Hallucal Sesamoid Pathology | Tibial and Fibular Sesamoids | Sesamoidectomy Complications
- Tibial (medial) sesamoid bears more weight and is most commonly affected (25:1 ratio)
- Bipartite sesamoid has smooth corticated margins, bilateral in 85%, larger total volume
- MRI is gold standard for differentiating sesamoiditis, fracture, and AVN
- Conservative management successful in over 90% of cases - trial 3-6 months minimum
- Sesamoidectomy risks: hallux valgus (tibial excision), hallux varus (fibular excision), cock-up toe
- “Passive dorsiflexion test (Windlass mechanism) reproduces pain by loading sesamoid complex
- “Axial (skyline) radiograph view is critical for visualizing sesamoid-metatarsal articulation
- “FHB tendon repair during sesamoidectomy is mandatory to prevent cock-up deformity
- “Blood supply enters proximal pole - distal fractures have high AVN and nonunion risk
Two sesamoid bones embedded in FHB tendons. Tibial (medial) and fibular (lateral) sesamoids articulate with plantar metatarsal head crista. They increase FHB mechanical advantage and absorb up to 300% body weight during gait.
Bipartite vs Fracture is critical. Bipartite: smooth margins, bilateral 85%, normal MRI signal. Fracture: sharp irregular line, unilateral, bone marrow edema on MRI. Always X-ray both feet for comparison.
Conservative first for at least 6 months. Offloading orthotics (dancer's pad), stiff-soled shoes, activity modification. Surgery only for failed conservative management or displaced acute fractures requiring ORIF.
Sesamoidectomy alters biomechanics. Tibial excision leads to hallux valgus (loss of medial buttress). Fibular excision leads to hallux varus (loss of lateral pull). Inadequate FHB repair causes cock-up toe deformity.
- Imaging Findings
- Normal radiographs, MRI shows bone marrow edema
- First-Line Treatment
- Conservative: offloading, NSAIDs, activity modification
- Key Pearl
- Typical sesamoiditis - 90% resolve non-operatively
- Imaging Findings
- Sharp irregular fracture line, unilateral
- First-Line Treatment
- NWB cast/boot 6 weeks, consider ORIF if displaced
- Key Pearl
- Differentiate from bipartite - check contralateral foot
- Imaging Findings
- Sclerosis, fragmentation, joint space narrowing
- First-Line Treatment
- Sesamoidectomy consideration
- Key Pearl
- AVN or sesamoid arthritis - surgical candidate
- Imaging Findings
- Rounded corticated margins, symmetric bilaterally
- First-Line Treatment
- Asymptomatic - no treatment needed
- Key Pearl
- Normal variant in 10-30% population - not a fracture
SMOOTHFeatures Distinguishing Bipartite from Fracture
Hook:A SMOOTH diagnosis on imaging prevents unnecessary treatment of a normal variant!
Overview and Epidemiology
Hallucal sesamoid pathology represents a spectrum from benign anatomical variants (bipartite sesamoid) to debilitating conditions requiring surgery (AVN, nonunion). The tibial sesamoid is the most commonly affected due to increased weight-bearing forces and more variable vascular supply. Understanding the differential diagnosis and appropriate imaging is critical for exam scenarios.
- Population: Athletes, dancers, runners most affected
- Age: Typically 20-40 years for acute injuries
- Gender: Male and female equally affected
- Activity: Ballet (relevé position), running (push-off phase), basketball (jumping)
- Footwear: High heels increase forefoot loading
- Foot morphology: Cavus foot (rigid, peaked MTPJ angle)
- Plantarflexed first ray: Drives sesamoid into ground
- Gastrocnemius tightness: Equinus deformity prolongs forefoot loading
- Training errors: Sudden volume increase, hard surfaces
- Previous injury: Prior sesamoid pathology increases reinjury risk
Anatomy and Biomechanics
The sesamoids receive their blood supply from the first plantar metatarsal artery (Rath 2009), with two major entry sources: proximal (at the FHB attachment) and plantar near the midline, plus a minor distal contribution (Sobel 1992). The watershed pattern means distal pole and mid-substance fractures can compromise perfusion and predispose to avascular necrosis and nonunion. Surgically, the proximal and plantar surfaces should be respected to preserve perfusion.
Sesamoid Complex Anatomy
The hallucal sesamoids are two small ovoid bones embedded within the tendons of flexor hallucis brevis (FHB), located plantar to the first metatarsal head.
Bony Anatomy:
- Tibial Sesamoid (Medial): Typically more elongated, bears greater weight
- Fibular Sesamoid (Lateral): More rounded, bears less load
- Articular Surface: Dorsal surface articulates with plantar metatarsal head crista
- Non-articular Surface: Plantar surface gives attachment to plantar plate and FHB
Soft Tissue Relationships:
- Relationship to Sesamoids
- Medial head encases tibial sesamoid; lateral head encases fibular
- Clinical Significance
- Main stabilizer - repair mandatory during sesamoidectomy
- Relationship to Sesamoids
- Strong fibrous band connecting the two sesamoids
- Clinical Significance
- Prevents separation; rupture occurs in severe turf toe
- Relationship to Sesamoids
- Passes in groove between sesamoids plantarly
- Clinical Significance
- Protected from ground contact; can develop tendonitis
- Relationship to Sesamoids
- Inserts partially on tibial sesamoid medially
- Clinical Significance
- Tibial excision allows valgus drift from loss of medial pull
- Relationship to Sesamoids
- Inserts on fibular sesamoid laterally
- Clinical Significance
- Fibular excision causes varus from unopposed abductor
- Relationship to Sesamoids
- Thick fibrocartilaginous structure attaching to sesamoids
- Clinical Significance
- Turf toe involves plantar plate rupture with sesamoid retraction
Biomechanical Function
The sesamoids serve multiple critical functions in first ray biomechanics:
- Mechanical Advantage: Increase moment arm of FHB by elevating the tendon away from joint center
- Load Absorption: Bear 2-3 times body weight during walking, up to 300% during running
- FHL Protection: Elevate metatarsal head to protect FHL tendon from compressive forces
- Weight Distribution: Distribute forces across metatarsal head during gait
Windlass Mechanism:
During toe-off, hallux dorsiflexion tightens the plantar fascia, elevating the arch and depressing the first metatarsal head. This dramatically increases force transmission through the sesamoid complex. Any pathology causing sesamoid pain disrupts this mechanism, leading to compensatory gait changes and potential transfer metatarsalgia.
