Quantitative measurements linking pelvis and spine - critical for deformity surgery and THA stability
- Pelvic incidence (PI) is FIXED - does not change with position or age after skeletal maturity
- PI-LL mismatch predicts disability: under 10° good, over 20° severely disabled
- SVA (sagittal vertical axis) measures global balance: under 50mm normal, over 95mm severe imbalance
- In THA: high PI increases dislocation risk by allowing more functional pelvic tilt
- Roussouly classification: PI determines ideal spinal shape (Type 1-4)
- “PI is the fundamental parameter - all others derive from or relate to it
- “Standing lateral X-ray from C7 to femoral heads required for full assessment
- “PI-LL mismatch drives compensatory mechanisms: pelvic retroversion, knee flexion, thoracic hyperkyphosis
- “In deformity surgery, goal is LL = PI ± 9 degrees
Spinopelvic Parameters
Pelvic incidence (PI) is the ONLY FIXED parameter - it does NOT change with position, posture, or surgery. All other parameters (PT, SS, LL) are positional and can change. This is the most tested concept in exams!
Under 10° = good outcomes (ODI under 20). 10-20° = moderate disability (ODI 20-40). Over 20° = severe disability (ODI over 40). These numbers are critical for exam answers!
In deformity surgery, target lumbar lordosis should equal pelvic incidence ± 9 degrees. This is the Schwab-SRS goal and is universally accepted. Know this formula!
High PI (over 60°) or stiff spine (fusion) increases THA dislocation risk. Standing and sitting lateral films assess spinopelvic mobility. Consider dual mobility or increased anteversion.
Overview and Fundamentals
Spinopelvic parameters provide a quantitative framework for understanding the biomechanical relationship between the pelvis and spine. These measurements are essential for planning deformity correction surgery, understanding sagittal balance, and assessing total hip arthroplasty stability.
Historical Context
Evolution of Understanding
- Contribution
- Recognition that sagittal balance matters, not just coronal deformity
- Contribution
- Duval-Beaupère describes pelvic incidence (PI) as fixed morphological parameter
- Contribution
- Schwab classification links PI-LL mismatch to disability
- Contribution
- Integration into deformity surgery planning and THA instability assessment
- Contribution
- Machine learning models predict optimal alignment for individual patients
Why Spinopelvic Parameters Matter
Clinical Applications
- Deformity surgery planning: Determine correction needed (osteotomy type, number of levels)
- Outcome prediction: PI-LL mismatch predicts postoperative disability
- THA instability: High PI increases functional acetabular anteversion and dislocation risk
- Degenerative disease: PI-LL mismatch accelerates adjacent segment degeneration
- Spondylolisthesis: High PI predisposes to isthmic spondylolisthesis
Pathophysiology
Biomechanical Foundation
Spinopelvic parameters describe the biomechanical relationship between the pelvis and spine in maintaining sagittal balance. The fundamental principle is that the pelvis serves as the foundation for the spine, and pelvic morphology (PI) determines the ideal spinal curvature.
Energy-Efficient Standing
The human body seeks an energy-efficient upright posture that maintains horizontal gaze with minimal muscular effort. This requires:
- C7 vertebra aligned over the sacrum (SVA near zero)
- Reciprocal curves in sagittal plane (thoracic kyphosis balances lumbar lordosis)
- Pelvic positioning that optimizes spinal alignment
Compensatory Cascade
When ideal alignment is lost (e.g., loss of lumbar lordosis), the body activates compensatory mechanisms in sequence:
- Mechanism
- Pelvic retroversion (increased PT)
- Energy Cost
- Low - bony compensation
- Mechanism
- Knee flexion, ankle dorsiflexion
- Energy Cost
- Moderate - muscular compensation
- Mechanism
- Thoracic hyperkyphosis
- Energy Cost
- Moderate - ligamentous stress
- Mechanism
- Hip extension loss, forward lean
- Energy Cost
- High - exhausted, symptomatic
As compensation progresses, energy expenditure increases and disability worsens, correlating with increasing PI-LL mismatch and SVA.
Pelvic Parameters
Pelvic Incidence (PI)
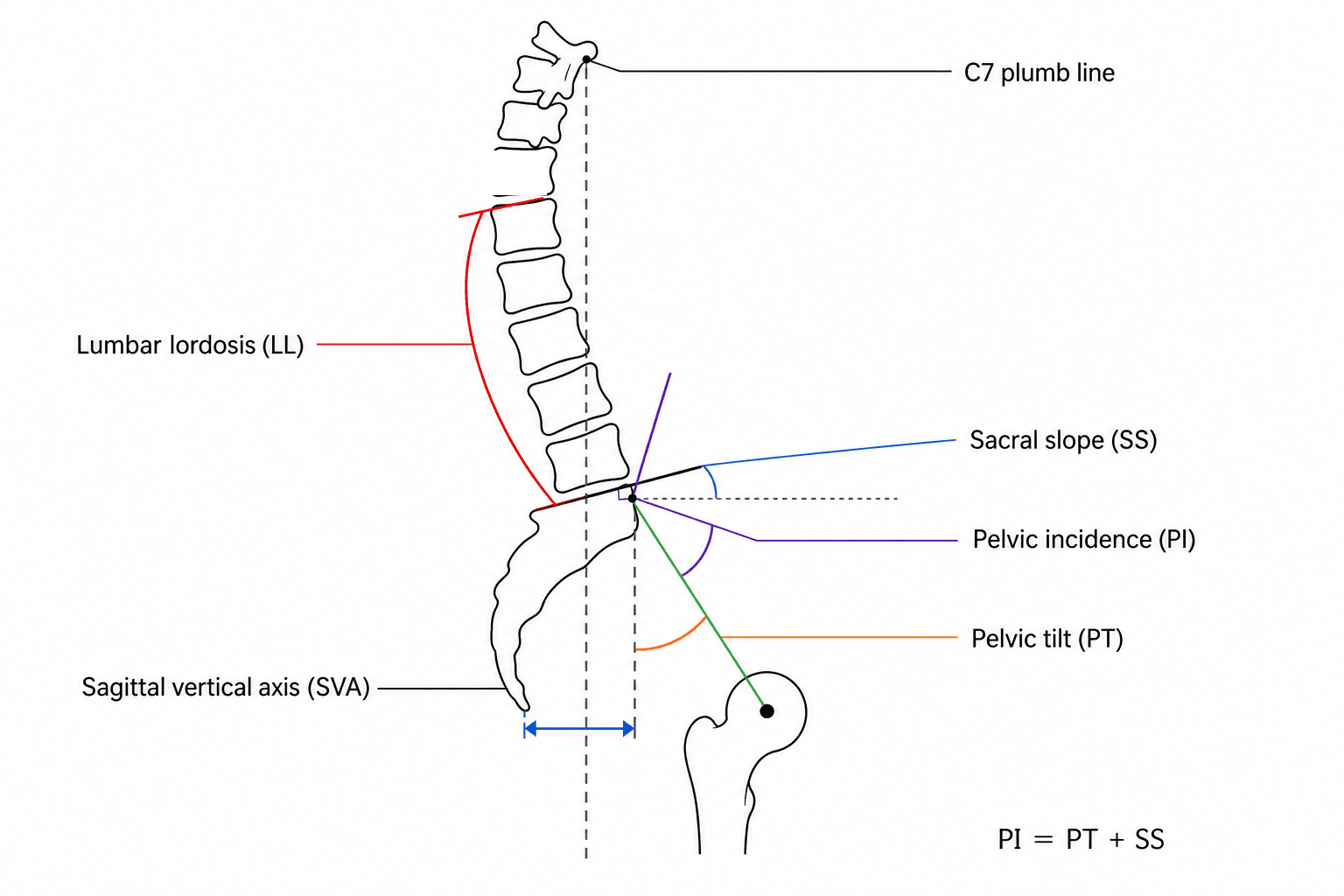
