Closed Forequarter Amputation | High-Energy Trauma | Neurovascular Emergency
- Scapulothoracic dissociation = traumatic disruption of the scapulothoracic articulation
- Lateral scapular displacement greater than 1.0 on scapular index = diagnostic
- Brachial plexus avulsion in 94% - often complete (C5-T1) with poor prognosis
- Subclavian/axillary injury in 88% - may be occult, requires angiography
- Flail extremity in 52%, early amputation in 21%, death in 10% (Damschen series, n=58)
- Type III (complete flail limb) often requires forequarter / above-elbow amputation
- “Called 'closed forequarter amputation' - internal degloving of shoulder girdle
- “High-energy mechanism: MVA, motorcycle, industrial traction injuries
- “CXR shows lateral scapular displacement - measure scapular index
- “Flail limb with absent pulses = emergent angiography + vascular surgery consult
10% mortality and 21% early amputation (Damschen series). Massive soft tissue disruption with occult hemorrhage. Polytrauma protocol - ATLS management takes priority over limb. Life before limb.
94% brachial plexus injury - often complete avulsion (C5-T1). 88% vascular injury - subclavian or axillary. Occult hemorrhage may cause hemodynamic instability.
Ratio of distance from midline to medial scapular border: injured/uninjured. Ratio greater than 1.0 is diagnostic. Lateral displacement on CXR is the key finding.
Complete neurological deficit + vascular injury = flail limb (Type III). Limb salvage rarely successful. Forequarter amputation may be the most functional outcome.
- Classification
- Type I (musculoskeletal)
- Management
- Treat bony injuries, observe
- Prognosis
- Good - preserve function
- Classification
- Type IIA (viable)
- Management
- Urgent vascular repair
- Prognosis
- Variable - depends on neuro
- Classification
- Type IIB (ischemic)
- Management
- Emergency revascularization
- Prognosis
- Reasonable if neuro intact
- Classification
- Type III (complete avulsion)
- Management
- Consider forequarter amputation
- Prognosis
- Poor - non-functional limb
SCAPSCAP - Scapulothoracic Dissociation Features
Hook:SCAP for SCAPulothoracic - remember the 4 key components of this devastating injury
FLAILFLAIL - Indications for Amputation
Hook:FLAIL limb = amputation consideration - all 5 features typically present in Type III
INDEXINDEX - Scapular Index Calculation
Hook:INDEX greater than 1.0 = lateral displacement = scapulothoracic dissociation
Overview and Epidemiology
Scapulothoracic dissociation is a true orthopaedic emergency. In the landmark Damschen review (n=58), mortality was 10%, early amputation 21%, and a flail extremity resulted in 52%. It represents a spectrum from isolated musculoskeletal injury to complete "closed forequarter amputation." Polytrauma assessment and resuscitation take absolute priority.
- Traumatic separation of the scapula from the thoracic wall
- Complete disruption of scapulothoracic articulation
- Involves AC joint, SC joint, or clavicle fracture
- Associated soft tissue envelope disruption
- Often called "closed forequarter amputation"
- Rare injury - true incidence unknown (frequently underdiagnosed)
- High-energy mechanism required (motorcycle, MVA, industrial traction)
- Young males predominate (typical high-energy trauma demographic; mean age ~32 years in Zelle series)
- 10% mortality, 21% early amputation, 52% flail extremity (Damschen, n=58)
- Neurological injury in 94%, vascular injury in 88%
High-energy lateral traction to the upper limb. Common mechanisms include:
- Motorcycle accidents - arm caught, body continues
- Motor vehicle accidents - ejection with arm traction
- Industrial accidents - machinery entrapment
- Agricultural accidents - PTO (power take-off) injuries
Pathophysiology and Anatomy
The scapula is connected to the axial skeleton only by the clavicle (via AC and SC joints). All other attachments are muscular. Scapulothoracic dissociation requires disruption of these bony connections PLUS the extensive muscular envelope, neurovascular structures, and soft tissues.
