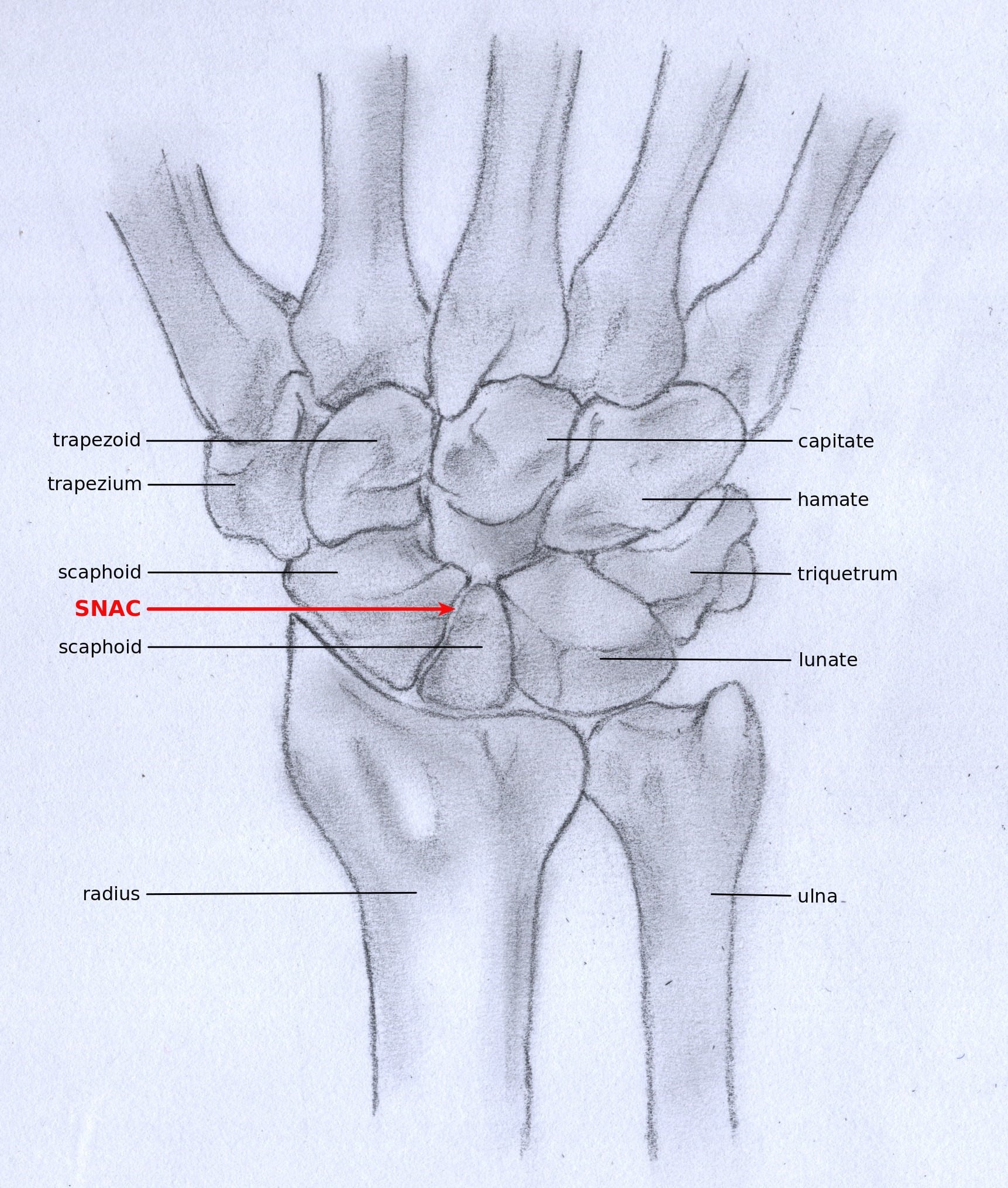
Progressive Carpal Arthritis | Watson Staging | SE4CF vs PRC
- SNAC follows a time-dependent, predictable pattern - styloid/scaphoid-confined first (mean ~8 yrs), then radioscaphoid (~17 yrs), then generalised/capitolunate (~32 yrs) per Mack 1984
- Radiolunate joint is spared - preserved spherical articulation allows motion-sparing procedures
- SE4CF and PRC are the two main surgical options for Stage II/III
- PRC contraindicated in Stage III - capitate head must be pristine for PRC
- DISI deformity develops - dorsal intercalated segment instability from scaphoid nonunion
- “Watson staging mirrors SLAC staging - both spare radiolunate joint
- “SNAC from nonunion vs SLAC from ligament injury - same treatment principles
- “Capitate head cartilage is the key decision point for PRC vs SE4CF
- “Motion preservation surgery is possible because radiolunate joint is spared
SNAC (Scaphoid Nonunion Advanced Collapse) and SLAC (Scapholunate Advanced Collapse) follow the same degenerative pattern but have different causes. SNAC results from scaphoid nonunion; SLAC from scapholunate ligament injury. Treatment principles are identical - both spare the radiolunate joint.
