SICK Scapula Syndrome
Kibler Classification
Critical Must-Knows
- Scapular dyskinesis is usually a SIGN of underlying pathology, not a primary diagnosis
- SICK Scapula: Scapular malposition, Inferior medial border prominence, Coracoid pain, dysKinesis
- Legs and trunk generate 50% of the force in throwing (Kinetic Chain)
- Pectoralis minor tightness is a key driver of anterior tilt
- Serratus anterior weakness causes medial winging
Clinical Pearls
- "Assess for 'Winging' during wall push-up (Serratus)
- "Scapular Assistance Test (SAT): Does manual stabilization relieve pain?
- "Scapular Retraction Test (SRT): Does retraction increase power?
- "Look for 'Pseudowinging' (Long thoracic nerve palsy vs Dyskinesis)
Critical Exam Points
Don't Operate
Contraindication. Scapular dyskinesis is a functional problem managed with REHAB. Do not operate on the scapula unless there is a structural cause (e.g., osteochondroma, nerve palsy).
SICK Acronym
Scapular malposition, Inferior border prominence, Coracoid pain, dysKinesis of movement. Learn this definition.
The Kinetic Chain
Proximal Stability for Distal Mobility. Weak core/hips transfer increased load to the shoulder. Rehab starts at the legs/trunk.
Nerve Exclusion
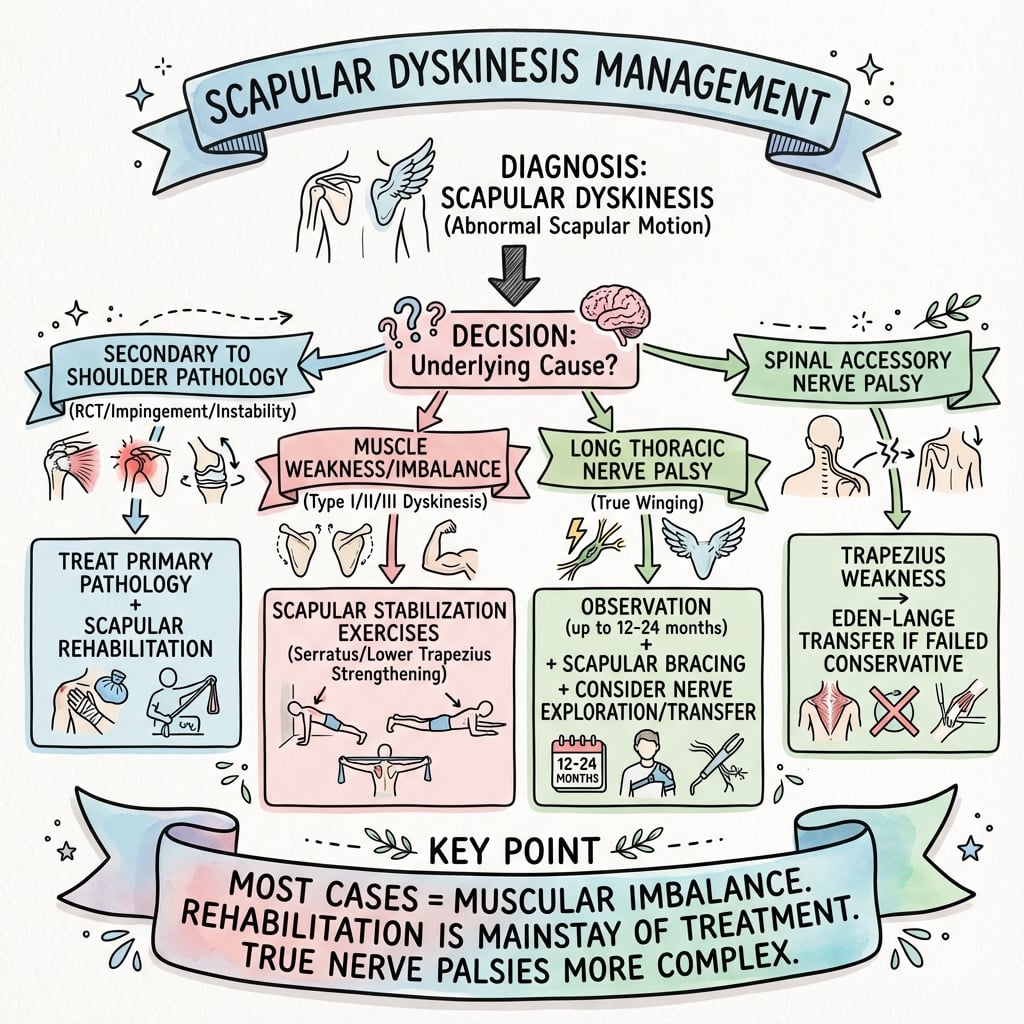
Always rule out Long Thoracic Nerve (Serratus) and Spinal Accessory Nerve (Trapezius) palsy. Dyskinesis is usually bilateral/functional; Palsy is unilateral/structural.