- Normal Function
- Bone bridge to axial skeleton
- Injury Pattern
- Fracture or dislocation
- Normal Function
- Scapular retraction/elevation
- Injury Pattern
- Complete rupture
- Normal Function
- Upper limb perfusion
- Injury Pattern
- Tear, avulsion, intimal injury
- Normal Function
- Venous return
- Injury Pattern
- May cause massive hemorrhage
- Normal Function
- Motor and sensory function
- Injury Pattern
- Avulsion (preganglionic) or rupture
- Normal Function
- Soft tissue envelope
- Injury Pattern
- Internal degloving (Morel-Lavallée)
- Avulsion (preganglionic): Root torn from cord - NOT repairable
- Rupture (postganglionic): Nerve torn in continuity - potentially repairable
- Complete plexus (C5-T1): Most common pattern in STD
- Avulsion features: Horner syndrome, absent SNAP, positive myelogram
- Complete transection: Obvious, requires repair
- Intimal tear: May thrombose hours later - occult
- Pseudoaneurysm: Delayed presentation
- Always assume vascular injury until proven otherwise
Avulsion (preganglionic) = root torn FROM the spinal cord = NOT repairable = poor prognosis Rupture (postganglionic) = nerve torn BEYOND ganglion = potentially repairable = better prognosis
Clinical clues to AVULSION:
- Horner syndrome (ptosis, miosis, anhidrosis) - T1 root
- Rhomboid/serratus paralysis - dorsal scapular and long thoracic nerves
- Preserved SNAP (Sensory Nerve Action Potential) despite anesthesia - dorsal root ganglion intact
Classification Systems
- Description
- Musculoskeletal injury only
- Neurovascular Status
- Intact
- Management
- Conservative/fixation
- Description
- Vascular injury, limb viable
- Neurovascular Status
- Perfused, variable neuro
- Management
- Urgent vascular repair
- Description
- Vascular injury, limb ischemic
- Neurovascular Status
- Non-perfused, variable neuro
- Management
- Emergency revascularization
- Description
- Complete neurovascular disruption
- Neurovascular Status
- Flail limb
- Management
- Amputation consideration
Type I is rare in true scapulothoracic dissociation (most have some neurovascular injury). The distinction between IIA and IIB is based on ischemia time - IIB requires emergent intervention. Type III represents complete "internal forequarter amputation."
For exam purposes, Damschen is the most commonly cited classification. The key decision points are:
- Is there vascular injury? (Type I vs II/III)
- Is the limb ischemic? (IIA vs IIB)
- Is there complete neurological loss? (Type III = flail limb)
1-2A-2B-3DAMSCHEN - Classification Types
Hook:Think 1-2-3: Type 2 splits into A (alive) and B (bad ischemia)
Clinical Assessment
These patients are polytrauma until proven otherwise. Complete ATLS primary and secondary survey before focused limb assessment. Hemorrhagic shock from occult vascular injury is common.
- Mechanism: High-energy lateral traction to arm
- Time from injury (ischemia time critical)
- Associated injuries (chest, spine, other limbs)
- Hand dominance (for functional prognosis)
- Occupation (manual labor vs sedentary)
- Massive swelling of shoulder girdle
- Lateral displacement of entire shoulder
- Skin changes (bruising, abrasions, degloving)
- Limb position (may hang flaccid)
- Open wounds (rare - usually closed injury)
Clinical Examination Sequence
Airway, Breathing, Circulation, Disability, Exposure. Address life-threatening injuries. IV access, resuscitation as needed.
Pulses (radial, ulnar, brachial). Capillary refill. Doppler if pulses absent. Hand temperature and color. Document ischemia time.
Brachial plexus assessment: C5 (shoulder abduction), C6 (wrist extension), C7 (elbow extension), C8 (finger flexion), T1 (finger abduction). Horner syndrome (T1 avulsion).
Clavicle palpation (fracture). AC joint stability. SC joint assessment. Scapular position. Associated limb injuries.
- Motor Function
- Shoulder abduction (deltoid)
- Sensory
- Lateral arm
- Reflex
- Biceps
- Motor Function
- Wrist extension (ECRL/ECRB)
- Sensory
- Lateral forearm, thumb
- Reflex
- Brachioradialis
- Motor Function
- Elbow extension (triceps)
- Sensory
- Middle finger
- Reflex
- Triceps
- Motor Function
- Finger flexion (FDP)
- Sensory
- Medial forearm
- Reflex
- -
- Motor Function
- Finger abduction (interossei)
- Sensory
- Medial arm
- Reflex
- -
Horner syndrome (ptosis, miosis, anhidrosis) indicates T1 root avulsion. This is a preganglionic injury and is NOT repairable. Its presence suggests complete plexus avulsion and poor prognosis for limb function.