The radiolunate articulation is ALWAYS spared in both SNAC and SLAC. This is because the spherical lunate-radius articulation does not experience the abnormal contact stresses that occur at the radioscaphoid and capitolunate joints after carpal kinematics are disrupted.
Proximal Row Carpectomy (PRC) is CONTRAINDICATED in Stage III SNAC/SLAC. PRC requires an intact capitate head articulating with the lunate fossa of the radius. Stage III has capitolunate arthritis meaning damaged capitate cartilage.
Scaphoid nonunion leads to DISI (Dorsal Intercalated Segment Instability). Without scaphoid linkage, the lunate tilts dorsally. Look for increased scapholunate angle greater than 70 degrees and increased capitolunate angle greater than 30 degrees on lateral radiograph.
- Details
- Progressive wrist arthritis from untreated scaphoid nonunion
- Details
- Scaphoid fracture nonunion → carpal malalignment → arthritis
- Details
- Most displaced/unstable nonunions arthritic beyond 10 years (Mack 1984)
- Details
- Watson: I (styloid), II (radioscaphoid), III (capitolunate)
- Details
- Radiolunate joint ALWAYS spared
- Details
- PRC or SE4CF (capitate status decides)
- Details
- SE4CF only (PRC contraindicated - damaged capitate)
- Details
- 85-90% pain relief, 40-60 degrees motion arc
PRC vs SE4CFMOTION OPTIONS - Salvage Procedures
Hook:PRC needs perfect Capitate; SE4CF works even in Stage III!
DISI LADDISI PATTERN - Radiographic Signs
Hook:DISI = Dorsal lunate tilt, increased SL angle on lateral radiograph
Overview and Epidemiology
- Scaphoid fractures are the most common carpal fracture, occurring predominantly in young adult males
- Up to a third of confirmed scaphoid fractures are radiographically occult on initial films (Burns/Duckworth, Edinburgh prospective series, PMID 23960052)
- Nonunion develops in roughly 5-10% of scaphoid fractures overall; proximal pole and displaced fractures carry the highest risk
- Mack 1984 (PMID 6707028) showed that few displaced or unstable nonunions remain free of arthritis beyond 10 years (the classic "untreated nonunion becomes arthritic" teaching)
- Male predominance, peak incidence in the second-to-fourth decades
- Proximal pole fracture location
- Delayed presentation (greater than 4 weeks)
- Displacement greater than 1mm
- Vertical oblique fracture pattern
- Smoking
- Non-compliance with immobilization