- Position: Medial, more prominent plantarly
- Load: Bears approximately 60% of sesamoid complex load
- Pathology: 25 times more likely to fracture than fibular
- Excision Effect: Hallux valgus deformity risk
- Blood Supply: More variable, higher AVN risk
- Position: Lateral, less prominent
- Load: Bears approximately 40% of sesamoid complex load
- Pathology: Fractures and AVN less common
- Excision Effect: Hallux varus deformity risk
- Blood Supply: More consistent arterial supply
Pathophysiology
Mechanisms of Sesamoid Pathology
Sesamoid disorders develop through several distinct pathophysiological mechanisms. Understanding these processes is essential for appropriate diagnosis and management.
Overuse and Repetitive Microtrauma:
Sesamoiditis represents an inflammatory response to chronic repetitive loading. During the push-off phase of gait, the sesamoid complex experiences forces up to 300% of body weight. In athletes performing repetitive toe-off activities (ballet, running, jumping), cumulative microtrauma exceeds the tissue's healing capacity, resulting in:
- Bone marrow edema visible on MRI
- Periosteal inflammation
- Soft tissue swelling in FHB tendons and plantar plate
- Bursitis between sesamoid and metatarsal head
Stress Fracture Development:
When cyclical loading exceeds bone remodeling capacity, stress fractures develop through a predictable sequence:
- Stress Reaction: Increased osteoclastic activity creating microscopic trabecular damage
- Cortical Disruption: Fracture line appears as bone remodeling fails to keep pace
- Propagation: Continued loading extends the fracture through cortex
- Displacement: In severe cases, complete cortical break with fragment separation
The tibial sesamoid is 25 times more susceptible due to increased load-bearing and more variable vascular supply.
Avascular Necrosis Pathway:
AVN develops when blood supply is critically compromised, most commonly from:
- Fracture-related: Distal pole fractures disrupt the proximal vascular pedicle
- Idiopathic: Gradual vascular insufficiency from chronic repetitive trauma
- Post-surgical: Excessive soft tissue stripping during surgery
The pathological sequence follows:
- Vascular compromise leads to osteocyte death
- Bone attempts repair but fails due to persistent ischemia
- Subchondral collapse as necrotic bone cannot support loads
- Fragmentation and sclerosis as body attempts to revascularize
- Secondary degenerative changes in metatarsosesamoid joint
Acute Traumatic Fracture:
High-energy axial loading (forced dorsiflexion, direct impact) exceeds bone's ultimate tensile strength, causing immediate fracture. Sharp irregular fracture lines differentiate these from bipartite variants. Displacement depends on magnitude of force and integrity of surrounding soft tissue envelope.
Degenerative Arthritis:
Chronic overload or post-traumatic changes lead to cartilage degeneration in the metatarsosesamoid articulation. Progressive joint space narrowing, osteophyte formation, and subchondral sclerosis follow typical osteoarthritic patterns.
Anatomical and biomechanical factors converge:
- Bears 60% of sesamoid complex load (vs 40% fibular)
- More prominent plantar position
- Variable vascular anatomy (higher AVN risk)
- Larger size creates greater stress concentration
- First ray plantarflexion drives tibial into ground contact
Poor healing potential due to:
- Limited blood supply (single proximal arterial pedicle)
- Constant mechanical loading during ambulation
- Small bone size limits revascularization
- Embedded in tendon creates shear forces
- Poor soft tissue coverage plantarly
Classification Systems
Spectrum of Sesamoid Disorders
Sesamoid pathology exists on a continuum from normal variants to surgical conditions. Classification is descriptive based on etiology and imaging characteristics.
- Mechanism
- Repetitive microtrauma, overuse inflammation
- Imaging Features
- Radiographs normal; MRI shows bone marrow edema
- Treatment Approach
- Conservative: offloading, NSAIDs, activity modification
- Mechanism
- Cyclical loading exceeds bone remodeling capacity
- Imaging Features
- Fine cortical break; MRI high T2 signal with surrounding edema
- Treatment Approach
- NWB immobilization 6-8 weeks in walking boot
- Mechanism
- Single high-energy traumatic event
- Imaging Features
- Sharp irregular fracture line, possible displacement
- Treatment Approach
- Cast immobilization vs ORIF if displaced over 2mm
- Mechanism
- Vascular compromise, often post-fracture
- Imaging Features
- Sclerosis, fragmentation, collapse, loss of height
- Treatment Approach
- Sesamoidectomy if symptomatic and failed conservative
- Mechanism
- Congenital variant (multipartite ossification)
- Imaging Features
- Smooth corticated margins, bilateral 85%, larger volume
- Treatment Approach
- Usually asymptomatic; conservative if symptomatic synchondrosis
- Mechanism
- Degenerative changes in metatarsosesamoid articulation
- Imaging Features
- Joint space narrowing, osteophytes, subchondral sclerosis
- Treatment Approach
- Conservative first; sesamoidectomy or shaving if severe
Understanding this spectrum is essential for appropriate treatment selection in exam scenarios.
Clinical Assessment
History
A detailed history often reveals the underlying pathology type.
