Thread Geometry | Pullout Strength | Lag Technique | Locking vs Non-Locking
- Pullout strength depends on thread engagement, bone density, and outer diameter
- Lag screw technique achieves compression through threads in far cortex only
- Thread pitch is distance between adjacent threads; lead is axial advance per rotation
- Core diameter determines bending and torsional strength of screw
- Locking screws create fixed-angle construct eliminating screw-plate toggling
- “70% of pullout strength comes from threads engaging outer cortex
- “Stripping torque proportional to outer diameter cubed and bone density
- “Lag screws require gliding hole and thread hole for compression
- “Locking screws function as internal fixator with reduced periosteal compression
Pitch vs Lead distinction: Pitch is distance between threads. Lead is axial advance per rotation. Single-lead screw: pitch equals lead. Dual-lead screw: lead is twice pitch. Thread depth and angle determine holding power.
Pullout force proportional to outer diameter, thread engagement length, and bone density. 70% of strength from outer cortex. Bicortical fixation provides 2-3 times strength of unicortical fixation.
Lag technique creates interfragmentary compression. Gliding hole allows screw shaft to pass freely. Threads engage far cortex only. Tightening pulls far fragment toward near fragment. No compression without gliding hole.
Locking screws thread into plate holes creating fixed-angle construct. Eliminates toggling and periosteal stripping. Acts as internal fixator. Angular stability independent of bone quality but requires precise insertion.
Overview
Screws are the fundamental fixation device in orthopaedic surgery, converting rotational torque into axial advancement and fixation force. Understanding screw biomechanics is essential for optimal implant selection, insertion technique, and construct stability.
Why screw biomechanics matters clinically:
Screw pullout or loosening is a common mode of fixation failure. Understanding the biomechanical principles of thread engagement, bone density effects, and optimal screw selection prevents clinical failure.
Lag screw technique for interfragmentary compression, locking versus non-locking screw selection, and bicortical versus unicortical fixation all depend on biomechanical principles. Improper technique compromises stability.
