Progressive Arthritis | Identical Pattern to SLAC | Motion-Preserving Salvage
- Identical arthritis pattern to SLAC wrist - only etiology differs (nonunion vs SL dissociation)
- Radiolunate joint preserved until Stage IV - allows motion-preserving procedures
- Stage I window: May still attempt nonunion repair with styloidectomy
- Stage II/III treatment: 4-corner fusion or proximal row carpectomy - comparable outcomes
- Few nonunions are free of arthritis beyond 10 years (Mack 1984); mean duration to radioscaphoid arthritis approximately 17 years
- “SNAC = SLAC pattern from different etiology
- “Lunate stays congruent with radius - preserved articulation
- “4CC fuses capitate-lunate-hamate-triquetrum after scaphoid excision
- “PRC removes entire proximal row - capitate articulates with lunate fossa
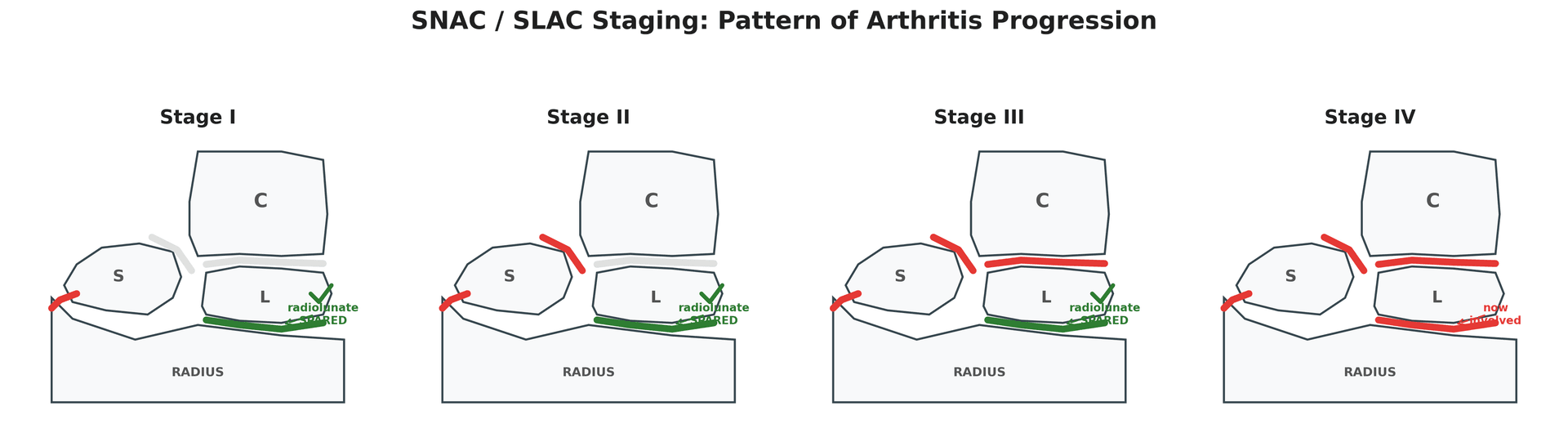
Identical arthritis progression: Radial styloid then scaphocapitate then capitolunate then pancarpal. Treatment concepts are the same - only etiology differs (nonunion vs SL dissociation).
Radiolunate joint preserved until Stage IV because lunate maintains normal articulation with radius. This allows motion-preserving salvage procedures in most patients.
