recommended. Type C (delayed) and Type D (nonunion) = surgery required. Know the subtypes.
- Key Finding
- Extra-articular, very stable
- Treatment
- Splint 4-6 weeks, excellent prognosis
- Key Finding
- Stable incomplete fracture
- Treatment
- Scaphoid cast 8-12 weeks or consider screw
- Key Finding
- Unstable distal fracture
- Treatment
- Operative fixation recommended
- Key Finding
- Displaced greater than 1mm
- Treatment
- Operative fixation recommended
- Key Finding
- High AVN and nonunion risk
- Treatment
- Operative fixation strongly recommended
- Key Finding
- Complex carpal injury
- Treatment
- Urgent operative fixation
- Key Finding
- Failed to heal, often with AVN
- Treatment
- Surgery with bone graft +/- vascularized graft
SCAPHOIDSCAPHOID - Key Features
Hook:SCAPHOID fractures need careful assessment and often surgery
Overview and Epidemiology
Scaphoid fractures are the most common carpal fracture and the second most common wrist fracture (after distal radius). They are critical to diagnose and treat appropriately due to the high risk of nonunion and avascular necrosis.
Mechanism of injury:
- Fall on outstretched hand (FOOSH) - most common
- Wrist in dorsiflexion and radial deviation
- Axial load through thenar eminence
- Compresses scaphoid between radius and capitate
- Sports injuries - common in young males
- Motor vehicle accidents
The typical scaphoid fracture patient is a young male (15-30 years) with a FOOSH injury playing sports or from a fall. This demographic has highest incidence. Be suspicious in any young person with wrist pain after fall.
Location distribution:
- Waist fractures: 70% (most common, highest absolute numbers of nonunion)
- Proximal pole: 20% (highest percentage nonunion and AVN)
- Distal pole/tubercle: 10% (excellent prognosis)
Anatomy and Blood Supply
- Boat-shaped carpal bone (Greek: skaphe = boat)
- Links proximal and distal carpal rows
- 80% covered by articular cartilage - limits blood entry points
- Oblique orientation in coronal and sagittal planes
- Tubercle palpable palmarly
- Proximal: articulates with radius (scaphoid fossa)
- Distal: articulates with trapezium and trapezoid
- Medial: articulates with lunate and capitate
- Forms floor of anatomic snuffbox
The scaphoid has retrograde blood supply. The dorsal carpal branch of the radial artery provides 70-80% of blood supply via dorsal ridge. Blood enters distally and flows proximally. The proximal pole has no direct blood supply - entirely dependent on intraosseous flow.
- 70-80%: Dorsal carpal branch - enters at dorsal ridge (waist level)
- 20-30%: Palmar branch - enters at tubercle and distal pole
- Proximal pole: No direct blood supply, relies on intraosseous vessels
- This explains why proximal pole fractures have highest AVN risk
- Waist fractures interrupt blood flow to proximal pole
- More proximal fractures = higher AVN risk
- Displaced fractures disrupt intraosseous vessels
- May take longer to heal than other carpal fractures
RETROGRADERETROGRADE - Blood Supply Pattern
Hook:Blood flows RETROGRADE - enters distal, travels to proximal pole
Classification Systems
Herbert Classification (most commonly used)
- Subtype
- Description
- Stable acute fractures
- Subtype
- A1
- Description
- Fracture of tubercle
- Subtype
- A2
- Description
- Incomplete fracture through waist
- Subtype
- Description
- Unstable acute fractures
- Subtype
- B1
- Description
- Distal oblique fracture
- Subtype
- B2
- Description
- Complete fracture of waist
- Subtype
- B3
- Description
- Proximal pole fracture
- Subtype
- B4
- Description
- Trans-scaphoid perilunate dislocation
- Subtype
- B5
- Description
- Comminuted fractures
- Subtype
- Description
- Delayed union
- Subtype
- Description
- Established nonunion
- Subtype
- D1
- Description
- Fibrous nonunion
- Subtype
- D2
- Description
- Pseudarthrosis
Type A = stable = conservative treatment reasonable. Type B = unstable = operative treatment recommended. Type B criteria: displaced, proximal pole, oblique, or with perilunate dislocation.
