Progressive Arthritis from SL Dissociation | Watson Classification | Radiolunate Preserved
- Most common degenerative wrist arthritis - from chronic SL ligament incompetence
- Radiolunate joint preserved until very late (Stage IV rare) - allows motion-preserving salvage
- Identical pattern to SNAC wrist - only etiology differs (SL dissociation vs scaphoid nonunion)
- Watson classification guides treatment: Stages II-III are most common presentation
- Four-corner fusion vs PRC both preserve approximately 50% motion with comparable outcomes
- DISI pattern - dorsal intercalated segment instability from scaphoid flexion and lunate extension
- “SLAC = SNAC in pattern, different in cause
- “Radiolunate preserved = motion-preserving salvage possible
- “4CC fuses capitate-lunate-hamate-triquetrum after scaphoid excision
- “PRC removes scaphoid-lunate-triquetrum, capitate articulates with radius
SLAC is the most common pattern of degenerative wrist arthritis. Results from chronic scapholunate ligament incompetence leading to progressive carpal malalignment and cartilage degeneration. Understand the natural history and predictable progression.
Radiolunate joint preserved until very late Stage IV. This is the key anatomic feature allowing motion-preserving salvage procedures. Lunate maintains congruent articulation with radius despite surrounding arthritis.
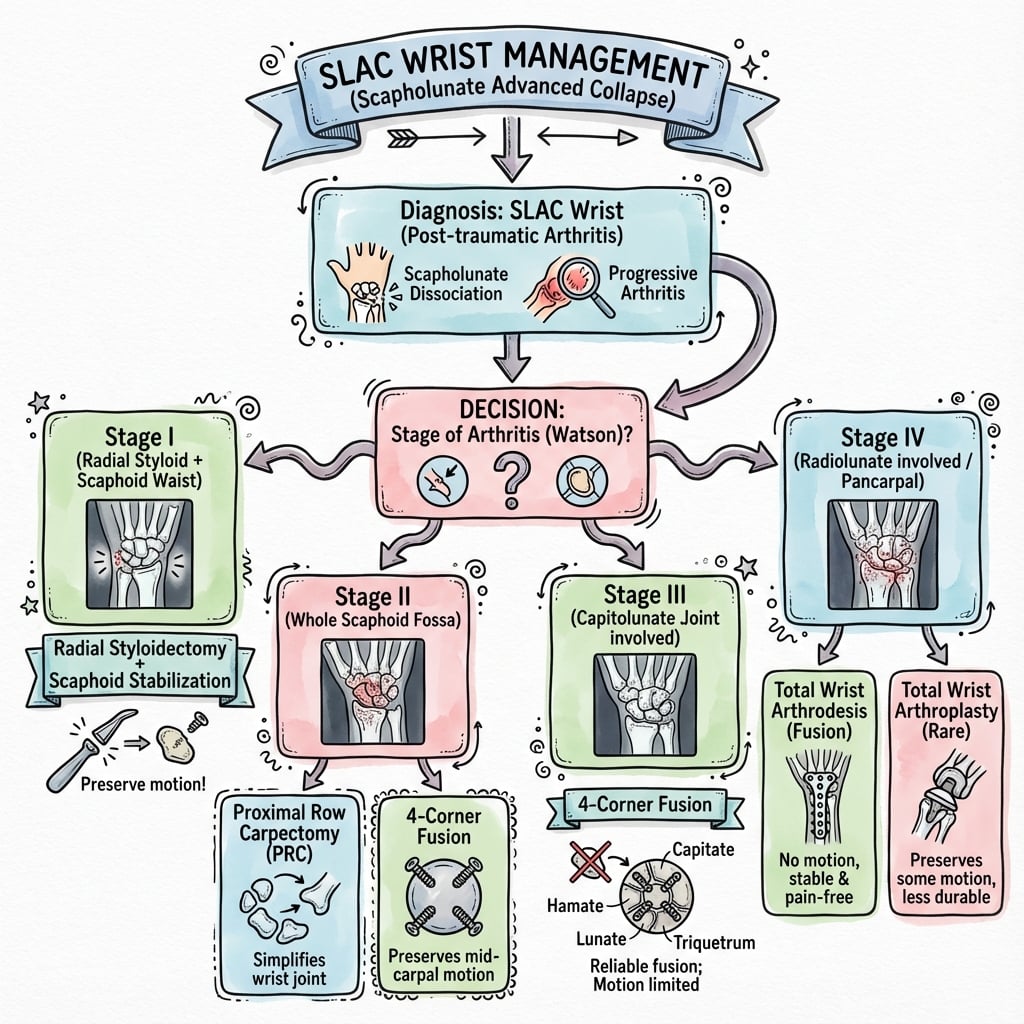
Watson staging guides treatment algorithm. Stage I: styloidectomy/denervation. Stage II-III: motion-preserving salvage (4CC or PRC). Stage IV: total wrist fusion. Most patients present at Stage II-III.
Both preserve approximately 50% motion. 4-corner fusion maintains carpal height, better grip strength. PRC is simpler surgery, faster rehab, requires intact capitate cartilage. No definitive superiority - surgeon and patient factors guide choice.
SPHERICALWhy Radiolunate Joint is Preserved
Hook:SPHERICAL lunate: The radiolunate joint stays intact because the lunate remains SPHERICAL and congruent!
PRESERVESalvage Options - 4CC vs PRC Decision
Hook:PRESERVE motion: Both procedures PRESERVE approximately 50% of wrist motion - choose based on cartilage status!
Overview and Definition
SLAC wrist is the most common pattern of degenerative wrist arthritis, making it essential knowledge for hand surgery examinations and clinical practice. Understanding the predictable progression, staging, and treatment algorithm is critical.
SLAC (Scapholunate Advanced Collapse) wrist is a pattern of progressive degenerative arthritis following chronic scapholunate ligament injury. The term was coined by Watson and Ballet in 1984 to describe the predictable sequence of arthritic changes.