Key Questions:
- Onset: Insidious (sesamoiditis, stress fracture) vs acute (traumatic fracture, turf toe)
- Mechanism: Forced dorsiflexion (turf toe), repetitive push-off (sesamoiditis), single impact (acute fracture)
- Activity: Ballet dancers (relevé position), runners (push-off phase), basketball players (jumping)
- Pain Characteristics: Localized plantar pain worsened by toe-off phase of gait
- Footwear: High heels, cleats, or minimalist shoes increase forefoot loading
- Previous Symptoms: Prior episodes suggest chronic overload or bipartite variant
- Sesamoiditis: 25-year-old ballet dancer, insidious onset over weeks, worsened by relevé
- Stress Fracture: 30-year-old marathon runner, progressive pain over 2-4 weeks, no specific event
- Acute Fracture: 22-year-old footballer, immediate pain after forced dorsiflexion tackle
- Bipartite: Incidental finding on radiographs for unrelated foot pain, bilateral
Physical Examination
Systematic examination localizes pathology and rules out differential diagnoses.
Examination Sequence
- Swelling: Mild plantar MTPJ edema suggests active inflammation
- Erythema: Redness may indicate gout, infection, or acute injury
- Callosities: Intractable plantar keratosis (IPK) under sesamoid indicates prominence
- Alignment: Check for cavus foot (high arch), hallux valgus, or first ray plantarflexion
- Gait: Antalgic gait with shortened stride and early heel rise to avoid push-off
- Point Tenderness: Direct pressure over specific sesamoid reproduces pain
- Dorsal vs Plantar: Ensure pain is plantar (sesamoid) not dorsal (arthritis, gout)
- Joint Line: Palpate MTPJ for synovitis or effusion
- FHL Excursion: Pain with FHL gliding suggests tendonitis
- Neurovascular: Check sensation (medial plantar nerve) and pulses
- Passive Dorsiflexion Test: Extend hallux while palpating sesamoid - reproduces pain by loading complex
- Resisted Flexion: Active flexion against resistance tests FHB/FHL integrity
- Push-off Test: Single leg heel raise - inability indicates significant pain
- Grind Test: Compression plus rotation reproduces arthritic pain
- Vertical Lachman: Dorsal translation indicates plantar plate injury (turf toe)
This completes the clinical examination sequence.
- Erythema + Fever + Systemic Symptoms: Septic arthritis or osteomyelitis
- Gout Crystals: Aspirate and send for crystal analysis if suspicious
- Neurovascular Compromise: Rare but check pulses and sensation
- Unable to Weight Bear: Suggests displaced fracture or complete plantar plate rupture
Investigations
Imaging Protocol
A systematic approach to imaging ensures accurate diagnosis and appropriate treatment selection.
Stepwise Imaging Strategy
- AP Foot: Assess sesamoid alignment, fracture diastasis, bipartite margins
- Lateral Foot: Check for sesamoid height, proximal migration (turf toe)
- Axial (Skyline) Sesamoid View: Critical for visualizing sesamoid-metatarsal articulation
- Bipartite Features: Smooth rounded margins, bilateral symmetric appearance
- Fracture Features: Sharp irregular fracture line, unilateral
- AVN Features: Sclerosis, fragmentation, collapse, loss of height
- Arthritis: Joint space narrowing, osteophytes, subchondral cysts
Critical: Always obtain bilateral comparison radiographs to assess for bipartite variant symmetry.
Radiographic assessment is the foundation of sesamoid disorder diagnosis.
Gold Standard for Sesamoid Pathology
MRI provides definitive diagnosis when radiographs are normal or equivocal.
- T1-weighted: Low signal indicates edema, AVN, or chronic changes
- T2/STIR: High signal confirms acute bone marrow edema
- Proton Density: Evaluates cartilage integrity and plantar plate
- Sesamoiditis: Bone marrow edema, intact cortex, normal FHB and plantar plate
- Stress Fracture: Linear T2 hyperintensity, surrounding edema, cortical disruption
- AVN: Low T1/T2 signal (sclerosis), fragmentation, subchondral collapse
- Bipartite Symptomatic: Edema at synchondrosis junction; asymptomatic shows normal signal
- Turf Toe: Plantar plate rupture, capsular tear, joint effusion, sesamoid retraction
MRI is the definitive test for difficult diagnostic scenarios.
- CT Scan: Best for assessing fracture healing (union vs nonunion), bony architecture, and surgical planning
- Bone Scan: High sensitivity for stress reactions and sesamoiditis but low specificity
- Use Case: CT for nonunion evaluation; bone scan if MRI contraindicated
Advanced imaging complements the diagnostic workup.
Five Features Confirming Bipartite Variant (Not Fracture):
- Smooth Corticated Margins: Rounded edges vs sharp jagged fracture line
- Bilateral Symmetry: Present in both feet (85% of cases) - always check
- Larger Total Volume: Sum of fragments exceeds normal single sesamoid size
- Unequal Fragment Sizes: Typically one large and one small piece
- Normal MRI Signal: No bone marrow edema unless symptomatic synchondrosis injury
If unsure, MRI is definitive - fractures show surrounding edema, bipartite does not (unless symptomatic).
