Adult Flatfoot Deformity | Medial Arch Collapse | Static Restraint Failure
- Spring ligament is the PRIMARY STATIC restraint to talar head plantar displacement
- Nearly always occurs with Stage II or higher PTTD (90% association)
- Superomedial band is most commonly injured (largest, under talar head)
- Direct repair fails - requires augmentation (FHL/FDL/allograft)
- MRI shows thickening, fluid signal, discontinuity on coronal views
- “Ask about progression - acute trauma rare, usually degenerative with PTTD
- “Palpable gap at spring ligament site indicates complete rupture
- “Always assess in context of adult flatfoot - never isolated pathology
- “Reconstruction is adjunct to PTT reconstruction, never alone
Spring Ligament Insufficiency
Talar Head Sling. 3 bands (superomedial largest) form a hammock suspending the talar head. Resists 50% of load on medial arch.
Always PTTD. Spring ligament failure occurs in Stage II-IV adult flatfoot. Isolated spring injury is extremely rare (trauma only).
Palpable Gap. With complete rupture, a gap can be palpated medial to talar head, especially with hindfoot eversion stress.
Augmentation Required. Primary repair fails. Use FHL/FDL autograft or allograft to reconstruct the superomedial band.
- Spring Ligament
- Static (ligamentous)
- PTT
- Dynamic (tendon)
- Combined Pathology
- Both systems fail
- Spring Ligament
- Rare (trauma only)
- PTT
- Common (degenerative)
- Combined Pathology
- Spring is secondary
- Spring Ligament
- Talar head plantar sag
- PTT
- Hindfoot valgus
- Combined Pathology
- Progressive flatfoot
- Spring Ligament
- Reconstruction + PTTD surgery
- PTT
- Stage-based algorithm
- Combined Pathology
- Combined procedures
Overview and Epidemiology
The plantar calcaneonavicular ligament (spring ligament) is a critical static restraint to medial longitudinal arch collapse. While isolated injury is rare, spring ligament insufficiency is present in 90% of patients with Stage II or higher posterior tibial tendon dysfunction (PTTD). The ligament acts as a hammock supporting the talar head, resisting approximately 50% of the load transmitted through the medial arch during weight bearing.
The name derives from the ligament's elastic properties, which were historically thought to provide a spring-like recoil to the arch. However, modern biomechanical studies show it functions primarily as a static restraint, not a dynamic spring.
Anatomy of the Spring Ligament Complex
- Origin: Sustentaculum tali (anterior aspect)
- Insertion: Medial navicular tuberosity
- Function: Primary restraint to talar head plantar displacement
- Characteristics: Thickest, fibrocartilaginous undersurface (articulates with talar head)
- Most commonly torn
- Inferior: Blends with plantar fascia, supports plantar aspect
- Oblique: Most lateral, overlaps with PTT insertion site
- Function: Secondary restraints, maintain arch integrity
- Clinical: Less commonly symptomatic in isolation
The inferior surface of the superomedial band undergoes fibrocartilaginous metaplasia where it articulates with the plantar aspect of the talar head. This allows the ligament to withstand compressive loads but also makes it vulnerable to degenerative failure under chronic stress.
SPRINGMedial Arch Static Restraints
Hook:The arch has a SPRING system - multiple static supports working together.
SIOSpring Ligament Anatomy (3 Bands)
Hook:SIO = Superomedial Is Overhead, supporting the talar head from below.
The Acetabulum Pedis (Talar Head Socket)
The topic repeatedly describes the spring ligament as a "hammock" and "static keystone" suspending the talar head. That imagery is best understood through the concept of the acetabulum pedis (also called the coxa pedis) — the ball-and-socket cradle that receives the talar head, functionally analogous to the acetabulum of the hip. Understanding this socket explains why spring ligament failure produces the specific deformity seen radiographically, rather than a vague "arch collapse."
- Anterior and middle facets of the calcaneus (on the sustentaculum tali) form the inferolateral floor
- Posterior (concave) articular surface of the navicular forms the anterior wall
- Spring (plantar calcaneonavicular) ligament bridges the gap between sustentaculum and navicular, completing the plantar-medial floor
- Together these cradle the talar head as a single peritalar unit
Because the superomedial band spans the interval where there is no bone beneath the talar head, its fibrocartilaginous undersurface is a genuine articular part of the socket. It must resist both tension (arch load) and compression (direct talar head contact) — which is why it develops fibrocartilage and why degeneration causes it to give way.