At a Glance
| Condition | Pathology | Management | Key Feature |
|---|---|---|---|
| Scapular Dyskinesis | Functional Imbalance | Physiotherapy (Kinetic Chain) | SICK Syndrome |
| Long Thoracic Palsy | Nerve Injury (Structural) | Observe to Transfer | Medial Winging |
| Snapping Scapula | Bursitis / Osteochondroma | Injection to Bursectomy | Crepitus |
Dyskinesis vs Winging (Nerve Palsy)
| Feature | Scapular Dyskinesis | True Winging (Nerve Palsy) |
|---|---|---|
| Cause | Muscle Imbalance / Inhibition | Neurological Injury |
| Appearance | Subtle, often Type 1-3 pattern | Gross deformity |
| Symptom | Pain / Impingement | Weakness / Deformity |
| Management | Physiotherapy (Scapula Setting) | Observation / Nerve Transfer / Fusion |
SICKSICK Scapula
| S | Scapular Malposition In resting position |
| I | Inferior Medial Border Prominence (Winging) |
| C | Coracoid Pain Tenderness (Pect Minor attachment) |
| K | dysKinesis Abnormal movement pattern |
| S | Scapular Malposition In resting position | C | Coracoid Pain Tenderness (Pect Minor attachment) |
| I | Inferior Medial Border Prominence (Winging) | K | dysKinesis Abnormal movement pattern |
Hook:A SICK scapula needs rehab, not surgery
IMSKibler Classification
| I | Inferior Type I: Inferior angle prominence (Anterior Tilt) |
| M | Medial Type II: Medial border prominence (Internal Rotation) |
| S | Superior Type III: Superior border prominence (Shrug) |
| I | Inferior Type I: Inferior angle prominence (Anterior Tilt) |
| M | Medial Type II: Medial border prominence (Internal Rotation) |
| S | Superior Type III: Superior border prominence (Shrug) |
Hook:Inferior, Medial, Superior (1, 2, 3)
CORERehab Principles
| C | Conscious Control Biofeedback / Mirrors |
| O | Open Chain Progress to open chain later |
| R | Retraction Focus on Lower Trap / Serratus |
| E | Endurance Low load, high repetition |
| C | Conscious Control Biofeedback / Mirrors | R | Retraction Focus on Lower Trap / Serratus |
| O | Open Chain Progress to open chain later | E | Endurance Low load, high repetition |
Hook:Restore the CORE stability
Overview and Epidemiology
Chicken or Egg?
Scapular dyskinesis is often a secondary phenomenon reacting to glenohumeral pathology (e.g., instability, cuff tear, SLAP). It serves as a compensatory mechanism (like a limp). Treating the dyskinesis is essential, but you must also address the primary pathology.
Definition
Alteration of the normal position and motion of the scapula during scapulohumeral movements.
The Role of the Scapula
- Stable Base: For rotator cuff origin.
- Gleneohumeral Alignment: Maintains ball-socket congruency (glenoid tracks the head).
- Force Transfer: Integral link in the kinetic chain transferring energy from trunk to arm.
Pathophysiology and Mechanisms
Key Force Couples
Stability relies on balanced force couples. In dyskinesis, these are disrupted.