Management Algorithm
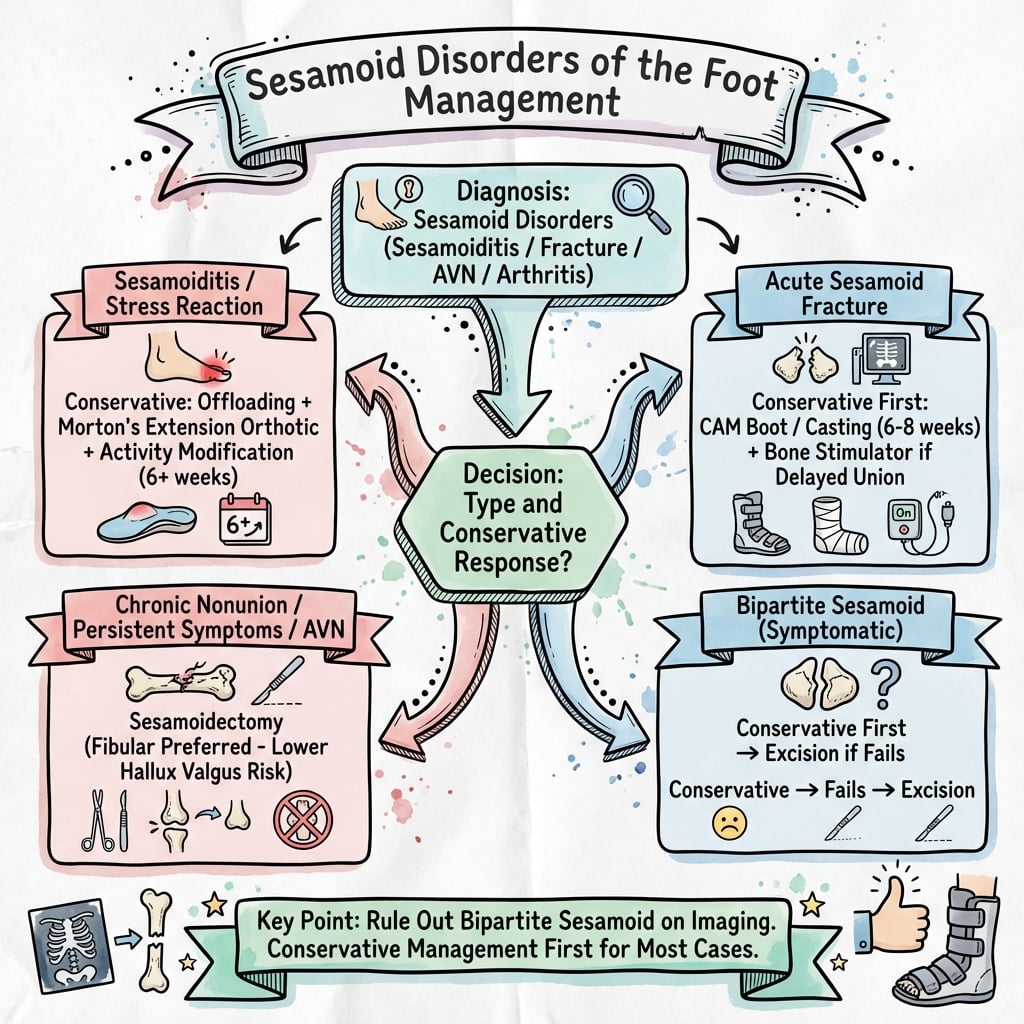
Non-Operative Treatment - First-Line for All Sesamoid Disorders
Over 90% of sesamoid disorders resolve with conservative management. A minimum 3-6 month trial is mandatory before surgical consideration.
Stepwise Conservative Protocol
- Complete cessation of aggravating activity (running, dancing, jumping)
- Transition to non-impact exercise (swimming, cycling)
- Stiff-soled shoe or rocker-bottom shoe to limit MTPJ extension
- Short leg walking boot (CAM boot) for acute fractures or severe pain
- Non-weight-bearing for 2 weeks if acute fracture, then heel weight-bearing
- Dancer's Pad: Felt pad with U-shaped cutout to float the painful sesamoid
- Sesamoid Relief Orthotic: Depression under sesamoid with metatarsal bar proximal
- Full-length Custom Orthotic: With first ray extension and arch support
- NSAIDs: Ibuprofen 400mg TDS or naproxen 500mg BD for 2-4 weeks
- Ice: 15-20 minutes TDS to reduce inflammation
Initial phase focuses on pain control and offloading.
- Intrinsic Strengthening: Towel curls, marble pickups
- Gastrocnemius Stretching: Address equinus contracture
- Arch Strengthening: Short foot exercises
- FHL/FHB Strengthening: Resistance band exercises
- Corticosteroid Injection: Diagnostic and therapeutic for sesamoiditis
- Technique: Fluoroscopic or ultrasound-guided to ensure accurate placement
- Limit: Maximum 1-2 injections (risk of fat pad atrophy and tendon weakening)
- Contraindication: Infection, acute fracture
- Bone Stimulator: For stress fractures or delayed healing
- Contrast Baths: Vascular flushing
- Iontophoresis: Dexamethasone penetration
Rehabilitation phase builds strength and addresses biomechanical factors.
- Week 1-2: Walking tolerance without pain
- Week 3-4: Brisk walking and light jogging
- Week 5-8: Running progression (50%, 75%, 100% intensity)
- Week 9-12: Sport-specific drills and return to full activity
- Continue orthotic use indefinitely for impact activities
- Address biomechanical factors (cavus foot correction, equinus treatment)
- Footwear selection (avoid minimalist shoes, high heels)
Return to activity requires patience and gradual progression.
Conservative management is successful in the vast majority of cases when compliance is good and offloading is adequate.
Surgical Technique
Total Sesamoidectomy - Medial (Tibial) Approach
Technique for excision of the tibial (medial) sesamoid - the most commonly affected.