Screws function in three mechanical modes: 1) Position screws hold fragments in reduced position without compression (threads engage both fragments equally). 2) Lag screws generate interfragmentary compression (threads engage far fragment only). 3) Locking screws create fixed-angle construct (threaded head locks to plate). Understanding these modes is fundamental to screw selection.
Concepts and Mechanisms
Understanding screw anatomy is essential for biomechanical analysis.
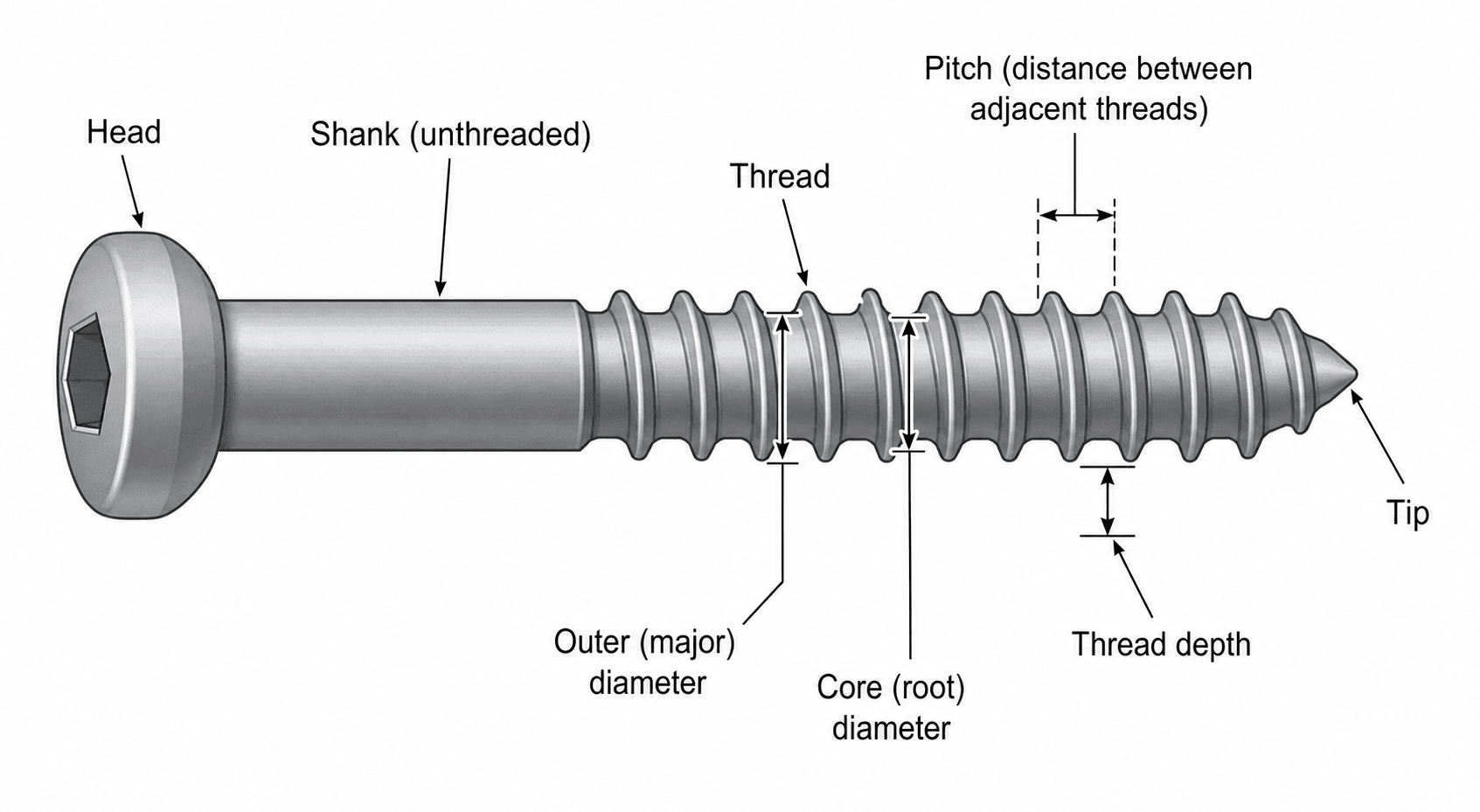
Anatomical Components of a Screw
Head:
- Transfers torque from driver to screw
- Compression surface (countersunk or buttress)
- May have threads (locking screws) or smooth (non-locking)
Shaft (Shank):
- Core diameter determines bending and torsional strength
- May be threaded (fully threaded) or smooth (partially threaded)
- Smooth shaft allows gliding for lag technique
Threads:
- External (outer) diameter determines thread contact area
- Core (root) diameter at base of threads
- Thread depth = (outer diameter - core diameter) / 2
- Thread angle typically 40-60 degrees
Tip:
- Self-tapping screws cut their own threads
- Non-self-tapping require pre-tapping
- Trocar (sharp) or blunt tip designs
Understanding each component is critical for biomechanical analysis and screw selection.
Pullout Strength and Failure Mechanisms
Pullout strength is the force required to extract a screw from bone and represents the primary mode of fixation failure in many constructs.
Factors Determining Pullout Strength
Screw factors:
-
Outer diameter (most important screw factor)
- Pullout force proportional to outer diameter
- Doubling diameter approximately doubles pullout strength
- Thread surface area increases with diameter
-
Thread engagement length
- Linear relationship with pullout strength
- 70% of strength from outer cortex in bicortical fixation
- Minimum 3-4 threads required for adequate purchase
-
Thread geometry
- Thread depth increases surface area
- Thread angle affects stripping resistance
- Pitch determines number of engaged threads per unit length
Bone factors:
-
Bone density (most important bone factor)
- Cortical bone: 3-4 times stronger than cancellous
- Osteoporotic bone: 50-70% reduction in pullout strength
- Proportional relationship with BMD
-
Thread engagement location
- Outer cortex provides 70% of pullout strength
- Near cortex engagement critical
- Far cortex adds 30% in bicortical fixation
Understanding these factors allows optimization of fixation strength.
Lag Screw Biomechanics and Technique
Lag screws generate interfragmentary compression, the gold standard for fracture fixation when anatomic reduction and absolute stability are desired.