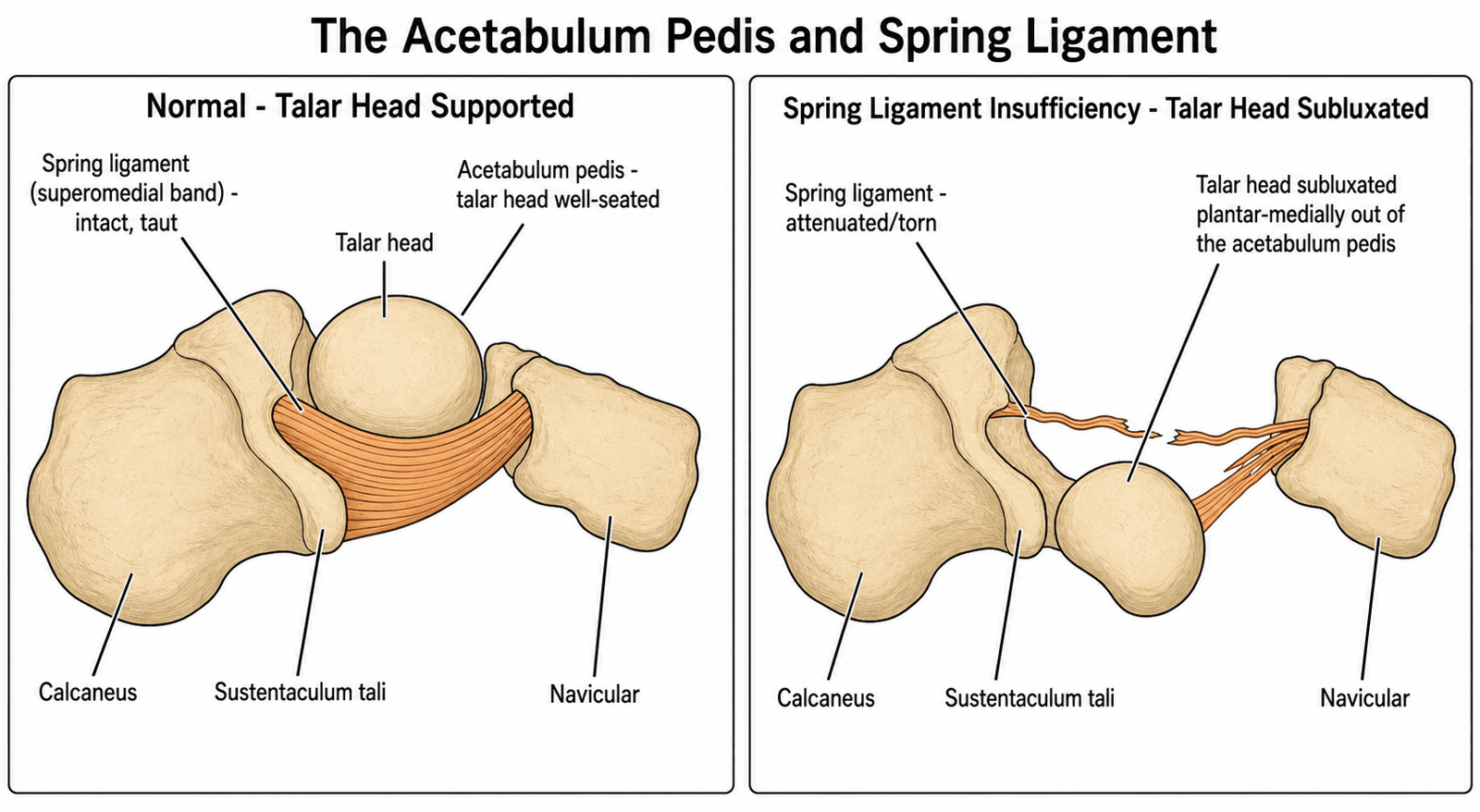
When the spring ligament attenuates, the medial-plantar floor of the acetabulum pedis fails and the talar head rotates plantar-medially out of its socket — true peritalar (peritalar/subtalar) subluxation. The navicular and midfoot swing into abduction and dorsiflexion around the sagging head, generating the talonavicular uncoverage and the break in Meary's line measured on weight-bearing films. Reframing flatfoot as subluxation of the talus out of the acetabulum pedis (rather than passive arch sag) clarifies why surgical reconstruction targets restoration of the socket floor and talonavicular coverage, not merely arch height.