Key Concepts
- Chronic SL ligament tear (most common)
- Failed SL repair or reconstruction
- Unrecognized acute injury progressing
- Idiopathic SL incompetence
Untreated SL dissociation inevitably leads to SLAC wrist over 5-15 years.
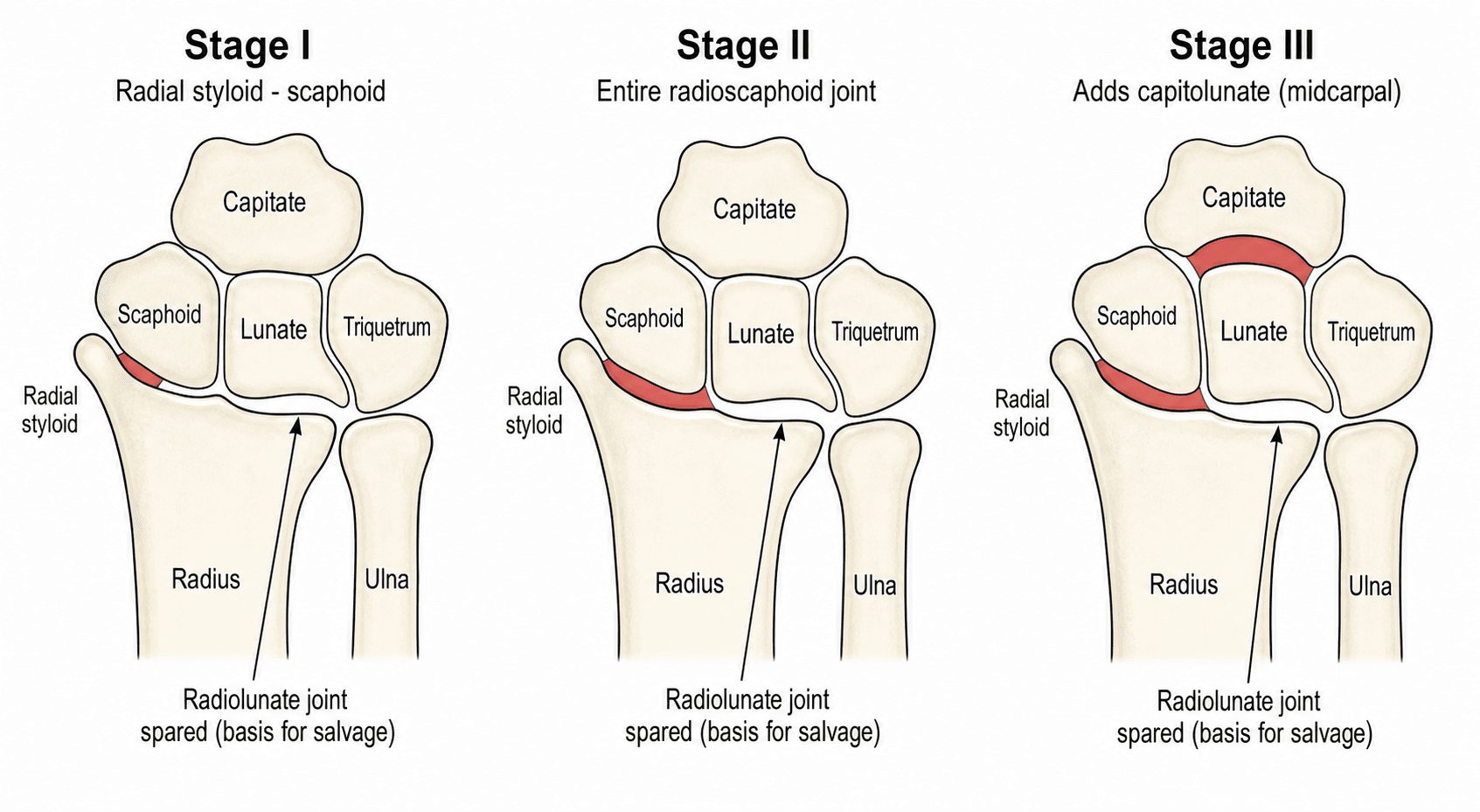
- Stage I: Radial styloid arthritis (years)
- Stage II: Radioscaphoid fossa (5-10 years)
- Stage III: Capitolunate joint (10-15 years)
- Stage IV: Pancarpal (very rare, over 20 years)
Progressive and irreversible once established.
SLAC vs SNAC Wrist
Identical arthritis pattern, different etiology:
- SLAC Wrist
- Scapholunate ligament tear
- SNAC Wrist
- Scaphoid nonunion
- SLAC Wrist
- Radial styloid → scaphoid fossa → capitolunate
- SNAC Wrist
- Identical progression
- SLAC Wrist
- Yes (until Stage IV)
- SNAC Wrist
- Yes (until Stage IV)
- SLAC Wrist
- Same staging and surgical options
- SNAC Wrist
- Same staging and surgical options
- SLAC Wrist
- More common
- SNAC Wrist
- Less common
The treatment principles are identical because the biomechanical problem (loss of scaphoid bridge function) and arthritis pattern are the same.
Anatomy
The scaphoid normally serves as a critical mechanical link between the proximal and distal carpal rows. Loss of this function (SL dissociation) leads to predictable carpal collapse and progressive arthritis.
Normal Carpal Kinematics
Scaphoid role in wrist mechanics:
- Span function: Bridges radiocarpal and midcarpal joints
- Load transmission: Transmits approximately 60% of axial load from distal row to radius
- Motion coupling: Coordinates flexion-extension between rows
- Stability: Prevents proximal migration of capitate
Consequences of SL Ligament Incompetence
- Loses connection to lunate
- Flexes with distal carpal row (driven by trapezium-trapezoid)
- Rotates into vertical position ("cortical ring sign" on PA X-ray)
- Creates abnormal contact with radial styloid (dorsal lip impingement)
- Loses scaphoid restraint
- Extends under influence of triquetrum (DISI pattern)
- Maintains normal articulation with radius (spherical geometry preserved)
- Scapholunate angle increases beyond 70 degrees
- Loses distal support from flexed scaphoid
- Migrates proximally into widened SL gap
- Creates abnormal contact with lunate
- Progressive capitolunate degeneration
The SLAC Progression Cascade
Biomechanical Cascade Leading to SLAC
Flexed scaphoid impinges on radial styloid. Abnormal point loading on dorsal lip of scaphoid against styloid tip. Osteophyte formation ("beaking"). Relatively early stage, may take several years.