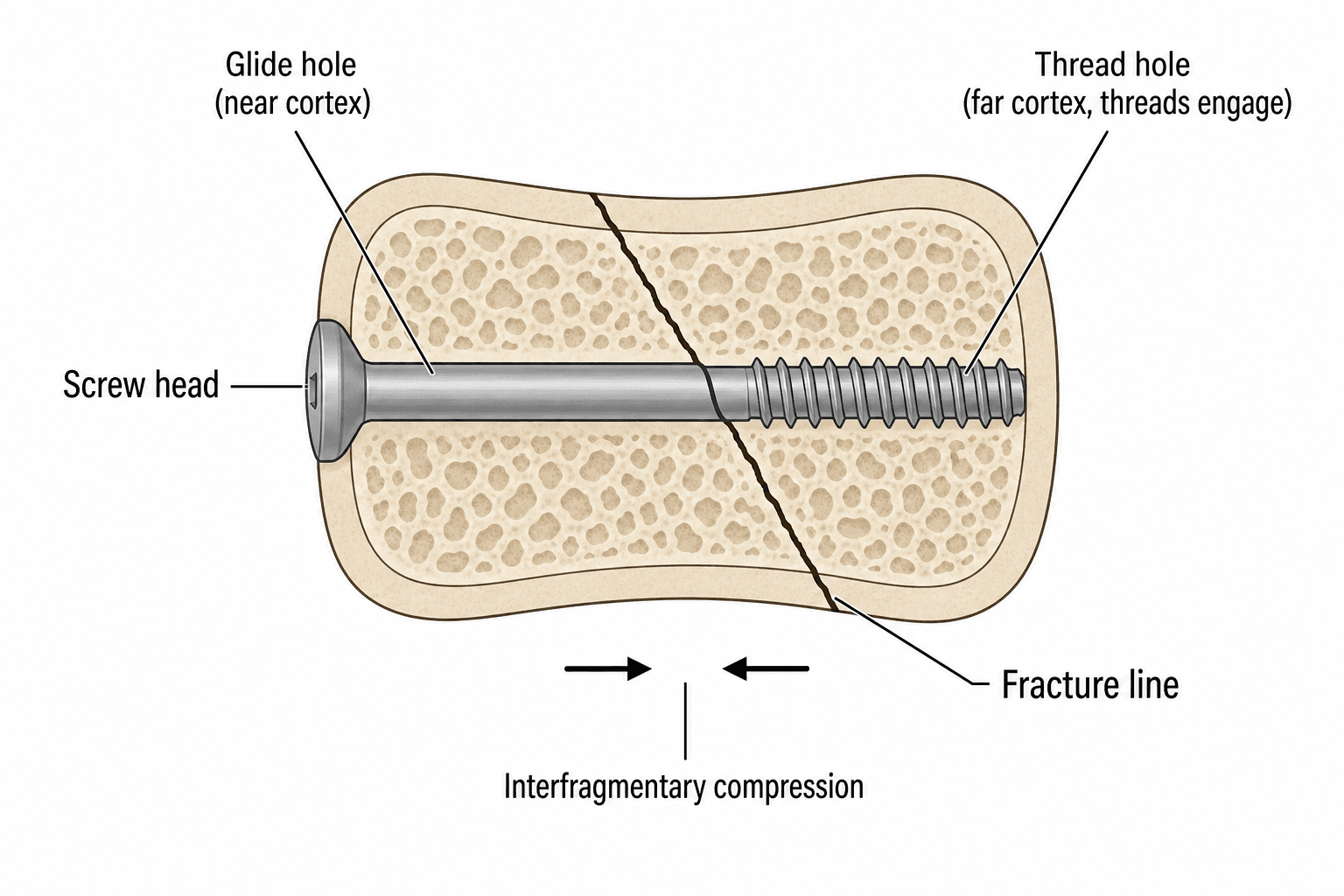
Biomechanical Principle of Lag Screws
Definition: A lag screw achieves compression by engaging threads in the far cortex/fragment only, while allowing the screw shaft to glide freely through the near cortex/fragment.
Mechanism:
-
Gliding hole drilled in near cortex/fragment
- Diameter equals or slightly exceeds screw outer diameter
- Allows screw shaft to pass without thread engagement
- No purchase in near fragment
-
Thread hole drilled in far cortex/fragment
- Diameter equals screw core diameter
- Threads cut into bone during insertion
- Provides purchase for compression
-
Compression generation:
- Screw head contacts near fragment
- Threads pull far fragment toward near fragment
- Continued tightening increases compression force
- Friction at fracture site provides stability
A screw only functions as lag screw if gliding hole is created. Without gliding hole, threads engage both fragments equally (position screw), preventing compression. This is the most tested concept about lag screws. Examiners often ask what happens if you forget the gliding hole.
The lag screw principle converts rotational torque into compressive force across fracture.
Anatomy
Screw Design and Structural Components
Key Screw Anatomy
- Head: Engages plate or countersinks into bone (hex, cruciate, star drive)
- Shaft/Core: Determines bending and torsional strength
- Thread: Engages bone, determines pullout strength
- Tip: Self-drilling, self-tapping, or blunt
Critical Dimensions
- Outer diameter: Thread peak-to-peak, determines pullout strength
- Core diameter: Shaft diameter, determines bending strength
- Pitch: Distance between threads, affects bone engagement
- Thread depth: (Outer - Core)/2, affects holding power
Thread Geometry
- V-thread: Standard, good general properties
- Buttress thread: Asymmetric, better axial pullout resistance
- Hi-Low thread: Variable thread depth, combines cortical and cancellous properties
Classification
Classification of Orthopaedic Screws
By Bone Type
- Cortical Screw
- Fine (closely spaced)
- Cancellous Screw
- Coarse (widely spaced)
- Cortical Screw
- Shallow
- Cancellous Screw
- Deep
- Cortical Screw
- Larger relative to outer
- Cancellous Screw
- Smaller relative to outer
- Cortical Screw
- Diaphyseal cortical bone
- Cancellous Screw
- Metaphyseal/epiphyseal bone
By Function
- Lag screw: Creates interfragmentary compression
- Position screw: Maintains position without compression
- Locking screw: Creates fixed-angle construct with plate
Investigations
Testing Methods for Screw Biomechanics
Mechanical Testing
- Pullout testing: Axial load to failure, measures screw-bone interface strength
- Insertion torque: Resistance during insertion, correlates with pullout
- Stripping torque: Maximum torque before thread failure
- Bending testing: Four-point bending to assess screw strength
Imaging Assessment
- Plain radiographs: Screw position, backing out, lucency around threads
- CT scan: Detailed assessment of screw purchase, cortical breach
- Fluoroscopy: Intraoperative confirmation of trajectory and depth

Headless Compression Screws and the Differential-Pitch Principle
The classification sections name the Herbert screw and "variable thread pitch... headless compression screws", but never explain how a screw with no head generates compression. This differential-pitch principle is a recurring basic-science viva question.