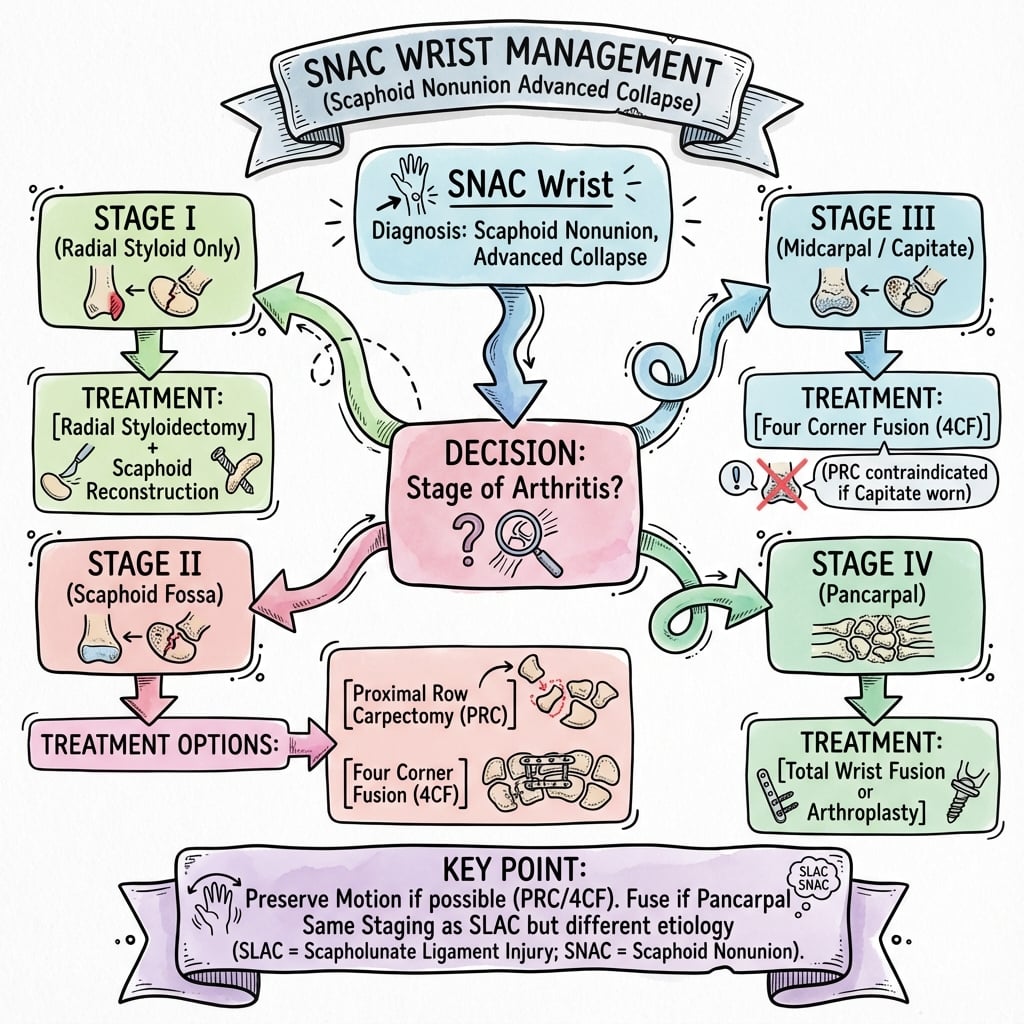
Stage I: May still repair nonunion (window closes with progression). Stage II/III: Motion-preserving salvage (4CC or PRC). Stage IV: Total wrist fusion.
Both preserve approximately 50% wrist motion with comparable outcomes. 4CC maintains carpal height better. PRC is simpler with faster rehabilitation. Choice depends on surgeon and patient factors.
Overview
SNAC (Scaphoid Nonunion Advanced Collapse) wrist represents the predictable pattern of progressive arthritis that develops following untreated or failed treatment of scaphoid nonunion. It shares an identical arthritis progression pattern with SLAC (Scapholunate Advanced Collapse) wrist, differing only in the underlying etiology.

The natural history of untreated scaphoid nonunion leads to SNAC wrist in the vast majority of cases. In the defining study by Mack et al. (1984), degenerative change followed a predictable, time-dependent sequence: lesions confined to the scaphoid at a mean of 8.2 years, radioscaphoid arthritis at 17.0 years and generalised wrist arthritis at 31.6 years, with few non-unions remaining free of arthritis beyond 10 years. Understanding this progression is essential for:
- Counseling patients regarding the importance of scaphoid nonunion treatment
- Staging the disease to guide appropriate surgical management
- Selecting motion-preserving versus motion-eliminating procedures
Anatomy
Normal Carpal Kinematics
The scaphoid serves as a critical link between the proximal and distal carpal rows:
- Span function: Bridges radiocarpal and midcarpal joints
- Load transmission: Transfers approximately 60% of axial load from distal row to radius
- Motion coupling: Coordinates proximal row flexion-extension with distal row motion
The scaphoid has a retrograde (distal-to-proximal) blood supply: the dorsal carpal branch of the radial artery enters through foramina at the dorsal ridge (distally) and supplies roughly 80% of the bone including the entire proximal pole by running proximally; the volar/distal tubercle branch supplies only the distal ~20-30%. Consequently a proximal pole fracture or nonunion cuts off the proximal fragment's supply, producing a high rate of avascular necrosis and nonunion - which is exactly why proximal-pole viability (MRI T1 signal, punctate bleeding at surgery) drives the Stage-I repair decision and the choice of a vascularized graft.