HERBERTHERBERT - Classification
Hook:HERBERT classification: A = stable, B = unstable, C = delayed, D = nonunion
Clinical Presentation and Assessment
History:
- Mechanism (FOOSH typical)
- Time since injury
- Hand dominance
- Occupation (manual worker implications)
- Smoking status (affects healing)
- Previous wrist injury
Physical examination:
- Test
- Palpate between EPL and EPB/APL
- Significance
- Classic sign, 90% sensitive
- Test
- Palpate palmarly at wrist crease
- Significance
- Equally sensitive, more specific
- Test
- Compress thumb metacarpal
- Significance
- Scaphoid compression test
- Test
- Watson test component
- Significance
- Suggests scaphoid involvement
- Test
- Compare to contralateral
- Significance
- May indicate fracture
- Test
- Observe/palpate
- Significance
- Less obvious than other wrist fractures
Key clinical points:
Anatomic snuffbox tenderness has high sensitivity (~90%) but low specificity. Scaphoid tubercle tenderness is equally sensitive and more specific. If both present with appropriate mechanism, treat as scaphoid fracture even if X-ray is negative.
Watson's test (for scaphoid instability):
- Pressure on scaphoid tubercle while moving wrist from ulnar to radial deviation
- Clunk or pain = positive
- Indicates scapholunate ligament injury or instability
Differential diagnosis of radial-sided wrist pain after a fall:
- Discriminating features
- Snuffbox AND tubercle tenderness, pain on axial thumb compression, FOOSH
- Key investigation
- Scaphoid-series radiographs; MRI if occult
- Discriminating features
- More diffuse swelling, dorsal/volar deformity, tenderness over distal radius not snuffbox
- Key investigation
- PA and lateral wrist radiographs
- Discriminating features
- Dorsal SL-interval tenderness, positive Watson test/clunk, SL gap on clenched-fist view
- Key investigation
- Stress/clenched-fist radiographs, MRI or arthroscopy
- Discriminating features
- Tenderness localised away from the scaphoid; dorsal triquetral flake on lateral view
- Key investigation
- Oblique/lateral radiographs, CT
- Discriminating features
- Pain at thumb base with grind test, distal to snuffbox
- Key investigation
- Thumb radiographs
- Discriminating features
- Subacute onset, no acute trauma, positive Finkelstein test, tenderness over first dorsal compartment
- Key investigation
- Clinical; ultrasound if uncertain
- Discriminating features
- Tenderness not localising to scaphoid or SL interval, normal advanced imaging
- Key investigation
- MRI to exclude occult fracture before labelling
A classic viva/ISAWE trap is the two-piece scaphoid on a film of a tender wrist: is it an acute fracture, an old nonunion, or a (rare, debated) congenital bipartite scaphoid? Calling a variant a fracture - or, worse, missing a real nonunion - both cause harm, so know the discriminators:
- Features favouring a true normal variant (bipartite): it is usually bilateral and symmetrical; the two fragments are roughly equal in size with smooth, well-corticated, rounded margins and no intervening lucent fracture line; there is no surrounding sclerosis, cyst formation or marrow oedema; and the patient is typically asymptomatic (the finding is incidental).
- Features favouring a fracture/nonunion (the far commoner reality): a sharp or irregular non-corticated line, unequal fragments, sclerosis/cysts/resorption at the margins, marrow oedema on MRI, a history of trauma and focal tenderness.
- The key caution: most apparent "bipartite scaphoids" are actually old ununited fractures - a genuinely congenital bipartite scaphoid is rare and even disputed. If there is any doubt (especially with symptoms or unilateral findings), treat it as a fracture/nonunion: get the contralateral wrist for comparison and an MRI (oedema, vascularity) or CT before labelling it a variant.
Exam point: bilateral, symmetric, smoothly corticated equal halves with no oedema in an asymptomatic wrist suggest a bipartite normal variant; anything unilateral, sclerotic, irregular, oedematous or tender is a fracture or nonunion until proven otherwise.