A headless compression screw is buried entirely beneath the articular or cortical surface, so it can cross a joint surface or fix a small bone without a prominent head to impinge. It generates interfragmentary compression by differential (variable) pitch: the leading (far) threads are coarser - they advance further per turn - than the trailing (near) threads, so as the screw is driven the far fragment is pulled toward the near fragment and the gap closes, producing compression along the screw without any head pressing on the cortex.
- Lag (headed) screw
- Screw head pressing the near fragment while threads pull the far fragment (needs a gliding hole)
- Headless differential-pitch screw
- Coarser leading threads advance the far fragment faster than the finer trailing threads, drawing the fragments together
- Lag (headed) screw
- Prominent head must seat on or in the cortex
- Headless differential-pitch screw
- Buried below the articular/cortical surface (headless) - no impingement
- Lag (headed) screw
- Diaphyseal/metaphyseal fragments where a head can sit
- Headless differential-pitch screw
- Small-bone and intra-articular fixation (scaphoid, osteochondral fragments, small-joint arthrodesis)
- Lag (headed) screw
- Titrated by the surgeon's feel on the head
- Headless differential-pitch screw
- Largely fixed by the design; both thread zones must gain purchase
A headless compression screw generates interfragmentary compression by DIFFERENTIAL PITCH - the leading threads are coarser (advance further per turn) than the trailing threads, so the far fragment is drawn toward the near fragment as the screw is driven, closing the gap without any head pressing on the cortex. This is fundamentally different from a lag screw (which needs a head plus a gliding hole). Being headless and buried beneath the articular surface, it suits the scaphoid, osteochondral fragments and small-joint fixation, but the compression it delivers is largely set by the design rather than titrated by the surgeon, and both fragments must be engaged by the differently-pitched thread zones.
Cortical versus Cancellous Screws
Screw design optimized for bone type improves fixation strength and reduces complications.
- Cortical Screw
- Fine (1.0-1.5 mm)
- Cancellous Screw
- Coarse (2.5-3.0 mm)
- Cortical Screw
- Shallow (0.5 mm)
- Cancellous Screw
- Deep (1.0-1.5 mm)
- Cortical Screw
- 70-80% of outer diameter
- Cancellous Screw
- 50-60% of outer diameter
- Cortical Screw
- High (7-10)
- Cancellous Screw
- Low (3-4)
- Cortical Screw
- Cortical bone, diaphyses, plates
- Cancellous Screw
- Cancellous bone, metaphyses, epiphyses
- Cortical Screw
- Higher in cortical bone
- Cancellous Screw
- Lower but adequate in trabecular bone
- Cortical Screw
- Higher (requires tapping often)
- Cancellous Screw
- Lower (usually self-tapping)
Biomechanical rationale for design differences:
Cortical screws:
- Fine pitch maximizes number of engaged threads in dense bone
- Shallow threads maintain larger core diameter for strength
- High thread count distributes force over more bone-screw interface
- Dense cortical bone provides high pullout strength per thread
- Examples: 3.5mm and 4.5mm cortical screws for plate fixation
Cancellous screws:
- Coarse pitch allows deeper penetration into trabecular bone
- Deep threads increase thread surface area in porous bone
- Larger thread spacing engages more trabeculae per thread
- Trabecular bone requires larger thread area for equivalent strength
- Examples: 6.5mm and 7.3mm cancellous screws for metaphyseal fixation
Using cortical screw in cancellous bone results in inadequate thread engagement (fine threads between trabeculae, not engaging). Using cancellous screw in cortical bone difficult to insert (coarse threads require high torque, large core reduces penetration). Match screw design to bone type for optimal fixation.
Understanding design differences enables appropriate screw selection for each clinical situation.
Cannulated Screw Biomechanics
The topic refers to cannulated screws repeatedly (guidewire placement, 6.5mm and 7.3mm designs, the cannulated technique) but never addresses the biomechanical trade-off of making a screw hollow.
A cannulated screw has a hollow axial core so it can be railed over a pre-placed guidewire, giving accurate, reproducible and percutaneous placement where the trajectory is critical. The cost is a small reduction in strength.