Consequences of Scaphoid Nonunion
When scaphoid nonunion occurs:
- Flexes with the distal carpal row
- Creates dorsal intercalated segment instability (DISI) pattern
- Causes abnormal contact between dorsal lip of distal fragment and radial styloid
- Extends with the lunate (remains linked)
- May develop AVN (especially proximal pole fractures)
- Loses normal articulation with distal fragment
- Abnormal point loading at styloscaphoid articulation
- Increased stress across scaphocapitate joint
- Progressive cartilage degeneration in predictable sequence
Why Radiolunate Joint is Preserved
The radiolunate joint remains congruent and normally loaded because:
- Lunate maintains spherical articulation with lunate fossa of radius
- No abnormal shear or point loading across this joint
- Preserved until very late stage disease (Stage IV - rare)
This preservation of the radiolunate articulation is the key anatomic feature that allows motion-preserving salvage procedures in SNAC wrist.
CONGRUENTWhy Radiolunate Preserved
Hook:CONGRUENT lunate: The radiolunate joint stays CONGRUENT until very late disease
Pathophysiology
Mechanism of Progressive Collapse
The progression from scaphoid nonunion to advanced collapse follows a predictable sequence:
Stage 1: Styloscaphoid Arthritis
- Nonunion allows distal fragment to flex
- Dorsal lip of distal fragment contacts radial styloid
- Abnormal point loading causes cartilage wear
- Osteophyte formation at styloid tip ("beaking")
Stage 2: Scaphocapitate Arthritis
- Loss of scaphoid span function
- Capitate migrates proximally
- Abnormal articulation between capitate and scaphoid fragments
- Midcarpal joint degeneration begins
Stage 3: Capitolunate Arthritis
- Further proximal migration of capitate
- Capitate-lunate articulation becomes incongruent
- Articular cartilage loss at capitolunate joint
- Radiolunate joint still preserved
Stage 4: Pancarpal Arthritis (Rare)
- Occurs only with severe long-standing disease
- Finally involves radiolunate articulation
- Loss of spherical lunate-radius relationship
- No motion-preserving options possible
In Mack et al.'s natural-history series (1984), few scaphoid nonunions remained free of arthritis beyond 10 years, with radioscaphoid arthritis appearing at a mean of approximately 17 years. The window for nonunion repair closes as arthritis progresses. Early treatment prevents this irreversible cascade.
Comparison: SNAC vs SLAC
- SNAC Wrist
- Scaphoid nonunion
- SLAC Wrist
- Scapholunate dissociation
- SNAC Wrist
- Distal fragment malrotation
- SLAC Wrist
- Scaphoid flexion, lunate extension
- SNAC Wrist
- Radial styloid OA
- SLAC Wrist
- Radial styloid OA
- SNAC Wrist
- Scaphocapitate OA
- SLAC Wrist
- Scaphocapitate OA
- SNAC Wrist
- Capitolunate OA
- SLAC Wrist
- Capitolunate OA
- SNAC Wrist
- Pancarpal (rare)
- SLAC Wrist
- Pancarpal (rare)
- SNAC Wrist
- Identical
- SLAC Wrist
- Identical
Key exam point: SNAC and SLAC wrist have identical arthritis progression patterns. The only difference is the underlying cause. This means treatment algorithms are the same for both conditions at each stage.