- Established nonunion with instability
- Heavy manual labor
- Recurrent trauma
- Delay in nonunion treatment
Anatomy and Pathophysiology
The scaphoid has a retrograde blood supply entering through the dorsal ridge. Fractures of the proximal pole or waist disrupt blood flow to the proximal fragment, leading to:
- Avascular necrosis of proximal pole
- Delayed or nonunion
- Progressive collapse if untreated
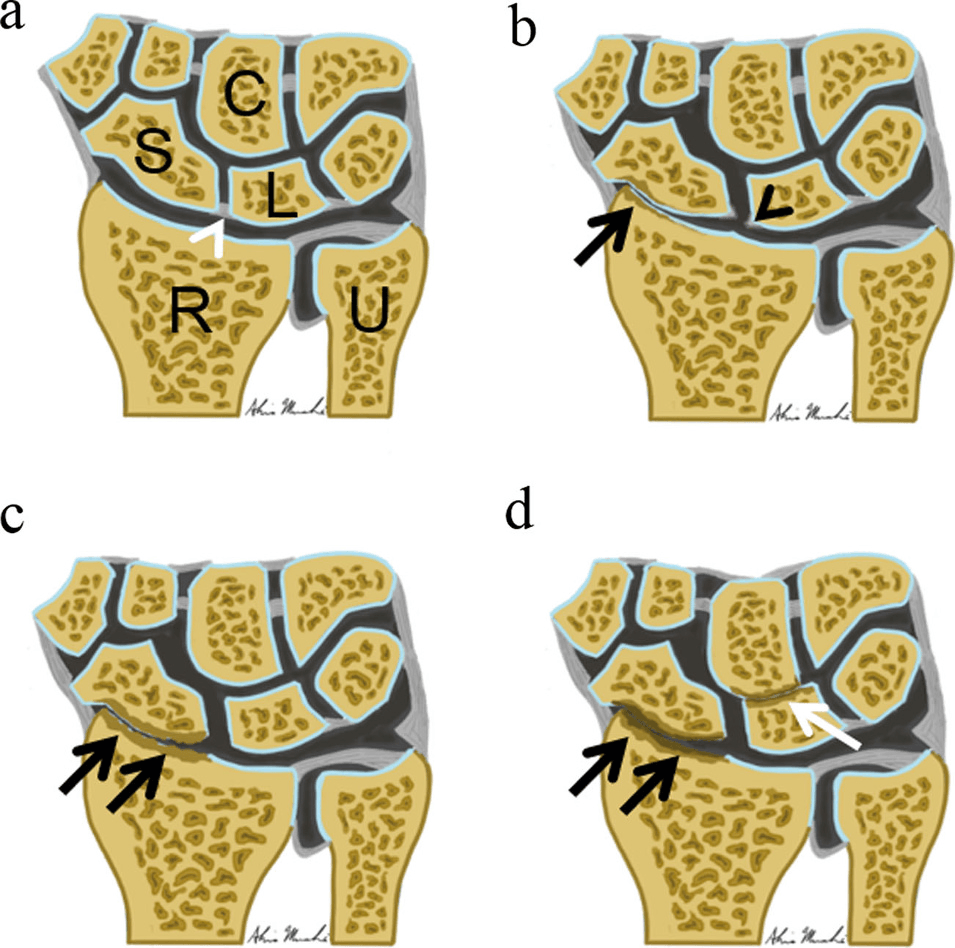
Mack 1984 (PMID 6707028) established that, without treatment, displaced and unstable scaphoid nonunions progress through a time-dependent, predictable sequence (scaphoid-confined change at a mean of ~8 years, radioscaphoid arthritis at ~17 years, generalised wrist arthritis at ~32 years):
- DISI develops - Lunate tilts dorsally without scaphoid tether
- Abnormal loading - Scaphoid fragments malrotate, causing point loading
- Radial styloid arthritis - First site of cartilage wear
- Radioscaphoid arthritis - Progressive involvement of scaphoid fossa
- Capitolunate arthritis - Final stage with midcarpal involvement
Why is the Radiolunate Joint Spared? The radiolunate articulation has:
- Spherical, congruent articulation
- Minimal shear forces during wrist motion
- Protected from abnormal point loading
- Preserved even in advanced SNAC/SLAC
This sparing is the KEY to understanding why motion-preserving surgery works.
Classification - Watson SNAC Staging
Watson Classification for SNAC Wrist:
- Arthritic Changes
- Radial styloid-scaphoid
- Radiographic Findings
- Styloid spurring, narrowed styloid-scaphoid interval
- Key Feature
- Isolated styloid involvement
- Arthritic Changes
- Radioscaphoid + Stage I
- Radiographic Findings
- Scaphoid fossa arthritis, narrowed radioscaphoid space
- Key Feature
- Entire scaphoid fossa involved
- Arthritic Changes
- Capitolunate + Stage I/II
- Radiographic Findings
- Midcarpal narrowing, capitate/lunate arthritis
- Key Feature
- Capitate head damaged
Stage II is the most common presentation for surgical intervention. Patients tolerate Stage I changes well but become symptomatic as arthritis extends into the scaphoid fossa. Stage III often represents end-stage disease with limited reconstruction options.
SNAC 123SNAC STAGES - Progressive Arthritis Pattern
Hook:SNAC progresses from styloid to scaphoid fossa to capitate - always SPARES radiolunate!
