Joint Infection | Cartilage Destruction | Surgical Emergency
- Septic arthritis is a surgical emergency - irreversible cartilage damage begins within 6-12 hours
- Synovial fluid WCC over 50,000 with over 90% PMNs strongly suggests septic arthritis
- Native joint sepsis = single washout + antibiotics. Prosthetic joint = DAIR or two-stage revision
- Kocher criteria (fever, non-weight bearing, ESR over 40, WCC over 12) predict pediatric septic hip
- Australian eTG recommends flucloxacillin plus ceftriaxone for empiric therapy
- “Gonococcal arthritis is the most common in sexually active young adults
- “Lyme arthritis is monoarticular large joint - serology positive
- “Prosthetic joint infection under 3 months = acute, debride and retain (DAIR)
- “Kingella kingae is common in children under 4 years - difficult to culture
Proteolytic enzymes destroy cartilage rapidly. Bacterial toxins and host PMN release collagenase, elastase, and metalloproteinases. Irreversible damage begins in 6-12 hours. This is why septic arthritis is a true orthopaedic emergency.
Synovial fluid analysis is diagnostic. WCC over 50,000 with over 90% polymorphs suggests sepsis. Gram stain positive in 50%. Culture gold standard but negative in 20-30%. Always send for crystal analysis to exclude gout.
Four criteria for pediatric septic hip: Fever over 38.5°C, Non-weight bearing, ESR over 40, WCC over 12. All 4 present = 99.6% probability. Use to decide urgency of surgical drainage.
Surgical drainage plus antibiotics. Native joint = arthroscopic or open washout, repeat if not improving. Prosthetic joint = DAIR if acute (under 3 months), two-stage if chronic. Empiric antibiotics must cover S. aureus.
Overview and Introduction
Septic arthritis is a bacterial infection of a joint that represents a true orthopaedic emergency. The condition results in rapid destruction of articular cartilage through the combined action of bacterial toxins and host inflammatory mediators. Understanding the pathophysiology is essential for recognizing the urgency of treatment.
Key Time Concept:
- Irreversible cartilage damage begins within 6-12 hours of bacterial invasion
- Surgical drainage required within 24 hours to prevent permanent joint damage
- Delayed treatment leads to chronic pain, stiffness, and potential need for arthrodesis or arthroplasty
Mechanisms of Joint Infection
Biofilm Formation and Bacterial Virulence
Bacteria can form biofilms on cartilage and synovial surfaces:
- Glycocalyx matrix protects bacteria from antibiotics and host immune cells
- Quorum sensing allows bacterial communication and coordinated toxin production
- Persistent infection develops if biofilm establishes on damaged cartilage
Host Inflammatory Response
The host response paradoxically contributes to cartilage destruction:
- PMN infiltration - neutrophils release proteolytic enzymes
- Collagenase and metalloproteinases - degrade cartilage matrix
- Cytokine cascade - IL-1, TNF-alpha drive continued inflammation
- Elevated intra-articular pressure - compromises cartilage nutrition
Pathophysiology of Septic Arthritis
Routes of Infection
Most common route - 80% of cases, Transient bacteremia seeds synovium, Synovium is highly vascular with no basement membrane, Bacteria easily penetrate into joint space, Risk factors: IV drug use, immunosuppression, diabetes
Iatrogenic - joint injection, arthroscopy, arthroplasty, Trauma - penetrating injury, open fracture, Extension - adjacent osteomyelitis breaking into joint, Typically lower bacterial load initially, May present with delayed symptoms
From adjacent osteomyelitis - especially pediatric, Hip, shoulder, elbow have intra-articular metaphysis, Metaphyseal infection ruptures into joint, Neonatal osteomyelitis commonly causes septic arthritis, Adult vertebral osteomyelitis can seed disc
Mechanism of Cartilage Destruction
Progressive Joint Destruction
Bacteria bind to synovium and proliferate. Synovial membrane has abundant blood supply but lacks basement membrane - bacteria easily penetrate. Rapid bacterial multiplication in nutrient-rich synovial fluid. Inflammatory response triggered.
Massive PMN infiltration and enzyme release. Neutrophils release proteolytic enzymes: collagenase, elastase, metalloproteinases. Bacterial toxins directly damage chondrocytes. Synovial inflammation increases intra-articular pressure. Irreversible cartilage damage begins.