Loss of congruent articulation. Scaphoid no longer sits properly in scaphoid fossa of radius. Increased contact pressure. Cartilage degeneration begins. Most common presentation.
Proximal capitate migration. Capitate moves into widened SL gap. Loss of normal capitolunate relationship. Incongruent articulation causes degeneration. Advanced stage but radiolunate still preserved.
Finally involves radiolunate. Only in very advanced, long-standing cases. Loss of spherical lunate-radius articulation. End-stage disease. No motion-preserving options remain.
Why Radiolunate Joint is Preserved
This is the key anatomic concept that allows motion-preserving salvage:
- Spherical articulation maintained
- Congruent radius of curvature unchanged
- Normal contact area preserved
- Even pressure distribution continues
The lunate "fits" normally in lunate fossa despite surrounding arthritis.
- No abnormal shear forces across joint
- Normal loading vectors maintained
- Intrinsic stability preserved
- Cartilage nutrition adequate
No mechanical factors driving degeneration at this articulation.
Clinical significance: Preserved radiolunate joint allows:
- Four-corner fusion (relies on intact radiolunate for motion)
- Proximal row carpectomy (capitate articulates with intact lunate fossa)
- Motion-preserving salvage in most patients (Stages I-III)
Pathophysiology
Mechanism of Progressive Arthritis
The progression from SL ligament tear to advanced arthritis follows a predictable biomechanical cascade:
- Scapholunate ligament rupture (acute trauma or chronic attenuation)
- Loss of scaphoid-lunate coupling
- Onset of carpal instability pattern
- Scaphoid assumes flexed position (driven by distal row)
- Lunate extends under triquetrum influence (DISI pattern)
- SL gap widens progressively (over 3mm = static instability)
- Dorsal scaphoid lip impinges on radial styloid
- Repetitive impingement at styloscaphoid articulation
- Abnormal point loading concentrates force
- Cartilage microtrauma and degradation begins
- Synovitis and osteophyte formation at styloid
- Pain localizes to radial aspect of wrist
- Loss of scaphoid bridge function complete
- Scaphoid no longer articulates congruently in fossa
- Increased contact pressure at radioscaphoid joint
- Cartilage degeneration progresses to bone-on-bone
- Subchondral sclerosis and cyst formation
- Capitate begins proximal migration into SL gap
- Proximal capitate migration exceeds 2-4mm
- Capitate head contacts lunate abnormally
- Loss of normal capitolunate articulation geometry
- Progressive capitolunate cartilage destruction
- Severe carpal collapse (carpal height ratio under 0.48)
- Radiolunate joint still preserved (spherical fit maintained)
- Only in very advanced, neglected cases
- Finally involves radiolunate articulation
- Loss of lunate spherical geometry
- Complete carpal collapse and pancarpal arthritis
- No motion-preserving options remain
Biomechanical Factors Driving Progression
60% load through radioscaphoid, 40% through radiolunate articulation.
Abnormal concentration at styloscaphoid and scaphocapitate joints. Radiolunate loading unchanged - explains preservation.
Proximal capitate migration as scaphoid bridge collapses.
Carpal height ratio decreases from 0.54 to under 0.45 in Stage III. Affects grip strength and motion.
Why Progression is Inevitable
Once SLAC arthritis begins, progression is inexorable because:
- Irreversible cartilage loss - chondrocytes cannot regenerate
- Perpetuating biomechanics - abnormal loading continues with every wrist motion
- Loss of shock absorption - cartilage loss increases bone contact pressure
- Inflammatory cascade - synovitis and cytokine release accelerate degeneration
- Subchondral bone changes - sclerosis and cysts represent end-stage damage
Clinical implication: Early intervention (SL ligament repair) prevents SLAC. Once arthritis established, salvage procedures are only option.
Classification Systems
Watson Classification (1984)
The gold standard staging system for SLAC wrist, based on radiographic arthritis pattern.
- Arthritis Location
- Radial styloid only
- Radiographic Findings
- Narrowing/sclerosis at styloid tip; scaphoid flexed
- Clinical Presentation
- Radial-sided pain, worse with radial deviation
- Arthritis Location
- Radioscaphoid fossa
- Radiographic Findings
- Sclerosis of scaphoid fossa; preserved capitolunate
- Clinical Presentation
- Diffuse dorsal pain, reduced motion 20-30%
- Arthritis Location
- Capitolunate added
- Radiographic Findings
- Proximal capitate migration; sclerosis CL joint
- Clinical Presentation
- Severe pain, reduced motion over 50%, weak grip
- Arthritis Location
- Pancarpal (radiolunate)
- Radiographic Findings
- Sclerosis/narrowing radiolunate joint
- Clinical Presentation
- End-stage; rare (under 5% of SLAC cases)
Key points:
- Stage II is the most common presentation (40-50% of patients)
- Stage III is second most common (30-40%)
- Stage I may be managed non-operatively or with styloidectomy
- Stage IV is exceedingly rare - most SLAC never reaches this stage
Staging determines surgical approach and expected outcomes.
RSCPSLAC Stage Progression (Watson Classification)
Hook:RSCP: Radial Styloid, Scaphoid fossa, CapitoLunate, Pancarpal - the predictable march of SLAC arthritis!
Clinical Assessment
- Pain: Dorsal wrist pain, activity-related
- Weakness: Grip strength reduced 30-60%
- Stiffness: Progressive loss of ROM
- Remote injury: History of wrist sprain years prior
- Occupation: Manual labor common
- Progression: Gradual worsening over years
Often no clear inciting event - insidious onset.