Think of the talar head like a femoral head sitting in an acetabulum whose medial-plantar wall is soft tissue (the spring ligament) rather than bone. Lose that wall and the "hip of the foot" subluxates medially — the mechanical basis of peritalar subluxation and progressive collapsing foot deformity.
Pathophysiology
Spring ligament insufficiency develops through a progressive degenerative process, nearly always in the context of posterior tibial tendon dysfunction:
Pathologic Cascade
PTT loses strength and begins to elongate. Increased load is transferred to spring ligament.
Chronic overload causes spring ligament elongation. Superomedial band begins to stretch, allowing talar head plantar sag.
Superomedial band develops longitudinal tears or interstitial degeneration. Flexible flatfoot deformity becomes apparent.
Full-thickness disruption of superomedial band. Talar head fully plantarflexes, creating rigid flatfoot if untreated.
Isolated acute spring ligament rupture is exceedingly rare but can occur with severe hindfoot eversion trauma (e.g., motor vehicle accident). Unlike degenerative failure, acute injury may present without pre-existing PTTD. MRI shows acute hemorrhage and complete discontinuity.
Classification Systems
Progressive Failure Classification
- Pathology
- Elongation, no tear
- MRI Findings
- Thickening under 8mm, normal signal
- Deformity
- Flexible, reducible
- Treatment
- Conservative + UCBL orthosis
- Pathology
- Partial tear
- MRI Findings
- Thickening greater than 8mm, increased T2 signal, partial discontinuity
- Deformity
- Flexible with talar sag
- Treatment
- Augmentation + PTT transfer
- Pathology
- Complete rupture
- MRI Findings
- Complete discontinuity, fluid gap
- Deformity
- Rigid, fixed flatfoot
- Treatment
- Reconstruction + Osteotomy
This classification parallels the Johnson and Strom PTTD staging, as spring ligament insufficiency nearly always occurs with PTTD.
Clinical Presentation
History
Typical Patient Profile
- Demographics: Middle-aged female (40-60 years), 9:1 F greater than M ratio
- Onset: Gradual progression over months to years
- Pain: Medial midfoot pain, worse with prolonged standing/walking
- Deformity: Progressive flatfoot, "arch is falling"
- Function: Difficulty with single-leg heel rise, uneven terrain
Red Flags for Acute Injury
- Sudden onset after trauma (rare)
- Immediate inability to weight bear
- Massive medial swelling
- Palpable medial defect
These red flags suggest acute traumatic rupture rather than degenerative insufficiency.
Examination
Inspection
- Standing: Medial arch collapse, talar head prominence medially
- "Too Many Toes": Hindfoot valgus (more than 3 toes visible from behind)
- Gait: Excessive pronation, loss of heel rise
Palpation
- Spring ligament zone: Palpate medial to talar head (between sustentaculum and navicular)
- Gap sign: Palpable defect with complete rupture (rare)
- Talar head: Prominent medially, may be tender
Special Tests
- Single heel rise: Inability indicates PTT weakness (associated finding)
- Passive arch correction: Assess flexibility vs rigidity
- Hindfoot alignment: Jack test (toe extension recreates arch if flexible)
Tests assess combined PTTD and spring ligament pathology, not spring ligament in isolation.
Investigations
Imaging Protocol
AP, Lateral, Hindfoot Alignment Views. Assess arch collapse (Meary angle, calcaneal pitch), talonavicular uncoverage, hindfoot valgus. Not specific for spring ligament but essential for surgical planning.
Coronal T2-weighted sequences are critical. Shows thickening, increased signal, partial or complete discontinuity of superomedial band. Sagittal views show talar head plantar sag. Also assesses PTT pathology.
Can visualize spring ligament tears dynamically but operator-dependent. Less commonly used than MRI.
FLUIDMRI Findings in Spring Ligament Tear
Hook:FLUID on MRI = spring ligament pathology.
Differential Diagnosis
Spring ligament insufficiency presents as medial-sided foot pain with arch collapse. The key task is distinguishing it from other causes of acquired flatfoot and medial foot pain, and recognising that it usually coexists with posterior tibial tendon dysfunction rather than occurring in isolation.