- Distinguishing Features
- Lateral scapular displacement (index greater than 1.0), combined neuro + vascular deficit, intact skin
- Pitfall to Avoid
- The closed skin envelope can mask the severity - look for the radiographic sign
- Distinguishing Features
- Neurological deficit WITHOUT scapular lateralisation or major vessel injury
- Pitfall to Avoid
- Do not assume an isolated plexus lesion - always exclude vascular injury and STD
- Distinguishing Features
- Pulseless limb, normal scapular position, neurology may be intact
- Pitfall to Avoid
- STD is suggested when vascular injury coexists with plexus deficit and scapular displacement
- Distinguishing Features
- Double disruption of the superior shoulder suspensory complex; scapula NOT lateralised
- Pitfall to Avoid
- STD is a more proximal, neurovascular catastrophe - not the same entity
- Distinguishing Features
- Mediastinal compression symptoms; localised SC deformity
- Pitfall to Avoid
- Posterior SC dislocation can itself threaten great vessels - image with CT angiography
- Distinguishing Features
- Open soft-tissue disruption / external degloving
- Pitfall to Avoid
- STD is the CLOSED equivalent - intact skin distinguishes it
Investigations
- Key Findings
- Lateral scapular displacement, fractures, hemothorax
- Utility
- Initial screening - measure scapular index
- Key Findings
- Vascular injury, intimal flap, occlusion
- Utility
- Gold standard for vascular assessment
- Key Findings
- Definitive vascular imaging, allows intervention
- Utility
- If CTA equivocal or intervention planned
- Key Findings
- Nerve root avulsion (pseudomeningoceles)
- Utility
- Delayed - for surgical planning
- Key Findings
- Distinguish avulsion vs rupture
- Utility
- Delayed (3 weeks) - preserved SNAP = avulsion
Scapular Index = Injured side / Normal side
Measure from midline (spinous processes) to medial border of scapula on CXR or CT scout
- Index greater than 1.0 = lateral displacement = positive
- The mean scapula index was 1.29 in the Zelle series (n=25)
- Any significant asymmetry on a non-rotated film is concerning
- Vessel occlusion - complete cutoff
- Intimal flap - linear filling defect
- Pseudoaneurysm - contained rupture
- Active extravasation - contrast blush
- Vessel displacement - with hematoma
Performed at 3+ weeks post-injury. The key finding distinguishing avulsion from rupture is:
- SNAP (Sensory Nerve Action Potential) preserved = AVULSION (dorsal root ganglion intact, sensory fibers still connected to ganglion but disconnected from cord)
- SNAP absent = RUPTURE (entire nerve disrupted including sensory fibers)
Management