Investigations
Radiographic assessment:
Standard scaphoid series (4 views):
- PA in ulnar deviation - elongates scaphoid
- Lateral - assess angulation, DISI
- 45° semi-pronated oblique - scaphoid profile
- AP with clenched fist - shows displacement

10-20% of scaphoid fractures are NOT visible on initial X-ray. If clinical suspicion is high (snuffbox tenderness, appropriate mechanism), either treat as fracture or obtain MRI for definitive diagnosis. Do not dismiss based on normal X-ray alone.
- Sensitivity 100%, Specificity 99% for fractures
- Shows bone marrow edema before visible fracture line
- Detects associated soft tissue injuries
- Can assess vascularity (gadolinium enhancement)
- Best for fracture characterization
- Shows displacement and angulation precisely
- Assess healing (union vs nonunion)
- Surgical planning for complex fractures
- High sensitivity, low specificity
- Positive within 72 hours (earlier than X-ray changes)
- Less used now with MRI availability
- Clinical suspicion + negative X-ray
- Options:
- Treat as fracture: Cast, repeat X-ray 10-14 days (bone resorption shows fracture)
- MRI: Immediate definitive diagnosis (cost-effective if high clinical suspicion)
- CT: If fracture confirmed, characterize for treatment planning
The topic describes the humpback (flexion collapse) deformity qualitatively, but a complete answer measures it on the sagittal CT reformatted along the scaphoid's long axis, because these numbers decide whether a malunion/nonunion needs a corrective opening-wedge osteotomy rather than simple in-situ grafting:
- Lateral intrascaphoid angle (LISA): the angle between the proximal and distal articular surfaces. Normal is roughly thirty to forty degrees; an angle over about forty-five degrees indicates significant flexion (humpback) collapse.
- Dorsal cortical angle: measured along the dorsal cortex; normal is around 140 degrees, with a smaller (more acute) angle as the scaphoid flexes - a more reproducible measure than the LISA, which has high inter-observer variability.
- Height-to-length ratio: scaphoid height divided by length; a ratio over about 0.65 signals loss of length with dorsal collapse.
- Carpal alignment: a flexed (foreshortened) scaphoid drags the lunate into extension - a DISI pattern (radiolunate angle over about fifteen degrees, scapholunate angle over about sixty degrees) - which is the carpal consequence of the humpback.
Exam point: a flexed scaphoid with a LISA over forty-five degrees / height-to-length ratio over 0.65 / DISI malalignment is a true humpback deformity that needs length and alignment restored with a volar opening-wedge (Fisk-Fernandez) graft, not just a simple inlay graft.





Management
Conservative management indications:
- Herbert Type A fractures (tubercle, non-displaced waist)
- Non-displaced, stable fractures
- Patient preference (understanding risks)
- Medical contraindications to surgery
- Scaphoid (thumb spica) cast
- Thumb IP joint free
- Wrist in slight flexion and radial deviation
- Controversy: above vs below elbow (evidence mixed)
- Duration: 8-12 weeks minimum
- X-ray at 6 weeks
- If healing: continue cast to 8-12 weeks
- If not healed: CT to assess, consider surgery
- Prolonged immobilization for proximal fractures (up to 20 weeks)
The position and extent of casting is debated. Evidence is mixed on above vs below elbow and thumb position. Key principles: stable fractures can heal in cast, but 8-12 weeks minimum and regular follow-up are essential.
Surgical Technique
Headless Compression Screw (Herbert Screw)
- Gold standard for acute fractures
- Variable pitch provides compression
- Buried entirely within bone
- Allows early motion without cast
- Volar approach (preferred for most)
- Access through thenar muscles
- Good for waist and distal fractures
- Screw placed perpendicular to fracture
- Dorsal approach (for proximal pole)
- Access between 3rd and 4th compartments
- Better for proximal pole fractures
- Screw enters at central axis
- K-wires (temporary or adjunct)
- Mini-fragment screws (rarely now)
The ideal screw position is along the central axis of the scaphoid, perpendicular to the fracture. This provides best compression and lowest risk of screw cutout. Fluoroscopy or navigation helps achieve this.