- Inspection: Dorsal prominence, swelling
- Palpation: Tender over dorsal wrist
- ROM: Flexion-extension reduced 30-60%
- Strength: Grip weakness 40-60% of normal
- Watson test: Usually negative (chronic, fixed)
- Provocative: Pain with axial loading
Late-stage findings, not early SL dissociation.
Clinical Findings by Stage
- Pain Pattern
- Radial-sided, activity-related
- Motion Loss
- Minimal (under 20%)
- Grip Strength
- Near normal
- Dominant Complaint
- Radial styloid pain with radial deviation
- Pain Pattern
- Dorsal wrist, constant
- Motion Loss
- Moderate (20-40%)
- Grip Strength
- Reduced 30-40%
- Dominant Complaint
- Stiffness and weakness
- Pain Pattern
- Severe, diffuse
- Motion Loss
- Severe (over 50%)
- Grip Strength
- Reduced over 50%
- Dominant Complaint
- Pain and severe functional limitation
Consider other causes of chronic wrist pain: Kienböck disease (lunate AVN), DRUJ arthritis, ulnocarpal impaction, midcarpal instability, occult scaphoid fracture/nonunion (SNAC), extensor tenosynovitis. Imaging differentiates.
Differential Diagnosis of Chronic Radial/Dorsal Wrist Pain
- Key distinguishing feature
- Intact scaphoid, widened SL gap over 3mm (Terry Thomas sign), staged radioscaphoid then capitolunate arthritis, radiolunate spared
- Best discriminating investigation
- PA + lateral radiographs; CT for staging
- Key distinguishing feature
- Scaphoid fracture nonunion with sclerosis/cysts; identical arthritis cascade but scaphoid is fractured, not just dissociated
- Best discriminating investigation
- Radiographs/CT showing waist nonunion
- Key distinguishing feature
- Lunate sclerosis, fragmentation and collapse (lunate AVN); SL gap normal
- Best discriminating investigation
- Radiographs; MRI for early (Lichtman I) disease
- Key distinguishing feature
- Ulnar-sided pain, positive ulnar variance, lunate/triquetral subchondral cysts on the ulnar side
- Best discriminating investigation
- PA radiograph (ulnar variance); MRI
- Key distinguishing feature
- Volar-radial pain at scaphotrapeziotrapezoidal joint; arthritis distal to scaphoid, radioscaphoid spared
- Best discriminating investigation
- PA radiograph showing STT joint narrowing
- Key distinguishing feature
- Ulnar-sided pain, painful/limited forearm rotation, DRUJ joint-space loss
- Best discriminating investigation
- Radiographs; CT of DRUJ in pronation/supination
- Key distinguishing feature
- Positive Watson scaphoid shift test, NO established arthritis (pre-SLAC, repairable)
- Best discriminating investigation
- Stress/clenched-fist views; arthroscopy/MRI
Special Tests
- Usually negative in SLAC wrist (chronic, fixed deformity)
- May be positive in earlier SL dissociation before arthritis
- Compare to contralateral side
- Axial load along thumb metacarpal
- Positive = pain at radioscaphoid joint
- Suggests Stage II arthritis
Investigations
Imaging Protocol for SLAC Wrist
PA, lateral, scaphoid views. PA shows: SL gap widening (over 3mm), scaphoid rotation ("cortical ring sign"), joint space narrowing, sclerosis. Lateral shows: SL angle over 70 degrees (DISI), capitolunate angle over 15 degrees, proximal capitate migration.
May reveal dynamic instability. SL gap widens with axial loading. Useful if static films normal but clinical suspicion high. Less helpful in established SLAC (already static deformity).
For surgical planning. Defines extent of arthritis (staging). Assesses capitate cartilage (critical for PRC decision). Evaluates scaphoid position and proximal pole viability. Essential before salvage surgery.
To exclude other pathology. Rules out Kienböck disease, TFCC tears, occult fractures. Assesses cartilage status. Less critical if plain films diagnostic for SLAC.
Imaging Atlas
Radiographic Staging
Stage I: Radial Styloid Arthritis
- Narrowing between scaphoid and radial styloid
- Osteophyte formation at styloid tip ("beaking")
- Scaphoid flexed (ring sign), lunate extended
- No sclerosis in scaphoid fossa of radius
- Capitolunate joint preserved
Stage II: Radioscaphoid Fossa Arthritis
- Joint space narrowing at radioscaphoid articulation
- Subchondral sclerosis in scaphoid fossa
- Proximal scaphoid pole may show cystic changes
- Capitolunate joint still preserved (key finding)
- Carpal height begins to decrease
Stage III: Capitolunate Arthritis
- Proximal migration of capitate into SL gap
- Joint space narrowing at capitolunate joint
- Sclerosis and cyst formation at CL articulation
- Severe carpal collapse (carpal height ratio under 0.48)
- Radiolunate joint STILL PRESERVED (critical)
Stage IV: Pancarpal Arthritis
- Radiolunate joint space narrowing
- Sclerosis at radiolunate articulation
- Complete carpal collapse
- Exceedingly rare (under 5% of SLAC cases)
Always obtain CT scan before four-corner fusion or PRC. Assesses: (1) capitate cartilage integrity (determines PRC feasibility), (2) exact arthritis extent (confirms staging), (3) bone quality for fusion, (4) scaphoid position for surgical planning.
Management Algorithm

Non-Operative Management
Indications:
- Patient refuses surgery
- Medical comorbidities prohibit surgery
- Low-demand, sedentary lifestyle
- Stage I with minimal symptoms
Conservative Treatment Options
Avoid provocative activities. Reduce heavy manual work. Ergonomic assessment. Job modification if possible. Success depends on patient compliance and occupation.
Wrist splint for symptom flares. Short opponens-style splint. Worn during activities. Nighttime use for pain relief. Does not alter natural history.