Clinical Presentation
History:
- Remote wrist injury - Often forgotten fall onto outstretched hand
- Gradual wrist pain - Progressive over months to years
- Radial-sided wrist pain - Worse with gripping, twisting
- Weakness - Reduced grip strength
- Clicking or clunking - Mechanical symptoms with motion
- Stiffness - Loss of wrist flexion and extension
Physical Examination:
- Description
- Persistent tenderness at scaphoid
- Significance
- Suggests scaphoid pathology
- Description
- Over scapholunate interval
- Significance
- DISI, carpal malalignment
- Description
- Especially extension
- Significance
- Dorsal capsular tightness from DISI
- Description
- Compared to contralateral
- Significance
- Usually 20-50% reduced
- Description
- Painful clunk with pressure on scaphoid tubercle
- Significance
- Scapholunate instability pattern
- Description
- Point tenderness at styloid
- Significance
- Styloid-scaphoid arthritis
Red Flags:
- Acute injury with deformity - acute fracture-dislocation
- Rapid onset in young patient - consider infection, tumour
- Night pain, constitutional symptoms - systemic cause
Differential Diagnosis of Chronic Radial-Sided Wrist Pain:
- 1
- Old scaphoid injury, scaphoid nonunion line, DISI
- 2
- Nonunion with sclerosis; styloid then radioscaphoid then capitolunate arthritis; radiolunate spared
- 3
- Scaphoid fracture/nonunion is the initiating lesion
- 1
- No scaphoid fracture; scapholunate ligament injury
- 2
- SL widening (Terry-Thomas sign), DISI; same arthritic sequence, radiolunate spared
- 3
- Intact scaphoid but disrupted SL ligament
- 1
- Pain at thumb base, positive grind test, older female
- 2
- Trapeziometacarpal joint-space loss and osteophytes
- 3
- Pain localises to thumb base, not snuffbox/dorsal SL interval
- 1
- Pain over first dorsal compartment, positive Finkelstein
- 2
- Normal bony architecture; possible tendon-sheath thickening on US/MRI
- 3
- Tendinous, not articular; no carpal arthritis
- 1
- No antecedent scaphoid fracture or SL injury
- 2
- Isolated radioscaphoid change without nonunion or SL gap
- 3
- Absence of scaphoid nonunion or SL diastasis
- 1
- Central/dorsal wrist pain, lunate sclerosis
- 2
- Lunate sclerosis, fragmentation, collapse (Lichtman stages)
- 3
- Pathology centred on the lunate, not the scaphoid
Investigations

PA View Findings:
Scapholunate widening or Terry-Thomas sign if concurrent SL injury. Scaphoid nonunion line with sclerosis or cystic change. Shortened scaphoid with humpback deformity. Radioscaphoid joint space narrowing in Stage II or III. Styloid spurring in Stage I or higher.
Lateral View Findings:
DISI pattern - increased scapholunate angle greater than 70 degrees. Increased capitolunate angle greater than 30 degrees (normal is less than 15 degrees). Volar flexion of distal scaphoid fragment.
Key Radiographic Measurements:
- Normal
- 30-60 degrees
- SNAC/DISI
- Greater than 70 degrees
- Normal
- Less than 15 degrees
- SNAC/DISI
- Greater than 30 degrees
- Normal
- Less than 15 degrees
- SNAC/DISI
- Greater than 15 degrees
- Normal
- 0.54 ± 0.03
- SNAC/DISI
- Reduced (carpal collapse)
Management Algorithm

Non-operative Management:
- Activity modification
- NSAIDs, wrist splinting
- Corticosteroid injections (temporary relief)
- Rarely successful long-term once SNAC established
Non-operative management is primarily for patients who are poor surgical candidates or those with minimal symptoms. It does not alter the natural history of progression.
Surgical Techniques
Proximal Row Carpectomy (PRC):
Removes the scaphoid, lunate, and triquetrum. The capitate head articulates with the lunate fossa of the radius creating a neoconcentric joint. Simpler procedure with no fusion to heal but requires pristine capitate head.
Stage II SNAC/SLAC with intact capitate head cartilage.
Stage III (capitolunate arthritis), damaged capitate head, inflammatory arthritis.
Dorsal approach, remove proximal row, preserve capsule for soft tissue interposition if desired, protect radial artery.
50-60 degrees arc of motion, grip strength 60-80% of contralateral. Long-term results show progressive radiographic changes but maintained function.