Preoperative Planning
- Confirm diagnosis: MRI showing AVN, nonunion, or arthritis
- Trial conservative: Minimum 6 months documented
- Counsel risks: Hallux valgus (10-15%), cock-up toe (5-10%), transfer metatarsalgia
- Imaging review: Assess remaining sesamoid health (avoid double sesamoidectomy)
Patient Positioning and Setup
- Position: Supine with sandbag under ipsilateral hip (prevents external rotation)
- Tourniquet: Thigh tourniquet preferred; ankle tourniquet acceptable
- Anesthesia: General or popliteal regional block (block provides excellent postop pain control)
- Fluoroscopy: Mini C-arm available to confirm complete excision
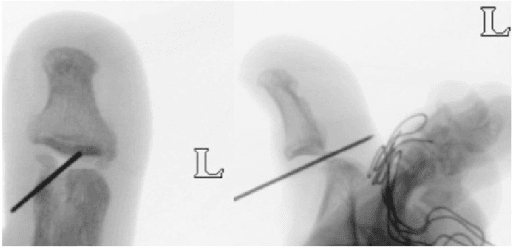
Operative Steps
- Longitudinal incision 3-4cm centered over medial aspect of MTPJ
- Avoid direct plantar incision (painful weight-bearing scar)
- Identify and protect dorsomedial cutaneous nerve (retract dorsally)
- Deepen to joint capsule in line with skin incision
- Curvilinear incision plantar to sesamoid (between weight-bearing areas)
- Higher risk to medial plantar nerve branches
- Direct visualization but potential painful scar
- Reserved for plantar pathology requiring direct access
Approach selection depends on pathology location and surgeon preference.
- Longitudinal capsulotomy along sesamoid axis
- Identify sesamoid within FHB tendon substance
- Divide metatarsosesamoid ligament (suspensory ligament)
- Inspect metatarsal head articular surface for arthritis
- Assess plantar plate integrity
Adequate exposure is essential for safe sesamoid removal.
"Shelling Out" Technique:
This is the most critical step to preserve FHB function.
- Use Beaver blade (#64 or #67) or small #15 scalpel
- Carefully dissect sesamoid from surrounding FHB tendon fibers
- Preserve as much tendon as possible - do not excise tendon with bone
- Remove all bony fragments (check with fluoroscopy)
- Inspect FHL tendon deep to sesamoid for pathology
Key Point: The sesamoid is embedded in the tendon, not attached to it. Careful dissection preserves the flexor mechanism integrity.
Meticulous technique prevents complications.
- Close the longitudinal defect in FHB tendon with #1 Vicryl or PDS suture
- Use figure-of-8 or horizontal mattress technique
- Restore tension to prevent cock-up deformity
- Ensure hallux can plantarflex actively before closure
- Tibial Sesamoidectomy: Consider abductor hallucis release if pre-existing valgus
- Fibular Sesamoidectomy: Consider adductor hallucis release to prevent varus
- Test alignment - hallux should sit in neutral without drift
Tendon repair is the most important step preventing complications.
- Capsule closed with 2-0 Vicryl (restore static stability)
- Subcutaneous layer with 3-0 Monocryl
- Skin with 3-0 or 4-0 nylon or Monocryl subcuticular
- Sterile dressing and post-op shoe or walking boot
Meticulous closure completes the procedure.
Failure to repair the FHB tendon defect is the single most common cause of cock-up toe deformity post-sesamoidectomy. The intrinsic flexor power is lost, allowing unopposed extensor pull causing MTP hyperextension and IP flexion (claw toe). Always test active plantarflexion before closure.
Sesamoid Shaving (Planing)
The surgical options table and the management algorithm both list sesamoid shaving for a plantar prominence with intractable plantar keratosis (IPK), and Richardson's review names "shaving of a prominent tibial sesamoid," but the technique is never described.
- Indication. A painful plantar prominence or intractable plantar keratosis (IPK) under the tibial sesamoid with a preserved metatarsosesamoid joint and no fracture, AVN or arthritis - the problem is mechanical prominence, not intra-articular disease. It is the least destructive surgical option and preserves the whole sesamoid and the FHB.
- Technique (planing). Through a medial or plantar-medial approach the sesamoid is exposed within the FHB without shelling it out. Using a burr or osteotome the plantar (non-articular) half is shaved/planed flush, reducing the prominence while leaving the dorsal articular surface and the FHB attachment intact. Because the FHB is not divided, the flexor mechanism and the medial buttress are preserved - avoiding the hallux valgus and cock-up risks of total excision.
- Aftercare and caveats. Offloading is similar to the non-operative protocol, with an earlier return than after excision. The main risks are inadequate debridement (persistent keratosis), fracture of the thinned sesamoid, or violating the articular surface; shaving does not help if the pain is intra-articular (arthritis or AVN), where excision is required.
Q: When and how would you shave (plane) a sesamoid rather than excise it? A: For an isolated painful plantar prominence or intractable plantar keratosis under the tibial sesamoid with a preserved joint and no fracture/AVN/arthritis. The plantar (non-articular) half is burred/planed flush through a medial approach, leaving the articular surface and FHB intact - preserving the flexor mechanism and medial buttress and avoiding the hallux valgus/cock-up risks of total excision. It fails if the pain is intra-articular, where excision is needed.
TIBIADifferential Diagnosis of Sesamoid Pain
Hook:The TIBIA bears weight - remember all causes of sesamoid pain under the first ray!
Partial Sesamoidectomy
Richardson's review lists "partial or complete resection" and the preservation-first algorithm implies it, but the surgical technique section only develops total sesamoidectomy - partial excision is never described.
- What it is. Removal of only the diseased fragment of a sesamoid (typically the smaller, avascular or ununited pole) while retaining the viable fragment and the FHB attachment. It is used for a fractured or symptomatic bipartite sesamoid where one pole is diseased, or for a stress-fracture nonunion of a bipartite sesamoid - most often the proximal-fragment excision described for medial (tibial) sesamoid stress fractures.
- Rationale. By preserving the larger viable pole and the FHB, it maintains more of the flexor lever and the medial/lateral buttress than total excision, reducing the risk of hallux valgus/varus and cock-up deformity while still removing the pain source. It is a middle option between planing and total sesamoidectomy.