- Distinguishing Features
- Talar head plantar-medial prominence, tenderness between sustentaculum and navicular
- Key Investigation
- Coronal MRI: superomedial band thickening then distal thinning
- Pitfall
- Assuming it is always secondary to PTTD
- Distinguishing Features
- Weak/absent single heel rise, too-many-toes sign, retromalleolar tenderness
- Key Investigation
- MRI of PTT (tenosynovitis, split, gap)
- Pitfall
- Treating PTTD alone and missing the spring tear
- Distinguishing Features
- Flexible flatfoot with a normal PTT and intact heel rise
- Key Investigation
- MRI tear plus normal PTT; confirmed intra-operatively
- Pitfall
- Mislabelling as PTTD and under-treating
- Distinguishing Features
- Valgus tilt of the talus within the ankle mortise
- Key Investigation
- Weight-bearing ankle AP shows valgus talar tilt
- Pitfall
- Missing the ankle component above the hindfoot
- Distinguishing Features
- Apex of deformity at the midfoot, not talonavicular
- Key Investigation
- Lateral weight-bearing radiograph: sag at NC or TMT
- Pitfall
- Osteotomy fails if true apex is more distal
- Distinguishing Features
- Diabetes/neuropathy, warmth, swelling, bony fragmentation
- Key Investigation
- Radiographs and MRI; check sensation and glucose
- Pitfall
- Operating during the active fragmentation phase
- Distinguishing Features
- Younger patient, rigid hindfoot, peroneal spasm
- Key Investigation
- CT: talocalcaneal or calcaneonavicular bar
- Pitfall
- Attempting soft-tissue reconstruction of a rigid foot
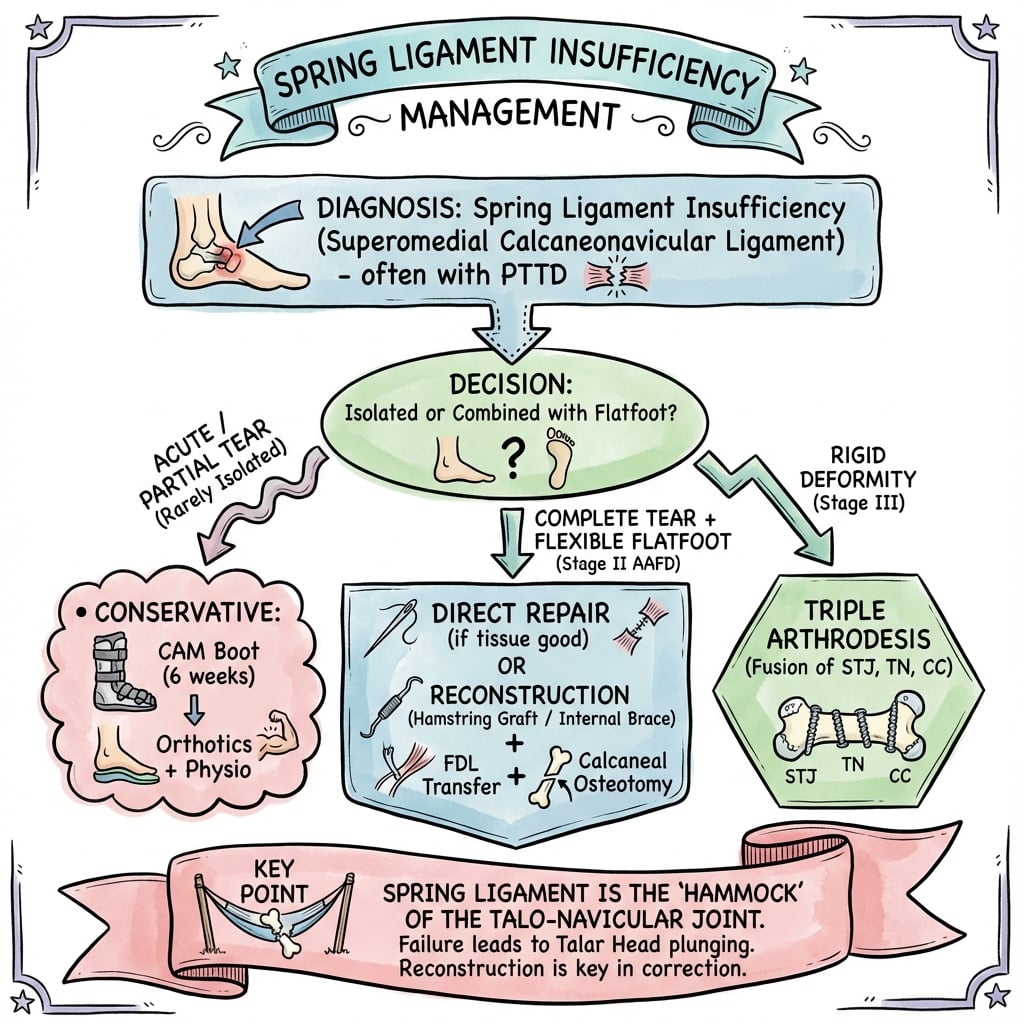
Management Algorithm
Indications
- Stage I (elongation, no tear)
- Minimal symptoms
- Reducible deformity
- Patient unfit for surgery
Protocol
Non-Operative Treatment
- Boot/Brace: CAM walker or Arizona brace to offload medial arch
- NSAIDs: Anti-inflammatory medication
- Activity modification: Avoid prolonged standing
- Custom UCBL orthosis: University of California Biomechanics Laboratory insole
- Medial posting: Supports talar head, reduces spring ligament load
- Arch support: Rigid arch maintains alignment
- PTT strengthening: Resisted inversion, toe curls
- Intrinsic foot muscles: Toe spreading, short foot exercises
- Proprioception: Single-leg balance, unstable surface training
Conservative management addresses PTT weakness but cannot reverse spring ligament elongation or tear. Success rate is 60-70% for symptom relief but does not prevent progression.
Surgical Technique
Patient Positioning
- Position: Supine with bump under ipsilateral hip
- Tourniquet: Thigh tourniquet (250-300 mmHg)
- Draping: Leg free draped to allow foot manipulation