Definition: Angle between line from femoral head centers to midpoint of sacral endplate and perpendicular to sacral endplate.
Key Characteristics
- Description
- Morphological (anatomical) parameter
- Description
- FIXED - does not change with position, posture, age, or surgery
- Description
- 35-85° (average 50°)
- Description
- Under 45° - flat back tendency, Type 1-2 Roussouly
- Description
- Over 60° - hyperlordotic tendency, Type 3-4 Roussouly
- Description
- Determines ideal lumbar lordosis (LL should equal PI ± 9°)
Measurement Technique
- Identify center of both femoral heads (draw line connecting them)
- Identify midpoint of sacral endplate (S1 superior endplate)
- Draw line from femoral head midpoint to sacral endplate midpoint
- Draw perpendicular line to sacral endplate at midpoint
- Measure angle between these two lines
PI never changes: Unlike PT and SS which vary with pelvic position, PI is determined by pelvic anatomy at skeletal maturity. Even after major deformity surgery that changes LL and PT dramatically, PI remains unchanged. This makes PI the foundational parameter - know PI and you know what the patient's ideal alignment should be!
Pelvic Tilt (PT)
Definition: Angle between line from femoral head centers to midpoint of sacral endplate and vertical axis.
Key Characteristics
- Description
- Positional parameter
- Description
- Changes with pelvic rotation (retroversion/anteversion)
- Description
- 10-25° (average 12°, should be under 20°)
- Description
- Pelvic retroversion - compensatory mechanism for positive SVA
- Description
- Pelvic anteversion - seen with hip flexion contracture
- Description
- Indicates degree of compensation for sagittal imbalance
Measurement Technique
- Identify center of both femoral heads
- Identify midpoint of sacral endplate
- Draw line connecting these two points
- Draw vertical line through femoral head midpoint
- Measure angle between these lines
Compensatory Mechanisms
- Interpretation
- Normal pelvic position
- Compensation
- Minimal compensation
- Interpretation
- Moderate retroversion
- Compensation
- Moderate compensation for imbalance
- Interpretation
- Severe retroversion
- Compensation
- Severe compensation, likely symptomatic
- Interpretation
- Extreme retroversion
- Compensation
- Exhausted pelvic compensation, knee flexion needed
Sacral Slope (SS)
Definition: Angle between sacral endplate and horizontal line.
Key Characteristics
- Description
- Positional parameter
- Description
- Changes with pelvic rotation
- Description
- 30-50° (average 40°)
- Description
- PI = PT + SS (always true)
- Description
- Affects lumbar lordosis and acetabular coverage in THA
Measurement Technique
- Identify sacral endplate (S1 superior endplate)
- Draw line along sacral endplate
- Draw horizontal line
- Measure angle between sacral endplate line and horizontal
The PI = PT + SS relationship: This is ALWAYS true mathematically. If PI is fixed and you increase PT (pelvic retroversion), SS must decrease by the same amount. This explains why pelvic retroversion (compensation) flattens the sacrum and reduces lumbar lordosis - as PT increases, SS decreases, reducing the lordotic drive from the pelvis.
Spinal Parameters
Lumbar Lordosis (LL)
Definition: Cobb angle from superior endplate of L1 to superior endplate of S1 (or L1-L5 in some systems).
Key Characteristics
- Description
- 40-70° (should approximate PI ± 9°)
- Description
- LL = PI ± 9° (Schwab-SRS goal)
- Description
- L1 superior endplate to S1 superior endplate
- Description
- More lordosis at L4-5 and L5-S1 (50% of total)
- Description
- Loss of LL drives PI-LL mismatch and disability
PI-LL Mismatch
- Disability (ODI)
- Under 20
- Interpretation
- Good balance, minimal symptoms
- Disability (ODI)
- 20-40
- Interpretation
- Moderate disability, increasing compensation
- Disability (ODI)
- Over 40
- Interpretation
- Severe disability, exhausted compensation
- Disability (ODI)
- Over 50
- Interpretation
- Extreme disability, strong surgical indication
Causes of LL Loss
- Degenerative disc disease (loss of disc height anteriorly)
- Compression fractures
- Iatrogenic (flat back syndrome post-Harrington rod)
- Ankylosing spondylitis
- Previous laminectomy with muscle stripping
Thoracic Kyphosis (TK)
Definition: Cobb angle from superior endplate of T4 to inferior endplate of T12.
