Musculoskeletal Manifestations
- Sjogren syndrome is a chronic AUTOIMMUNE EXOCRINOPATHY in which lymphocytic infiltration of the LACRIMAL and SALIVARY glands produces SICCA - keratoconjunctivitis sicca (dry, gritty eyes) and xerostomia (dry mouth) - with systemic extraglandular involvement; it is PRIMARY when it occurs alone and SECONDARY when it accompanies another connective-tissue disease (rheumatoid arthritis, SLE, systemic sclerosis).
- MUSCULOSKELETAL involvement is among the most common extraglandular features: ARTHRALGIA is very frequent, and there is often a NON-EROSIVE inflammatory ARTHRITIS in a symmetric small-joint (RA-like) distribution that, unlike rheumatoid arthritis, usually does NOT cause erosive joint destruction - recognising this helps distinguish it from RA at presentation.
- MYALGIA is common, and an inflammatory MYOPATHY can occur (overlap with the inflammatory myopathies); a fibromyalgia-type widespread pain and fatigue frequently coexist and contribute to the musculoskeletal symptom burden.
- The SEROLOGY is characteristic - ANTI-Ro (SSA) and ANTI-La (SSB) antibodies, positive ANA and rheumatoid factor, and a polyclonal raised IgG - and these antibodies (especially anti-Ro) are important beyond diagnosis (e.g. neonatal lupus/congenital heart block in pregnancy); classification uses validated criteria incorporating serology and gland involvement.
- A clinically important feature is the increased risk of B-cell (MALT) LYMPHOMA in Sjogren syndrome, so persistent salivary-gland swelling, lymphadenopathy or new systemic features warrant vigilance - this is the most serious complication and a recurring exam point.
- MANAGEMENT is directed at SYMPTOMS and the SYSTEMIC disease: symptomatic care of the sicca (artificial tears/saliva), NSAIDs, and DMARDs/immunosuppression for significant systemic involvement; the ORTHOPAEDIC relevance is mainly to recognise Sjogren syndrome as the systemic disease behind a seropositive, usually non-erosive arthritis (and to coordinate joint care, sicca and perioperative considerations with rheumatology).
- KNOW THAT HYDROXYCHLOROQUINE FAILED ITS TRIAL. It is the most-prescribed immunosuppressant in Sjogren, but in the JOQUER randomised double-blind trial (n = 120, 400 mg daily versus placebo for 24 weeks) the primary endpoint was met by 17.9% on drug versus 17.2% on placebo (OR 1.01, 95% CI 0.37-2.78, P = 0.98) - and it had NO efficacy even in patients with anti-SSA antibodies, high IgG or systemic involvement. Blood levels confirmed adherence, so this is not a compliance artefact. The trial measured dryness, pain and fatigue over 24 weeks rather than articular inflammation specifically, but the honest position is that no drug has been shown to relieve the symptom burden of primary Sjogren syndrome.
- JOINT INVOLVEMENT IS THE RULE, AND IS NOT ALWAYS NON-EROSIVE. In a cohort of 133 patients, 115 (86%) had articular involvement and 91 (68%) already had it when Sjogren was diagnosed; hands and wrists were commonest, then knees, shoulders and ankles. The spectrum runs from arthralgia through to EROSIVE ARTHRITIS RESEMBLING RA - most cases are mild and self-limiting, but an erosive course occurs and does not by itself reclassify the patient as rheumatoid.
- “Sjogren = autoimmune exocrinopathy (sicca: dry eyes + mouth) + anti-Ro (SSA)/anti-La (SSB). PRIMARY (alone) vs SECONDARY (with RA/SLE/other CTD).
- “MSK: arthralgia is VERY common; arthritis is usually NON-EROSIVE (RA-like distribution but not destructive). Myalgia/inflammatory myopathy can occur.
- “Key complication = increased B-cell (MALT) LYMPHOMA risk - be alert to persistent gland swelling/lymphadenopathy.
- “HYDROXYCHLOROQUINE FAILED ITS RCT (JOQUER, n = 120): 17.9% vs 17.2% responders, OR 1.01, P = 0.98, with no efficacy even in anti-SSA-positive, high-IgG or systemically involved patients. Adherence was verified by blood levels.
- “Articular involvement in 115 of 133 (86%), present at diagnosis in 68%; hands/wrists then knees, shoulders, ankles. Usually non-erosive - but the spectrum extends to EROSIVE arthritis resembling RA.
Sicca (dry eyes/mouth) + arthralgia and a usually non-erosive RA-like arthritis, with anti-Ro (SSA)/anti-La (SSB) antibodies. Primary (alone) or secondary (with RA/SLE/CTD).