Medial Incision
- Location: Centered over interval between PTT and FHL
- Length: 8-12 cm from navicular tuberosity to sustentaculum
- Deepening: Identify PTT sheath first (dorsal structure), then spring ligament (plantar)
Exposure
- Incise PTT sheath longitudinally
- Inspect PTT (usually requires debridement or transfer)
- Identify spring ligament inferior to talar head
- Assess tear pattern (longitudinal split vs complete rupture)
Exposure requires careful dissection to avoid injury to the plantar medial neurovascular bundle, which runs deep to the spring ligament.
Suture-Tape (Internal Brace) Augmentation
The Controversies section names synthetic suture-tape (internal brace) augmentation as an option but does not develop it. Because this is an increasingly discussed spring-ligament-specific adjunct, it warrants explanation.
What it is. A high-strength non-absorbable suture tape (for example a braided FiberTape-type construct) is anchored bone-to-bone from the sustentaculum tali / medial calcaneus to the navicular tuberosity, running along the anatomic course of the superomedial band, and tensioned with the foot held in the corrected position (talar head reduced, hindfoot neutral).
- Acts as an internal ligament that offloads the healing native repair or tendon graft during the vulnerable early phase
- Augments rather than replaces — used alongside primary repair, tendon autograft, or deltoid-spring (TCNL) reconstruction
- No tendon-harvest donor morbidity; immediate mechanical restraint may permit earlier protected rehabilitation
- A non-elastic tape over-constrains a normally viscoelastic ligament and may stress-shield native tissue or cut through bone/soft tissue if over-tensioned
- Isometric anchor placement and correct tension are critical — a poorly placed tape either does nothing or blocks reduction
- Comparative outcome data are limited (small, level IV series), so it remains an adjunct, not a proven standalone
Crucially, tape augmentation follows the same rule as every soft-tissue step in this operation: it does not substitute for a medializing (or lateral column lengthening) osteotomy when fixed hindfoot valgus or forefoot abduction is present. Bony realignment restores alignment; the internal brace protects the medial soft-tissue reconstruction that maintains it.
If asked about internal-brace augmentation, frame it as a load-sharing protector of the biologic reconstruction, tensioned in the corrected position, with the caveat that a rigid synthetic tape can stress-shield or over-constrain and has only low-level evidence. It never removes the need to correct bony deformity first.