Key Characteristics
- Description
- 20-50° (average 40°)
- Description
- Reciprocal - increased TK often compensates for decreased LL
- Description
- TK approximately equal to LL in balanced spine
- Description
- Hyperkyphosis develops when pelvic compensation exhausted
- Description
- T4 superior to T12 inferior endplate
Sagittal Vertical Axis (SVA)
Definition: Horizontal distance from C7 plumb line to posterior-superior corner of S1 endplate.
Key Characteristics
- Category
- Normal
- Clinical Impact
- Minimal symptoms, good balance
- Category
- Moderate imbalance
- Clinical Impact
- Moderate disability, compensating
- Category
- Severe imbalance
- Clinical Impact
- Severe disability, surgical consideration
- Category
- Extreme imbalance
- Clinical Impact
- Exhausted compensation, high surgical risk
Measurement Technique
- Drop vertical plumb line from center of C7 vertebral body
- Identify posterior-superior corner of S1 endplate
- Measure horizontal distance between plumb line and S1 corner
- Positive SVA = C7 plumb line ANTERIOR to S1 (imbalance)
- Negative SVA = C7 plumb line POSTERIOR to S1 (overcorrected)
Compensatory Cascade
- SVA
- 0-50mm
- Compensation
- Pelvic retroversion (increased PT)
- SVA
- 50-80mm
- Compensation
- Knee flexion, ankle dorsiflexion
- SVA
- 80-120mm
- Compensation
- Thoracic hyperkyphosis
- SVA
- Over 120mm
- Compensation
- Hip extension loss, cannot compensate
Cervical Sagittal Alignment Parameters
The parameters above stop at the lumbar spine and pelvis, but the compensatory cascade and gaze regulation continue cranially - and the cervical analogues are examinable in their own right.
- T1 slope: the angle of the T1 superior endplate to horizontal. It behaves as the cervical spine's "pelvic incidence/sacral slope" - it sets the cervical lordosis the neck must generate to keep the head balanced (a high T1 slope demands more cervical lordosis).
- C2-C7 cervical lordosis (CL): the cervical Cobb angle.
- T1 slope minus cervical lordosis (T1S-CL) mismatch: the cervical equivalent of PI-LL. A mismatch over roughly 20 degrees indicates cervical malalignment and correlates with disability, exactly as PI-LL does in the lumbar spine.
- C2-C7 sagittal vertical axis (cSVA): plumb line from the C2 centroid to the posterosuperior corner of C7; over roughly 40 mm indicates cervical sagittal imbalance.
- Chin-brow vertical angle (CBVA): the angle between the chin-to-brow line and the vertical, with the neck in its fixed/neutral position. It is the parameter for horizontal gaze and is used to plan correction of a fixed cervical/cervicothoracic flexion deformity (classically ankylosing spondylitis) so that a cervical or C7 osteotomy restores forward gaze without over- or under-correction.
Key principle: cervical alignment is coupled to global alignment - thoracolumbar positive sagittal balance drives compensatory cervical hyperlordosis, and correcting a lumbar deformity changes the cervical requirement. Never assess the neck in isolation from the whole sagittal profile.
Roussouly Classification
Roussouly Classification of Sagittal Alignment
Roussouly described 4 types of normal sagittal spinal alignment based on pelvic incidence and the shape of lumbar lordosis. This classification helps define what "normal" looks like for individual patients.
- PI Range
- Low (under 45°)
- Sacral Slope
- Low (under 35°)
- Lordosis Shape
- Short, flat lordosis
- Characteristics
- Lordosis apex at L5, flat thoracolumbar junction
- PI Range
- Medium (45-50°)
- Sacral Slope
- Medium (35-45°)
- Lordosis Shape
- Long, harmonious lordosis
- Characteristics
- Lordosis apex at L4, balanced TK and LL
- PI Range
- High (50-60°)
- Sacral Slope
- High (45-50°)
- Lordosis Shape
- Long lordosis
- Characteristics
- Lordosis apex at L3-4, well-developed lordosis
- PI Range
- Very high (over 60°)
- Sacral Slope
- Very high (over 50°)
- Lordosis Shape
- Long, hyperlordosis
- Characteristics
- Lordosis apex at L2-3, exaggerated curves
The classification is based on the fundamental concept that PI determines the ideal spinal shape.