- Trapezius Force Couple:
- Upper Trap: Elevates.
- Lower Trap: Depresses/Retracts.
- Imbalance: Overactive Upper + Weak Lower = Scapular Shrug (Type III).
- Serratus Anterior:
- Protracts and stabilizes medial border.
- Weakness = Medial Winging (Type II).
- Pectoralis Minor:
- Depresses and Anteriorly Tilts.
- Tightness = Anterior Tilt (Type I).
Classification Systems
Kibler Classification
Qualitative visual assessment during elevation.
| Type | Prominence | Mechanism | Associated Muscle |
|---|---|---|---|
| Type I | Inferior Medial Angle | Anterior Tiliting | Tight Pect Minor / Weak Lower Trap |
| Type II | Entire Medial Border | Internal Rotation | Weak Serratus Anterior |
| Type III | Superior Medial Border | Early Elevation (Shrug) | Overactive Upper Trap |
| Type IV | Symmetric | Normal Motion | Normal |
Clinical Assessment
Visual Inspection
- Inspect from back. Look for asymmetry in resting height and distance from spine.
- Check for Pect Minor Tightness (Forward shoulder posture).
- Palpate Coracoid (Tenderness).
Dynamic Assessment
- Scapular Dyskinesis Test: Patient performs weighted flexion/abduction (3-5 lbs).
- Observe for medial border prominence or dysrhythmia (shuddering).
- Wall Push-Up: Accentuates winging (Serratus weakness).
Corrective Maneuvers
- Examiner actively assists upward rotation and posterior tilt during elevation.
- Positive Test: Reduction in impingement pain.
- Significance: Confirms that scapular dysfunction is contributing to symptoms.
- Examiner manually stabilizes medial border in retraction.
- Patient performs isometric elevation.
- Positive Test: Increase in strength (or reduction in pain).
- Significance: Indicates weak retractors (Rhomboids/Traps).
Investigations
Clinical Diagnosis
Scapular Dyskinesis is a Clinical Diagnosis. Imaging is used to rule out other causes, not to verify dyskinesis.
EMG
Electromyography is the gold standard if nerve palsy is suspected (Long Thoracic / Spinal Accessory). It differentiates neuropathic weakness from functional inhibition.
Imaging Protocol
- AP / Axillary / Outlet.
- Check for structural causes: Osteochondroma (Snapping Scapula), fracture malunion, AC joint pathology.
- Assess for the "Primary" cause: Rotator Cuff Tear, Labral Tear (SLAP).
- Assess periscapular muscles for denervation atrophy (edema/fatty infiltration).
- Indicated for "Snapping Scapula" to visualize rib cage incongruity or Luschka's tubercle.
Management Algorithm
The Mainstay of Treatment
Protocol phases (Kibler):
- Acute Phase:
- Address primary pathology (e.g., pain control, cuff inflammation).
- Soft tissue work: Release tight Pectoralis Minor and Posterior Capsule.
- Core stability.
- Recovery Phase (Static):
- Isometrics ("Scapular Setting").
- "Low Row", "Inferior Glide".
- Closed chain exercises (Wall slides).
- Maintenance Phase (Dynamic):
- Open chain strengthening.
- Plyometrics.
- Sport-specific mechanics.
Surgical Technique
Arthroscopic Release
- Indication: Persistent anterior tilt + coracoid pain refractory to stretching.
- Position: Beach chair or Lateral Decubitus.
- Visualisation: Scope in standard posterior portal.
- Technique: Locate Pect Minor insertion at coracoid. Release using radiofrequency probe.
- Outcome: Improves scapular tipping and reduces impingement.
Complications
| Issue | Consequence | Solution |
|---|---|---|
| Ignore the Scapula | Failed Cuff Rehab | Include Kinetic Chain |
| Over-strengthening | Upper Trap Dominance | Focus on Lower Trap |
| Snapping Scapula | Bursal Inflammation | Bursectomy (Rare) |
| Post-Fusion Breathlessness | Restricted Chest Expansion | Pre-op Warning |
Rehabilitation Protocols
Closed Chain
Start Here. Hand fixed (e.g., Wall push-up, Quadruped). Promotes joint stability via compression and co-contraction. Safer for rotator cuff.