Complications
- Incidence
- 10-15%
- Risk Factors
- Inadequate correction, non-compliance
- Management
- Revision reconstruction, osteotomy
- Incidence
- 5-8%
- Risk Factors
- Diabetes, smoking, peripheral vascular disease
- Management
- Local wound care, VAC therapy
- Incidence
- 2-3%
- Risk Factors
- Deep dissection, excessive retraction
- Management
- Observation (usually neuropraxia), neurolysis if persistent
- Incidence
- 5-10%
- Risk Factors
- Inadequate fixation, early mobilization
- Management
- Revision with allograft augmentation
- Incidence
- 10-20%
- Risk Factors
- Over-correction, aggressive immobilization
- Management
- Physiotherapy, subtalar mobilization
The medial plantar nerve runs deep to the spring ligament and can be injured during deep dissection or bone tunnel creation. Injury causes numbness to the medial forefoot and weakness of intrinsic muscles. Use careful retraction and stay superficial to the neurovascular bundle.
Postoperative Care and Rehabilitation
Rehabilitation Protocol
Splint immobilization. Below-knee backslab or boot. Leg elevation, DVT prophylaxis, wound care.
Transition to removable boot. Continue non-weight bearing. Begin ankle ROM exercises (plantarflexion/dorsiflexion only, no inversion/eversion).
Progressive weight bearing in boot. 25% at week 6, 50% at week 8, 75% at week 10, full at week 12. Boot worn full-time.
Wean from boot to supportive shoe with custom orthosis. UCBL or full-length rigid orthotic mandatory. Continue gait retraining, strengthening.
Gradual return to sports/high-demand activities. Permanent orthotic use recommended. Avoid barefoot walking, unsupportive shoes.
Outcomes and Prognosis
Risk factors for failure:
- Rigid deformity (fixed flatfoot despite reconstruction)
- Severe hindfoot valgus not corrected (greater than 20 degrees)
- Obesity (BMI greater than 35)
- Peripheral neuropathy (diabetes)
- Non-compliance with orthotic use postoperatively
Guidelines, Registries & Global Practice
Spring ligament insufficiency is managed within the broader framework of adult acquired flatfoot deformity (AAFD), now increasingly termed progressive collapsing foot deformity (PCFD). There is no isolated society guideline for the spring ligament itself; practice is guided by foot-and-ankle society consensus on flatfoot and by the underlying evidence.
Global epidemiology
- AAFD predominantly affects middle-aged women (typical onset 40 to 65 years), with a strong female preponderance.
- Spring ligament pathology is identified in the large majority of advanced (flexible stage II and beyond) flatfeet at surgery; isolated rupture with a normal PTT is rare but real and under-recognised.
- Obesity, hypertension, diabetes and seronegative inflammatory arthropathy are recognised associations with degenerative medial-arch failure.
- Position Relevant to Spring Ligament
- Classify by flexibility and deformity class; soft-tissue reconstruction is an adjunct to osseous realignment
- Emphasis
- Class-based, deformity-specific algorithm
- Position Relevant to Spring Ligament
- Trial structured non-operative care first; reserve reconstruction for failed conservative management
- Emphasis
- Stepwise, evidence-graded care
- Position Relevant to Spring Ligament
- Stage-based flatfoot pathway; combined tendon transfer, osteotomy and ligament repair for flexible deformity
- Emphasis
- Combined-procedure reconstruction
- Position Relevant to Spring Ligament
- Anatomic reduction of talonavicular sag with osteotomy plus medial soft-tissue restoration
- Emphasis
- Restore the medial column mechanically
- Position Relevant to Spring Ligament
- Endorse flexible-deformity reconstruction; recognise heterogeneity and low-level evidence
- Emphasis
- Joint preservation where feasible
Registry note. No arthroplasty-style registry tracks spring ligament reconstruction; it is a soft-tissue procedure with no implant. Evidence is therefore confined to small retrospective and prospective series rather than registry survivorship data, which is why recommendations remain level IV.
- MRI-guided staging and 3T imaging of the superomedial band
- Combined reconstruction: FDL transfer + medializing calcaneal osteotomy + spring/TCNL reconstruction, with allograft or suture-tape augmentation available
- Custom orthoses and supervised rehabilitation
- Clinical staging and weight-bearing radiographs where MRI is unavailable
- Reliance on autograft (FDL/FHL/peroneus longus) and standard osteotomy without costly implants or allograft
- Prefabricated arch supports; arthrodesis reserved for rigid or salvage deformity
Set expectations: spring ligament reconstruction is part of a combined flatfoot operation, recovery is prolonged (around 12 months to full activity), long-term orthotic support is usually advised, and recurrence occurs in roughly 10 to 15 percent. Document the flexibility assessment and the failed conservative trial before surgery.