Proteoglycan depletion and collagen degradation. Loss of cartilage matrix leads to chondrocyte death. Subchondral bone exposed in severe cases. Joint capsule distends with purulent effusion. Vascular compromise from elevated pressure.
Pannus formation and fibrous ankylosis. Granulation tissue (pannus) grows over remaining cartilage. Fibrous adhesions form. May progress to bony ankylosis. Growth plate damage in children. Chronic pain and stiffness.
Irreversible articular cartilage damage begins within 6-12 hours of bacterial invasion. This is why septic arthritis is classified as an orthopaedic emergency requiring urgent surgical drainage. Delays beyond 24 hours significantly worsen outcomes - permanent joint damage, chronic pain, and need for arthrodesis or arthroplasty.
Microbiology
- Most Common Organism
- Group B Streptococcus
- Second Most Common
- E. coli, S. aureus
- Key Clinical Feature
- Can spread from osteomyelitis via transphyseal vessels
- Most Common Organism
- Kingella kingae
- Second Most Common
- S. aureus
- Key Clinical Feature
- Difficult to culture - fastidious organism
- Most Common Organism
- Staphylococcus aureus
- Second Most Common
- Streptococcus pyogenes
- Key Clinical Feature
- 70% of pediatric septic arthritis
- Most Common Organism
- Neisseria gonorrhoeae
- Second Most Common
- S. aureus
- Key Clinical Feature
- Polyarticular, migratory arthritis, skin lesions
- Most Common Organism
- Staphylococcus aureus
- Second Most Common
- Streptococcus species
- Key Clinical Feature
- 60-70% of adult septic arthritis
- Most Common Organism
- S. aureus, Pseudomonas
- Second Most Common
- Candida species
- Key Clinical Feature
- Unusual joints: sternoclavicular, sacroiliac
- Most Common Organism
- Gram-negative rods
- Second Most Common
- Fungi, atypical mycobacteria
- Key Clinical Feature
- Indolent course, multiple joints
- Most Common Organism
- S. aureus
- Second Most Common
- Coagulase-negative Staph
- Key Clinical Feature
- Acute presentation - DAIR candidate
- Most Common Organism
- Coagulase-negative Staph
- Second Most Common
- Propionibacterium
- Key Clinical Feature
- Low virulence biofilm - two-stage revision
Kocher Criteria for Pediatric Septic Hip
The Four Kocher Criteria
Temperature over 38.5°C (101.3°F)
- May be absent in immunocompromised
- Low-grade fever less predictive
- Documented fever most reliable
Refusal to bear weight on affected limb
- Most specific clinical sign
- Also present in transient synovitis
- Inability to weight bear worse than limp
Erythrocyte sedimentation rate over 40 mm/hr
- Less specific than CRP
- Slower to rise and normalize
- CRP over 20 mg/L is alternative cutoff
White cell count over 12,000 per microliter
- Systemic inflammatory response
- May be normal in early infection
- Less reliable than synovial fluid WCC
- Probability of Septic Arthritis
- Less than 3%
- Recommendation
- Observe, serial examination
- Probability of Septic Arthritis
- 40%
- Recommendation
- Urgent aspiration and synovial fluid analysis
- Probability of Septic Arthritis
- 93%
- Recommendation
- Strong indication for surgical drainage
- Probability of Septic Arthritis
- 99.6%
- Recommendation
- Emergency surgical washout required
The Kocher criteria were derived for pediatric hip septic arthritis to distinguish from transient synovitis. They should NOT be used to diagnose septic arthritis in adults, other joints, or to exclude infection in high-risk patients. A child with 0-1 criteria still has 3% risk - clinical judgment remains essential.