- Solid screw
- Free-hand trajectory
- Cannulated screw
- Passed over a pre-placed guidewire - accurate, reproducible, percutaneous
- Solid screw
- Higher for a given outer diameter
- Cannulated screw
- Slightly reduced (central core removed), but the penalty is modest - see pearl
- Solid screw
- Set by outer diameter and thread engagement
- Cannulated screw
- Essentially preserved (pullout is a thread-bone property, not a core property)
- Solid screw
- General fixation
- Cannulated screw
- Trajectory-critical or percutaneous fixation (femoral neck, scaphoid, SCFE, sacroiliac)
A cannulated screw is hollow so it can be railed over a guidewire, giving accurate, reproducible and percutaneous placement where trajectory matters - the femoral neck, scaphoid, SCFE and sacroiliac joint. The hollow core does reduce bending, torsional and fatigue strength relative to a SOLID screw of the same outer diameter, but the penalty is modest: bending stiffness rises steeply with radius (with the fourth power), and the central core is the lowest-stressed material, so removing it costs relatively little, while pullout - a thread-bone property - is essentially preserved. Manufacturers often make cannulated designs a touch larger in diameter to offset the difference; the practical cautions are guidewire bending, inadvertent advancement or breakage during drilling.
Locking versus Non-Locking Screws
Locking screw technology revolutionized fracture fixation by creating fixed-angle constructs with angular stability.
Biomechanical Principle of Locking Screws
Locking screw definition: Screw head has threads that engage matching threads in plate hole, creating fixed-angle construct where screw cannot toggle or back out.
Mechanism of angular stability:
- Threaded screw head engages threaded plate hole
- Fixed angle between screw and plate (typically perpendicular)
- No toggling - screw cannot change angle relative to plate
- Load transfer through screw-plate interface, not friction
- Internal fixator principle - plate spans fracture without compressing periosteum
Comparison to conventional (non-locking) screws:
- Non-Locking
- Friction (compression)
- Locking
- Thread engagement (fixed)
- Non-Locking
- No (screw can toggle)
- Locking
- Yes (fixed angle)
- Non-Locking
- Required (friction)
- Locking
- Not required (bridge)
- Non-Locking
- Yes (may devascularize)
- Locking
- No (preserves perfusion)
- Non-Locking
- High (relies on pullout)
- Locking
- Lower (angular stability)
- Non-Locking
- Tolerant of angle variation
- Locking
- Requires precise perpendicular insertion
The locking mechanism creates fundamentally different biomechanics from conventional screws.
Management
Screw Selection Principles
Matching Screw to Bone Type
- Cortical bone: Cortical screws, bicortical purchase when possible
- Cancellous bone: Cancellous screws, maximize thread engagement
- Osteoporotic bone: Locking screws, consider augmentation
Matching Screw to Fixation Strategy
- Compression fixation: Lag screws (partially threaded or lag technique)
- Bridging fixation: Locking screws, position screws
- Angular stability needed: Locking plate-screw constructs
Screw Length Selection
- Measure depth accurately (depth gauge)
- Bicortical when strength needed
- Avoid excessive protrusion (soft tissue irritation)
Surgical Technique
Screw Insertion Technique
Standard Screw Insertion Steps
- Drill pilot hole (appropriate drill bit for screw core diameter)
- Measure depth with depth gauge
- Tap hole (if not self-tapping)
- Insert screw to appropriate torque
Lag Screw Technique (Fully Threaded Screw)
- Position fragments anatomically
- Drill glide hole through near cortex (same as screw outer diameter)
- Drill pilot hole through far cortex (same as screw core diameter)
- Countersink if needed
- Measure and insert screw - compression achieved
Key Technical Points
- Drill perpendicular to fracture plane for optimal compression
- Avoid heat generation (use sharp drills, irrigation)
- Don't overtighten (strips threads in osteoporotic bone)
Complications
Screw-Related Complications
Thread Stripping
- Occurs when insertion torque exceeds bone purchase capacity
- More common in osteoporotic bone
- Prevention: Stop at appropriate torque, avoid overtightening
- Salvage: Larger diameter screw, cement augmentation, alternative fixation point
Screw Pullout
- Loss of purchase due to cyclic loading exceeding pullout strength
- Risk factors: Osteoporosis, unicortical fixation, short screws
- Prevention: Maximize thread engagement, bicortical fixation, locking screws
Screw Breakage
- Failure at stress concentration points (thread-shaft junction)
- Fatigue failure from cyclic loading
- Risk factors: Delayed union, high activity level, inadequate construct stability
Hardware Prominence
- Screws too long or incorrect angle