Life before Limb. ATLS resuscitation takes absolute priority. Hemorrhagic shock is common from occult vascular injury. Once stable, address vascular emergency before definitive orthopaedic management.
Acute Resuscitation
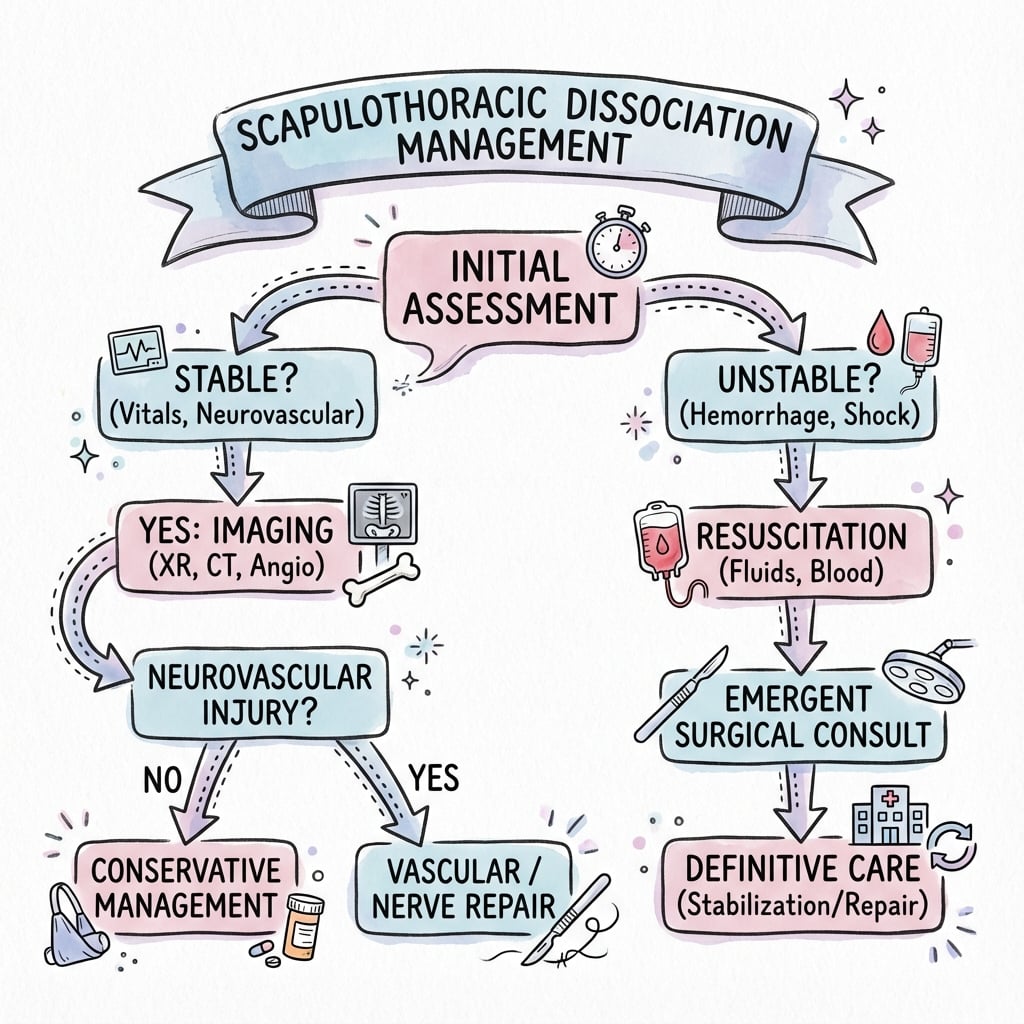
Emergency Management Algorithm
Airway, Breathing, Circulation, Disability, Exposure. Large bore IV access. Blood products if shocked. Address life-threatening injuries (tension pneumothorax, hemothorax).
Pulse check. If absent/diminished: emergent CTA or direct to angiography. Vascular surgery consult. Document ischemia time.
Complete brachial plexus examination. Document motor (0-5 scale) and sensory function for each root. Look for Horner syndrome.
CXR (scapular index), CT chest/shoulder, CTA (vascular injury). MRI delayed for nerve root assessment.
Surgical Technique
Scapulothoracic dissociation requires coordinated multidisciplinary surgical management. Vascular surgery takes priority, with orthopaedic and reconstructive procedures staged appropriately.
- Subclavian artery disruption
- Axillary artery injury
- Active hemorrhage
- Limb ischemia with salvageable limb
- Supraclavicular incision for proximal control
- Infraclavicular/deltopectoral extension as needed
- Median sternotomy for proximal subclavian access (rare)
- Primary repair (rare - usually too damaged)
- Interposition vein graft (saphenous vein)
- Interposition prosthetic graft (PTFE/Dacron)
- Temporary shunting if staged procedures needed
Warm ischemia time of greater than 6 hours results in near 100% amputation rate. Document time of injury and time of revascularization. Fasciotomies may be required after revascularization.
Discussion fixates on the artery, but the subclavian/axillary VEIN is injured in a large proportion of cases and matters for two reasons. First, venous disruption is a major source of the occult haemorrhagic shock that kills these patients - low-pressure but high-volume bleeding into the disrupted shoulder girdle and chest, easily underestimated behind intact skin. Second, the repair principle differs from the artery: a damaged subclavian/axillary vein is usually ligated rather than repaired in the unstable polytrauma patient (ligation is well tolerated because of collateral venous drainage), whereas the artery is repaired/grafted to save the limb. Be alert to venous air embolism if a large central vein is open to atmosphere (place the patient head-down, pack/occlude the wound). So when you say "88 percent vascular injury," remember that means artery AND vein - control both, repair the artery, ligate the vein if needed, and treat the vein as a real contributor to the shock.