Classification
Classification of Septic Arthritis
By Mechanism of Infection
- Hematogenous: Bacteremia seeding synovium (most common in native joints)
- Direct inoculation: Trauma, surgery, injection
- Contiguous spread: From adjacent osteomyelitis or soft tissue infection
By Joint Type
- Native joint: Higher cure rates with appropriate treatment
- Prosthetic joint: More complex, often requires implant removal
Clinical Classification
- Findings
- Turbid fluid, hyperemic synovium
- Treatment Implications
- Single arthroscopic lavage often sufficient
- Findings
- Purulent fluid, fibrin deposits
- Treatment Implications
- Arthroscopic lavage, may need repeat
- Findings
- Thick fibrin, compartmentalization
- Treatment Implications
- May require open synovectomy
- Findings
- Cartilage destruction, osteolysis
- Treatment Implications
- Open debridement, poor prognosis
Clinical Relevance and Diagnosis
Understanding the pathophysiology directly informs clinical management:
- Removes bacterial load and proteolytic enzymes from joint
- Reduces intra-articular pressure
- Prevents biofilm establishment on cartilage
- Allows direct visualization and debridement
- Antibiotics cannot penetrate established biofilm
- Do not remove proteolytic enzymes already released
- Cannot reduce mechanical effects of elevated pressure
- Delay allows irreversible cartilage damage
Diagnosis
Synovial Fluid Analysis
- Normal
- Under 200
- Inflammatory (Gout)
- 2,000-50,000
- Septic Arthritis
- Usually over 50,000
- Clinical Note
- Overlap exists - over 90% PMN more specific
- Normal
- Under 25%
- Inflammatory (Gout)
- 50-75%
- Septic Arthritis
- Over 90%
- Clinical Note
- Over 90% polymorphs highly specific for sepsis
- Normal
- Negative
- Inflammatory (Gout)
- Negative
- Septic Arthritis
- Positive in 50%
- Clinical Note
- Immediate result - guides empiric therapy
- Normal
- Sterile
- Inflammatory (Gout)
- Sterile
- Septic Arthritis
- Positive in 70-80%
- Clinical Note
- Gold standard - obtain before antibiotics
- Normal
- Similar to blood
- Inflammatory (Gout)
- Normal
- Septic Arthritis
- Less than half blood glucose
- Clinical Note
- Bacteria consume glucose
- Normal
- None
- Inflammatory (Gout)
- MSU or CPPD positive
- Septic Arthritis
- None (may coexist)
- Clinical Note
- Always check - gout can be septic too
Finding crystals on synovial fluid analysis does NOT exclude septic arthritis. Gout and pseudogout can precipitate septic arthritis or coexist. If WCC is over 50,000 or clinical suspicion high, treat as septic arthritis regardless of crystal presence. Send culture and start antibiotics.
Imaging
First-line investigation:
- Joint space widening from effusion
- Soft tissue swelling
- Loss of fat planes
- Exclude fracture or foreign body
- Chronic: joint space narrowing, erosions
- Cannot rule out sepsis on XR alone
Useful for detecting effusion:
- Hip effusion in children
- Guides aspiration
- Differentiates effusion from synovitis
- Cannot distinguish septic from aseptic
- Operator-dependent
Differential Diagnosis of the Acute Monoarticular Hot Joint
- Typical Features
- Acutely hot, exquisitely painful joint; often febrile; refusal to move/bear weight
- Synovial Fluid
- Turbid/purulent; WCC usually over 50,000 with over 90% PMN; Gram stain positive in ~50%
- Key Discriminator
- Positive Gram stain or culture; very high WCC with PMN predominance - treat empirically if in doubt
- Typical Features
- Recurrent, often first MTP joint; rapid onset; tophi; hyperuricaemia
- Synovial Fluid
- WCC 2,000-75,000; negatively birefringent needle-shaped MSU crystals
- Key Discriminator
- Crystals on polarised microscopy - but crystals do NOT exclude coexisting sepsis
- Typical Features
- Older patient; knee/wrist; chondrocalcinosis on XR
- Synovial Fluid
- WCC 2,000-50,000; positively birefringent rhomboid CPPD crystals
- Key Discriminator
- Rhomboid crystals plus chondrocalcinosis
- Typical Features
- Post-enteric/urogenital infection; oligoarthritis; enthesitis; may have conjunctivitis/urethritis
- Synovial Fluid
- Inflammatory, sterile (WCC often 2,000-50,000)
- Key Discriminator
- Sterile fluid with antecedent GI/GU infection; HLA-B27 association
- Typical Features
- Trauma, anticoagulation, or haemophilia; rapid swelling
- Synovial Fluid
- Frankly bloody aspirate; may show fat (lipohaemarthrosis) if intra-articular fracture
- Key Discriminator
- Blood (and fat globules) on aspiration; coagulation/trauma history
- Typical Features
- Well child, low-grade or no fever; able to bear some weight; recent viral illness
- Synovial Fluid
- Sterile inflammatory effusion; lower synovial WCC
- Key Discriminator
- Few/no Kocher predictors; settles with rest and NSAIDs - but aspirate if uncertain
- Typical Features
- Known RA/psoriatic/JIA; polyarticular history
- Synovial Fluid
- Inflammatory; sterile (RA itself raises septic risk - have a low threshold to aspirate)
- Key Discriminator
- Pattern and prior diagnosis - but immunosuppressed RA patients are HIGH-risk for superimposed sepsis
A hot joint with crystals can still be septic. If the synovial WCC is very high, the patient is systemically unwell, or clinical suspicion is significant, send culture and treat as septic arthritis regardless of crystals. Crystal arthropathy and infection coexist, especially in the elderly and immunosuppressed.