- Causes soft tissue irritation, tendon damage
- Prevention: Accurate measurement, fluoroscopic confirmation
Postoperative Care
Postoperative Considerations
Weight-Bearing Progression
- Based on construct stability, fracture pattern, and bone quality
- Locking constructs may allow earlier weight-bearing in osteoporotic bone
- Lag screw fixation requires protected weight-bearing until healing
Radiographic Monitoring
- Serial X-rays to assess fracture healing and implant position
- Watch for screw loosening (lucency around screw threads)
- Assess for hardware migration or breakage
Activity Modifications
- Restrict high-impact activities during healing phase
- Gradually progress based on radiographic and clinical progress
- Consider patient factors: age, bone quality, compliance
Hardware Concerns to Monitor
- Screw prominence causing soft tissue irritation
- Signs of loosening or migration
- Symptoms suggesting hardware failure
Outcomes
Fixation Outcomes
Factors Affecting Screw Fixation Success
- Bone quality: Osteoporotic bone has 50-70% reduced pullout strength
- Surgical technique: Proper drilling, tapping, and insertion torque
- Construct design: Appropriate screw selection for application
- Patient factors: Compliance, comorbidities, smoking status
Union Rates by Fixation Type
- Lag screw fixation: 90-95% union for simple fractures
- Plate fixation (conventional): 85-95% depending on fracture pattern
- Locking plate fixation: Similar union rates, advantageous in osteoporotic bone
Hardware Removal Rates
- Overall symptomatic hardware: 5-15%
- Higher in subcutaneous locations (ankle, wrist, clavicle)
- Locking screws may have higher removal difficulty
Clinical Relevance and Applications
Screw selection depends on fracture pattern, bone quality, fixation goals, and anatomic location.
- Optimal Screw Choice
- Cortical lag screw through plate
- Rationale
- Compression with adequate pullout strength in cortical bone
- Optimal Screw Choice
- Locking screws, bridge plate
- Rationale
- Angular stability without compression of fragments
- Optimal Screw Choice
- Locking screws with cement augmentation
- Rationale
- Fixed-angle support with enhanced pullout in weak bone
- Optimal Screw Choice
- Partially threaded cancellous lag screw
- Rationale
- Maximum compression with lag by design
- Optimal Screw Choice
- Locking screws, bypass fixation
- Rationale
- Avoid stress risers near prosthesis, maintain stability
- Optimal Screw Choice
- Smooth pins or small cortical screws
- Rationale
- Avoid crossing physis, adequate strength in young bone
Two fundamental fixation strategies: 1) Absolute stability with compression (lag screws, compression plates) for simple fractures with good bone contact. 2) Relative stability with bridging (locked plates, external fixators) for comminuted fractures or osteoporotic bone. Screw choice follows fixation strategy: lag screws for compression, locking screws for bridging.
- Prefer locking screws for angular stability
- Consider cement augmentation for critical screws
- Maximize screw length and bicortical purchase
- Avoid compression (risk of fragmentation)
- Use plates with greater working length (distribute stress)
- Bridge plating to preserve soft tissue and biology
- Locking screws for angular stability across comminution
- Minimize periosteal stripping (use locked plates as internal fixators)
- Consider lag screws for main fragments only
- Leave comminuted zone unfixed (allow callus formation)
Guidelines, Registries & Global Practice
Why Screw Biomechanics Matters Globally
Internal fixation with screws is among the most frequently performed orthopaedic interventions worldwide, and the burden is rising with an ageing, increasingly osteoporotic population. Fragility fractures of the hip, pelvis, distal radius, proximal humerus and ankle dominate the elderly trauma workload, and these are precisely the metaphyseal, low-density sites where screw purchase is most marginal and where locking and augmentation strategies are most often required.
Population drivers of fixation difficulty
- Fall-related fractures are increasing across most adult age ranges, not only the very elderly, with the steepest relative rises in younger women and in men over 80. [1]
- Osteopenic bone already reduces screw pullout strength to roughly three-quarters of normal, so the at-risk population extends well beyond those with established osteoporosis. [2]
- Bone mineral density is the single most important patient determinant of screw holding power across cortical, cancellous and pedicle screw studies. [2]
Because the underlying physics of thread engagement, compression and angular stability are universal, screw biomechanics is examined in essentially identical form across FRCS (Tr & Orth), FRACS, EBOT, ABOS, DNB and SICOT boards.