Classification Systems
SNAC Staging System
Radial Styloid Arthritis
Between radial styloid and scaphoid
- Styloid "beaking" (osteophyte formation)
- Narrowed styloscaphoid joint space
- Sclerosis at styloid tip
- Preserved scaphocapitate and capitolunate joints
Window for nonunion repair still open - last chance to restore near-normal wrist function
Nonunion repair with bone graft and radial styloidectomy OR motion-preserving salvage
Clinical Assessment
History
- Wrist pain, often long-standing
- Decreased grip strength
- Limited wrist motion
- History of prior scaphoid fracture (often remote)
- May recall wrist injury years prior that was never treated
- Activity-related initially
- May become constant in advanced stages
- Dorsoradial location typically
- Worse with gripping and loading
- Difficulty with push-ups or weight-bearing on hand
- Problems with twisting motions (opening jars)
- Reduced work capacity (especially manual laborers)
- Sports participation affected
Physical Examination
- Dorsal wrist swelling (synovitis)
- Reduced visible wrist motion
- Possible radial deviation deformity
- Tenderness over radial styloid
- Anatomical snuffbox tenderness
- Scaphoid tubercle tenderness
- May have palpable crepitus with motion
- Reduced flexion and extension
- Reduced radial deviation
- Document pre-operative ROM for comparison
- Watson scaphoid shift test: May be difficult due to nonunion
- Grip strength: Typically reduced
- Radiolunate grind test: Positive only in Stage IV
Provocative Testing
- Axially load wrist while moving through flexion-extension
- Positive: Pain or crepitus at midcarpal level
- Suggests Stage II or higher
- Direct pressure over capitate with wrist in neutral
- Positive: Tenderness suggests Stage III involvement
Differential Diagnosis
Dorsoradial wrist pain with degenerative change has several mimics. The key discriminator for SNAC is an established scaphoid nonunion driving the styloid-to-pancarpal pattern with a preserved radiolunate joint.
- Key distinguishing feature
- Established scaphoid nonunion; styloid then scaphocapitate then capitolunate arthritis
- Radiolunate joint
- Preserved until Stage IV
- Defining investigation
- Scaphoid-view radiographs / CT showing nonunion
- Key distinguishing feature
- Scapholunate dissociation (widened SL interval), no nonunion
- Radiolunate joint
- Preserved until Stage IV
- Defining investigation
- PA radiograph showing SL gap; identical arthritis pattern
- Key distinguishing feature
- Diffuse change without nonunion or SL gap
- Radiolunate joint
- Often involved early
- Defining investigation
- Radiographs; absence of scaphoid nonunion or SL injury
- Key distinguishing feature
- Symmetrical, periarticular erosions, raised inflammatory markers
- Radiolunate joint
- Involved early/diffusely
- Defining investigation
- Serology (RF/anti-CCP), erosive radiographic pattern
- Key distinguishing feature
- Pain at base of thumb, positive grind, radial-sided
- Radiolunate joint
- Not involved
- Defining investigation
- Trapeziometacarpal radiographs
- Key distinguishing feature
- Tendinous (1st dorsal compartment), positive Finkelstein, no joint-space loss
- Radiolunate joint
- Normal
- Defining investigation
- Clinical; ultrasound if uncertain
- Key distinguishing feature
- Lunate sclerosis/collapse rather than scaphoid pathology
- Radiolunate joint
- Lunate-centred change
- Defining investigation
- Radiographs/MRI of the lunate
Investigations
Plain Radiographs
Standard Views:
- PA view: Overall carpal alignment, joint spaces
- Lateral view: Carpal height ratio, DISI pattern
- Scaphoid views: Nonunion characteristics, fragment positions
Key X-ray Findings by Stage:
- PA View Findings
- Styloid beaking, styloscaphoid narrowing
- Lateral View Findings
- DISI pattern (SL angle greater than 70 degrees)
- PA View Findings
- Scaphocapitate narrowing, sclerosis
- Lateral View Findings
- Proximal capitate migration
- PA View Findings
- Capitolunate narrowing added
- Lateral View Findings
- Further capitate migration
- PA View Findings
- Radiolunate narrowing
- Lateral View Findings
- Complete carpal collapse
Measurements:
- Scapholunate angle: Greater than 70 degrees indicates DISI
- Carpal height ratio: Decreased with proximal migration
- Radiolunate angle: Normal until Stage IV
CT Scan
- Assess nonunion characteristics
- Evaluate proximal pole vascularity (indirect)
- Pre-operative planning for salvage procedures
- Better visualization of arthritic changes
- Nonunion site: Gap, cystic changes, sclerosis
- Fragment positions and rotation
- Articular surface integrity at each joint
- Cystic changes in carpal bones
MRI
- Proximal pole vascularity assessment (if considering repair)
- Evaluate ligamentous structures
- Assess for associated pathology
- Proximal pole signal: Low T1 signal suggests AVN
- Cartilage assessment: Can visualize articular damage
- SL ligament: Often attenuated or torn
Management
Non-operative Treatment
- May provide temporary symptom relief
- Does not alter disease progression
- Generally used only for:
- Patients unfit for surgery
- Patients declining surgery
- Bridge to definitive treatment
- Activity modification
- Splinting/bracing
- NSAIDs
- Intra-articular corticosteroid injections
Non-operative treatment does NOT prevent SNAC progression. Untreated disease continues to advance through stages. Surgery is indicated for symptomatic SNAC in appropriate surgical candidates.