Controversies and Areas of Uncertainty
The long-held view that spring ligament failure is always secondary to PTTD has been challenged: small series document isolated rupture with a normal PTT (Orr and Nunley). The true incidence of isolated injury is unknown and likely under-recognised.
Cadaveric work suggests a strictly anatomic superomedial-band reconstruction may correct less deformity than grafts with more proximal/oblique fixation lines, implying other medial structures share the load. The optimal graft path remains debated.
FHL versus FDL autograft, peroneus longus, allograft and synthetic suture-tape (internal brace) augmentation all have advocates. High-quality comparative outcome data are lacking, so choice is largely surgeon preference and tissue availability.
Regression data show the medializing calcaneal osteotomy, not the ligament reconstruction, drives hindfoot correction. How much soft-tissue reconstruction adds once bony alignment is restored, and whether it improves durability, is unresolved.
Acknowledge the uncertainty honestly: spring ligament reconstruction is an adjunct within a staged flatfoot algorithm, the evidence base is level IV with small numbers, and correction of bony alignment (osteotomy, lateral column lengthening) is the foundation. Avoid claiming any single graft or technique is proven superior.
MCQ Practice Points
Q: What percentage of medial arch load is resisted by the superomedial band of the spring ligament? A: 50% - The superomedial band is the primary static restraint to talar head plantar displacement, bearing approximately half of the medial longitudinal arch load during weight bearing.
Q: What is the most common associated pathology in spring ligament insufficiency? A: Posterior tibial tendon dysfunction (PTTD) - Spring ligament insufficiency occurs in 90% of patients with Stage II or higher PTTD. Isolated spring ligament injury without PTTD is exceedingly rare and typically only seen with acute trauma.
Q: Which MRI sequence and plane are most sensitive for diagnosing spring ligament tears? A: Coronal T2-weighted sequences - These show high signal intensity (fluid), thickening greater than 8mm, and discontinuity of the superomedial band. Sagittal views are adjunctive for assessing talar head plantar sag.
Q: Why does primary repair of the spring ligament fail, requiring augmentation? A: Degenerative tissue quality and chronic attenuation - The native spring ligament in insufficiency has undergone degenerative elongation and has poor healing potential. Primary suture repair cannot restore the ligament's original length and strength. Augmentation with autograft or allograft is required to recreate the superomedial band.
Q: What is the minimum conservative management trial before considering surgical reconstruction for spring ligament insufficiency? A: 6 months - Conservative management with UCBL orthosis, NSAIDs, activity modification, and PTT strengthening should be trialed for at least 6 months. Surgery is reserved for patients who fail conservative management with persistent symptoms and functional limitation.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old female presents with progressive medial foot pain and arch collapse over 2 years. MRI shows thickening and partial discontinuity of the spring ligament superomedial band. How would you manage this patient?”
“You are performing spring ligament reconstruction using FHL autograft. Walk me through your surgical technique, focusing on graft passage and fixation.”
“A patient returns 8 months after spring ligament reconstruction with FHL autograft, FDL transfer, and medializing calcaneal osteotomy. They report recurrent medial foot pain and progressive arch collapse. X-rays show loss of correction. How would you manage?”