- Evidence and caveats. Biedert and Hintermann reported excision of the proximal fragment in young athletes with medial-sesamoid stress fractures, with all patients pain-free and back to full sport within six months. It is only appropriate when one pole is clearly the pain source and the retained pole is viable; if the whole sesamoid is necrotic or arthritic, total excision with FHB repair is required.
Partial (Proximal-Fragment) Sesamoidectomy for Medial Sesamoid Stress Fracture
- 5 athletes (6 feet, mean age 16.8 years), mostly rhythmic gymnasts, with medial great-toe sesamoid stress fractures
- Bone scan and axial/sagittal CT were more reliable than plain films or MRI for confirming the fracture
- After failed conservative care, excision of the proximal fragment (partial sesamoidectomy) was performed in all
- All patients were pain-free and returned to full sport within six months with no complications (mean AOFAS 95.3)
Q: What is a partial sesamoidectomy and when is it indicated? A: Excision of only the diseased pole of a fractured or bipartite sesamoid, retaining the viable fragment and the FHB - most often proximal-fragment excision for a medial-sesamoid stress-fracture nonunion (Biedert and Hintermann). It preserves more of the flexor lever and buttress than total excision, lowering deformity risk, and is indicated when one pole is clearly the pain source and the other is viable; a wholly necrotic or arthritic sesamoid needs total excision with FHB repair.
Complications
- Mechanism
- Tibial sesamoidectomy removes medial buttress; unopposed lateral pull from adductor
- Prevention Strategy
- Meticulous FHB repair; consider abductor release if pre-existing valgus
- Management
- Early: orthotic and taping; Late: distal metatarsal osteotomy or MTP fusion
- Mechanism
- Fibular sesamoidectomy removes lateral stabilizer; unopposed medial pull
- Prevention Strategy
- FHB repair; consider adductor release at time of excision
- Management
- EHL split transfer (reverse Jones) or MTP fusion if rigid
- Mechanism
- Loss of FHB flexor function from inadequate tendon repair
- Prevention Strategy
- Robust tendon repair with #1 Vicryl; test active plantarflexion before closure
- Management
- Girdlestone-Taylor FDL transfer or MTP fusion
- Mechanism
- Loss of first ray weight-bearing; overload of lesser metatarsals
- Prevention Strategy
- Custom orthotic with met pad; avoid excessive first ray elevation
- Management
- Metatarsal osteotomies (Weil) to equalize metatarsal parabola
- Mechanism
- Injury to medial plantar nerve or dorsomedial cutaneous nerve
- Prevention Strategy
- Careful dissection; early identification and retraction of nerves
- Management
- Nerve excision proximal to weight-bearing area; bury in muscle
- Mechanism
- Incomplete excision of fragments; arthritis in remaining sesamoid
- Prevention Strategy
- Fluoroscopy to confirm complete removal; assess other sesamoid preop
- Management
- Revision excision or contralateral sesamoidectomy (if necessary)
- Mechanism
- Capsular fibrosis, prolonged immobilization
- Prevention Strategy
- Early ROM exercises (2 weeks postop); aggressive PT
- Management
- Manipulation under anesthesia; capsular release if severe
Complication Rates
Published literature reports:
- Overall satisfaction: 85-95% at 2-year follow-up
- Hallux valgus/varus: 5-15% (reduced with modern repair techniques)
- Cock-up toe: 5-10% (preventable with FHB repair)
- Transfer metatarsalgia: 10-20% (managed with orthotics)
- Neuroma: 5% (nerve protection critical)
The key to minimizing complications is meticulous surgical technique with emphasis on FHB tendon preservation and repair.
CHOVSesamoidectomy Complications
Hook:CHOV (Shove) away these complications with meticulous surgical technique and FHB repair!
Postoperative Care and Rehabilitation
Rehabilitation Protocol After Sesamoidectomy
- Post-op stiff-soled shoe or short leg walking boot
- Weight-bearing: Heel weight-bearing only (avoid push-off)
- Strict elevation to prevent hemarthrosis and swelling
- Keep clean and dry
- Suture or staple removal at 14 days
- Monitor for signs of infection
Immediate postoperative care focuses on wound healing.
- Start passive and active MTPJ ROM exercises at 2 weeks
- FHL excursion exercises (toe curls, towel grabs)
- Avoid aggressive dorsiflexion (protect repair)
- Transition from heel weight-bearing to full forefoot loading
- Progressive weight-bearing in stiff-soled shoe
- Wean from boot by week 4-6 based on pain
- Scar massage and desensitization (especially plantar incisions)
- Silicone sheeting to minimize hypertrophic scarring
Early mobilization prevents stiffness.
- Intrinsic foot strengthening (short foot exercises)
- Gastrocnemius/soleus stretching
- Proprioception training (single leg balance)
- Progressive resistance exercises
- Transition to supportive athletic shoe
- Custom orthotic with sesamoid cutout or dancer's pad
- Rocker-bottom sole to reduce MTPJ extension forces
Strengthening phase prepares for return to activity.
- Month 3: Walking unlimited, stationary cycling, swimming
- Month 4: Light jogging, elliptical trainer
- Month 5: Running progression (50%, 75%, 100% intensity)
- Month 6: Sport-specific drills, return to full activity
- Watch for hallux drift (valgus/varus) - early taping can correct
- Monitor for transfer metatarsalgia - adjust orthotics
- Assess for loss of push-off power - strengthen FHL/FHB
- Continue orthotic use indefinitely for impact sports
- Avoid minimalist footwear or high heels
- Maintain gastrocnemius flexibility
Return to sport requires gradual progression and monitoring.