Increased risk of B-cell (MALT) lymphoma - persistent salivary-gland swelling or lymphadenopathy needs vigilance/investigation.
What It Is & Its Musculoskeletal Footprint
Sjogren syndrome is a chronic autoimmune exocrinopathy - lymphocytic infiltration of the lacrimal and salivary glands causing sicca (dry eyes and mouth) - that is primary (alone) or secondary (with another connective-tissue disease). Musculoskeletal involvement is among the commonest extraglandular features: arthralgia is very frequent and there is often a non-erosive inflammatory arthritis in an RA-like symmetric small-joint distribution that, unlike rheumatoid arthritis, usually does not destroy the joints; myalgia and an inflammatory myopathy can also occur. The serology - anti-Ro (SSA)/anti-La (SSB), ANA, rheumatoid factor and a raised IgG - is characteristic, and there is an increased risk of B-cell (MALT) lymphoma.
- Sjogren syndrome
- Usually NON-erosive
- Rheumatoid arthritis
- Erosive, destructive
- Sjogren syndrome
- Symmetric small-joint (RA-like)
- Rheumatoid arthritis
- Symmetric small-joint
- Sjogren syndrome
- Anti-Ro (SSA)/anti-La (SSB)
- Rheumatoid arthritis
- Anti-CCP / rheumatoid factor
- Sjogren syndrome
- Prominent (dry eyes/mouth)
- Rheumatoid arthritis
- Can be secondary Sjogren
- Sjogren syndrome
- B-cell (MALT) lymphoma
- Rheumatoid arthritis
- Erosive joint destruction
Diagnosis: Objective Tests and the 2016 Classification Criteria
- Ocular tests. The Schirmer test (filter paper in the lower fornix; abnormal at 5 mm or less of wetting in 5 minutes) and the ocular staining score (lissamine green/fluorescein; abnormal at 5 or more) confirm the keratoconjunctivitis sicca.
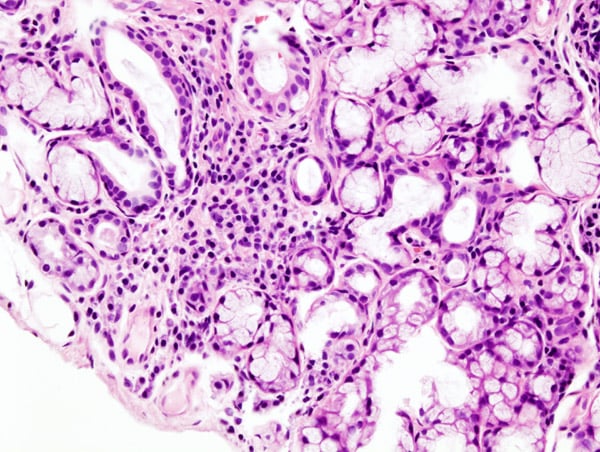
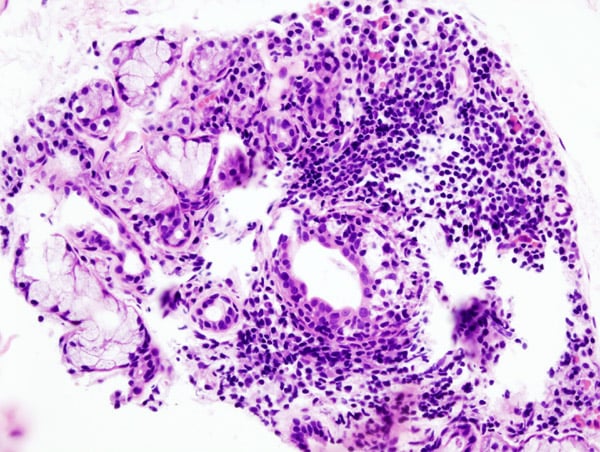
- Oral/glandular tests. Unstimulated whole salivary flow (abnormal at 0.1 mL/min or less) and the histological hallmark - a labial (minor) salivary-gland biopsy showing focal lymphocytic sialadenitis with a focus score of at least 1 (one or more foci of 50 or more lymphocytes per 4 mm squared).
- The 2016 ACR/EULAR classification criteria. In a patient with sicca symptoms and no exclusions, a weighted score in which focus score of at least 1 (3 points) and anti-Ro/SSA positive (3 points) are the two heavy items, plus one point each for ocular staining, Schirmer and salivary flow; a total of at least 4 points classifies Sjogren. Note that anti-La/SSB is NOT weighted in the 2016 criteria - only anti-Ro/SSA counts.
Q: How is Sjogren syndrome diagnosed and classified?