Clinical Assessment
History Taking
Key Symptoms
- Back pain: Location, character, aggravating/relieving factors
- Leg symptoms: Radiculopathy vs neurogenic claudication
- Walking tolerance: Distance before symptoms force rest
- Forward lean: Need to lean on shopping cart or walker
- Functional limitations: Ability to stand upright, cook, socialize
Disability Scores
- Assessment
- Oswestry Disability Index (0-100)
- Correlation
- Strong correlation with PI-LL mismatch
- Assessment
- Scoliosis Research Society questionnaire
- Correlation
- Quality of life in deformity patients
- Assessment
- Short Form 36 health survey
- Correlation
- General health status
Physical Examination
Posture Assessment
- Standing posture: Forward lean, pelvic retroversion visible
- Gait: Flexed knees, shortened stride, unsteady balance
- Plumb line: C7 falls anterior to sacrum (positive SVA)
- Compensatory mechanisms: Hip and knee flexion to maintain balance
Flexibility Testing
- Forward flexion: Assess lumbar spine mobility
- Extension: Loss of extension correlates with LL loss
- Side bending: Evaluate coronal plane flexibility
- Sitting vs standing: Change in posture and symptoms
Investigations
Imaging Protocol
Standing Lateral Radiograph
- Specification
- 36-inch cassette (full spine and pelvis)
- Specification
- Standing, comfortable stance, knees straight
- Specification
- Fists on clavicles or arms on supports (out of field)
- Specification
- C7 vertebra to femoral heads
- Specification
- Both femoral heads clearly visible
- Specification
- Adequate to visualize L5-S1 disc space
Measurement Landmarks
- Key Landmarks
- Femoral head centers, sacral endplate midpoint
- Key Landmarks
- Femoral head centers, sacral endplate midpoint, vertical
- Key Landmarks
- Sacral endplate, horizontal
- Key Landmarks
- L1 superior endplate, S1 superior endplate
- Key Landmarks
- T4 superior endplate, T12 inferior endplate
- Key Landmarks
- C7 vertebral body center, posterior-superior S1 corner
Common Measurement Errors
- Problem
- Cannot measure PI, PT
- Solution
- Ensure pelvis in field, adequate exposure
- Problem
- Obscures upper thoracic spine
- Solution
- Fists on clavicles or arms on supports
- Problem
- Alters PT, SS, creates artificial compensation
- Solution
- Instruct patient to stand with knees straight
- Problem
- Missing functional alignment
- Solution
- Must be standing radiograph
- Problem
- Artificial balance
- Solution
- Patient must stand unsupported if able
Advanced Imaging
Dynamic Imaging (THA Planning)
- Standing lateral radiograph
- Sitting lateral radiograph
- Calculate pelvic tilt change (standing to sitting)
- Stiff spine: PT change less than 10° (high dislocation risk)
- Mobile spine: PT change 20-30° (normal protective mechanism)
Flexion-Extension Films (Deformity Surgery)
- Assess lumbar spine mobility
- Rigid spine: SPO will not work, need PSO
- Mobile disc spaces: SPO may be effective
Management
Principles of Spinopelvic Alignment Restoration
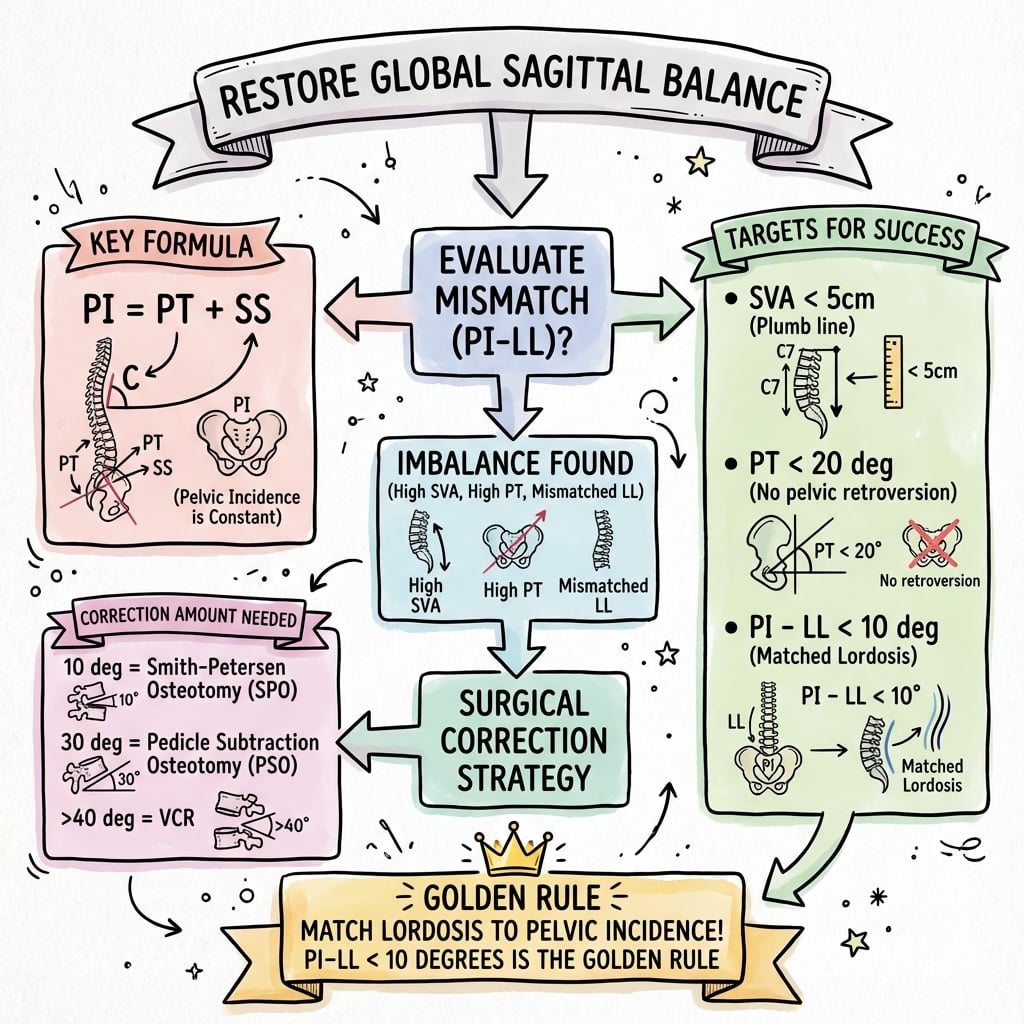
The fundamental goal of deformity surgery is to restore sagittal balance by matching lumbar lordosis to pelvic incidence (LL = PI ± 9°) and achieving normal SVA (under 50mm).
Surgical Planning Algorithm
- Measure spinopelvic parameters on standing lateral radiograph
- Calculate PI-LL mismatch (PI minus LL)
- Assess spine rigidity (flexion-extension films)
- Select osteotomy type based on mismatch magnitude and spine flexibility
- Determine fusion levels to achieve stable construct
- Set postoperative goals: PI-LL under 10°, SVA under 50mm, PT under 25°
Surgical Goals
- Preoperative (Typical)
- 20-40° (symptomatic)
- Postoperative Goal
- Under 10°
- Preoperative (Typical)
- 80-150mm (imbalanced)
- Postoperative Goal
- Under 50mm
- Preoperative (Typical)
- 30-50° (compensating)
- Postoperative Goal
- Under 25°
- Preoperative (Typical)
- 20-40° (loss of lordosis)
- Postoperative Goal
- PI ± 9°
These numerical goals are evidence-based and predict optimal outcomes.