Investigations
Laboratory Investigations
Joint Aspirate (Most Important)
- WCC: Greater than 50,000/μL highly suggestive (greater than 25,000/μL suspicious)
- Gram stain: Positive in 50-70% of cases
- Culture: Gold standard, positive in 85-95%
- Crystal analysis: Rule out gout/pseudogout (can coexist)
Blood Tests
- WCC: Often elevated (may be normal in immunocompromised)
- CRP: Elevated (useful for monitoring response)
- ESR: Elevated but slower to change than CRP
- Blood cultures: Positive in 30-50%, always obtain if febrile
Kocher Criteria (Paediatric Hip)
- Fever greater than 38.5°C
- Non-weight bearing
- WCC greater than 12,000/μL
- ESR greater than 40mm/hr
- 4/4 criteria = 99% probability of septic arthritis
Management
Native Joint Septic Arthritis Management
Treatment Algorithm
Urgent joint aspiration before antibiotics. Send for WCC, Gram stain, culture (aerobic, anaerobic, fungal). Document gross appearance (purulent, cloudy, bloody). Check for crystals. Blood cultures if febrile.
Start antibiotics after cultures obtained. Australian eTG: flucloxacillin 2g IV 6-hourly PLUS ceftriaxone 2g IV daily. Covers S. aureus, Streptococcus, and Gram-negatives. Adjust when cultures available.
Arthroscopic or open washout within 24 hours. Copious irrigation (minimum 9 liters). Debride fibrin, synovial debris. Take multiple tissue samples. Hip requires open arthrotomy. Small joints may respond to repeat aspiration.
Repeat washout if not improving. Persistent fever, rising CRP, persistent joint swelling indicates inadequate drainage. Up to 3 washouts may be needed. Consider open if arthroscopy failing.
Total 2-6 weeks antibiotics. IV for 2 weeks, then oral if improving. Monitor CRP weekly - should fall by 50% at 2 weeks. Small joints 2 weeks, large joints 4 weeks, hip 6 weeks.
The hip joint is too deep for effective arthroscopic drainage in septic arthritis. Open anterior (Smith-Petersen) or anterolateral (Watson-Jones) approach allows complete debridement of fibrinous material and copious irrigation. Leaving a drain is controversial - most surgeons do not use drain to avoid retrograde infection.
The topic refers to "MSIS/EBJIS definitions" but the examinable detail is the criteria themselves, which standardise the diagnosis of periprosthetic joint infection (PJI) beyond a single test:
- Major criteria (either one confirms PJI): a sinus tract communicating with the prosthesis/joint, OR two positive cultures of the same organism from the joint.
- Minor criteria (a threshold combination confirms PJI when no major criterion is met): raised serum CRP and/or ESR; raised synovial fluid white-cell count; raised synovial polymorphonuclear percentage; positive synovial alpha-defensin (or leucocyte esterase); positive periprosthetic tissue histology (neutrophils per high-power field); and a single positive culture.
- The EBJIS framework adds practical categories (infection "confirmed / likely / unlikely") and emphasises multiple periprosthetic tissue samples (commonly several, with a threshold number positive), prolonged culture incubation (to catch Cutibacterium/low-virulence organisms), and sonication of the explant to dislodge biofilm and raise culture yield.
Why it matters: PJI is a composite diagnosis - a single negative aspirate does not exclude it, and the thresholds differ from native-joint septic arthritis (synovial WCC cut-offs for PJI are much lower, in the low thousands, not over fifty thousand).
Exam point: define PJI by MSIS/EBJIS - one major criterion (sinus tract or two same-organism cultures) or a combination of minor criteria (CRP/ESR, synovial WCC/PMN%, alpha-defensin, histology, single culture), with multiple tissue samples, prolonged incubation and explant sonication to maximise yield.