NSAIDs for pain control. Topical agents (diclofenac gel). Acetaminophen. Corticosteroid injections (temporary relief only). No disease-modifying effect.
Reality: Conservative treatment is palliative only in SLAC wrist. Arthritis is progressive and irreversible. Surgery is definitive treatment for most patients.
Conservative management is temporizing, not curative.
Wrist denervation is more than a Stage I adjunct: it can be offered as a stand-alone procedure at any stage for the patient who wants to keep wrist motion and avoid bony surgery. It works by dividing the articular sensory branches to the wrist — principally the terminal posterior interosseous nerve (PIN) and anterior interosseous nerve (AIN) branches (a limited PIN/AIN neurectomy), with more extensive options dividing additional dorsal and volar sensory branches (the total, Wilhelm-type denervation). Crucially it relieves pain without altering the arthritis, the carpal alignment or the range of motion — nothing is fused or excised, so it burns no bridges to a later four-corner fusion, PRC or total wrist fusion. A diagnostic local-anaesthetic block of the PIN/AIN (temporary pain relief) helps predict who will respond. The trade-offs are that it does not halt disease progression and a proportion lose benefit over time, but for a high-demand worker who needs motion, or as a lower-morbidity option in the elderly or unfit, it is a legitimate motion-preserving choice. The exam point: denervation treats the pain, not the joint.
Surgical Technique Details
Four-Corner Fusion Technique
- Supine, arm on hand table
- Tourniquet high on arm
- Forearm pronated
- Longitudinal dorsal incision (8-10cm) over Lister tubercle
- Elevate extensor retinaculum as radially-based flap
- Enter wrist between 3rd and 4th compartments
- Protect PIN branches
- Incise dorsal capsule in longitudinal T-shape
- Expose and excise entire scaphoid piecemeal
- Use rongeurs to remove all fragments
- Protect radial artery volarly
- Inspect radioscaphoid joint (confirm stage)
- Denude cartilage from:
- Proximal capitate
- Distal lunate
- Proximal hamate
- Distal triquetrum
- Use curette, rongeur, or burr
- Expose subchondral bone (bleeding surface)
- Shape surfaces for good apposition
- Pack autograft (excised scaphoid) into interfaces
- Dorsal circular plate (spider plate) most common
- Alternative: Individual screws or headless compression screws
- Plate advantages: Low profile, rigid fixation, fewer screws
- Reduce carpal alignment (20-30 degrees flexion)
- Temporary K-wire stabilization
- Apply dorsal circular plate
- Verify screw trajectories under fluoroscopy
- Insert screws (typically 4-6 screws total)
- Confirm no radiocarpal or CMC joint penetration
- Repair dorsal capsule
- Close retinaculum over plate
- Skin closure
- Short-arm cast 8-12 weeks
- Radiographs at 6 weeks for fusion assessment
- Remove cast when fusion solid
- Therapy for ROM and strengthening
Four-corner fusion is technically demanding but provides reliable outcomes.
Complications
Early Complications (Under 6 weeks)
Common to Both Procedures (4CC and PRC):
- Delayed healing (thin dorsal skin)
- Superficial infection (redness, drainage)
- Deep infection (rare, under 1%)
- Wound dehiscence (tension on closure)
Prevention: Careful skin handling, prophylactic antibiotics, early suture removal.
- Radial artery injury during scaphoid excision
- PIN neuritis from retraction
- Dorsal sensory branch injury
- Superficial radial nerve traction
Management: Recognize early, repair artery primarily, nerve injuries usually temporary.
- Malreduction (5%): Improper carpal alignment before plating
- Screw malposition (3%): Penetration into radiocarpal or CMC joints
- Plate prominence (10%): Inadequate soft tissue coverage
- Excessive bleeding (2%): From exposed cancellous surfaces
- Capitate instability (rare): If volar ligaments disrupted
Late Complications (After 6 weeks)
-
Nonunion (5-10%)
- Most common late complication
- Risk factors: smoking, NSAIDs, diabetes, poor bone quality
- May be asymptomatic or painful
- Treatment: Revision fusion with bone graft and rigid fixation
-
Plate Irritation and Tendinopathy (10-15%)
- Dorsal plate prominence causes extensor tendon irritation
- Painful tenosynovitis over 4th compartment
- Usually manifests 6-18 months postop
- Treatment: Plate removal after fusion solid (12+ months)
-
Radiocarpal Arthritis (10-20% at 10 years)
- Progressive degeneration at radiolunate joint
- May be asymptomatic or cause recurrent pain
- More common in heavy manual laborers
- Treatment: Observation if tolerable; total wrist fusion if severe
-
Progressive Arthritis (10-20% at 10 years)
- Capitate-radius articulation degeneration
- Higher risk if pre-existing capitate damage
- Presents as recurrent pain, reduced ROM
- Treatment: Activity modification; convert to total wrist fusion if failed
-
Ulnar Impaction Syndrome (5-10%)
- Carpal height loss causes ulnocarpal abutment
- DRUJ symptoms, ulnar-sided wrist pain
- Treatment: Ulnar shortening osteotomy or TFCC debridement
-
Capitate Subluxation (Under 5%)
- Instability pattern from excessive ligament stripping
- Capitate migrates dorsally or volarly
- Treatment: Revision to four-corner fusion or total fusion
Functional Complications
Common to Both:
- Incidence
- 20-30%
- Impact
- Under 30 degrees arc (goal 40-50)
- Management
- Aggressive early physiotherapy
- Incidence
- 30-40%
- Impact
- Under 60% of normal (goal 70-80%)
- Management
- Strengthening program, occupational modifications
- Incidence
- 15-25%
- Impact
- Activity-limiting discomfort despite surgery
- Management
- Wrist denervation, activity modification, revision surgery
- Incidence
- 3-5%
- Impact
- Disproportionate pain, swelling, stiffness
- Management
- Early recognition, desensitization, sympathetic blocks
Revision Surgery
- Failed salvage procedure with persistent pain (most common)
- Nonunion of four-corner fusion
- Progressive arthritis after PRC
- Hardware irritation requiring removal
- Inadequate function or motion
- After failed 4CC: Revision fusion with bone graft; convert to PRC if radiolunate intact; total wrist fusion
- After failed PRC: Convert to total wrist fusion (cannot convert to 4CC)
- Nonunion 4CC: Revision with iliac crest graft and rigid fixation
- Less predictable than primary surgery