PANDAPANDA - Surgical Indications
Hook:Think of a PANDA - these fractures need surgery to avoid becoming extinct (nonunion)!
Complications
- Incidence
- 5-15% (higher proximal)
- Management
- Surgery with bone graft
- Incidence
- 13-50% proximal pole
- Management
- Vascularized bone graft
- Incidence
- Variable
- Management
- Corrective osteotomy if symptomatic
- Incidence
- Progressive with nonunion
- Management
- Salvage procedures
- Incidence
- 10-20%
- Management
- Physiotherapy, rarely surgical
- Incidence
- Variable
- Management
- Screw removal
- Incidence
- Common
- Management
- High index of suspicion, MRI
Nonunion is the most important complication to avoid.
- Most common significant complication after scaphoid fracture
- Highest risk with proximal pole fractures, displacement, delayed diagnosis and smoking
- Persistent nonunion allows progressive carpal collapse and later arthritis
- Treatment is fracture-site preparation, deformity correction, bone grafting and stable fixation
- Use a vascularized graft when proximal pole vascularity is poor

Postoperative Care and Rehabilitation
Post-operative protocol:
- Bulky dressing and thumb spica splint
- Elevation
- Finger motion immediately
- Wound check at 10-14 days
- Convert to removable thumb spica splint
- Begin gentle wrist ROM
- Active finger motion
- May remove splint for exercises
- X-ray/CT to assess healing
- If united: progressive ROM and strengthening
- If not united: continue protection
- Wean from splint as comfort allows
- Full activity after confirmed union
- Grip strengthening
- Return to sport/work
- Final outcome assessment
Key rehabilitation principles:
- Early finger motion is critical
- Wrist motion after initial healing (2-4 weeks for operative)
- Confirm union before loading
- Grip strength returns over 6-12 months
A key advantage of operative fixation with a Herbert screw is the ability to begin early motion without prolonged casting. This is particularly valuable for athletes and manual workers who cannot tolerate 8-12 weeks in cast.
Outcomes and Prognosis
Outcomes by fracture type:
- Conservative Union
- Over 95%
- Operative Union
- N/A
- Notes
- Excellent prognosis
- Conservative Union
- 90-95%
- Operative Union
- 95%+
- Notes
- Cast reasonable
- Conservative Union
- 60-70%
- Operative Union
- 90-95%
- Notes
- Surgery recommended
- Conservative Union
- 60-70%
- Operative Union
- 85-90%
- Notes
- Surgery strongly recommended
Prognostic factors:
- Fracture location (proximal worse)
- Displacement (over 1mm = worse)
- Time to treatment (delay = worse)
- AVN present (much worse)
- Smoking (significant negative impact)
Delay in diagnosis/treatment over 4 weeks significantly increases nonunion risk. This is why treating suspected fractures (clinical signs, negative X-ray) is important. The mantra: "If in doubt, treat as a scaphoid fracture."
Guidelines, Registries & Global Practice
Global Epidemiology
Scaphoid fractures are the most common carpal fracture, occurring predominantly in young, active males. In a large UK regional study the annual incidence was 12.4 per 100,000, with the highest rate in males aged 15-19 years; 64% were at the waist and 18% at the tubercle, and incidence was higher in more socially deprived groups and peaked in summer (Garala et al., Bone Joint J 2016 — DOI). The classic mechanism is a fall on the outstretched hand; sport and manual occupations dominate the risk profile, though low-energy injuries are increasingly recognised in older adults. The true prevalence among clinically suspected fractures is low — roughly 16% in consecutive suspected presentations, which is why over-treatment of the radiograph-negative wrist is a recognised problem (Jenkins et al., Injury 2008 — DOI).