Complications
- Incidence
- 21%
- Prevention/Management
- ATLS resuscitation, hemorrhage control
- Incidence
- 10-15%
- Prevention/Management
- May require amputation
- Incidence
- Common
- Prevention/Management
- Pain management, amputation may help
- Incidence
- Risk with revascularization
- Prevention/Management
- Prophylactic fasciotomy
- Incidence
- High
- Prevention/Management
- Staged procedures, VAC therapy
- Incidence
- With soft tissue trauma
- Prevention/Management
- Indomethacin, radiation
After revascularization of an ischemic limb, consider:
- Prophylactic forearm fasciotomy - especially if ischemia time greater than 6 hours
- Monitor for compartment syndrome
- Reperfusion can cause myoglobinuria and acute kidney injury
- Hydration and urine alkalinization may be needed
Postoperative Care and Rehabilitation
Rehabilitation Phases
Hemodynamic monitoring. Wound care. Pain management. Vascular graft surveillance (duplex daily). Limb elevation. Compartment monitoring.
Gentle passive ROM if stable fixation. Edema control. Wound healing. Psychosocial support. Pain team involvement.
Active ROM as nerve function returns. Strengthening as tolerated. Occupational therapy for ADLs. Reassess for nerve reconstruction.
Ongoing therapy. Orthotics/prosthetics if needed. Vocational rehabilitation. Chronic pain management.
- Phase 1 (0-6 weeks): Protect vascular repair, passive ROM
- Phase 2 (6-12 weeks): Active ROM, gentle strengthening
- Phase 3 (3-6 months): Progressive strengthening, functional activities
- Phase 4 (6+ months): Return to modified activities
- Nerve recovery takes 12-18 months
- Motor recovery before sensory
- Therapy focus on available function
Expect nerve regeneration at approximately 1mm/day (1 inch/month). Proximal injuries (brachial plexus level) take 12-18 months to reach distal targets. Recovery is never complete after severe injury.
- Multimodal analgesia
- Neuropathic pain medications (gabapentin, pregabalin)
- Pain team early involvement
- Chronic pain clinic referral
- Consider spinal cord stimulator
- Early psychological assessment
- PTSD screening and treatment
- Peer support programs
- Vocational counseling
- Family support services
Outcomes and Prognosis
- Functional Outcome
- Good
- Notes
- Full recovery expected if fractures heal
- Functional Outcome
- Variable
- Notes
- Depends on neurological recovery
- Functional Outcome
- Variable
- Notes
- Depends on ischemia time and neuro status
- Functional Outcome
- Poor limb function
- Notes
- Amputation often provides better QOL
- Complete brachial plexus avulsion
- Delayed revascularization (greater than 6 hours)
- Associated severe injuries
- Complete flail limb
- Preganglionic injury (Horner syndrome)
- Incomplete plexus injury
- Early revascularization
- Type I (musculoskeletal only)
- Postganglionic injury (repairable)
- Young patient
Guidelines, Registries & Global Practice
Scapulothoracic dissociation is too rare for dedicated society guidelines, randomised trials, or arthroplasty-style registries. The evidence base is small retrospective series and reviews, and management principles are extrapolated from broader trauma frameworks (ATLS / vascular trauma) and brachial plexus injury practice. There is no country-specific "correct" pathway - the priorities below apply worldwide.
- Relevant Principle
- Life-threatening haemorrhage and airway/breathing take priority
- Application to STD
- Resuscitate and control occult chest-wall/neurovascular bleeding before limb surgery
- Relevant Principle
- Damage-control orthopaedics; staged fixation in the unstable polytrauma patient
- Application to STD
- Temporary stabilisation then delayed definitive clavicle/scapula fixation
- Relevant Principle
- Combined ortho-vascular pathway, time-critical revascularisation, fasciotomy after prolonged ischaemia
- Application to STD
- Joint vascular-orthopaedic team; document ischaemia time; low threshold for fasciotomy
- Relevant Principle
- Early specialist referral; staged neurophysiology before reconstruction
- Application to STD
- EMG/NCS at ~3 weeks, plexus reconstruction typically at 3-6 months in a specialist centre
- Consistently rare across all reported series and likely underdiagnosed worldwide
- Affects predominantly young males after high-energy trauma
- Mechanisms vary by region: motorcycle/MVA in most settings; agricultural PTO and industrial traction injuries more prominent in rural and lower-resource settings
- Pooled outcomes (Damschen, n=58): 94% neuro, 88% vascular, 52% flail, 21% amputation, 10% death
- High-resource: CT angiography on demand, 24/7 vascular and microsurgery, hybrid/endovascular options, specialist brachial plexus reconstruction, advanced prosthetics
- Limited-resource: reliance on clinical examination and plain radiographs, longer transfer and ischaemia times, earlier amputation more common, limited access to nerve reconstruction and prosthetic services