- Total wrist fusion most reliable option
- Patient counseling critical for realistic expectations
Prevention Strategies
- Smoking cessation 6 weeks before surgery
- Optimize comorbidities (diabetes control)
- CT scan to assess cartilage and plan procedure
- Patient selection (avoid salvage in end-stage arthritis)
- Meticulous soft tissue handling
- Fluoroscopic verification of hardware placement
- Proper carpal alignment before fixation
- Preserve volar ligaments in PRC
- Appropriate immobilization duration
- Early protected ROM when allowed
- Avoid NSAIDs until fusion solid (4CC)
- Aggressive hand therapy for motion recovery
Postoperative Care and Rehabilitation
Four-Corner Fusion Outcomes
- Pain relief: 75-85% good to excellent
- Motion: 50% of normal (30-40 degrees flexion-extension)
- Grip strength: 70-80% of normal
- Patient satisfaction: 75-85%
- Fusion rate: 90-95%
- Pain relief maintained in 70-80%
- Motion stable or slight decline
- Radiocarpal arthritis develops in 10-20%
- Revision rate: 5-10%
Proximal Row Carpectomy Outcomes
- Pain relief: 75-85% good to excellent
- Motion: 50% of normal (30-40 degrees flexion-extension)
- Grip strength: 60-75% of normal
- Patient satisfaction: 80-90%
- Return to work: 3-4 months
- Pain relief maintained in 65-75%
- Progressive capitate-radius arthritis in 10-20%
- Conversion to fusion: 5-10%
- Overall satisfaction remains good
Comparative Studies
- No significant difference in pain relief
- No significant difference in motion
- Slight grip strength advantage for 4CC (10-15%)
- Faster recovery with PRC
- Lower complication rate with PRC (no nonunion)
- Equivalent long-term function
- Age: Younger patients have better functional outcomes
- Occupation: Manual laborers have lower satisfaction
- Expectations: Realistic expectations correlate with satisfaction
- Compliance: Early ROM crucial for motion recovery
Key Exam Takeaways
Definition and Etiology
- SLAC = Scapholunate Advanced Collapse - most common degenerative wrist arthritis
- Caused by chronic SL ligament incompetence (tear, failed repair, idiopathic)
- Identical pattern to SNAC wrist (scaphoid nonunion) but different etiology
- Progressive over 5-15 years: radial styloid → scaphoid fossa → capitolunate
- Radiolunate joint preserved until very late (Stage IV rare, under 5%)
Watson Classification (Staging)
- Stage I: Radial styloid arthritis only - styloidectomy or denervation
- Stage II: Radioscaphoid fossa arthritis - most common presentation (40-50%)
- Stage III: Capitolunate arthritis added - second most common (30-40%)
- Stage IV: Pancarpal arthritis (radiolunate involved) - rare, under 5%
- Staging determines treatment: I = palliative; II-III = salvage; IV = fusion
Pathophysiology
- Loss of scaphoid bridge function - cannot coordinate proximal-distal rows
- Scaphoid flexes with distal row, lunate extends (DISI pattern)
- SL angle over 70 degrees on lateral X-ray = DISI malalignment
- Abnormal contact: scaphoid dorsal lip impinges radial styloid (Stage I)
- Proximal capitate migration into SL gap causes capitolunate arthritis (Stage III)
Clinical Presentation
- Dorsal wrist pain, progressive over years, activity-related initially
- Weakness: grip strength reduced 30-60% depending on stage
- Stiffness: ROM reduced 30-60% (flexion-extension arc 40-80 degrees)
- Watson test often negative (chronic, fixed deformity unlike acute SL tear)
- Remote wrist injury history in 50%, but often no clear inciting event
Radiographic Findings
- PA view: SL gap over 3mm (Terry Thomas sign), scaphoid ring sign (rotation)
- Lateral: SL angle over 70 degrees (DISI), capitolunate angle over 15 degrees
- Stage-specific arthritis: I = styloid; II = scaphoid fossa; III = capitolunate
- CT scan essential before salvage: assess capitate cartilage (for PRC decision)
- MRI to exclude other pathology: Kienböck, TFCC tear, occult fracture
Treatment Algorithm
- Stage I: Radial styloidectomy (4-6mm) + wrist denervation = 70-80% relief
- Stage II-III: Motion-preserving salvage - 4CC or PRC (both ~50% motion)
- Four-corner fusion: Maintains height, better grip, but nonunion risk 5-10%
- PRC: Simpler, faster recovery, requires intact capitate cartilage
- Stage IV: Total wrist fusion (reliable) or arthroplasty (selected patients)
Surgical Technique Pearls
- 4CC: Excise scaphoid, fuse capitate-lunate-hamate-triquetrum with dorsal plate
- PRC: Excise scaphoid-lunate-triquetrum, capitate articulates with radius
- Critical: Assess capitate cartilage intraoperatively - if degenerated, abort PRC
- 4CC alignment: 20-30 degrees wrist flexion, verify screws under fluoroscopy
- PRC: Preserve volar ligaments to prevent capitate subluxation instability
Outcomes and Complications
- Both 4CC and PRC: 75-85% pain relief, 50% motion, 70-80% satisfaction
- Grip strength: 4CC slightly better (70-80% vs 60-75% normal)
- 4CC complications: Nonunion 5-10%, plate irritation 10-15% (may need removal)
- PRC complications: Progressive arthritis 10-20% at 10 years, ulnar impaction 5-10%
- Conversion to total wrist fusion if salvage fails: 5-10% at long-term
High-Yield Exam Points
- SLAC is MOST COMMON degenerative wrist arthritis pattern
- Radiolunate preserved = allows motion-preserving salvage (key concept)
- SLAC vs SNAC: Same pattern, different cause, same treatment
- 4CC vs PRC: No definitive superiority - equivalent outcomes in meta-analyses
- Stage determines treatment: Do NOT offer styloidectomy for Stage II-III
Guidelines, Registries & Global Practice
Global Epidemiology
SLAC is the single most common pattern of degenerative wrist arthritis worldwide. In Watson and Ballet's defining radiographic review of 4,000 wrists, the SLAC pattern accounted for 57% of all degenerative wrist arthritis (Watson & Ballet, J Hand Surg Am 1984; PMID 6725894), confirmed in Watson and Ryu's later series at 55%, with triscaphe arthritis 26% and combined disease 14% (PMID 3955970). Presentation is typically in the fifth to sixth decade, with a male predominance reflecting the manual-labour occupations (carpentry, construction, mining, agriculture) most affected by chronic scapholunate injury. The latency from the initiating scapholunate ligament injury to symptomatic arthritis is long (commonly 5-15 years), which has medicolegal relevance for occupational-injury causation in any jurisdiction.