Surgical Technique
Surgical Drainage Techniques
Arthroscopic Lavage (Preferred for Most Joints)
- Standard arthroscopic portals for the affected joint
- Thorough inspection and documentation of cartilage status
- Copious irrigation: Minimum 9-12 liters saline
- Debridement of fibrinous debris and synovitis
- Take multiple tissue samples for culture
Open Arthrotomy (Required for Hip, Some Failures)
- Standard surgical approach (anterior for hip)
- Complete capsulotomy for drainage
- Copious irrigation and debridement
- Leave drain controversial - most avoid (retrograde infection risk)
- Closure in layers
Repeat Aspiration (Small Joints)
- Serial daily aspirations may be adequate for fingers/toes
- Must demonstrate falling WCC and sterile cultures
- Convert to surgical drainage if not improving
Complications
Complications of Septic Arthritis
Cartilage Destruction
- Occurs within 48-72 hours of untreated infection
- Enzymatic degradation from bacterial toxins and host proteases
- Irreversible once established - leads to arthritis
- Prevention: Early diagnosis and aggressive treatment
Systemic Complications
- Sepsis and septic shock (5-10%)
- Multi-organ dysfunction
- Death (mortality 5-15% in adults, higher in elderly)
- Metastatic infection (other joints, endocarditis)
Joint-Specific Complications
- Hip in children: Avascular necrosis of femoral head
- Knee: Stiffness, secondary osteoarthritis
- Shoulder: Rotator cuff damage, stiffness
Postoperative Care
Postoperative Management
Antibiotic Therapy
- Continue IV antibiotics minimum 2 weeks
- Transition to oral when clinically improving and CRP falling
- Total duration: 2-6 weeks depending on joint and response
- Culture-directed therapy once sensitivities available
Monitoring
- Daily clinical assessment (pain, swelling, ROM)
- Temperature monitoring
- CRP every 2-3 days initially, then weekly
- Expect CRP to fall by 50% at 2 weeks
Rehabilitation
- Gentle passive ROM as soon as tolerated
- Protected weight-bearing until infection controlled
- Progressive strengthening after infection resolution
The traditional teaching of "weeks of IV antibiotics" for bone and joint infection has been overturned by the OVIVA trial (Oral Versus Intravenous Antibiotics), which is examinable and practice-changing:
- Design: a large multicentre randomised non-inferiority trial in adults with bone and joint infection (including native septic arthritis, osteomyelitis and prosthetic-joint infection), randomising patients in the first six weeks of treatment to continued IV versus an early switch to oral antibiotics, after initial surgical management as indicated.
- Result: oral antibiotics were non-inferior to IV for the primary endpoint of treatment failure at one year - oral was not worse, and was associated with shorter hospital stay and fewer line-related complications (catheter problems, line infections).
- Caveats: it relied on specialist infection input/oral agents with good bone bioavailability (e.g. fluoroquinolones, often with rifampicin for staphylococcal implant infection) and assured oral absorption/compliance; it does not mean "oral for everyone from day one" - source control and appropriate agent selection still apply.
Why it matters: it justifies an early IV-to-oral switch once the patient is improving with a suitable, well-absorbed oral agent, reducing line complications and hospital stay - a direct change from the old reflex of prolonged IV therapy.
Exam point: cite OVIVA - oral antibiotics are non-inferior to IV in the first six weeks of bone/joint infection (with specialist guidance and bioavailable agents), supporting early oral switch rather than mandatory prolonged IV therapy.
Outcomes
Outcomes of Septic Arthritis
Overall Prognosis
- Mortality: 5-15% in adults (higher in elderly, comorbidities)
- Joint destruction: 40-50% develop secondary osteoarthritis
- Full recovery: 50-60% with early aggressive treatment
Factors Affecting Outcome
- Better Outcome
- Under 24 hours
- Worse Outcome
- Over 72 hours
- Better Outcome
- Young, healthy
- Worse Outcome
- Elderly, comorbid
- Better Outcome
- Streptococcus
- Worse Outcome
- S. aureus, Gram-negative
- Better Outcome
- Small joint
- Worse Outcome
- Hip, shoulder
Guidelines, Registries & Global Practice
Global Epidemiology
Native-joint septic arthritis affects approximately 4-10 per 100,000 person-years in high-income populations, rising to 30-70 per 100,000 in those with rheumatoid arthritis or a prosthetic joint. Incidence is increasing worldwide, driven by an ageing population, more joint replacement surgery, immunosuppression, diabetes and injecting drug use. Staphylococcus aureus is the leading pathogen globally, but the proportion of MRSA varies markedly by region (low in much of Scandinavia and the Netherlands, substantially higher in parts of the USA and Asia), which directly affects empirical antibiotic choice. In sexually active young adults, Neisseria gonorrhoeae remains an important cause where prevalence is high. Reported mortality is 7-15% and long-term joint dysfunction occurs in roughly a third of survivors despite treatment.