Complications
Proximal Row Carpectomy Complications:
- Incidence
- 20-40% at 10 years
- Prevention/Management
- Salvage with fusion if symptomatic
- Incidence
- 10-20%
- Prevention/Management
- Early ROM exercises, therapy
- Incidence
- Universal
- Prevention/Management
- Expected - counsel patient preop
- Incidence
- Under 1%
- Prevention/Management
- Careful dorsal approach
- Incidence
- 2-5%
- Prevention/Management
- Early recognition, therapy
SE4CF Complications:
- Incidence
- 3-5%
- Prevention/Management
- Adequate bone graft, stable fixation
- Incidence
- 5-10%
- Prevention/Management
- Recessed hardware, low-profile plates
- Incidence
- Common
- Prevention/Management
- Aggressive therapy protocol
- Incidence
- 5%
- Prevention/Management
- Address DRUJ pathology concurrently
- Incidence
- 5-10%
- Prevention/Management
- Salvage option if failed
ALWAYS inspect the capitate head cartilage intra-operatively before committing to PRC. If any cartilage damage is identified, convert to SE4CF. Proceeding with PRC with a damaged capitate will result in rapid failure and pain.
Postoperative Care
Proximal Row Carpectomy (PRC) Protocol:
- Timeframe
- 0-2 weeks
- Activities
- Bulky dressing, elevation, finger ROM
- Timeframe
- 2-4 weeks
- Activities
- Removable splint, begin wrist AROM
- Timeframe
- 4-8 weeks
- Activities
- Strengthen grip, increase activities
- Timeframe
- 8-12 weeks
- Activities
- Full activities, no restrictions
SE4CF Postoperative Protocol:
- Timeframe
- 0-6 weeks
- Activities
- Short arm cast, finger ROM only
- Timeframe
- 6 weeks
- Activities
- Confirm fusion progression on XR
- Timeframe
- 6-10 weeks
- Activities
- Removable splint, begin wrist AROM if healing
- Timeframe
- 10-16 weeks
- Activities
- Progressive grip and wrist strengthening
- Timeframe
- 4-6 months
- Activities
- Full activities once fusion confirmed solid
Key Postoperative Considerations:
- PRC: Earlier motion than SE4CF (no fusion to protect)
- SE4CF: Strict immobilization until fusion - smoking cessation critical
- Both procedures: Hand therapy for ROM and strength
- Pain management: Multimodal analgesia, minimize opioids
- DVT prophylaxis: Mechanical; chemical if high risk
SE4CF nonunion is the main complication to avoid. Strict casting for 6 weeks, smoking cessation, and adequate bone grafting are key. If nonunion suspected at 3 months, consider CT scan to assess fusion status. Revision bone grafting with extended immobilization may achieve union.
Outcomes and Prognosis
Comparative Outcomes - PRC vs SE4CF:
- PRC
- 85-90%
- SE4CF
- 85-90%
- PRC
- 50-60 degrees
- SE4CF
- 40-50 degrees
- PRC
- 60-80%
- SE4CF
- 70-80%
- PRC
- 3-4 months
- SE4CF
- 4-6 months
- PRC
- 5-10% at 10 years
- SE4CF
- 5-10% at 10 years
- PRC
- 85%
- SE4CF
- 85%
Long-term Considerations:
- Both PRC and SE4CF show progressive radiographic changes over time
- Clinical outcomes remain stable despite radiographic deterioration
- Conversion to total wrist fusion remains salvage option if needed
- Younger patients may require revision surgery in their lifetime
Guidelines, Registries & Global Practice
Global epidemiology (PMID-backed):
- Scaphoid fractures are the commonest carpal fracture, predominating in young adult males, and are a leading cause of wrist disability when missed.
- Up to one-third of confirmed scaphoid fractures are radiographically occult on initial presentation, driving wide international variation in imaging pathways (Burns/Duckworth, Edinburgh, PMID 23960052).
- The natural history of untreated displaced/unstable nonunion to SNAC is the most consistently reproduced finding across decades (Mack 1984, PMID 6707028).