A: Confirm the sicca objectively - Schirmer test (5 mm or less per 5 min), ocular staining score (5 or more), unstimulated salivary flow (0.1 mL/min or less) - and the histological hallmark, a labial salivary-gland biopsy showing focal lymphocytic sialadenitis with a focus score of at least 1. The 2016 ACR/EULAR criteria weight the focus score (3 points) and anti-Ro/SSA (3 points) most heavily, plus a point each for ocular staining, Schirmer and salivary flow; 4 or more points classifies Sjogren. Note anti-La/SSB is NOT counted in the 2016 criteria - only anti-Ro/SSA.
The Lymphoma Risk: Why It Happens and Who Is at Risk
- Why it happens. Sjogren carries the highest lymphoma risk of the autoimmune connective-tissue diseases (roughly a 5% lifetime risk, about 15-20 times the general population). Chronic B-cell hyperactivation and antigen drive within the lymphocyte-infiltrated glands leads to clonal B-cell expansion, most often an extranodal marginal-zone (MALT) B-cell lymphoma arising in the parotid/salivary gland itself.
- The predictors (high-yield). The high-risk patient is flagged by persistent parotid/salivary-gland enlargement, lymphadenopathy or splenomegaly, palpable purpura / cutaneous vasculitis, low C4 (hypocomplementaemia), cryoglobulinaemia, a serum monoclonal band, and lymphopenia / low CD4 - these should prompt investigation (imaging, gland biopsy).
- The message. New or persistent gland swelling in Sjogren is lymphoma until proven otherwise.
Q: Why does Sjogren carry a lymphoma risk, and what predicts it?
A: Sjogren has the highest lymphoma risk of the autoimmune CTDs (~5% lifetime, ~15-20 times). Chronic B-cell hyperactivation/antigen drive in the infiltrated glands causes clonal expansion, usually an extranodal marginal-zone (MALT) lymphoma of the parotid. The high-risk patient is flagged by persistent parotid enlargement, lymphadenopathy/splenomegaly, palpable purpura/vasculitis, low C4, cryoglobulinaemia, a monoclonal band and lymphopenia/low CD4 - so persistent gland swelling is lymphoma until proven otherwise.
Management
- Sicca: artificial tears/saliva, eye/mouth care, secretagogues - symptomatic.
- Inflammatory MSK disease: NSAIDs, and DMARDs/immunosuppression for significant systemic involvement. Hydroxychloroquine is the most-prescribed drug but failed a placebo-controlled trial (17.9% versus 17.2% responders, P = 0.98), including in anti-SSA-positive and systemically involved patients - prescribe it, if at all, knowing that.
- Vigilance for lymphoma: investigate persistent salivary-gland swelling, lymphadenopathy or new systemic features.
- Orthopaedic relevance: recognise Sjogren behind a seropositive, usually non-erosive arthritis; coordinate joint care (and dry-eye/mouth and perioperative considerations) with rheumatology.
The two practical lessons in the musculoskeletal aspects of Sjogren syndrome are diagnostic. First, although the arthralgia and arthritis can look like rheumatoid arthritis in distribution, the Sjogren arthritis is usually non-erosive and is defined by anti-Ro/anti-La antibodies (rather than anti-CCP), and the prominent sicca points to the diagnosis - so a seropositive, non-erosive symmetric arthritis with dry eyes and mouth should be recognised as Sjogren (primary or secondary) rather than simply managed as rheumatoid disease. Second, Sjogren syndrome carries a well-recognised increased risk of B-cell (MALT) lymphoma, so persistent salivary-gland enlargement, new lymphadenopathy, or new systemic features should not be dismissed but investigated. For the orthopaedic surgeon the disease is mostly a systemic context to recognise behind joint symptoms, to be managed with the rheumatology team, with attention to the sicca and to perioperative immunosuppression.
Hydroxychloroquine: The Most-Prescribed Drug, and the Trial That Found It Did Not Work
Hydroxychloroquine is the most frequently prescribed immunosuppressant in primary Sjogren syndrome, and it is routinely offered for the arthralgia. The best evidence does not support that practice, and a candidate who quotes hydroxychloroquine as effective without the caveat is quoting habit rather than evidence.
- The trial. JOQUER randomised 120 patients with primary Sjogren syndrome across 15 French university hospitals to hydroxychloroquine 400 mg daily or placebo, double-blind, for 24 weeks.
- The result was flatly negative. The primary endpoint - a 30% or greater reduction in two of three analogue scales for dryness, pain and fatigue - was met by 17.9% (10 of 56) on hydroxychloroquine versus 17.2% (11 of 64) on placebo (odds ratio 1.01, 95% CI 0.37-2.78, P = 0.98). The pain score moved from 5.09 to 4.59 on drug and from 4.92 to 5.08 on placebo: no meaningful separation.