Side-by-Side Guidance
- Scope
- Hot swollen joint - adults
- Core Recommendations
- Aspirate before antibiotics; urgent synovial Gram stain, culture, cell count; empirical anti-staphylococcal cover then organism-directed; joint drainage (aspiration, arthroscopic or open)
- Evidence Strength
- Consensus / low-moderate (largely observational base)
- Scope
- Prosthetic joint infection
- Core Recommendations
- Defines DAIR vs one-/two-stage exchange; rifampin combination for stable staphylococcal implant infection; structured antibiotic duration
- Evidence Strength
- Guideline - mostly low-quality evidence, strong consensus
- Scope
- Periprosthetic joint infection definition
- Core Recommendations
- Standardised diagnostic criteria (synovial WCC, alpha-defensin, culture, histology) for consistent diagnosis and research
- Evidence Strength
- International consensus definition
- Scope
- Periprosthetic hip/knee infection
- Core Recommendations
- Diagnostic work-up (ESR/CRP screen, then aspiration with WCC/differential and culture); supports staged management of chronic PJI
- Evidence Strength
- Appraised guideline - variable evidence levels
- Scope
- Empirical antimicrobials
- Core Recommendations
- Flucloxacillin (di/cloxacillin) plus a third-generation cephalosporin empirically; vancomycin where MRSA likely; ceftriaxone if gonococcal; de-escalate on culture
- Evidence Strength
- National antimicrobial guideline
Shared across guidelines:
- Aspirate and culture BEFORE antibiotics whenever feasible (do not delay treatment in the septic patient)
- Empirical cover always includes anti-staphylococcal activity; add MRSA cover (e.g. vancomycin) where local MRSA prevalence is high
- Ceftriaxone where gonococcal or Gram-negative infection is likely
- De-escalate to organism-directed therapy on sensitivities
- Typical duration 2-6 weeks (longer for prosthetic joints); increasingly oral switch is supported by the OVIVA trial in bone and joint infection
Registry and system evidence:
- Arthroplasty registries (AOANJRR, NJR England/Wales, Swedish & Australian registries) track PJI as a leading cause of revision and benchmark infection rates
- Practice varies in first-line drainage: arthroscopic lavage vs open arthrotomy vs serial aspiration, with no high-level RCT establishing superiority for native joints
- Australian eTG guidance is purely clinical and antimicrobial, not administrative or reimbursement-based
- Time-to-drainage and antibiotic stewardship are common quality metrics
MCQ Practice Points
Q: What synovial fluid WCC threshold suggests septic arthritis? A: Over 50,000 cells per microliter with over 90% polymorphs - this combination has 92% specificity. However, overlap exists with crystal arthropathy - gout can have WCC over 50,000.
Q: What is the most common organism causing septic arthritis in adults? A: Staphylococcus aureus - causes 60-70% of adult septic arthritis. Exception: sexually active young adults where Neisseria gonorrhoeae is most common.
Q: A child has all 4 Kocher criteria present. What is the probability of septic arthritis? A: 99.6% probability - this mandates emergency surgical washout. The 4 criteria are: fever over 38.5C, non-weight bearing, ESR over 40, WCC over 12.
Q: What is the time window for considering DAIR in prosthetic joint infection? A: Under 3 months from surgery OR acute hematogenous infection with symptoms under 3 weeks - beyond this window, biofilm is established and two-stage revision is required.
At a Glance
Septic arthritis is an orthopaedic emergency—irreversible cartilage destruction begins within 6-12 hours due to proteolytic enzymes from bacteria and host PMNs. S. aureus is the most common organism in adults; Kingella kingae in children under 4 years; Neisseria gonorrhoeae in sexually active young adults. Diagnosis requires synovial fluid WCC over 50,000 with over 90% PMNs; Gram stain is positive in only 50% of cases. The Kocher criteria (fever, non-weight bearing, ESR over 40, WCC over 12) predict pediatric septic hip with 99.6% probability when all four are present. Treatment is urgent surgical washout plus empiric IV antibiotics (Australian eTG: flucloxacillin + ceftriaxone).