Complications and Pitfalls
Surgical Complications Related to Spinopelvic Mismatch
- Relationship to Parameters
- Over-correction (negative PI-LL), high PI
- Prevention
- Match LL to PI, extend fusion if high PI
- Relationship to Parameters
- Excessive stress if PI-LL not corrected
- Prevention
- Adequate correction at index surgery
- Relationship to Parameters
- Residual PI-LL mismatch
- Prevention
- Aim for PI-LL under 10°
- Relationship to Parameters
- Under-correction, residual SVA
- Prevention
- Achieve SVA under 50mm, PI-LL under 10°
- Relationship to Parameters
- High PI, spinal imbalance
- Prevention
- Dual mobility, increased anteversion
Pitfalls in Deformity Correction
Under-Correction
- Not correcting enough lordosis (residual PI-LL over 10°)
- Patient remains symptomatic and disabled
- May progress to late deformity and junctional failure
Over-Correction
- Excessive lordosis (negative PI-LL mismatch)
- Proximal junctional kyphosis risk
- Patient feels "thrown backward"
- Difficult to correct without major revision
Wrong Osteotomy Type
- SPO in rigid spine (will not achieve correction)
- PSO in low PI patient (over-corrects)
- Insufficient number of levels for SPO
Clinical Applications
Deformity Surgery Planning
Surgical Goals Based on PI-LL Mismatch
- Disability
- Minimal (ODI under 20)
- Correction Needed
- None or minimal
- Technique
- Conservative Rx, possibly decompression only
- Disability
- Moderate (ODI 20-40)
- Correction Needed
- Moderate (10-20° LL gain)
- Technique
- Interbody fusions (LLIF/TLIF), multi-level
- Disability
- Severe (ODI 40-50)
- Correction Needed
- Large (20-30° LL gain)
- Technique
- PSO (pedicle subtraction osteotomy)
- Disability
- Extreme (ODI over 50)
- Correction Needed
- Very large (over 30°)
- Technique
- Multi-level PSO or VCR (vertebral column resection)
Adjacent Segment Disease
PI-LL Mismatch Accelerates Degeneration
- Annual ASD Risk
- 2-3% per year
- Mechanism
- Minimal mechanical stress
- Annual ASD Risk
- 4-6% per year
- Mechanism
- Moderate stress, compensatory hypermobility
- Annual ASD Risk
- 8-12% per year
- Mechanism
- Severe stress, rapid degeneration
Clinical Implication: Patients with residual PI-LL mismatch after fusion have accelerated adjacent segment degeneration. Adequate correction at index surgery reduces long-term revision risk.
Spinopelvic Parameters in Spondylolisthesis
The overview notes that a high pelvic incidence predisposes to spondylolisthesis; this is a developed examinable concept in its own right. A high PI increases lumbosacral shear (anterior shear force at L5-S1) and is an established risk factor for the development and progression of both isthmic and developmental (dysplastic) spondylolisthesis - PI is consistently higher in patients with spondylolisthesis than in controls, and tends to be highest in high-grade slips.
In high-grade slip the lumbosacral junction kyphoses (the slip angle / lumbosacral kyphosis), which drives global sagittal imbalance and forces the pelvis to retrovert (high PT, low SS - a "vertical/retroverted sacrum").
Spinal Deformity Study Group (SDSG) classification of high-grade spondylolisthesis is built on PI and on whether the spinopelvis is balanced or unbalanced:
- Balanced pelvis - high SS, low PT (nutated sacrum).
- Unbalanced (retroverted) pelvis - low SS, high PT, often with an unbalanced (kyphotic) spine where the C7 plumb line falls forward.
Why it matters clinically: the balanced-versus-unbalanced distinction informs the reduction-versus-in-situ-fusion debate. An unbalanced, retroverted pelvis with global imbalance benefits from reduction of the slip angle and restoration of lumbosacral lordosis to rebalance the spine (accepting the risk of L5 nerve-root stretch), whereas a balanced high-grade slip may be managed by in-situ fusion. Always measure PI and pelvic balance (PT/SS) in spondylolisthesis - they predict progression and guide whether to reduce.
Guidelines, Registries & Global Practice
Global Epidemiology
Adult spinal deformity is common and increasingly prevalent with population ageing. In community-dwelling adults older than 60, the prevalence of adult scoliosis has been reported as high as 68% in a volunteer cohort, although clinically and radiographically significant sagittal malalignment is less frequent. Sagittal, rather than coronal, parameters are the dominant drivers of disability across populations.
- Reported value
- About 50-55° (wide range 35-85°)
- Source (PubMed)
- Roussouly 2005 (PMID 15682018)
- Reported value
- About 47% (352/752)
- Source (PubMed)
- Glassman 2005 (PMID 16166889)
- Reported value
- Roughly linear worsening of SRS/SF-12/ODI with rising C7 plumb-line offset
- Source (PubMed)
- Glassman 2005 (PMID 16166889)
- Reported value
- 0.8% overall; 99.2% 5-yr survival free of dislocation
- Source (PubMed)
- Vigdorchik 2021 (PMID 34192913)
Guideline and Society Positions (Side-by-Side)
There is no single randomised-trial-based guideline mandating specific spinopelvic targets; practice is driven by validated classifications and society consensus. Evidence levels below reflect the underlying literature, not formal GRADE recommendations.
- Position on spinopelvic alignment
- Restore PI-LL to less than 10°, PT less than 20-25°, SVA less than 50mm
- Evidence basis
- Validation/reliability study (PMID 22045006)
- Position on spinopelvic alignment
- Aim for a "proportioned" spine using PI-based proportional targets and lordosis distribution
- Evidence basis
- Development/validation cohort, AUC 0.92 (PMID 28976431)
- Position on spinopelvic alignment
- Screen THA candidates for PI-LL mismatch and standing-to-seated spinal stiffness; use dual mobility for stiff flatback
- Evidence basis
- Prospective series, Otto Aufranc Award (PMID 34192913)
- Position on spinopelvic alignment
- Match restored lordosis shape to the patient's native PI-defined type
- Evidence basis
- Prospective descriptive cohort (PMID 15682018)
Imaging and Planning - Global Standards
- Full-length standing radiograph from C7 (ideally external auditory meatus) to femoral heads is the universal standard for measurement.
- EOS biplanar imaging delivers low-dose, weight-bearing whole-body assessment and is widely used in high-volume European, North American and Australasian centres.
- Standing-and-seated lateral films are standard for hip-spine assessment before THA in patients with spinal pathology (PMID 34192913).