Open Chain
Progress To This. Hand free (e.g., Dumbbell press, Throwing). Requires greater dynamic control. Higher shear forces.
| Exercise | Target Muscle | Phase |
|---|---|---|
| Sleeper Stretch | Posterior Capsule | Phase 1 |
| Doorway Stretch | Pectoralis Minor | Phase 1 |
| Scapular Clock | Serratus / Traps | Phase 2 |
| Wall Slides | Serratus Anterior | Phase 2 |
| Push-Up Plus | Serratus Anterior | Phase 3 |
| Prone Y-W-T | Lower Trap / Rhomboids | Phase 3 |
Postoperative Care
There is rarely 'Postoperative' care as surgery is rare. For Pect Minor release:
Pect Minor Release Rehab
- Sling for comfort only.
- Immediate active assist ROM.
- Focus on posterior tilt and retraction.
- Lower trapezius activation.
- Unrestricted strengthening.
Outcomes and Prognosis
Conservative
Highly Successful. 80-90% of patients improve with a dedicated, scapula-focused rehabilitation program (usually 3-6 months).
Recurrence
Common if patients revert to poor mechanics or stop maintenance exercises.
Surgery
Outcomes for nerve transfers (Pect Major) are variable. Fusion provides stability but eliminates scapulothoracic motion (loss of 30% elevation).
Evidence Base
SICK Scapula / Disabled Throwing Shoulder Part III
- Defined the SICK scapula syndrome (Scapular malposition, Inferior medial border prominence, Coracoid pain, dysKinesis)
- Linked scapular dysfunction to glenohumeral injury in overhead throwers
- Established the kinetic-chain rehabilitation framework
2013 Scapular Summit Consensus
- Dyskinesis is present in a high percentage of shoulder injuries but is an impairment, not a stand-alone diagnosis
- Impingement symptoms are particularly affected by dyskinesis
- A reliable observational (yes/no) clinical method is available, and scapular rehabilitation is effective within a comprehensive programme
Reliability of Qualitative Classification
- Tested the four-pattern visual classification of scapular dysfunction
- Interrater reliability kappa = 0.4 (moderate); intrarater kappa = 0.5
- Modest reliability later led to a Yes/No (present-absent) observational method
Scapular Dyskinesis and Future Shoulder Pain
- Pooled 5 prospective studies (419 athletes)
- Baseline dyskinesis carried a 43% greater risk of future shoulder pain (RR 1.43, 95% CI 1.05-1.93)
- 35% of athletes with dyskinesis vs 25% without developed pain at 9-24 months
Kinetic Chain Rehabilitation
- Described the proximal-to-distal kinetic-link model for shoulder rehabilitation
- Energy and force are generated in the legs and trunk and transmitted through the scapula to the arm
- Closed-chain and integrated movement patterns activate weakened shoulder musculature
Pectoralis Minor Length and Scapular Kinematics
- 50 asymptomatic volunteers grouped by pectoralis minor resting length
- Short pectoralis minor was associated with persistent anterior tipping and increased internal rotation of the scapula
- These kinematics mirror those seen in subacromial impingement
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: The Throwing Athlete
"A 22-year-old baseball pitcher presents with anterior shoulder pain and dropping velocity. You diagnose subacromial impingement. On exam, he has a drooped shoulder. Describe your assessment of his scapula."
Scenario 2: Winging Differential
"How do you differentiate functional Scapular Dyskinesis from a Long Thoracic Nerve Palsy (True Winging)?"
Scenario 3: Management Principles
"Outline your rehabilitation strategy for a swimmer with Type 2 Scapular Dyskinesis."
MCQ Practice Points
SICK Scapula
Q: What does the 'C' in SICK Scapula stand for? A: Coracoid Pain. This is due to traction tendinopathy of the tight Pectoralis Minor insertion.