ASKINGOrganisms by Age Group
Hook:When ASKING about septic arthritis organisms, think of patient age and risk factors!
WGCSynovial Fluid Findings in Septic Arthritis
Hook:When you Get Synovial Fluid, check WGC - White cells, Gram stain, Culture!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 3-year-old boy presents with 2 days of right hip pain and refusal to walk. Temperature 39.2°C. Held in flexion, abduction, external rotation. Blood tests: WCC 14,000, CRP 65, ESR 48. Ultrasound shows hip joint effusion. How would you assess and manage this child?”
“A 68-year-old woman presents 6 weeks after primary total knee replacement with 1 week of increasing pain, swelling, and wound drainage. Temperature 38.1°C. Knee warm, effusion present, small amount of serous drainage from wound. CRP 145. The implant appears well-fixed on plain radiographs. Is she a candidate for DAIR or does she need two-stage revision?”
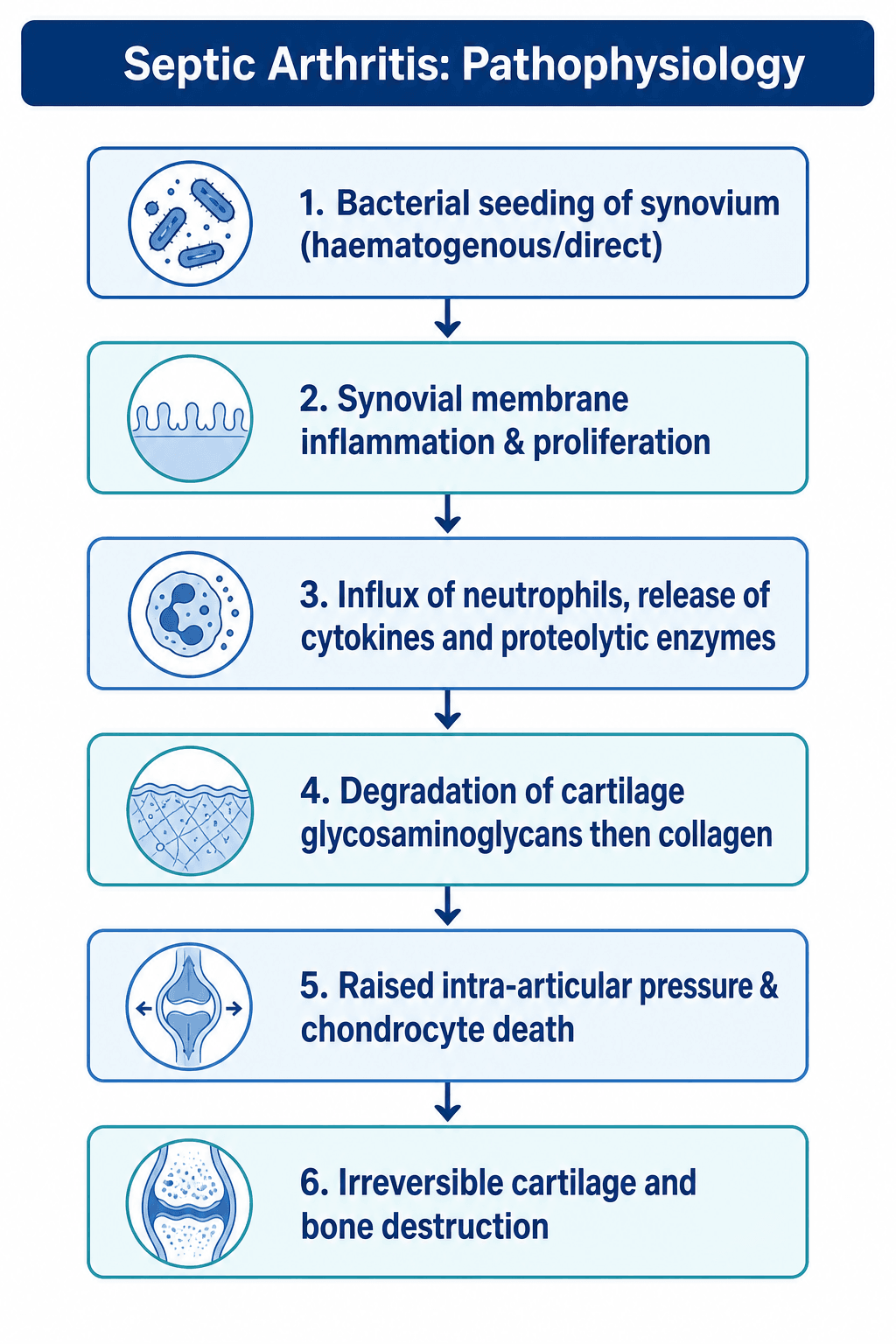
Key Pathophysiology
- Irreversible cartilage damage begins 6-12 hours
- PMN enzymes (collagenase, elastase) destroy matrix
- Elevated intra-articular pressure compromises blood supply
- Pannus formation leads to fibrous ankylosis
Kocher Criteria (Pediatric Hip)
- Fever over 38.5C, Non-weight bearing, ESR over 40, WCC over 12
- 4/4 criteria = 99.6% probability septic arthritis
- 3/4 criteria = 93% probability
- 2/4 criteria = 40% probability - urgent aspiration
Synovial Fluid Analysis
- WCC over 50,000 with over 90% PMN suggests sepsis
- Gram stain positive in 50% - immediate result
- Culture gold standard - obtain before antibiotics
- Crystals can coexist with sepsis - do not exclude
Microbiology
- Adult: S. aureus (60-70%), N. gonorrhoeae in sexually active
- Child: S. aureus, Kingella kingae (under 4 years)
- Neonate: Group B Strep, E. coli, S. aureus
- IV drug user: S. aureus, Pseudomonas, Candida
Treatment
- Native joint: washout within 24h + 2-6 weeks antibiotics
- Hip requires open arthrotomy (too deep for arthroscopy)
- PJI acute: DAIR if under 3 months, well-fixed, under 3 weeks symptoms
- PJI chronic: Two-stage revision (90% success)
- eTG empiric: Flucloxacillin + ceftriaxone
Evidence Base