- It was not a compliance failure. All but one patient in the treatment arm had detectable blood levels of the drug, so the null result cannot be explained away by patients not taking it.
- The subgroups you would most expect to respond did not. Hydroxychloroquine had no efficacy in patients with anti-SSA antibodies, with high IgG, or with systemic involvement - precisely the seropositive, systemically active patients in whom it is usually justified.
- What this does and does not mean. The trial measured dryness, pain and fatigue over 24 weeks. It did not test hydroxychloroquine against articular inflammation as a specific endpoint, nor over a longer horizon, and the authors call for studies of longer-term outcomes. Serious adverse events were few and comparable between arms, so the drug is not dangerous - it is simply unproven for symptoms. Prescribing decisions sit with rheumatology, but the honest statement is that no drug has been shown to relieve the symptom burden of primary Sjogren syndrome.
How Common Is the Joint Involvement, and Is It Really Never Erosive?
"Very common" and "usually non-erosive" are both defensible, but each needs qualifying.
- The denominator. In a cohort of 133 patients with primary Sjogren syndrome, 115 (86%) had articular involvement - so joint disease is the rule, not an occasional extra. Notably, 91 patients (68% of the whole cohort) already had articular manifestations at the time of the Sjogren diagnosis, with the remainder developing them during the disease course; those whose joints declared later had been diagnosed younger and reported more dryness.
- Which joints. Hands and wrists were most frequently involved, followed by knees, shoulders and ankles
- so the distribution is not confined to the small joints.
- The important qualification to "non-erosive". Articular manifestations in primary Sjogren syndrome span a spectrum from arthralgia through to EROSIVE ARTHRITIS RESEMBLING RHEUMATOID ARTHRITIS. Most cases are mild and self-limiting, but some patients develop a chronic polyarthritis requiring DMARDs. Teaching "Sjogren arthritis is non-erosive" as an absolute will mislead: it is usually non-erosive, and an erosive course does not exclude the diagnosis or automatically reclassify the patient as rheumatoid.
- Imaging. In that cohort MRI detected more abnormalities than ultrasound, and both were used to quantify the extent of involvement and guide treatment - though this was a retrospective descriptive study with no reference standard, so it reports relative detection, not diagnostic accuracy.
Mnemonics & Memory Aids
DRYNESS
Hook:DRYNESS: Dry eyes/mouth, Ro/La antibodies, Yet usually non-erosive, Non-erosive arthritis (but erosive occurs), Either primary/secondary, Swelling -> Suspect lymphoma, Symptomatic+Systemic Rx.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient with dry eyes and dry mouth has a symmetric small-joint arthralgia. How do you approach this, and how does it differ from rheumatoid arthritis?”
What it is
- Autoimmune exocrinopathy: sicca (dry eyes/mouth) from lymphocytic gland infiltration
- Primary (alone) or secondary (with RA/SLE/other CTD)
- Serology: anti-Ro (SSA)/anti-La (SSB), ANA, RF, raised IgG
Musculoskeletal
- Articular involvement in 115 of 133 (86%); present at Sjogren diagnosis in 68%
- Hands and wrists commonest, then knees, shoulders, ankles
- Usually NON-EROSIVE - but the spectrum runs to EROSIVE arthritis resembling RA
- Myalgia common; inflammatory myopathy (overlap) can occur
- Distinguish from RA: usually non-erosive, anti-Ro/La (not anti-CCP)
Key risk
- Increased B-cell (MALT) lymphoma risk
- Investigate persistent salivary-gland swelling/lymphadenopathy
- Most serious complication
Management
- Sicca: artificial tears/saliva, secretagogues (symptomatic)
- Inflammatory MSK: NSAIDs; DMARDs/immunosuppression for significant systemic disease
- Hydroxychloroquine failed JOQUER (n = 120): 17.9% vs 17.2% responders, OR 1.01, P = 0.98
- No efficacy even in anti-SSA-positive, high-IgG or systemically involved patients (adherence verified)
- No drug has been shown in an RCT to relieve the symptom burden of primary Sjogren
- Coordinate joint care + perioperative considerations with rheumatology
Evidence & Key Studies
Effects of hydroxychloroquine on symptomatic improvement in primary Sjogren syndrome: the JOQUER randomised clinical trial
- Double-blind, placebo-controlled, multicentre randomised trial: 120 patients with primary Sjogren syndrome from 15 French university hospitals, randomised 1:1 to hydroxychloroquine 400 mg daily or placebo to week 24, then all received hydroxychloroquine to week 48.