- Planning software (e.g. Surgimap and equivalents) computes PI-based ideal lordosis; the GAP score adds proportional and lordosis-distribution targets (PMID 28976431).
Practice Variation and Registry Evidence
- Targets are largely consistent internationally (PI-LL less than 10°, SVA less than 50mm), but osteotomy preference varies: three-column osteotomy (PSO) use is higher in some North American series, while anterior-column realignment and multilevel interbody techniques are increasingly favoured to reduce three-column-osteotomy morbidity.
- National arthroplasty registries (e.g. AOANJRR, NJR, AJRR) record dislocation and revision but do not yet capture spinopelvic parameters, so registry data underestimate the hip-spine contribution to instability - a recognised data gap.
- Dual-mobility uptake for stiff-spine THA has risen markedly following hip-spine classification evidence (PMID 34192913).
MCQ Practice Points
Q: What is pelvic incidence (PI) and why is it clinically important?
A: Pelvic incidence (PI) is the angle between a line perpendicular to the sacral endplate at its midpoint and a line connecting this point to the femoral head centers. It is the only fixed spinopelvic parameter (does not change with posture) and determines the amount of lumbar lordosis needed for sagittal balance. PI = PT + SS. Higher PI requires more lordosis. The ideal relationship is PI minus LL within 10 degrees (PI-LL mismatch). Average PI is approximately 50-55 degrees.
Q: What is the sagittal vertical axis (SVA) and what values indicate positive sagittal balance?
A: SVA is the horizontal distance from the C7 plumb line to the posterosuperior corner of S1. Normal SVA is less than 5cm (C7 plumb line falls over or behind the sacrum). Positive sagittal balance (SVA greater than 5cm) means C7 is anterior to the sacrum, requiring compensatory mechanisms (pelvic retroversion, knee flexion, hip extension). SVA greater than 9.5cm is associated with significant disability. Every 1cm increase in SVA correlates with worsening patient-reported outcomes (Glassman study).
Q: What is pelvic tilt (PT) and what does an elevated PT indicate?
A: Pelvic tilt (PT) is the angle between a vertical line and the line connecting the sacral endplate midpoint to the femoral head centers. Normal PT is 10-25 degrees. Elevated PT (greater than 25-30 degrees) indicates pelvic retroversion - a compensatory mechanism for positive sagittal balance where the pelvis rotates backward to bring the trunk over the pelvis. High PT is associated with poor clinical outcomes, increased energy expenditure for walking, and indicates the patient is "using up" their compensatory reserve.
Q: How do you calculate the ideal lumbar lordosis for a patient?
A: The Schwab formula: Ideal LL = PI plus or minus 10 degrees. For example, a patient with PI of 60 degrees needs LL of 50-70 degrees. Other formulas exist: LL = PI + 9 (Legaye) or LL = 0.5 × PI + 25 (Le Huec). The lordosis should be distributed with two-thirds between L4-S1. When planning corrective surgery, target SVA less than 5cm, PT less than 25 degrees, and PI-LL mismatch less than 10 degrees. Failure to restore appropriate lordosis leads to flatback syndrome.
Q: What are the compensatory mechanisms for sagittal imbalance?
A: Compensatory mechanisms occur in sequence: 1) Pelvic retroversion (increased PT) - pelvis rotates backward; 2) Hip extension - reduces hip flexion contracture reserve; 3) Knee flexion - moves center of mass posteriorly; 4) Cervical hyperlordosis - attempts to maintain horizontal gaze. When all mechanisms are exhausted, the patient develops positive sagittal imbalance with forward stooped posture. Assessment should include full-length standing spine radiographs with hips and knees in view to evaluate compensation.
At a Glance
- Key Information
- Fixed anatomical parameter, average 50° (range 35-85°)
- Key Information
- Positional, normal under 20°, increased in imbalance
- Key Information
- Positional, PI = PT + SS
- Key Information
- Positional, target = PI ± 9°
- Key Information
- Under 10° good, 10-20° moderate, over 20° severe disability
- Key Information
- C7 plumb to S1, under 50mm normal, over 95mm severe
- Key Information
- Type 1-4 based on PI (low to high)
- Key Information
- Deformity surgery planning, THA instability assessment
PI = PT + SSPelvic Parameters Relationship
Hook:Pelvic Incidence equals Pelvic Tilt plus Sacral Slope - the fundamental equation!
TEN TWENTYPI-LL Mismatch Severity
Hook:TEN degrees - you're okay. TWENTY degrees - you're severely disabled!
FIFTY NINETY FIVESagittal Vertical Axis (SVA)
Hook:FIFTY mm is normal. NINETY FIVE mm is severe imbalance!
Exam Day Cheat Sheet
Differential Diagnosis - Causes of Positive Sagittal Imbalance / Loss of Lumbar Lordosis
When a patient presents with forward stooped posture and a positive SVA, the underlying driver must be identified, as it changes management. Key discriminators are whether the deformity is fixed or flexible and where the lordosis loss originates.
- Key Feature
- Anterior disc-height loss across lower lumbar levels
- PI / Parameters
- PI normal; LL reduced; PI-LL mismatch
- Flexibility / Distinguisher
- Often partly flexible early; rigid late
- Key Feature
- Lordosis lost within a prior straight fusion
- PI / Parameters
- Fixed PI; rigid fused segment, large PI-LL
- Flexibility / Distinguisher
- Rigid - needs osteotomy, not SPO alone
- Key Feature
- Global ankylosis, chin-on-chest, raised inflammatory markers
- PI / Parameters
- Rigid spine, large SVA, fused SI joints
- Flexibility / Distinguisher
- Rigid; HLA-B27; needs PSO; anaesthetic airway risk
- Key Feature
- Focal kyphosis at fracture level, osteoporosis
- PI / Parameters
- Focal angular deformity; may be mobile
- Flexibility / Distinguisher
- Acute vs chronic; MRI marrow oedema if acute
- Key Feature
- Posture corrects when supine; truncal weakness
- PI / Parameters
- Dynamic, position-dependent, often flexible
- Flexibility / Distinguisher
- Reducible supine - distinguishes from fixed bony deformity
- Key Feature
- Trunk lean driven by the hip, not the spine
- PI / Parameters
- Reduced PT/anteversion; LL may be preserved
- Flexibility / Distinguisher
- Thomas test positive; correct hip before judging spine
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 65-year-old woman presents 20 years post-Harrington rod instrumentation for adolescent idiopathic scoliosis. She has progressive forward lean and can only walk 50 meters before back and leg pain forces her to sit. Standing lateral radiograph shows PI 55°, LL 25°, PT 35°, SVA 120mm. She asks if surgery can help.”