Key Anatomy
- 3 bands: Superomedial (largest, most commonly torn), Inferior, Oblique
- Superomedial band = sustentaculum tali to navicular tuberosity
- Fibrocartilaginous undersurface articulates with talar head
- Primary static restraint to talar head plantar displacement (50% load)
- Medial plantar nerve runs deep to ligament (at risk during surgery)
Classification
- Stage I = Elongation, no tear, reducible = Conservative + Orthosis
- Stage II = Partial tear, flexible deformity = Augmentation + PTT transfer
- Stage III = Complete tear, rigid deformity = Reconstruction + Osteotomy
- Nearly always associated with PTTD (90%)
Diagnosis
- Clinical: Medial foot pain, arch collapse, palpable gap (if complete rupture)
- MRI: Coronal T2 shows thickening greater than 8mm, fluid signal, discontinuity
- Weight-bearing X-rays: Assess arch collapse (Meary angle, calcaneal pitch)
- Always assess PTT function: single heel rise test, too many toes sign
Management Algorithm
- Conservative first: UCBL orthosis, NSAIDs, PTT strengthening (6 months minimum)
- Surgery for failed conservative, flexible deformity, functional limitation
- Reconstruction: FHL autograft augmentation (sustentaculum to navicular tunnels)
- Always combined: PTT transfer (FDL) + Calcaneal osteotomy (if hindfoot valgus)
- Never isolated spring ligament surgery (will fail)
Surgical Pearls
- FHL harvest distal to master knot of Henry (8-10 cm graft)
- Bone tunnels: Sustentaculum (medial to lateral), Navicular (dorsal to plantar)
- Tension graft with foot in corrected position (arch recreated, hindfoot neutral)
- Protect medial plantar nerve during deep dissection
- Postop: Non-weight bearing 6 weeks, protected weight bearing 6 weeks, permanent orthotic
Complications
- Recurrent deformity: 10-15% (inadequate correction, non-compliance)
- Nerve injury (medial plantar): 2-3% (deep dissection)
- Wound healing: 5-8% (diabetes, smoking)
- Graft failure: 5-10% (inadequate fixation, early mobilization)
- Subtalar stiffness: 10-20% (over-correction)
Evidence Base and Key Studies
Anatomical Spring Ligament Reconstruction with Peroneus Longus (Biomechanical)
- Cadaveric model (10 foot-ankle specimens) of failed spring ligament with 5 to 15 degrees talonavicular abduction
- Compared three peroneus longus reconstruction passages under 357 N vertical ground-reaction load
- Superomedial/plantar passage through calcaneus and navicular corrected talonavicular abduction from 9.1 degrees abducted to 1.0 degree adducted
- Same passage restored subtalar joint from 3.1 degrees everted toward neutral
Peroneus Longus Autograft Spring Ligament Reconstruction (Clinical Outcomes)
- Retrospective series of 13 patients (14 feet), mean age 63.5 years, where lateral column lengthening failed to fully correct talonavicular deformity
- AOFAS ankle-hindfoot score improved from 43.1 to 90.3 at mean 8.9-year follow-up
- Significant radiographic correction of talonavicular coverage, calcaneal pitch and lateral talonavicular angles into normal ranges
- Mean residual hindfoot alignment 2.7 degrees valgus; few complications
MRI Features of Surgically Proven Spring Ligament Tears
- Retrospective review of 13 surgically proven spring ligament tears versus a 96-patient comparison group
- Superomedial band proximal thickening over 5mm seen in 92% and distal thinning under 2mm in 85% of proven tears
- Medioplantar band findings (thickening over 7mm, signal heterogeneity) were far less reliable
- Superomedial band abnormalities were consistent, reproducible and correlated with surgical pathology
Isolated Spring Ligament Failure as a Cause of Flatfoot
- Six consecutive patients (all female, mean age 42) with flexible flatfoot from spring ligament rupture and an intact tibialis posterior tendon
- MRI suggested a spring ligament tear in all 5 patients imaged preoperatively
- All had a normal PTT confirmed intraoperatively, refuting the assumption that spring ligament failure is always secondary
- At mean 13 months, 5 of 6 were pain-free without orthoses and all were free of residual deformity
Deltoid-Spring (TCNL) Ligament Reconstruction for Medial Peritalar Instability
- 14 feet (12 patients) with advanced flexible flatfoot (stage IIB with large spring tears, or stage IV) had osseous correction plus allograft tibiocalcaneonavicular reconstruction
- FAAM activities-of-daily-living improved from 69.3 to 90.1 at mean 24 months
- Meary angle improved from 29.7 to 12.5 degrees and talonavicular coverage from 47.4 to 23.1 degrees
- The superficial deltoid blends with the superomedial spring ligament to form the TCNL, the rationale for combined reconstruction
Medializing Calcaneal Osteotomy Drives Hindfoot Correction
- Prospective study of 30 stage II flatfoot reconstructions analysing 19 variables against hindfoot moment arm
- On multivariate regression, the amount of medializing calcaneal osteotomy was the only significant predictor of hindfoot correction
- Spring ligament reconstruction and lateral column lengthening contributed on univariate analysis but not independently
- Final regression model fit well (R-squared 0.93)