- NEGATIVE PRIMARY ENDPOINT: a 30% or greater reduction in 2 of 3 analogue scales (dryness, pain, fatigue) at 24 weeks was achieved by 17.9% (10/56) on hydroxychloroquine versus 17.2% (11/64) on placebo - odds ratio 1.01, 95% CI 0.37-2.78, P = 0.98.
- Individual scores confirm the null: pain moved 5.09 to 4.59 on drug versus 4.92 to 5.08 on placebo; dryness and fatigue likewise showed no separation.
- NOT A COMPLIANCE PROBLEM: all but one patient in the hydroxychloroquine arm had detectable blood levels of the drug.
- Hydroxychloroquine had NO efficacy in the subgroups where it is most often justified - patients with anti-SSA autoantibodies, high IgG, or systemic involvement.
- Limitations and scope: the endpoint was dryness, pain and fatigue over 24 weeks, not articular inflammation specifically, and the authors call for evaluation of longer-term outcomes. Serious adverse events were few and comparable between arms (2 vs 3 in the first 24 weeks), so this is evidence of inefficacy for symptoms, not of harm.
Characterisation of articular manifestations in primary Sjogren's syndrome: clinical and imaging features
- 133 patients with primary Sjogren syndrome, of whom 115 (86%) had articular involvement - giving a denominator to the claim that joint involvement is 'very common'.
- 91 patients (68% of the cohort) had articular manifestations already at the time of Sjogren diagnosis, the remainder developing them during the disease course. Those developing them later had been diagnosed at a younger age and reported higher dryness scores.
- Hands and wrists were the most frequently involved sites, followed by knees, shoulders and ankles - so involvement is not restricted to the small joints.
- IMPORTANT QUALIFICATION: articular manifestations span a spectrum from arthralgia to EROSIVE ARTHRITIS RESEMBLING RHEUMATOID ARTHRITIS. Most are mild and self-limiting, but some patients develop chronic polyarthritis requiring DMARDs - so 'non-erosive' is a generalisation, not an absolute rule.
- MRI detected more abnormalities than ultrasound, and imaging was used to quantify extent and guide treatment.
- Limitations: retrospective, single-country, and a referral cohort assembled around articular manifestations, which will inflate the 86% figure relative to unselected Sjogren patients. No reference standard was used, so the MRI-versus-ultrasound comparison describes relative detection, not diagnostic accuracy. Percentages in the source are internally inconsistent in places, so the counts are quoted here in preference to derived proportions.
Rheumatic-disease arthritis of the temporomandibular joint - rehabilitative pain relief
- SCOPE CAVEAT: this review concerns the TEMPOROMANDIBULAR JOINT in rheumatic disease generally, not the peripheral joint involvement of Sjogren syndrome. Sjogren appears only as one of the rheumatic diseases encompassed. It should not be read as evidence about Sjogren arthritis of the hands, wrists or knees.
- Conservative rehabilitative approaches (for example intra-articular corticosteroid injection and low-level laser therapy) may relieve pain in rheumatic-disease-related temporomandibular arthritis, though the authors note the evidence quality is limited.
- It offers general support for a symptomatic, conservative-first approach, but supplies no Sjogren-specific prevalence, outcome or treatment-effect figure.
The hydroxychloroquine trial figures - the 17.9% versus 17.2% response, the odds ratio of 1.01 (95% CI 0.37-2.78, P = 0.98), the verified blood levels and the absence of efficacy in anti-SSA-positive, high-IgG and systemically involved patients - come from the JOQUER randomised trial (DOI), 120 patients across 15 French hospitals. The articular prevalence (115 of 133, 86%), the 68% present at diagnosis, the joint distribution and the arthralgia-to-erosive spectrum come from Carubbi (PMID 33025895), a retrospective Italian cohort assembled around articular manifestations. The temporomandibular rehabilitation review (DOI) concerns rheumatic disease of the TMJ generally and supplies no Sjogren-specific figure. The exocrinopathy and sicca, the anti-Ro/anti-La serology, the 2016 ACR/EULAR criteria and their weightings, the focus-score histology, and the B-cell (MALT) lymphoma risk with its predictors are standard, well-established teaching.
What is not established: no drug has been shown in a randomised trial to relieve the symptom burden of primary Sjogren syndrome, and there is no trial evidence supporting any specific agent for its articular disease in particular. No validated prognostic score predicts which patients progress to erosive arthritis, and no agreed surveillance interval exists for the lymphoma risk - the predictors listed are recognised risk markers that should prompt investigation, not a validated scoring system.