“A 68-year-old man undergoes primary THA for osteoarthritis. He has a history of L4-S1 fusion for degenerative spondylolisthesis performed 5 years ago. At 3 months post-THA, he has had 2 posterior dislocations despite standard positioning (40° inclination, 20° anteversion). Standing spine films show PI 70°, LL 45°, PT 35°, rigid lumbar spine. The referring surgeon asks your opinion on revision strategy.”
“A 62-year-old woman with degenerative scoliosis (Cobb 45°) has severe disability (ODI 55). She has neurogenic claudication limiting walking to 100 meters. Standing films show PI 50°, LL 20°, PT 40°, SVA 140mm. L2-S1 is rigid on flexion-extension films. She asks if surgery can help and if so, what type.”
“A 58-year-old man presents with increasing low back pain and difficulty standing upright. He leans forward when walking and uses a shopping cart for support. Standing lateral radiograph shows PI 45°, LL 35°, PT 25°, SVA 60mm. He works as a pharmacist and finds it difficult to stand for long periods. ODI score is 32. He asks if he needs surgery.”
Pelvic Parameters (Fixed vs Positional)
- Pelvic Incidence (PI): FIXED morphological parameter, average 50° (35-85°), does NOT change
- Pelvic Tilt (PT): Positional, normal under 20°, increases with retroversion (compensation)
- Sacral Slope (SS): Positional, average 40°, PI = PT + SS (always true)
- PI determines ideal lumbar lordosis: Target LL = PI ± 9°
Spinal Parameters
- Lumbar Lordosis (LL): L1-S1, normal 40-70°, should match PI ± 9°
- PI-LL Mismatch: Under 10° good, 10-20° moderate, over 20° severe disability (ODI over 40)
- Sagittal Vertical Axis (SVA): C7 plumb to S1, under 50mm normal, over 95mm severe imbalance
- Thoracic Kyphosis (TK): T4-T12, normal 20-50°, reciprocal to LL
PI-LL Mismatch - Disability Correlation
- Under 10°: ODI under 20, minimal disability, good balance, no surgery needed
- 10-20°: ODI 20-40, moderate disability, consider surgery if symptomatic
- 20-30°: ODI 40-50, severe disability, strong surgical indication
- Over 30°: ODI over 50, extreme disability, major correction needed (PSO/VCR)
Roussouly Classification (PI-Based Types)
- Type 1: PI under 45°, flat back, short lordosis apex L5, prone to flatback
- Type 2: PI 45-50°, harmonious alignment, apex L4, ideal balanced spine
- Type 3: PI 50-60°, well-developed lordosis, apex L3-4, common pattern
- Type 4: PI over 60°, hyperlordosis, apex L2-3, high THA dislocation risk
Surgical Planning - Osteotomy Selection
- SPO (Smith-Petersen): 5-10° per level, for MOBILE discs, PI-LL 10-20°, multi-level
- PSO (Pedicle Subtraction): 25-35° per level, for RIGID spine, PI-LL 20-35°, single level
- VCR (Vertebral Column Resection): 40-60° per level, extreme deformity, PI-LL over 35°
- Surgical goals: PI-LL under 10°, SVA under 50mm, PT under 25°
THA Considerations
- High PI (over 60°): Increased dislocation risk via greater functional anteversion change
- Stiff spine (fused): Lost protective pelvic tilt when sitting, increased dislocation risk
- PI-LL mismatch: Pelvic retroversion reduces functional anteversion in sitting
- Revision strategy: Dual mobility for stiff spine, increased anteversion 25-30°
Compensatory Mechanisms (Cascade)
- Stage 1 (SVA 0-50mm): Pelvic retroversion (increased PT up to 30°)
- Stage 2 (SVA 50-80mm): Knee flexion, ankle dorsiflexion added
- Stage 3 (SVA 80-120mm): Thoracic hyperkyphosis develops
- Stage 4 (SVA over 120mm): Exhausted compensation, hip extension loss, cannot stand upright
Measurement Technique
- PI: Femoral heads to sacral endplate, perpendicular to sacral plate
- PT: Femoral heads to sacral endplate, vertical reference
- SS: Sacral endplate angle to horizontal
- LL: L1 superior to S1 superior endplate (Cobb angle)
- SVA: C7 plumb line horizontal distance to posterior-superior S1
Evidence Base
Schwab Realignment Objectives - Current Concepts Review
- Current concepts review establishing spinopelvic realignment objectives for adult spinal deformity surgery
- Identified sagittal vertical axis, pelvic tilt and lumbar lordosis as the key parameters correlating with pain and disability
- Proposed restoring a low SVA and low PT combined with lumbar lordosis proportional to pelvic incidence
- Advocated a global, individualised alignment approach rather than universal numerical targets
- Provided the conceptual framework later operationalised in the SRS-Schwab classification
SRS-Schwab Adult Deformity Classification - Validation
- Reliability/validation study of the SRS-Schwab classification incorporating pelvic parameters
- Adds three sagittal modifiers - PI-LL mismatch, pelvic tilt and SVA - each graded 0, plus or double-plus
- Modifier cut-offs were derived from health-related quality of life data in a multicentre deformity database
- Inter-rater kappa was 0.75 to 0.86 for PI-LL, 0.97 to 0.98 for PT and 0.96 for SVA (substantial to almost perfect)
- Nine readers grading 21 cases twice demonstrated excellent intra-rater reliability (kappa about 0.88 to 0.97)
Roussouly Classification - Normal Sagittal Alignment
- Prospective radiographic study of 160 asymptomatic volunteers in standardised standing position
- Described four reproducible types of normal sagittal lumbopelvic morphology
- Sacral slope (and thus PI) determined lordosis magnitude, apex position and number of lordotic vertebrae
- Type 1-2 (low PI/SS) show short or flat lordosis; Type 3-4 (high PI/SS) show longer, more curved lordosis
- Provided a normative framework so restoration targets the patient's own type rather than a universal value
Acetabular Anteversion Change After Spinal Realignment
- Retrospective multicentre series of 41 hips (33 patients) with prior THA who later underwent spinal realignment