Guidance & Evidence by Region
- Region
- UK / international
- Key recommendation
- Minimally displaced waist fractures (2mm or less): initial below-elbow cast, fix only confirmed nonunions
- Evidence basis
- Level I RCT (DOI)
- Region
- USA
- Key recommendation
- Displaced (over 1mm), proximal pole, unstable patterns: operative fixation; non-displaced waist: cast or fixation by shared decision
- Evidence basis
- Expert consensus + RCT/meta-analysis
- Region
- UK
- Key recommendation
- Clinical exam + dedicated scaphoid views; if radiograph-negative with ongoing suspicion, immobilise and re-image or proceed to MRI/CT rather than discharge
- Evidence basis
- Standard of care / diagnostic pathway
- Region
- International
- Key recommendation
- Central-axis headless compression screw; reserve volar approach for waist/distal and dorsal approach for proximal pole
- Evidence basis
- Technical consensus
- Region
- Europe
- Key recommendation
- Concur with cast-first for minimally displaced waist; advanced imaging for occult fractures
- Evidence basis
- Aligned with SWIFFT
Cost-effectiveness modelling supports immediate MRI or CT over empiric casting plus repeat radiographs for the occult fracture, as advanced imaging was the dominant strategy on both cost and outcome (Karl, Swart, Strauch, JBJS Am 2015 — DOI).
Global Practice Variation
- Casting configuration: No RCT evidence favours above- versus below-elbow casting or thumb inclusion (Doornberg, Buijze et al., J Trauma 2011 — DOI); below-elbow casting excluding the thumb is increasingly standard, though practice remains heterogeneous.
- Surgery vs cast for minimally displaced fractures: Rates of early fixation rose internationally before SWIFFT; the trial has shifted high-resource practice back toward cast-first with selective fixation, but operative thresholds still vary by surgeon and patient (athlete, manual worker) preference.
- Imaging access: In high-resource settings MRI/CT is used early for occult fractures; in limited-resource or remote settings empiric thumb-spica immobilisation with delayed re-imaging at 10-14 days remains common and acceptable.
- Reconstruction: Vascularised bone grafting and salvage procedures are typically concentrated in specialist hand units worldwide.
Registry Note
There is no dedicated international scaphoid-fracture registry; population-level epidemiology derives from national administrative and regional datasets (e.g. UK and German fracture surveillance), which consistently show the young-male predominance and waist-fracture majority described above.
Be ready to discuss retrograde blood supply anatomy, the Herbert classification, the algorithm for the radiograph-negative but clinically suspected fracture, the SWIFFT message (cast-first for minimally displaced waist fractures), and nonunion treatment (vascularised vs non-vascularised graft indications). Smoking cessation materially improves union and should be addressed in every counselling answer. Medicolegal aspects of the missed scaphoid fracture are examined across boards.
MCQ Practice Points
Q: What is the blood supply pattern of the scaphoid? A: Retrograde - the dorsal carpal branch of the radial artery enters at the distal pole (dorsal ridge) and blood flows proximally. The proximal pole has no direct blood supply - it relies entirely on intraosseous vessels. This is why proximal pole fractures have highest AVN risk.
Q: In Herbert classification, what defines a Type B fracture? A: Unstable acute fractures. Subtypes: B1 (distal oblique), B2 (displaced waist), B3 (proximal pole), B4 (trans-scaphoid perilunate), B5 (comminuted). Type B fractures generally require operative fixation.
Q: What is the best investigation for a clinically suspected scaphoid fracture with negative X-rays? A: MRI - sensitivity and specificity approaching 100%. It shows bone marrow edema before fracture line is visible on X-ray and can identify alternative diagnoses. CT is better for characterizing known fractures.
Q: Which scaphoid fracture location has the highest nonunion and AVN rate? A: Proximal pole - due to the retrograde blood supply, the proximal pole is entirely dependent on intraosseous vessels. Fractures here interrupt this flow, leading to highest rates of nonunion (up to 30-40%) and AVN (up to 50%).
Q: What is the indication for vascularized bone graft in scaphoid nonunion? A: Avascular necrosis of the proximal pole. Standard non-vascularized bone graft has high failure rate when the proximal pole is avascular. Vascularized grafts (1,2 ICSRA or medial femoral condyle) bring new blood supply to the dead bone.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old man falls playing football, landing on his outstretched hand. He has anatomic snuffbox tenderness and scaphoid tubercle tenderness. X-rays are normal. How do you manage this patient?”