Management Algorithm
S.T.A.G.ESNAC Treatment Algorithm
Hook:S.T.A.G.E guides treatment: Save (repair), Transition, Arthrodesis (4CC), Gone (PRC), End-stage (TWF)
Primary Goal: Attempt salvage of scaphoid nonunion if possible
Option 1: Nonunion Repair + Radial Styloidectomy
- Requirements:
- Viable proximal pole (MRI assessment)
- Repairable nonunion configuration
- Patient willing to accept prolonged recovery
- Technique:
- Open reduction internal fixation of nonunion
- Vascularized or non-vascularized bone graft
- Radial styloidectomy (2-3mm) to address OA
- Headless compression screw fixation
- Outcomes:
- Union rates 70-90% with appropriate selection
- If successful, prevents SNAC progression
- Return to near-normal wrist function
Option 2: Proceed to Motion-Preserving Salvage
- Indicated if:
- Proximal pole AVN present
- Nonunion not reconstructable
- Patient prefers single definitive procedure
If nonunion repair is not feasible, proceed directly to Stage II/III salvage procedures (4CC or PRC).
The graft is matched to vascularity and deformity: (1) a non-vascularized cancellous/structural graft (distal radius or iliac crest, e.g. a volar interpositional Russe/Fisk-Fernandez wedge to correct a humpback flexion deformity) for a well-vascularized nonunion; (2) a pedicled vascularized graft - the 1,2-intercompartmental supraretinacular artery (1,2-ICSRA) graft from the dorsal distal radius - for proximal-pole nonunion with avascularity; (3) a free vascularized medial femoral condyle (MFC) corticoperiosteal flap (descending genicular artery) for avascular proximal-pole nonunion, failed prior surgery, or significant bone loss/humpback, where it gives the highest union rates in AVN. Fix with a headless compression screw, and add a 2-3 mm radial styloidectomy to address the Stage-I styloid arthritis.
4CC vs PRC Comparison
- 4CC
- More demanding
- PRC
- Simpler
- 4CC
- Longer
- PRC
- Shorter
- 4CC
- 5-10%
- PRC
- None
- 4CC
- Possible
- PRC
- None
- 4CC
- Better maintained
- PRC
- Decreased
- 4CC
- Slower (8-12 weeks)
- PRC
- Faster (6-8 weeks)
- 4CC
- Similar (50%)
- PRC
- Similar (50%)
- 4CC
- Similar (80-90%)
- PRC
- Similar (80-90%)
- 4CC
- Similar
- PRC
- Similar
- 4CC
- Convert to TWF
- PRC
- Convert to TWF or TWA
- 4CC
- None
- PRC
- Capitate head + lunate fossa intact
Critical for exam: PRC requires intact cartilage on the capitate head AND the lunate fossa. If either articular surface is damaged, PRC is contraindicated - proceed to 4CC.
Surgical Technique
Step 1: Approach
- Dorsal longitudinal incision
- Develop interval between 3rd and 4th extensor compartments
- Ligate terminal branch of posterior interosseous nerve
- Perform dorsal capsulotomy
Step 2: Scaphoid Excision
- Identify and excise scaphoid completely
- Careful removal of all fragments
- Preserve volar radiocarpal ligaments
Step 3: Cartilage Preparation
- Remove cartilage from capitate, lunate, hamate, triquetrum
- Preserve subchondral bone plate initially
- Create bleeding bone surfaces
Step 4: Bone Grafting
- Harvest cancellous bone from distal radius or iliac crest
- Pack graft into prepared fusion surfaces
- Fill scaphoid void
Step 5: Fixation
- Options: Circular dorsal plate (most common), spider plate, individual screws, K-wires
- Ensure compression across all fusion surfaces
Step 6: Closure
- Capsular closure if possible
- Extensor retinaculum repair
- Skin closure and splint in neutral position
The four-corner fusion creates a stable construct while preserving the radiolunate articulation.