References
- Court-Brown CM, Clement ND, Duckworth AD, Biant LC, McQueen MM. The changing epidemiology of fall-related fractures in adults. Injury. 2017;48(4):819-824. doi:10.1016/j.injury.2017.02.021
- Lee SJ, Lee JH, Lee HJ, Oh JW, Park IH. Pullout strength of pedicle screws using cadaveric vertebrae with or without artificial demineralization. Spine J. 2021;21(9):1580-1586. doi:10.1016/j.spinee.2021.04.010
- Yerby S, Scott CC, Evans NJ, Messing KL, Carter DR. Effect of cutting flute design on cortical bone screw insertion torque and pullout strength. J Orthop Trauma. 2001;15(3):216-221. doi:10.1097/00005131-200103000-00012
- Stoffel K, Dieter U, Stachowiak G, Gachter A, Kuster MS. Biomechanical testing of the LCP - how can stability in locked internal fixators be controlled? Injury. 2003;34(Suppl 2):B11-19. doi:10.1016/j.injury.2003.09.021
- Perren SM. Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation. J Bone Joint Surg Br. 2002;84(8):1093-1110. doi:10.1302/0301-620X.84B8.13752
- Konig A, Oberkircher L, Beeres FJP, Babst R, Ruchholtz S, Link BC. Cement augmentation of sacroiliac screws in fragility fractures of the pelvic ring. Injury. 2019;50(8):1411-1417. doi:10.1016/j.injury.2019.06.025
- Schatzker J, Sanderson R, Murnaghan JP. The holding power of orthopedic screws in vivo. Clin Orthop Relat Res. 1975;(108):115-126. doi:10.1097/00003086-197505000-00019
MCQ Practice Points
Q: What are the key design parameters of a screw that affect its holding power?
A: (1) Outer diameter: Larger = more bone contact, greater pullout resistance. (2) Root diameter (core): Determines bending/torsional strength. (3) Pitch: Distance between threads; smaller pitch = more threads per unit length. (4) Thread depth: Outer minus root diameter; deeper = more purchase. (5) Thread profile: Buttress, V-thread, asymmetric designs. Pullout strength proportional to thread depth × thread length × bone density.
Q: What is the difference between cortical and cancellous screws?
A: Cortical screws: Smaller pitch (more threads/cm), smaller thread depth, fully threaded, designed for dense cortical bone. Cancellous screws: Larger pitch, deeper threads, often partially threaded, designed for trabecular bone. Cancellous screws have larger outer:core ratio for better purchase in soft bone. Partially threaded cancellous screws allow lag effect.
Q: What is the mechanism of lag screw fixation?
A: Lag technique creates interfragmentary compression. Mechanism: Threads engage only the far cortex (glide hole in near cortex), as screw is tightened, the head compresses fragments together. Can be achieved with: (1) Partially threaded screw (thread length shorter than fracture gap), or (2) Fully threaded screw with overdrilled glide hole. Compression generates friction resistance to shear.
Q: What is the relationship between screw insertion torque and pullout strength?
A: Insertion torque does NOT equal pullout strength. Insertion torque: Rotational force to advance screw (friction-dependent). Pullout strength: Axial force to extract screw (thread engagement in bone). Overtightening (excessive torque) can strip threads, reducing pullout strength. Optimal insertion: "Hand-tight" feel. Self-tapping screws have lower insertion torque than non-self-tapping.
Q: How do locking screws differ from conventional screws biomechanically?
A: Conventional screws: Compression between plate and bone, friction-based stability, pullout depends on bone quality, toggle under load. Locking screws: Threaded head locks to plate (fixed-angle construct), load shared across all screws, no plate-bone compression needed, better in osteoporotic bone. Locking construct acts as internal fixator. Disadvantage: Cannot achieve interfragmentary compression.
At a Glance
Screw pullout strength depends on thread engagement length, bone density, and outer (major) diameter—70% of pullout strength comes from outer cortex engagement alone. Pitch is the distance between adjacent threads; lead is axial advance per rotation. Core (root) diameter determines bending and torsional strength. Cortical screws have fine pitch (1.0-1.5mm) and shallow threads for dense bone; cancellous screws have coarse pitch (2.5-3.0mm) and deep threads for trabecular bone. Lag screw technique achieves interfragmentary compression: the gliding hole (outer diameter) allows shaft passage while threads engage only the far cortex, pulling fragments together. Locking screws thread into plate holes creating fixed-angle constructs that eliminate toggling and periosteal compression—acting as internal fixators independent of bone quality.
SCREWSCREW - Biomechanical Principles
Hook:SCREW mechanics: core for strength, cortex for pullout, outer diameter matters most
PITCHPITCH - Thread Geometry
Hook:PITCH determines insertion efficiency and bone engagement in screw design
LAGLAG - Interfragmentary Compression
Hook:LAG technique requires three elements: gliding hole, thread purchase, and gap closure
Basic Science Viva Scenarios
Practise clinical reasoning and management decisions out loud
“Explain the factors that determine screw pullout strength and how you would optimize fixation in osteoporotic bone.”
“You are fixing a simple oblique diaphyseal fracture. Explain the biomechanical principle of lag screw technique and describe how to achieve compression with a fully threaded screw.”
“Compare the biomechanics of locking and non-locking screws. When would you choose each type and what are the potential complications of locking screws?”