Bone Grafting Protocol (Stricter)
For bone grafting procedures, rehabilitation is more conservative:
- NWB strict for 8 weeks in short leg cast
- Radiographs at 6 and 12 weeks to confirm union
- Transition to weight-bearing boot weeks 8-12
- Full weight-bearing by 12 weeks if healed
- Return to sport 6-9 months (slower than sesamoidectomy)
Guidelines, Registries & Global Practice
Global Epidemiology
- Population at risk: Predominantly athletes and dancers worldwide. Sesamoid injuries account for roughly 9% of foot and ankle injuries in athletic populations and up to 12% of great-toe injuries.
- Sport distribution (international): Running and sprinting (push-off loading), ballet and dance (relevé), football/soccer and rugby (forced dorsiflexion), basketball and gymnastics (jump landings), and cricket fast bowling (repetitive forefoot impact).
- Bipartite prevalence: 10-30% of the general population; bilateral in around 85%; tibial sesamoid roughly 10 times more likely to be bipartite than fibular.
- Fracture distribution: Tibial-to-fibular fracture ratio approximately 25:1, reflecting greater medial load-bearing.
Side-by-Side Society Guidance
There is no dedicated AAOS or NICE clinical practice guideline specific to sesamoid disorders; recommendations are extrapolated from foot and ankle society consensus, AO Foundation principles, and sports-medicine bodies. Where guidance genuinely differs, it is on the threshold for surgery and choice of preservation vs excision.
- Emphasis
- Preservation-first; biomechanical balance
- Practical Recommendation
- Prolonged offloading trial; sesamoid-preserving fixation/grafting before excision; mandatory FHB repair if excising
- Emphasis
- Conservative trial then staged surgery
- Practical Recommendation
- Minimum 3-6 months non-operative care; MRI confirmation before resection; avoid double sesamoidectomy
- Emphasis
- Return-to-sport optimisation in elite athletes
- Practical Recommendation
- Internal fixation favoured for stress-fracture nonunion to preserve push-off; sport-specific counselling
- Emphasis
- Individualised, stepwise algorithm
- Practical Recommendation
- Tailored decision (Artioli 2025); excision reserved for refractory symptomatic nonunion or AVN
Registry and Evidence Notes
- No national joint registry captures sesamoid procedures (they are non-arthroplasty), so the evidence base is systematic reviews of case series rather than registry survivorship data.
- Best available syntheses: Shimozono 2018 (sesamoidectomy, 196 feet), Robertson 2017 (stress-fracture return to sport), and Artioli 2025 (nonunion algorithm).
High- vs Limited-Resource Practice Variation
- High-resource settings: Early MRI and CT for diagnosis; custom orthoses; access to arthroscopic and sesamoid-preserving fixation/grafting; bone stimulators for delayed union.
- Limited-resource settings: Diagnosis often radiograph-based with contralateral comparison films; conservative management with stiff-soled footwear and felt dancer's pads; open sesamoidectomy is the dominant surgical option where preservation techniques or implants are unavailable.
Universal Consent Points for Sesamoidectomy
- Hallux valgus (after tibial excision) or varus (after fibular excision)
- Cock-up toe deformity from inadequate FHB repair
- Transfer metatarsalgia to the lesser rays
- Neuroma (medial plantar or dorsomedial cutaneous nerve)
- Loss of push-off power, career-relevant for sprinters and dancers
- Possible revision surgery
- Always document a minimum 3-6 month conservative trial and MRI-confirmed pathology, and discuss preservation alternatives in athletes.
Controversies and Areas of Uncertainty
The evidence base for sesamoid disorders is composed almost entirely of small case series and systematic reviews of them; no randomised trials and no registry data exist. Several genuine areas of debate remain.
- Argument For
- Preservation maintains FHB power and avoids deformity; union 90-100% in series
- Argument Against / Caveat
- Technically demanding, prolonged NWB, persistent nonunion risk; excision more predictable for pain
- Argument For
- Older series quote low deformity rates with good FHB repair
- Argument Against / Caveat
- Shimozono 2018 found an overall complication rate of 22.5%, higher than commonly taught
- Argument For
- Classic teaching: blood enters the proximal pole only
- Argument Against / Caveat
- Sobel 1992 shows proximal AND plantar are both major sources; distal is minor
- Argument For
- Diagnostic and therapeutic for refractory sesamoiditis
- Argument Against / Caveat
- Risk of fat-pad atrophy and tendon weakening; no high-level evidence of durable benefit
- Argument For
- Internal fixation gives best return-to-sport in athletes (Robertson 2017)
- Argument Against / Caveat
- Optimal modality undefined; many resolve with 2-6 months conservative care
MCQ Practice Points
Q: Which sesamoid is most commonly affected by fracture and AVN?
A: Tibial (medial) sesamoid - 25:1 ratio compared to fibular sesamoid. This is due to increased weight-bearing forces (tibial bears 60% of load), more prominent plantar position, and more variable vascular supply with higher AVN risk.
Q: What percentage of the population has bipartite sesamoids?
A: 10-30% of the population has bipartite sesamoids, and they are bilateral in 85% of cases. The tibial sesamoid is 10 times more likely to be bipartite than the fibular sesamoid. This is why bilateral comparison radiographs are mandatory when evaluating suspected sesamoid fractures.
Q: Why are distal pole sesamoid fractures at higher risk for AVN?
A: The blood supply enters the sesamoid via the proximal pole (branches of medial plantar artery and plantar arch). Fractures through the distal pole disrupt this vascular pedicle, creating a distal fragment with compromised blood supply that is prone to avascular necrosis and nonunion.
Q: Which sesamoid excision leads to hallux valgus deformity?
A: Tibial (medial) sesamoidectomy leads to hallux valgus. The tibial sesamoid and medial FHB act as a medial stabilizer. Excision removes this buttress, allowing unopposed lateral pull from the adductor hallucis, causing valgus drift. Prevention: meticulous FHB repair and consider prophylactic abductor hallucis release.