- Universal priorities: early recognition, haemorrhage control, timely revascularisation of the salvageable limb, and honest shared decision-making for the flail limb
Any suspected scapulothoracic dissociation should be transferred to a major trauma centre with:
- Level 1 trauma capability
- Vascular surgery available around the clock
- Microsurgery / plastics capability
- Critical care capacity
- Access to brachial plexus reconstruction expertise (often at a regional specialist centre)
Controversies and Areas of Uncertainty
- Multiple competing schemes exist (Oreck radiographic, Damschen spectrum, Zelle neurology-based)
- No system is prospectively validated
- Zelle (Level II evidence) argues neurological status, not vascular status, should define severity
- For exams, name Damschen as most-cited but acknowledge the limitation
- Some advocate early above-elbow amputation for the confirmed flail limb (Clements; Brucker)
- Others favour limb preservation with delayed, patient-led decision-making
- No comparative trial exists; the choice is shared and value-laden
- Phantom and neuropathic pain occur with either pathway
- A ratio greater than 1.0 is abnormal, but the exact diagnostic cut-off is debated
- Patient rotation on the film readily produces false asymmetry
- Zelle found the index did NOT predict functional outcome - it is diagnostic, not prognostic
- Hybrid/endovascular techniques for subclavian-axillary injury are emerging in case reports
- Evidence is limited to small series; open repair remains the default for unstable patients
- Decisions should involve vascular surgery early
MCQ Practice Points
- Key Point
- Greater than 1.0 = positive
- Exam Trap
- Don't confuse with absolute measurement
- Key Point
- Damschen I/IIA/IIB/III
- Exam Trap
- Know all 4 types and what distinguishes them
- Key Point
- T1 avulsion (preganglionic)
- Exam Trap
- Indicates poor prognosis - NOT repairable
- Key Point
- Indicates avulsion NOT rupture
- Exam Trap
- Counter-intuitive finding
- Key Point
- ATLS resuscitation
- Exam Trap
- NOT immediate surgery for the limb
Q: A patient with complete brachial plexus injury undergoes nerve conduction studies at 4 weeks. SNAP is preserved. What does this indicate?
A: Preganglionic avulsion injury (NOT repairable). When SNAP is preserved despite clinical sensory loss, it indicates the dorsal root ganglion is intact but disconnected from the spinal cord. The sensory nerve still conducts because the injury is proximal to the ganglion. This is counter-intuitive but a classic exam question.
Q: What chest X-ray finding suggests scapulothoracic dissociation?
A: Scapular index greater than 1.0 (lateral scapular displacement). Calculate by comparing the distance from spine to medial scapular border on injured vs uninjured side. A ratio greater than 1.0 indicates abnormal lateral displacement of the injured scapula.
Q: A polytrauma patient has ptosis, miosis, and anhidrosis on one side. Which brachial plexus root avulsion does this suggest?
A: T1 avulsion (preganglionic). Horner syndrome indicates disruption of sympathetic fibers traveling through T1. This is a poor prognostic sign indicating preganglionic injury (not surgically repairable). It suggests high-energy mechanism with severe nerve damage.
Q: A patient presents with suspected scapulothoracic dissociation after a motorcycle accident. What is the first management priority?
A: ATLS resuscitation - Life before Limb. These injuries have 21% mortality from associated vascular injury and hemorrhagic shock. After stabilization, address vascular emergency (subclavian/axillary artery) before definitive orthopaedic management.
Q: What distinguishes Damschen Type IIA from Type IIB scapulothoracic dissociation?
A: Vascular status. Both have neurological injury, but Type IIA has intact vascular supply while Type IIB has vascular injury requiring repair. Type I has musculoskeletal injury only, Type III has complete flail limb (complete vascular + neurological disruption).
Q: A Type III scapulothoracic dissociation results in a 'flail limb'. What management options should be discussed with the patient?
A: Limb preservation vs forequarter amputation. A flail limb has no motor or sensory function. Many patients ultimately choose amputation because it: eliminates a painful non-functional limb, improves quality of life, reduces infection/wound risks. Patient autonomy is paramount - amputation should be discussed but never mandated.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old motorcyclist is brought to ED after high-speed collision. His left arm is massively swollen and hangs flaccid. There are no pulses in the left upper limb and complete motor/sensory loss. CXR shows lateral displacement of the left scapula. How do you proceed?”
“Describe the scapular index and how you would calculate it on a chest X-ray. What is the diagnostic threshold?”