Guidelines and Society Guidance (Side by Side)
There is no high-level dedicated society guideline for SLAC salvage; practice is guided by systematic reviews and surgeon consensus. The table summarises how the major bodies and the evidence base frame the key decisions.
- Position on SLAC salvage
- Both 4-corner fusion and PRC endorsed as motion-preserving salvage; shared decision-making; PRC discouraged in patients under ~35y
- Evidence level
- Expert consensus + Level IV
- Position on SLAC salvage
- Stage-based approach; PRC favoured for simplicity and lower complication rate when capitate cartilage intact
- Evidence level
- Expert consensus
- Position on SLAC salvage
- Emphasises preserving the spared radiolunate joint; total wrist fusion reserved for pancarpal (Stage IV) disease or failed salvage
- Evidence level
- Expert consensus
- Position on SLAC salvage
- Equivalence of 4CC and PRC for motion and pain; complication profile differs
- Evidence level
- Level IV meta-analysis
- Position on SLAC salvage
- PRC: better motion, lower conversion-to-fusion (5.2% vs 11%); grip strength equivalent
- Evidence level
- Level IV (PMID 38416092)
Registry and Pooled Evidence
National joint registries (NJR, AOANJRR, AJRR) capture wrist arthroplasty but not the carpal salvage procedures (4CC, PRC, styloidectomy) that dominate SLAC management, so the evidence base is pooled cohort data rather than registry data:
- Largest pooled series (2024): 61 studies, 3,174 wrists - PRC associated with better motion and a lower conversion-to-fusion rate (5.2% vs 11%); grip equivalent; 4CF nonunion 8.9% (PMID 38416092).
- Systematic review (2015): 7 studies, 242 wrists - 4CC gave greater radial deviation and grip (74% vs 67%), PRC gave a wider flexion-extension arc and lower overall complication rate (14% vs 29%) (Saltzman et al., PMID 25294736).
- Long-term PRC cohort: 18% failure at minimum 10 years, concentrated entirely in patients aged 35 or younger (DiDonna et al., PMID 15523004).
Global Practice Variation
- Procedure preference: PRC predominates where simplicity, faster rehabilitation and implant-free salvage are prioritised; 4-corner fusion is favoured by surgeons prioritising carpal-height maintenance and in higher-demand patients, and is mandated when the capitate head cartilage is degenerate.
- Implant choice for 4CC: dorsal circular ("spider") plate versus headless compression screws versus K-wires varies by region and cost setting; circular-plate fixation carries a recognised dorsal-impingement/nonunion profile (Shindle et al.).
- Resource-limited settings: PRC and styloidectomy are attractive where implants, fluoroscopy or hand-therapy access are limited, as they need no internal fixation.
- Surgical-site antibiotic prophylaxis: a single preoperative dose of an intravenous first-generation cephalosporin (e.g. cefazolin) within 60 minutes of incision is the near-universal standard for clean hand surgery, with a glycopeptide alternative for beta-lactam allergy or MRSA risk.
Examination Relevance
SLAC wrist is high-yield across all major boards (FRCS Tr & Orth, FRACS, EBOT, ABOS, DNB), particularly in:
- Hand/upper-limb viva (staging, treatment algorithm, surgical technique)
- Clinical stations (chronic wrist pain presentation)
- Radiology viva (DISI deformity, Terry Thomas sign, Watson staging)
Be ready to justify the biomechanical basis for radiolunate preservation and to argue the 4CC-versus-PRC decision from the contemporary evidence above.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old male carpenter presents with 2 years of progressive left (dominant) wrist pain and weakness. He recalls a wrist sprain 8 years ago. Examination shows 40 degrees total flexion-extension arc, grip 30kg (right 55kg). Radiographs demonstrate scapholunate gap of 5mm, scapholunate angle 75 degrees, and sclerosis of the radioscaphoid fossa with preserved capitolunate joint. CT scan confirms Stage II SLAC with intact capitate cartilage. How would you manage this patient?”
“You are performing a four-corner fusion for Stage III SLAC wrist. After scaphoid excision and fusion site preparation, you are ready for fixation. The examiner asks: Walk me through your technique for applying a dorsal circular plate. What are the key technical points?”
“A 45-year-old female presents with chronic wrist pain. Radiographs show Stage II arthritis with radial styloid and radioscaphoid involvement. The examiner asks: How would you differentiate SLAC from SNAC wrist? Does it matter for treatment?”