Kocher Criteria: Original Derivation Study
- Retrospective review (1979-1996) of children with an acutely irritable hip at a tertiary paediatric centre
- Four independent multivariate predictors identified by logistic regression: history of fever, non-weight-bearing, ESR at least 40 mm/hr, serum WCC over 12,000/mm3
- Predicted probability of septic arthritis: 0 predictors under 0.2%, 1 = 3.0%, 2 = 40.0%, 3 = 93.1%, 4 = 99.6%
- Combining variables gave excellent discrimination where single variables overlapped
Diagnostic Accuracy of Synovial Fluid WCC (Rational Clinical Examination)
- Systematic review of 14 studies (6242 patients, 653 with confirmed septic arthritis) of the clinical evaluation for non-gonococcal bacterial arthritis
- Synovial WCC likelihood ratios rise with the count: over 50,000/uL LR 7.7 (95% CI 5.7-11.0); over 100,000/uL LR 28.0 (95% CI 12.0-66.0); under 25,000/uL LR 0.32
- Synovial PMN at least 90% gives LR 3.4 (95% CI 2.8-4.2); under 90% lowers likelihood (LR 0.34)
- Joint pain (sens 85%), history of swelling (78%) and fever (only 57%) are the most frequent findings; no clinical sign reliably excludes infection
Time-Course of Cartilage Matrix Destruction in Infective Arthritis
- Rabbit model of E. coli and S. aureus infective arthritis with biochemical quantification of matrix loss
- Glycosaminoglycan (proteoglycan) loss is the earliest event - by 48 hours GAG was reduced ~20% (E. coli) and ~42% (S. aureus tibial plateau)
- By the 3rd week GAG loss reached up to 73%; significant collagen loss (~42%) lagged behind, appearing only at 3 weeks
- Proteoglycan depletion precedes collagen degradation - the biochemical basis of rapid cartilage softening
Early Antibiotics Limit Cartilage Loss in Experimental Septic Arthritis
- Rabbit S. aureus knee arthritis treated with ceforanide started at varying times after inoculation
- Starting antibiotics at 4-12 hours limited GAG loss to ~18%, whereas treatment at 1, 2 or 7 days failed to prevent loss of over half the GAG by 3 weeks
- Treatment at 1 day reduced overall collagen loss by 37% and the area of articular erosion
- Antibiotic prophylaxis (before infection established) completely prevented cartilage degradation