“A 28-year-old mechanic presents 2 days after a fall. X-rays show a displaced scaphoid waist fracture with 2mm displacement and carpal instability (DISI pattern). How do you manage this?”
“A 35-year-old presents with chronic wrist pain. He recalls an injury 2 years ago that was never treated. X-rays show scaphoid nonunion with humpback deformity and sclerosis of the proximal pole. How do you assess and manage this patient?”
BLOOD SUPPLY
- Retrograde - enters distally, flows proximally
- Dorsal carpal branch of radial artery
- Enters at dorsal ridge (waist level)
- Proximal pole has NO direct blood supply
HERBERT CLASSIFICATION
- Type A: Stable (A1=tubercle, A2=non-displaced waist)
- Type B: Unstable (B1-B5, see subtypes)
- Type C: Delayed union
- Type D: Established nonunion
OPERATIVE INDICATIONS
- Displacement greater than 1mm
- Proximal pole fractures
- Associated carpal instability
- Nonunion
- Relative: athlete, manual worker, patient choice
X-RAY NEGATIVE MANAGEMENT
- 10-20% not visible initially
- Option 1: Treat as fracture, repeat X-ray 10-14 days
- Option 2: MRI (gold standard, 100% sensitive)
- Never dismiss with clinical findings
NONUNION TREATMENT
- Assess proximal pole vascularity (MRI + gadolinium)
- Viable: non-vascularized bone graft (Fisk-Fernandez)
- AVN: vascularized bone graft (1,2 ICSRA, MFC)
- SNAC wrist: salvage procedures
KEY NUMBERS
- 70% waist fractures (most common)
- 20% proximal pole (highest AVN risk)
- 10-20% X-ray negative initially
- 5-15% nonunion rate overall
- greater than 1mm displacement = surgery
Evidence Base
- Pragmatic multicentre RCT (31 UK hospitals, 439 adults) comparing early surgical fixation versus below-elbow cast (with immediate fixation if nonunion confirmed) for bicortical scaphoid waist fractures displaced by 2mm or less.
- No significant difference in patient-rated wrist evaluation (PRWE) at 52 weeks: surgery 11.9 vs cast 14.0 (adjusted difference -2.1, 95% CI -5.8 to 1.6, p=0.27).
- Serious surgical complications occurred in 14% of the surgery group versus 1% of the cast group; cast-related complications were higher in the cast group (18% vs 2%).
- Introduced the double-threaded (variable-pitch) headless compression screw and the eponymous classification of scaphoid fractures (Types A-D).
- Prospective series of 158 operations (1977-1981): union rate 100% for acute fractures and 83% overall, with most patients returning to work within a few weeks and a plaster cast rarely required.
- Meta-analysis of four RCTs (523 patients) comparing cast variables (above- vs below-elbow, thumb inclusion, wrist position).
- No significant difference in union rate, pain, grip strength, time to union or osteonecrosis between any nonoperative casting method.
- Cadaveric injection study (15 specimens) defining scaphoid vascular anatomy.
- 70-80% of intraosseous blood supply and the entire proximal pole derive from radial artery branches entering through the dorsal ridge; 20-30% (distal tuberosity) from volar radial branches.
- The volar operative approach was shown to be least traumatic to the proximal pole's blood supply.
- Decision-analysis model comparing empiric cast immobilisation, immediate CT, and immediate MRI for suspected occult scaphoid fracture with negative radiographs.
- Advanced imaging (CT or MRI) was dominant — lower overall cost and better projected outcomes than empiric casting; MRI was marginally more cost-effective than CT but sensitive to local test performance and cost.
- Empiric casting would only become cost-effective if advanced imaging cost exceeded $2000 or sensitivity fell below 25-32%.
- Retrospective regional study of 415 confirmed scaphoid fractures: annual incidence 12.4 per 100,000, with the highest rate in males aged 15-19 years (365 of 415 fractures occurred in males).
- Waist fractures accounted for 64% and tubercle fractures for 18.1% of cases; incidence was higher in the most socially deprived groups and peaked seasonally in June.