Guidance and society positions (no single global guideline mandates one salvage procedure):
- Position on suspected scaphoid injury / nonunion
- Standards support early advanced imaging (MRI/CT) for clinically suspected but radiograph-negative fractures to avoid missed nonunion; salvage by PRC or SE4CF for established SNAC
- Evidence basis
- Consensus standards + cohort evidence
- Position on suspected scaphoid injury / nonunion
- No mandated salvage procedure; choice individualised to stage, capitate cartilage, age and demand; motion-preserving options favoured before total wrist fusion
- Evidence basis
- Expert consensus, systematic reviews
- Position on suspected scaphoid injury / nonunion
- Emphasises anatomical reduction and stable fixation of acute/displaced fractures to prevent nonunion and downstream SNAC
- Evidence basis
- Technical principles + outcome data
- Position on suspected scaphoid injury / nonunion
- Reflects European practice of early MRI for occult injury and stage-based salvage selection
- Evidence basis
- Educational consensus
- There is no dedicated SNAC arthroplasty registry; salvage of SNAC predates and largely avoids prosthetic replacement, so national joint registries (AOANJRR/NJR) capture little SNAC-specific data.
- The best comparative evidence remains systematic review level (Mulford 2009, PMID 19369301): PRC and SE4CF give similar pain relief and satisfaction, with PRC offering slightly more motion but higher subsequent radiographic arthritis.
- PRC is often preferred in lower-demand and older patients (simpler, no fusion to heal); SE4CF is favoured when the capitate head is damaged (Stage III) or in younger/higher-demand wrists.
- Fixation for SE4CF varies internationally between K-wires, headless compression screws and circular plates; reported nonunion and hardware-complication rates depend heavily on technique (Vance 2005, PMID 16344166; Merrell 2008, PMID 18590844).
Scaphoid nonunion is common in young males following sport, motor-vehicle and workplace trauma, frequently presenting late.
For the FRACS examination, candidates must understand the natural history of scaphoid nonunion progressing to SNAC (Mack 1984), the Watson staging system, and the rationale for motion-preserving surgery based on radiolunate joint sparing (Watson and Ballet 1984). Be prepared to discuss PRC vs SE4CF indications and the importance of capitate head assessment.
MCQ Practice Points
Q: What is the difference between SNAC and SLAC? A: SNAC (Scaphoid Nonunion Advanced Collapse) results from untreated scaphoid nonunion. SLAC (Scapholunate Advanced Collapse) results from scapholunate ligament injury. Both follow the same degenerative pattern and have identical treatment.
Q: Which joint is characteristically spared in SNAC and SLAC? A: The radiolunate joint is always spared. This is because the spherical lunate-radius articulation maintains congruent contact even when carpal kinematics are disrupted. This sparing allows motion-preserving salvage surgery.
Q: Why is PRC contraindicated in Stage III SNAC? A: In Stage III, the capitolunate joint is arthritic. PRC requires the capitate head to articulate with the lunate fossa of the radius. Damaged capitate cartilage will cause rapid failure and pain. SE4CF is the motion-preserving option for Stage III.
Q: What carpal instability pattern develops with scaphoid nonunion? A: DISI (Dorsal Intercalated Segment Instability). The lunate tilts dorsally when it loses its connection to the scaphoid. Radiographically: scapholunate angle greater than 70 degrees, capitolunate angle greater than 30 degrees.
Q: Compare the outcomes of PRC versus SE4CF. A: Both provide 85-90% pain relief and similar satisfaction. PRC: simpler, faster recovery, slightly more motion (50-60 degrees), but requires intact capitate. SE4CF: more complex, slower recovery, slightly less motion (40-50 degrees), but works even in Stage III.
Q: Why does scaphoid nonunion occur? A: The scaphoid has a retrograde blood supply entering through the dorsal ridge. Proximal pole and waist fractures disrupt blood flow to the proximal fragment, causing AVN and nonunion. This is why proximal pole fractures have the highest nonunion rate.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old carpenter presents with 2 years of progressive radial wrist pain. He recalls a fall 15 years ago but never sought treatment. Radiographs show scaphoid nonunion with radioscaphoid arthritis but preserved capitolunate joint. What is your management?”
“A 55-year-old presents with severe wrist pain and stiffness. Radiographs show scaphoid nonunion with arthritis at the radioscaphoid AND capitolunate joints. What are the treatment options?”
“A 25-year-old presents 2 years after a wrist injury. Radiographs show scaphoid waist nonunion but NO arthritis. Should you treat this?”
“A patient underwent PRC for Stage II SNAC 3 years ago. They now present with recurrent pain and stiffness. Radiographs show progressive arthritis at the capitate-lunate fossa articulation. What are the options?”