Kibler Type II
Q: Which muscle weakness is primarily associated with Kibler Type II dyskinesis (Medial Border Prominence)? A: Serratus Anterior weakness (or inhibition) leads to medial border winging.
Corrective Tests
Q: A positive Scapular Assistance Test (SAT) implies what? A: That scapular dyskinesis is contributing to the patient's impingement symptoms (pain is relieved when the examiner assists motion).
Nerve Injury
Q: Injury to the Spinal Accessory Nerve results in what type of winging? A: Lateral Winging (Trapezius palsy). The scapula translates laterally and rotates downward. (Contrast with Medial Winging in Long Thoracic/Serratus palsy).
Kinetic Chain
Q: What percentage of energy in the throwing motion is generated by the legs and trunk? A: Approximately 50-55%. Only half is generated by the shoulder/arm.
Controversies & Areas of Uncertainty
Cause or Consequence?
Whether dyskinesis is a primary driver of shoulder pathology or a secondary adaptation remains unresolved. The 2013 Scapular Summit concluded it is best regarded as a potential impairment rather than a discrete diagnosis, and its exact causal role is not clearly defined.
Subtype Classification
The Kibler I/II/III/IV subtypes have only moderate interrater reliability (kappa around 0.4). Many authorities now favour a binary present vs absent judgement, supplemented by the SAT/SRT corrective tests.
Predictive Value
Meta-analysis shows a real but modest 43% relative increase in future shoulder pain. However, a large mixed-sex handball cohort could NOT confirm dyskinesis as an independent risk factor, so it should not be used in isolation to predict injury.
Visualisation vs Instrumented
Visual observation is practical but imperfect; 3D motion capture and scapular dyskinesis test scoring improve objectivity but are largely research tools. There is no agreed gold-standard quantitative bedside measure.
Guidelines, Registries & Global Practice
Society / Consensus Positions
| Body | Position on Scapular Dyskinesis |
|---|---|
| 2013 Scapular Summit (BJSM, intl.) | Impairment, not a diagnosis; reliable yes/no assessment; scapular rehab within a comprehensive programme |
| AAOS (US) / sports medicine | Address scapular control as part of rotator cuff and impingement rehabilitation; surgery reserved for structural causes |
| BOA / UK practice | Physiotherapy-led, kinetic-chain rehabilitation first-line; refer for nerve studies if true winging suspected |
| IOC / overhead-sport consensus | Screen overhead athletes; combine GIRD, cuff strength and scapular control in injury-prevention programmes |
Global Epidemiology
Dyskinesis is found in 60-100% of shoulders with injury (rotator cuff disease, instability, SLAP) and in a high proportion of asymptomatic overhead athletes. There is no implant registry — this is a functional, non-operative condition.
High-Resource Settings
Access to specialist sports physiotherapy, video and 3D motion analysis, and EMG. Generic cuff exercises frequently fail when the scapular component is ignored.
Limited-Resource Settings
Diagnosis is purely clinical and free: inspection, the scapular dyskinesis test, SAT and SRT. Home-based stretching (pectoralis minor, posterior capsule) and closed-chain wall exercises require no equipment.
Occupational Context
Common in repetitive overhead workers (painters, electricians, assembly) worldwide. Management is functional rehabilitation and ergonomic modification, not surgery.
SCAPULAR DYSKINESIS CHEATSHEET
Clinical summary
The S.I.C.K Scapula
- •S: Scapular Malposition
- •I: Inferior Medial Prominence
- •C: Coracoid Pain
- •K: dysKinesis
Kibler Classification
- •Type I: Inferior (Ant Tilt)
- •Type II: Medial (Int Rot)
- •Type III: Superior (Shrug)
- •Type IV: Normal
Key Muscles
- •Serratus Ant: Weakness = Winging
- •Pect Minor: Tightness = Tilt
- •Lower Trap: Weakness = Dysfunction
- •Upper Trap: Overactivity = Shrug
Management Rules
- •NO Surgery (Functional)
- •Stretch Pect Minor
- •Kinetic Chain (Core/Legs)
- •Closed Chain before Open