- Acetabular anteversion fell significantly after spinal correction (mean change about minus 5°, p less than 0.001)
- Change in anteversion correlated most strongly with change in pelvic tilt (r about 0.83)
- Anteversion decreased roughly 1° for every 1.1° reduction in pelvic tilt - close to a one-to-one relationship
- Patients with spinopelvic malalignment frequently had excessively anteverted cups that normalised after realignment
Pelvic Tilt and Truncal Inclination Predict Disability
- Prospective analysis of 125 adult deformity patients (mean age 57) with full-length standing radiographs
- Pelvic tilt correlated with health-related quality of life (r about 0.28 to 0.42) and with SVA (r about 0.64)
- High PT reflects compensatory pelvic retroversion for sagittal malalignment
- T1 spinopelvic inclination (truncal inclination) correlated with HRQOL and outperformed raw SVA
- Sagittal, not coronal, parameters drove disability - establishing PT as a key compensatory marker
Positive Sagittal Balance Predicts Disability (SVA)
- Multicentre review of 752 adult deformity patients; 352 had positive sagittal balance
- All health-status measures (SRS, SF-12, ODI) worsened as C7 plumb-line deviation increased
- Symptom severity rose in a roughly linear fashion with progressive sagittal imbalance
- Even mildly positive sagittal balance was detrimental to patient-reported outcomes
- Lumbar (relative) kyphosis was poorly tolerated, whereas upper thoracic kyphosis was better tolerated
Global Alignment and Proportion (GAP) Score
- Developed and validated in 222 patients fused 4 or more levels and followed at least 2 years
- PI-based proportional score using relative pelvic version, relative lumbar lordosis, lordosis distribution index and relative spinopelvic alignment plus age
- Area under the ROC curve of 0.92 for predicting mechanical complications
- Proportioned spines had a 6% mechanical complication rate versus 47% (moderate) and 95% (severe disproportion)
- Improves on absolute Schwab targets by accounting for the whole PI spectrum and lordosis distribution
Hip-Spine Classification Reduces THA Dislocation
- Prospective multicentre series of 2,081 THAs (2021 Otto Aufranc Award)
- Flatback deformity defined as PI-LL greater than 10°; stiff spine as less than 10° change in sacral slope standing to seated
- Group 2B (flatback plus stiff spine) and patients with more than three fused levels all received dual-mobility components
- Five-year survivorship free of dislocation was 99.2% (overall dislocation rate 0.8%)
- Patient-specific component positioning guided by spinopelvic mobility markedly reduced instability in high-risk hips
References
- Duval-Beaupère G, Schmidt C, Cosson P. A Barycentremetric study of the sagittal shape of spine and pelvis: the conditions required for an economic standing position. Ann Biomed Eng. 1992;20(4):451-462.
- Legaye J, Duval-Beaupère G, Hecquet J, Marty C. Pelvic incidence: a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J. 1998;7(2):99-103.
- Schwab F, Patel A, Ungar B, et al. Adult spinal deformity-postoperative standing imbalance: how much can you tolerate? An overview of key parameters in assessing alignment and planning corrective surgery. Spine. 2010;35(25):2224-2231.
- Schwab F, Ungar B, Blondel B, et al. Scoliosis Research Society-Schwab adult spinal deformity classification: a validation study. Spine. 2012;37(12):1077-1082.
- Roussouly P, Gollogly S, Berthonnaud E, Dimnet J. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine. 2005;30(3):346-353.
- Lafage V, Schwab F, Patel A, Hawkinson N, Farcy JP. Pelvic tilt and truncal inclination: two key radiographic parameters in the setting of adults with spinal deformity. Spine. 2009;34(17):E599-E606.
- Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine. 2005;30(18):2024-2029.
- Buckland AJ, Vigdorchik JM, Schwab FJ, et al. Acetabular anteversion changes due to spinal deformity correction: bridging the gap between hip and spine surgeons. J Bone Joint Surg Am. 2015;97(23):1913-1920.
- Vigdorchik JM, Sharma AK, Buckland AJ, et al. 2021 Otto Aufranc Award: A simple Hip-Spine Classification for total hip arthroplasty: validation and a large multicentre series. Bone Joint J. 2021;103-B(7 Supple B):17-24.
- Smith JS, Klineberg E, Schwab F, et al. Change in classification grade by the SRS-Schwab Adult Spinal Deformity Classification predicts impact on health related quality of life measures: prospective analysis of operative and nonoperative treatment. Spine. 2013;38(19):1663-1671.
- Yilgor C, Sogunmez N, Boissiere L, et al. Global Alignment and Proportion (GAP) Score: development and validation of a new method of analyzing spinopelvic alignment to predict mechanical complications after adult spinal deformity surgery. J Bone Joint Surg Am. 2017;99(19):1661-1672.
- Bridwell KH, Glassman S, Horton W, et al. Does treatment (nonoperative and operative) improve the two-year quality of life in patients with adult symptomatic lumbar scoliosis: a prospective multicenter evidence-based medicine study. Spine. 2009;34(20):2171-2178.
- Protopsaltis T, Schwab F, Bronsard N, et al. The T1 pelvic angle, a novel radiographic measure of global sagittal deformity, accounts for both spinal inclination and pelvic tilt and correlates with health-related quality of life. J Bone Joint Surg Am. 2014;96(19):1631-1640.
- Barrey C, Roussouly P, Le Huec JC, D'Acunzi G, Perrin G. Compensatory mechanisms contributing to keep the sagittal balance of the spine. Eur Spine J. 2013;22 Suppl 6:S834-S841.
- Senteler M, Weisse B, Rothenfluh DA, Snedeker JG. Pelvic incidence-lumbar lordosis mismatch results in increased segmental joint loads in the unfused and fused lumbar spine. Eur Spine J. 2014;23(7):1384-1393.