Screw Anatomy
- Core diameter: determines bending and torsional strength
- Outer diameter: determines pullout strength (thread contact area)
- Pitch: distance between threads (1.0-1.5mm cortical, 2.5-3.0mm cancellous)
- Lead: axial advance per rotation (equals pitch for single-lead screws)
- Thread depth: (outer - core diameter) / 2 (shallow cortical, deep cancellous)
Pullout Strength Factors
- Outer diameter (most important screw factor) - proportional to thread area
- Thread engagement length - linear relationship with pullout force
- 70% from outer cortex, 30% from far cortex (bicortical fixation)
- Bone density (most important bone factor) - cortical 3-4x cancellous
- Bicortical fixation: 2-3x strength of unicortical
- Osteoporotic bone: 50-70% reduction in pullout strength
Lag Screw Principle
- Compression via threads engaging far cortex only
- Gliding hole (near cortex): diameter = screw outer diameter
- Thread hole (far cortex): diameter = screw core diameter
- No gliding hole = no compression (becomes position screw)
- Lag by design: partially threaded screw (smooth shaft glides)
- Lag by technique: fully threaded screw with deliberate gliding hole
Cortical vs Cancellous Screws
- Cortical: fine pitch (1.0-1.5mm), shallow threads, 70-80% core/outer ratio
- Cancellous: coarse pitch (2.5-3.0mm), deep threads, 50-60% core/outer ratio
- Cortical: diaphyseal, plate fixation, high pullout in dense bone
- Cancellous: metaphyseal, epiphyseal, deep threads engage trabeculae
- Wrong type = poor fixation (cortical in cancellous, cancellous in cortical)
Locking vs Non-Locking
- Non-locking: friction-based, screw toggles, plate-bone compression
- Locking: threaded head-plate interface, fixed angle, angular stability
- Locking advantages: osteoporotic bone, comminution, periosteum preservation
- Locking complications: cross-threading, cold welding, locks malreduction
- Non-locking advantages: compression (lag), angle adjustment, cost
- Achieve perfect reduction BEFORE locking screws (cannot adjust after)
Clinical Applications
- Simple fracture, good bone: non-locking with lag compression
- Comminuted metaphyseal: locking screws, bridge plating
- Osteoporotic periarticular: locking screws with cement augmentation
- Periprosthetic: locking screws, bypass fixation
- Hybrid constructs: lag screws for main fragments, locking for metaphyses
- Bicortical when safe: 2-3x strength, need 3-4 threads beyond far cortex
Evidence Base
The Holding Power of Orthopaedic Screws In Vivo
- Classic in vivo push-out study of screws implanted for 3 months in a canine model
- Self-tapping and non-self-tapping screws of similar material and size maintained comparable holding power at all intervals tested
- Largest screw (4.5mm AO cortical) provided the greatest safety factor against push-out in the unloaded system
- No histological evidence that self-tapping insertion caused bone necrosis or fibrous-tissue loss of purchase
Pullout Strength of Pedicle Screws and Bone Mineral Density
- Paired cadaveric hemivertebrae compared normal versus artificially demineralised (osteopenic) bone
- Mean pullout strength of the osteopenic model was 76% of the control (1284 N versus 1679 N)
- Pullout strength correlated positively with bone mineral density; displacement before failure increased as BMD fell
- Even osteopenic (not yet osteoporotic) bone significantly reduced screw pullout strength
Cutting Flute Design, Insertion Torque and Pullout Strength
- Self-tapping 4.5mm cortical screws of differing flute geometry tested in human cadaveric femoral diaphysis
- Insertion torque and pullout strength were normalised to local bone mineral density
- The design with four full-length cutting flutes had the lowest normalised insertion torque
- The four-flute design also showed the greatest normalised pullout (holding) strength of the screws tested
Biomechanical Testing of the Locked Internal Fixator (LCP)
- Composite-bone and finite-element study of the Locking Compression Plate in bridging mode
- Working length (distance from fracture to nearest screw) was the principal determinant of axial and torsional stiffness
- Omitting one screw hole either side of the fracture made the construct almost twice as flexible
- More than three screws per fragment added little axial stiffness; plate failure occurred at the empty hole nearest the fracture
The Scientific Basis of Biological Internal Fixation
- Landmark review establishing the locked internal fixator as a splint based on relative, not absolute, stability
- The interfragmentary strain theory defines the instability a healing gap will tolerate and the minimum required to induce callus
- Locked threaded bolts remove the need to contour the plate to bone, enabling minimally invasive percutaneous osteosynthesis (MIPO)
- Minimising implant-bone contact preserves periosteal perfusion and reduces necrosis-driven bone loss
Cement Augmentation of Screws in Osteoporotic Bone
- Systematic review of cement-augmented versus non-augmented sacroiliac screws in pelvic fragility fractures
- Most biomechanical studies showed augmented screws had greater pullout force and stability
- Cement provided no consistent advantage under cyclic loading, questioning direct clinical translation
- Three asymptomatic cement leaks into neuroforamina occurred across 122 augmented screw fixations