Complications
Four-Corner Fusion Complications
Nonunion (5-10%)
- Most significant complication
- Risk factors: Smoking, inadequate fixation, poor bone quality
- Management: Revision with bone graft, improved fixation
Hardware Problems
- Prominent hardware causing extensor tendon irritation
- Screw loosening
- Plate failure
- May require hardware removal after union
Stiffness
- ROM less than expected
- Usually from prolonged immobilization
- Therapy may improve
DRUJ Issues
- Pre-existing DRUJ arthritis may become symptomatic
- Consider concurrent Darrach or DRUJ fusion
Radiocarpal Arthritis Progression
- Radiolunate joint may develop arthritis long-term
- May require conversion to total wrist fusion
Proximal Row Carpectomy Complications
Progressive Arthritis
- Cartilage wear at radiocapitate articulation
- Concern for long-term durability
- May require conversion to fusion
Carpal Instability
- Capitate subluxation rare
- Usually stable construct
Weakness
- Grip strength typically 60-80% of normal
- Some patients disappointed with strength
Conversion to Fusion
- May be needed if progressive arthritis develops
- PRC does not "burn bridges" for future fusion
General Complications
Infection: Standard surgical infection risk Nerve injury: Superficial radial nerve, PIN Stiffness: Expected - counsel patients pre-operatively Complex regional pain syndrome: Rare but devastating
Postoperative Care
Four-Corner Fusion Protocol
- Bulky dressing and splint
- Strict elevation
- Finger range of motion exercises
- Short arm cast or removable splint
- Continue finger motion
- No loading
- Serial radiographs to assess fusion
- Begin wrist ROM when fusion evident
- Gradual strengthening
- Progressive loading as tolerated
- Full activities when fully fused (typically 3-4 months)
- Grip strengthening program
Proximal Row Carpectomy Protocol
- Bulky dressing and splint
- Elevation
- Finger motion
- Begin active wrist ROM
- Splint for comfort between exercises
- No loading
- Progressive strengthening
- Discontinue splint
- Gradual return to activities
- Full activities as tolerated
- Typically faster recovery than 4CC
Outcomes/Prognosis
Natural History Without Treatment
- Few nonunions remain free of arthritis beyond 10 years (Mack 1984); mean time to radioscaphoid arthritis approximately 17 years
- Progressive pain and functional decline
- Eventual pancarpal arthritis in some (mean approximately 31 years in Mack's series)
- Grip strength deterioration
Outcomes After Surgical Treatment
- Union rates 70-90% with proper selection
- If union achieved, good long-term function
- Prevents SNAC progression
- Pain relief: 80-90%
- ROM: 50% of normal (30-40 degrees F/E arc)
- Grip: 60-80% of normal
- Patient satisfaction: 75-85%
- Revision rate: 5-10% (mostly nonunion)
- Pain relief: 80-90%
- ROM: 50% of normal
- Grip: 60-80% of normal
- Patient satisfaction: 75-85%
- 10-year survival: 90%+ in most series
- Pain relief: 90%+
- ROM: 0 degrees (complete fusion)
- Grip: Often improves from pre-operative
- High satisfaction for appropriate patients
Guidelines, Registries & Global Practice
Global Epidemiology
- Scaphoid fracture incidence: A validated Swedish nationwide registry of 34,377 patients reported a true incidence of 22 per 100,000 person-years after correcting a 41% false-positive diagnosis rate (Swärd 2019).
- Nonunion as the substrate for SNAC: In the same registry, nonunion risk was higher in men than women (3% versus 1%), mirroring the male predominance seen in SNAC populations.
- Time course: Mack's natural-history series (1984) remains the reference: radioscaphoid arthritis at a mean of approximately 17 years and pancarpal arthritis at approximately 31 years, with displacement and carpal instability accelerating collapse.