Q: What percentage of sesamoid disorders resolve with conservative management?
A: The majority of sesamoid disorders resolve with adequate conservative management (offloading orthotics, activity modification, NSAIDs, stiff-soled shoes). A minimum 3-6 month trial is mandatory before considering surgical intervention. Robertson et al. (2017) endorse a 2-6 month non-operative pathway before any surgery for sesamoid stress fractures.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old professional ballet dancer presents with 4 months of progressive pain under the great toe. Worse in relevé position. No specific trauma. Exam shows point tenderness over the medial plantar MTPJ and pain with passive dorsiflexion. Weight-bearing radiographs show a two-part medial sesamoid with smooth margins.”
“A 28-year-old professional footballer sustained a tibial sesamoid fracture 6 months ago. He was treated in a boot NWB for 8 weeks then progressive weight-bearing. He remains symptomatic with pain on push-off. CT scan shows a persistent 2mm fracture gap with sclerotic margins suggesting nonunion. MRI shows no AVN. He is desperate to return to professional sport.”
“A 35-year-old patient returns 18 months after tibial sesamoidectomy for chronic sesamoiditis. She complains that her big toe is drifting outward. On examination, there is 25 degrees of hallux valgus with a positive drawer test (MTP joint instability). Radiographs confirm progressive valgus deformity compared to immediate postoperative films.”
Key Anatomy
- Two sesamoids: Tibial (medial) and Fibular (lateral)
- Embedded in FHB tendons, articulate with MT head crista
- Blood supply: Proximal pole entry (medial plantar artery)
- FHL tendon runs in groove between sesamoids
- Tibial bears 60% load, Fibular 40%
Pathology Spectrum
- Sesamoiditis: Inflammation/overuse, normal X-ray, MRI edema
- Stress Fracture: Cortical break, MRI linear T2 high signal
- Acute Fracture: Sharp irregular line, unilateral
- AVN: Sclerosis, fragmentation, low T1/T2 signal
- Bipartite: Smooth margins, bilateral 85%, normal MRI
Bipartite vs Fracture (SMOOTH)
- Smooth corticated margins vs sharp jagged fracture line
- Bilateral 85% - always X-ray BOTH feet
- Larger total volume (sum of parts exceeds normal)
- MRI normal signal (bipartite) vs edema (fracture)
Conservative Management (90% success)
- Dancer's pad with U-shaped cutout to offload sesamoid
- Stiff-soled shoe or CAM boot (NWB 6 weeks for fractures)
- Activity modification: stop aggravating activity
- NSAIDs, ice, physiotherapy
- Minimum 3-6 month trial before surgery
Surgical Indications
- Failed conservative minimum 6 months
- AVN with fragmentation/collapse
- Symptomatic nonunion
- Displaced acute fracture over 2mm (ORIF consideration)
Sesamoidectomy Technique (Critical)
- Medial approach (protect dorsomedial cutaneous nerve)
- Shell out sesamoid preserving FHB tendon
- Repair FHB with #1 Vicryl (MANDATORY)
- Soft tissue balancing (abductor release if valgus risk)
- Test active plantarflexion before closure
Sesamoidectomy Complications (CHOV)
- Cock-up toe: Loss of FHB function (prevent with repair)
- Hallux Valgus: After tibial excision (loss medial buttress)
- Offloading loss: Transfer metatarsalgia (10-20%)
- Varus deformity: After fibular excision (unopposed abductor)
Exam Pearls
- Tibial:Fibular fracture ratio is 25:1
- Bipartite bilateral in 85% - check other foot
- Distal pole fractures high AVN risk (blood enters proximal)
- FHB repair is critical step preventing cock-up toe
- Sesamoidectomy 85-95% satisfaction but alters biomechanics
Evidence Base
Sesamoidectomy for Hallux Sesamoid Disorders: Systematic Review
- 10 studies, 196 feet; mean age 36.6 years, mean follow-up 45.1 months
- Mean VAS improved from 6.5 to 1.2; mean postoperative AOFAS 92.7
- 94.4% returned to sport (90.0% to previous level) at mean 11.8 weeks
- Hallux valgus angle change non-significant (13.1 to 14.8 degrees, p=0.47)
- Overall complication rate 22.5%; revision rate only 3.0%
Return to Sport After Stress Fractures of the Great Toe Sesamoids
- 14 studies of conservatively and surgically managed great-toe sesamoid stress fractures
- Standard pathway: 2-6 month conservative trial (activity modification, orthotics, analgesia, physiotherapy)
- Surgery (internal fixation or sesamoidectomy) reserved for persistent symptoms
- Internal fixation showed the best return-to-full-sport rates with low complication rates
- Optimal treatment modality not yet defined; evidence base remains low quality
Autogenous Bone Grafting of Hallux Sesamoid Nonunions
- 21 patients (mean age 33 years) with symptomatic tibial hallux sesamoid nonunion
- Autogenous bone grafting achieved bony union in all but 2 patients
- Most patients obtained symptom relief and returned to pre-injury activity level
- Procedure preserves the sesamoid and flexor hallucis brevis mechanism
- Proposed as an alternative to excision in selected, viable-bone cases
Hallux Sesamoid Nonunion: Comprehensive Systematic Review
- 6 studies, 80 patients; PRISMA-compliant synthesis of sesamoid nonunion surgery
- Techniques: open/arthroscopic sesamoidectomy, bone grafting +/- screw fixation, percutaneous screw fixation
- Union rates 90.5% to 100% with consistent functional improvement
- Complication and reoperation rates both 6.5%; commonest reoperation was salvage sesamoidectomy
- Supports a stepwise, preservation-first algorithm with excision reserved for refractory cases