Evidence Base
The Original SLAC Description (Watson & Ballet, 1984)
- Review of 4,000 wrist radiographs; 210 cases of degenerative arthritis analysed
- SLAC (scaphoid-lunate-radius) was the most common pattern at 57%
- Coined the term SLAC and defined the staged radiographic progression
- 18 of 19 operated patients had less pain postoperatively, none requiring analgesia
- Flexion-extension and radioulnar deviation improved after limited salvage fusion
PRC vs Scaphoid Excision + Four-Corner Arthrodesis (Direct Comparison)
- Two matched cohorts of 19 patients (PRC vs scaphoid excision + 4-corner fusion)
- Flexion-extension arc near-identical: 81 degrees (PRC) vs 80 degrees (4CC)
- Grip strength 71% (PRC) vs 79% (4CC) of the opposite wrist
- 4CC group retained greater radial deviation
- Pain relief and patient satisfaction equivalent between procedures
Meta-analysis: Four-Corner Fusion vs PRC for SLAC/SNAC (3,174 wrists)
- 61 studies, 3,174 wrists (54% PRC, 46% 4CF); mean follow-up 61 months
- PRC gave significantly greater postoperative extension and ulnar deviation
- No significant difference in grip strength between the procedures
- Subsequent arthrodesis required in 5.2% (PRC) vs 11% (4CF)
- 4CF nonunion rate 8.9% (57/640) with 2.2% hardware removal rate
Landmark Series: Scaphoid Excision + Limited Fusion (4CC) for SLAC
- 100 cases treated with scaphoid excision and limited wrist arthrodesis
- Flexion-extension averaged 72 degrees (53% of the normal opposite wrist)
- Grip strength averaged 80% of the contralateral side
- Radiolunate joint preserved in 98/100 - the basis for motion-sparing salvage
- Nonunion in only 3 cases; capitate-radius impingement (technique-related) in 12%
Long-term PRC Outcomes (minimum 10-year follow-up)
- 22 wrists; average follow-up 14 years (minimum 10 years)
- 4 failures (18%) requiring fusion - all in patients aged 35 years or younger
- Non-failed wrists: flexion-extension arc averaged 72 degrees, grip 91% of opposite side
- Radiocapitate space narrowing on radiographs did NOT correlate with clinical outcome
- Caution advised before performing PRC in patients younger than 35 years
Defining Epidemiology: Evolution of Wrist Arthritis Patterns
- About 95% of wrist degenerative arthritis is periscaphoid in distribution
- SLAC pattern accounted for 55% of cases (the most common pattern)
- Triscaphe (STT) arthritis 26%; combined SLAC + triscaphe 14%
- SLAC progression is driven by scaphoid-radius articular malalignment
- Capitolunate change is secondary to carpal collapse - confirming the staged cascade
References
-
Watson HK, Ballet FL. The SLAC wrist: scapholunate advanced collapse pattern of degenerative arthritis. J Hand Surg Am. 1984;9(3):358-365.
-
Watson HK, Ryu J. Evolution of arthritis of the wrist. Clin Orthop Relat Res. 1986;(202):57-67.
-
Ashmead D 4th, Watson HK, Damon C, Herber S, Paly W. Scapholunate advanced collapse wrist salvage. J Hand Surg Am. 1994;19(5):741-750.
-
Wyrick JD, Stern PJ, Kiefhaber TR. Motion-preserving procedures in the treatment of scapholunate advanced collapse wrist: proximal row carpectomy versus four-corner arthrodesis. J Hand Surg Am. 1995;20(6):965-970.
-
Krakauer JD, Bishop AT, Cooney WP. Surgical treatment of scapholunate advanced collapse. J Hand Surg Am. 1994;19(5):751-759.
-
DiDonna ML, Kiefhaber TR, Stern PJ. Proximal row carpectomy: study with a minimum of ten years of follow-up. J Bone Joint Surg Am. 2004;86(11):2359-2365.
-
Dacho AK, Baumeister S, Germann G, Sauerbier M. Comparison of proximal row carpectomy and midcarpal arthrodesis for the treatment of scaphoid nonunion advanced collapse (SNAC-wrist) and scapholunate advanced collapse (SLAC-wrist) in stage II. J Plast Reconstr Aesthet Surg. 2008;61(10):1210-1218.
-
Cohen MS, Kozin SH. Degenerative arthritis of the wrist: proximal row carpectomy versus scaphoid excision and four-corner arthrodesis. J Hand Surg Am. 2001;26(1):94-104.
-
Vanhove W, De Vil J, Van Seymortier P, Boone B, Verdonk R. Proximal row carpectomy versus four-corner arthrodesis as a treatment for SLAC (scapholunate advanced collapse) wrist. J Hand Surg Eur Vol. 2008;33(2):118-125.
-
Lumsden BC, Stone A, Engber WD. Treatment of advanced-stage Kienböck's disease with proximal row carpectomy: an average 15-year follow-up. J Hand Surg Am. 2003;28(3):422-430.
-
Saltzman BM, Frank JM, Slikker W, Fernandez JJ, Cohen MS, Wysocki RW. Clinical outcomes of proximal row carpectomy versus four-corner arthrodesis for post-traumatic wrist arthropathy: a systematic review. J Hand Surg Eur Vol. 2015;40(5):450-457.
-
Wall LB, Didonna ML, Kiefhaber TR, Stern PJ. Proximal row carpectomy: minimum 20-year follow-up. J Hand Surg Am. 2013;38(8):1498-1504.
-
Chim H, Moran SL. Long-term outcomes of proximal row carpectomy: a systematic review of the literature. J Hand Surg Eur Vol. 2012;37(9):787-793.
-
Mulford JS, Ceulemans LJ, Nam D, Axelrod TS. Proximal row carpectomy vs four corner fusion for scapholunate (SLAC) or scaphoid nonunion advanced collapse (SNAC) wrists: a systematic review of outcomes. J Hand Surg Eur Vol. 2009;34(2):256-263.
-
Shindle MK, Burton KJ, Weiland AJ, Domb BG, Wolfe SW. Complications of circular plate fixation for four-corner arthrodesis. J Hand Surg Eur Vol. 2007;32(1):50-53.