Guidance and Society Positions, Side by Side
There is no high-level prospective randomised trial comparing four-corner fusion (4CC) and proximal row carpectomy (PRC); guidance is therefore consensus- and cohort-based rather than from formal guideline committees. Positions converge internationally:
- Position
- Stage II/III: 4CC or PRC both accepted; PRC favoured in older patients, 4CC where capitate-head or lunate-fossa cartilage is worn
- Evidence level
- Cohort / expert consensus (Level III-IV)
- Position
- Motion-preserving salvage for established midcarpal SNAC; total wrist arthrodesis reserved for pancarpal (Stage IV) or failed salvage
- Evidence level
- Cohort / consensus (Level III-IV)
- Position
- Equivalent functional outcomes for 4CC and PRC; selection by cartilage status, age and demand
- Evidence level
- Systematic review (Level III)
- Position
- Emphasis on preventing SNAC by early fixation/grafting of displaced scaphoid nonunion; low-profile constructs preferred for 4CC
- Evidence level
- Expert consensus (Level V)
Registry and Comparative Evidence
- No dedicated arthroplasty registry captures SNAC salvage, because 4CC and PRC are not implant-arthroplasty procedures (no AOANJRR/NJR/AJRR implant survival data apply). Total wrist arthroplasty for Stage IV is captured in some registries but represents a small, low-demand subset.
- The strongest comparative synthesis is Mulford 2009 (systematic review of 52 studies): comparable grip, pain relief and subjective outcomes; PRC tended to give better motion but more radiographic osteoarthritis (mostly asymptomatic).
- Age is the key practice modifier: DiDonna 2004 showed all PRC failures occurred in patients aged 35 or younger, so many surgeons favour 4CC (or attempted reconstruction) in younger, higher-demand patients.
Practice Variation
- High-resource settings offer the full ladder (vascularised grafting for Stage I, 4CC, PRC, total wrist arthroplasty for selected Stage IV).
- Limited-resource settings more often default to PRC (technically simpler, no implant cost, faster rehabilitation) or total wrist arthrodesis for advanced disease.
- In high-income settings, both 4CC and PRC are routine at hand surgery units; sports- and work-related scaphoid injuries in young men are the dominant feeder population, consistent with the registry epidemiology above.
SNAC and SLAC remain core FRACS/FRCS (Tr & Orth) topics, examined on pattern recognition, staging and the 4CC-versus-PRC decision.
MCQ Practice Points
Q: What is the relationship between SNAC wrist and SLAC wrist arthritis patterns?
A: They are identical. Both progress in the same sequence: radial styloid to scaphocapitate to capitolunate to pancarpal. The only difference is the underlying etiology (scaphoid nonunion vs scapholunate dissociation).
Q: Which carpal articulation is preserved until late-stage SNAC wrist, and why?
A: The radiolunate joint is preserved until Stage IV because the lunate maintains its normal congruent articulation with the lunate fossa of the radius. There is no abnormal loading across this joint until very late disease.
Q: What is the critical cartilage requirement for proximal row carpectomy?
A: PRC requires intact cartilage on both the capitate head AND the lunate fossa of the radius. If either surface is damaged, PRC is contraindicated - proceed to 4-corner fusion instead.
Q: Why is Stage I SNAC wrist particularly important?
A: Stage I represents the last window for nonunion repair. If the proximal pole is viable and the nonunion is repairable, treatment at Stage I can restore near-normal wrist function and prevent progression. Once Stage II develops, salvage procedures become necessary.
Q: How do outcomes compare between 4-corner fusion and proximal row carpectomy?
A: Similar outcomes for both procedures: 80-90% pain relief, approximately 50% of normal ROM (30-40 degrees flexion-extension arc), 60-80% grip strength, and 75-85% patient satisfaction. The choice is based on surgeon and patient factors, not outcome differences.
At a Glance Table
- Arthritis Location
- Radial styloid only
- Key Features
- Last window for nonunion repair; few nonunions free of arthritis beyond 10y if untreated
- Treatment Options
- Nonunion repair + styloidectomy OR motion-preserving salvage
- Arthritis Location
- Scaphocapitate added
- Key Features
- Midcarpal involvement, radiolunate preserved
- Treatment Options
- 4-corner fusion OR proximal row carpectomy
- Arthritis Location
- Capitolunate added
- Key Features
- Further proximal migration, radiolunate still preserved
- Treatment Options
- 4-corner fusion OR proximal row carpectomy
- Arthritis Location
- Pancarpal (radiolunate)
- Key Features
- Rare, all joints involved
- Treatment Options
- Total wrist fusion OR total wrist arthroplasty
R-S-C-PSNAC Stage Progression
Hook:RSC-P: Radial Styloid, ScaphoCapitate, CapitoLunate, Pancarpal - same sequence as SLAC!