“A patient with Type III scapulothoracic dissociation asks about the option of keeping his arm versus amputation. How would you counsel him?”
Key Numbers
- Scapular Index greater than 1.0 = positive diagnosis
- 94% have brachial plexus injury
- 88% have vascular injury
- 21% mortality rate
- 6 hours ischemia threshold for poor outcomes
Diagnosis
- High-energy traction mechanism (motorcycle, MVA)
- Massive shoulder girdle swelling
- Lateral scapular displacement (scapular index)
- Absent/diminished distal pulses
- Brachial plexus deficit (C5-T1)
Damschen Classification
- Type I: Musculoskeletal injury only
- Type IIA: Neuro injury, vascular intact
- Type IIB: Neuro + vascular injury
- Type III: Complete flail limb (total disruption)
Management Priorities
- ATLS resuscitation (Life before Limb)
- CTA for vascular assessment
- Emergent revascularization if ischemic
- Document neuro status before intervention
- Type III: Discuss forequarter amputation
High-Yield Exam Points
- Preserved SNAP = preganglionic avulsion (NOT repairable)
- Horner syndrome = T1 avulsion (poor prognosis)
- Complete plexus avulsion = consider amputation
- Know scapular index calculation method
Evidence Base
Original radiographic description of lateral scapular displacement
- Three cases with radiographic and pathological evidence of complete scapulothoracic disruption without an overlying open wound.
- Established lateral scapular displacement with AC separation as the defining radiographic sign, with associated brachial plexus and subclavian artery/vein injury.
- Coined the recognition that the injury may be missed in the multiply-injured patient, with potentially fatal consequences.
Scapulothoracic dissociation caused by blunt trauma (landmark spectrum/classification series)
- Four institutional cases plus 54 adequately described literature cases (n=58).
- Neurologic injury in 94% and vascular injury in 88%.
- Flail extremity in 52%, early amputation in 21%, and death in 10%.
- Defined a broader spectrum of injury and a rational, severity-based approach to diagnosis and intervention.
Functional outcome following scapulothoracic dissociation
- 25 patients over 24 years; mean ISS 22; mean follow-up 12.6 years.
- Subjective Shoulder Rating System 33.8 (complete plexus avulsion) versus 72.5 (no/incomplete avulsion), p=0.046; SF-36 physical and mental scores also significantly lower with complete avulsion.
- Mean scapula index 1.29; initial index did NOT correlate with functional scores.
- Proposed modifying classification so that complete brachial plexus avulsion defines the most severe injury type.
Newly recognised variant and a new classification with review of treatment options
- Described scapulothoracic dissociation with sternoclavicular separation (a previously unreported radiographic combination) and an isolated, non-polytrauma case.
- Reviewed treatment options including amputation, shoulder arthrodesis, prosthetic fitting and reconstructive tendon transfers.
- Characterised the injury as a closed complete traumatic forequarter amputation with a flail pulseless arm.
Above-elbow amputation recommended for the flail extremity
- Defining constellation: subclavian/axillary vascular disruption, lateral scapular displacement, clavicular articulation separation, and cervical root avulsion or plexus injury.
- Recommended orthopaedic stabilisation, vascular repair and brachial plexus exploration.
- Advocated above-elbow amputation, either primarily or within 24 hours, for the flail extremity.
Level of vascular insult as a prognostic indicator
- 8 institutional cases plus 37 from the literature (n=45).
- Subclavian artery injury was associated more often with COMPLETE brachial plexus involvement; axillary artery injury with PARTIAL plexus injury (p less than 0.05).
- The more proximal the vascular injury, the more severe the neurological damage.
Scapulothoracic dissociation: evaluation and management (review)
- Synthesised the small case-series literature on evaluation, management and functional outcome.
- Emphasised timely diagnosis of neurovascular injury, with early above-elbow amputation for severe neurovascular and soft-tissue compromise.
- Complete brachial plexus avulsions carry limited potential for functional recovery.
Scapulothoracic dissociation: evaluation and management (AAOS review)
- Emergent surgery is reserved for limb-threatening ischaemia or active arterial haemorrhage; neurologic management can be delayed.
- Diagnosis relies on the scapular index on a non-rotated chest radiograph plus a distracted clavicle fracture or AC/SC disruption.
- Outcome is determined by the extent of neurological injury; SF-36 scores are significantly lower with complete plexus avulsion than postganglionic injury.