Watson Staging
- Stage I: Radial styloid-scaphoid arthritis ONLY
- Stage II: Radioscaphoid arthritis (entire scaphoid fossa)
- Stage III: Capitolunate arthritis (midcarpal joint)
- RADIOLUNATE JOINT IS ALWAYS SPARED
- Staging identical for SLAC (different cause, same pattern)
Surgical Decision Making
- Stage I: Styloidectomy plus/minus scaphoid reconstruction
- Stage II: PRC or SE4CF - capitate status decides
- Stage III: SE4CF only (PRC contraindicated)
- Total wrist fusion: salvage or high-demand patient
- ALWAYS inspect capitate head intra-operatively
PRC Key Points
- Remove scaphoid, lunate, triquetrum
- Capitate articulates with lunate fossa of radius
- REQUIRES pristine capitate head cartilage
- Contraindicated in Stage III
- Motion: 50-60 degrees arc, grip 60-80%
SE4CF Key Points
- Remove scaphoid, fuse capitate-lunate-hamate-triquetrum
- Works even with damaged capitate head
- Motion: 40-50 degrees arc, grip 70-80%
- Nonunion rate 3-5% (smoking increases risk)
- Can be done in Stage II or III
Why Radiolunate Spared
- Spherical, congruent articulation
- Minimal shear forces during wrist motion
- Not subject to abnormal point loading
- Allows motion-preserving salvage surgery
- Same principle in both SNAC and SLAC
DISI Pattern
- Dorsal Intercalated Segment Instability
- Lunate tilts dorsally without scaphoid linkage
- Scapholunate angle greater than 70 degrees
- Capitolunate angle greater than 30 degrees
- Seen on lateral radiograph
Evidence Base
PRC vs SE4CF — Systematic Review of Outcomes
- Systematic review of 52 studies of PRC or four-corner fusion for SLAC/SNAC wrists
- Both procedures improve pain and subjective outcomes for appropriately staged wrists
- PRC may give better postoperative range of movement and avoids fusion-specific complications (nonunion, hardware, dorsal impingement)
- Risk of subsequent radiographic osteoarthritis was significantly higher after PRC, though mostly asymptomatic at review; grip strength and pain relief were similar
Long-term PRC Outcomes (minimum 10-year follow-up)
- Twenty wrists followed for an average of 13.1 years (range 10.0-17.2 years)
- Average wrist arc was 63% and grip strength 83% of the opposite side; 17 of 20 patients satisfied
- Two patients (10%) required conversion to radiocapitate arthrodesis for persistent pain
- Radiocapitate radiographic changes did not correlate with pain or satisfaction
Natural History of Scaphoid Non-union (the defining study)
- Forty-seven symptomatic nonunions reviewed; duration of nonunion ranged from 5 to 53 years
- Three radiographic stages by duration: scaphoid-confined change (mean 8.2 years), radioscaphoid arthritis (mean 17.0 years), generalised wrist arthritis (mean 31.6 years)
- Fracture displacement and carpal instability correlated with severity of degenerative change; lunate dorsiflexion of 10 degrees or more flagged instability
- Few nonunions remained free of arthritis beyond 10 years
SLAC Wrist — Original Description of the Degenerative Pattern
- Review of 4000 wrist radiographs; 210 cases of degenerative arthritis analysed
- Scapholunate advanced collapse (radioscaphoid then capitolunate) was the most common pattern (57%)
- Radiolunate joint characteristically spared, providing the rationale for motion-preserving salvage
- Motion-preserving surgery in 19 patients reduced pain in 18 of 19
Four-Corner Fusion — Circular Plate vs Traditional Fixation
- 58 four-corner fusions: 27 circular-plate vs 31 traditional (wires, staples, screws)
- Major complication rate (nonunion or impingement) markedly higher with circular plates (48%) than traditional fixation (6%)
- Plate group: 26% nonunion with loose hardware versus 3% in the traditional group
- Grip and arc of motion were similar (~70-80% and ~48-50% of contralateral) but dissatisfaction was higher with plates
Standardised Circular-Plate Four-Corner Fusion (reproducible technique)
- Consecutive series of 28 SLAC/SNAC/midcarpal-arthrosis wrists, mean follow-up 46 months
- Capitolunate fusion mass united in all cases using a recessed second-generation circular plate plus distal radius graft
- Arc averaged 45% and grip 82% of the uninjured side; low mean pain and activity scores
- No secondary radiolunate arthritic change, supporting durability when technique and graft are optimal