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 48-year-old mechanic presents with wrist pain. He recalls injuring his wrist playing football 15 years ago but never sought treatment. X-rays show an ununited scaphoid fracture with scaphocapitate joint arthritis but a preserved radiolunate joint.”
Pattern (= SLAC)
- Radial styloid leads to Scaphocapitate leads to Capitolunate leads to Pancarpal
- Radiolunate preserved until Stage IV (rare)
- Few nonunions free of arthritis beyond 10 years if untreated (Mack 1984)
- Etiology differs (nonunion vs SL dissociation) but arthritis pattern identical
- Treatment algorithms same for SNAC and SLAC at each stage
Staging
- Stage I: Radial styloid OA only - repair window
- Stage II: Scaphocapitate OA - salvage indicated
- Stage III: Capitolunate OA added - salvage indicated
- Stage IV: Pancarpal OA (rare) - total fusion
Treatment by Stage
- Stage I: Nonunion repair + styloidectomy (if viable proximal pole)
- Stage II/III: 4CC or PRC (both preserve 50% ROM)
- Stage IV: Total wrist fusion or arthroplasty
- Stage I decision: MRI T1 signal confirms proximal pole viability for repair
- Stage II/III: Choice between 4CC and PRC based on patient factors, not outcomes
4CC vs PRC
- Similar outcomes: 80-90% pain relief, 50% ROM
- 4CC: Better carpal height, 5-10% nonunion risk
- PRC: Simpler, faster rehab, needs intact cartilage
- PRC requirement: Capitate head + lunate fossa cartilage intact
Key Points
- SNAC = SLAC pattern, different etiology
- Stage I = last chance for repair
- Radiolunate preservation enables motion-preserving salvage
- Choose 4CC vs PRC based on patient factors, not outcomes
- Mack 1984: few nonunions free of arthritis beyond 10 years; radioscaphoid OA at mean approximately 17 years
- 4CC/PRC both achieve 80-90% pain relief, 50% ROM preservation
Evidence Base
The Natural History of Scaphoid Non-Union (defining study)
- 47 symptomatic scaphoid non-unions reviewed; degenerative change followed a time-dependent sequence. Lesions confined to the scaphoid had a mean non-union duration of 8.2 years, radioscaphoid arthritis 17.0 years and generalised wrist arthritis 31.6 years.
- Few non-unions remained free of arthritis beyond 10 years; fracture displacement and carpal instability (lunate dorsiflexion of 10 degrees or more) correlated with severity.
Epidemiology of Scaphoid Fractures: Swedish Nationwide Registry
- Nationwide registry of 34,377 patients (2006-2015); validated true scaphoid fracture incidence was 22 per 100,000 person-years after correcting a 41% false-positive rate.
- Men were treated surgically more often than women (6% versus 3%) and had a higher nonunion risk (3% versus 1%).
Proximal Row Carpectomy: Minimum 10-Year Follow-Up
- 20 wrists at mean 13.1-year follow-up; 2 (10%) failed requiring radiocapitate arthrodesis. Survivors retained 63% of contralateral motion and 83% grip strength.
- Radiographic radiocapitate change did not correlate with pain or satisfaction; progressive symptomatic deterioration was not observed.
PRC Long-Term Results: Caution Under Age 35
- 22 wrists, minimum 10-year (mean 14-year) follow-up. 4 failures (18%) required fusion, and ALL occurred in patients aged 35 years or younger at surgery (p = 0.03).
- Wrists that did not fail averaged a 72-degree flexion-extension arc and 91% grip strength; radiocapitate space narrowing did not preclude a good clinical result.
Four-Corner Arthrodesis: Circular Plate vs Traditional Fixation
- 58 four-corner arthrodeses: first-generation circular dorsal plates had a 26% nonunion rate and 48% major complication rate versus 6% with traditional wires/staples/screws.
- Flexion-extension arc was approximately 48-50% of the opposite wrist with either technique; plate patients had lower satisfaction (60% versus 100%).
PRC versus Four-Corner Fusion: Systematic Review (SLAC/SNAC)
- Systematic review of 52 studies of PRC and four-corner fusion for SLAC/SNAC wrists. Grip strength, pain relief and subjective outcomes were similar; PRC tended to give better postoperative range of movement and avoided nonunion, hardware and impingement complications.
- Subsequent radiographic osteoarthritis was significantly more common after PRC, though the majority were asymptomatic at review.