Tension vs Compression | MRI Gold Standard | Surgical Emergency if Tension Side
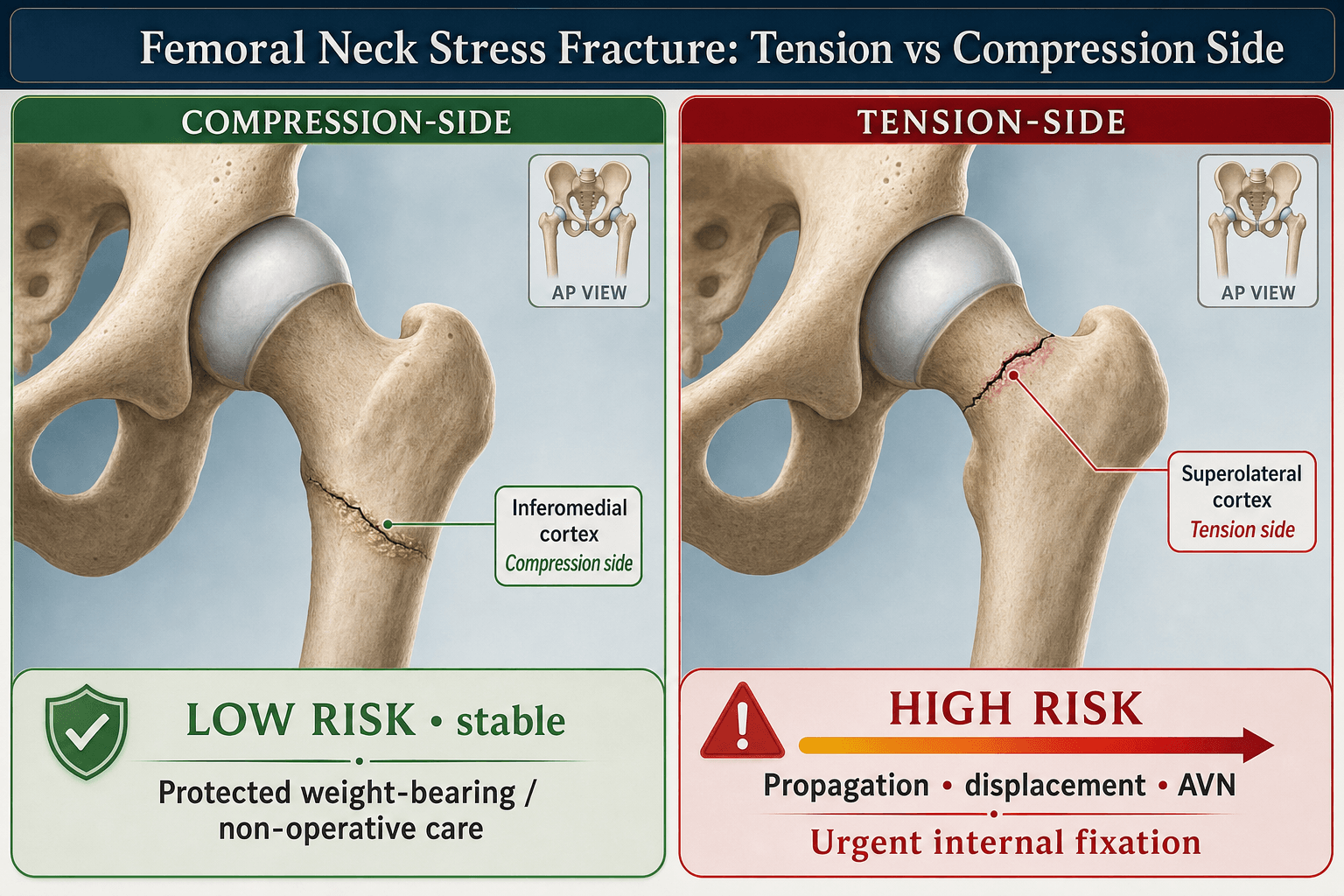
- Tension side (superior cortex) requires prophylactic surgical fixation - high displacement risk
- Compression side (inferior cortex) can be managed conservatively with non-weight bearing
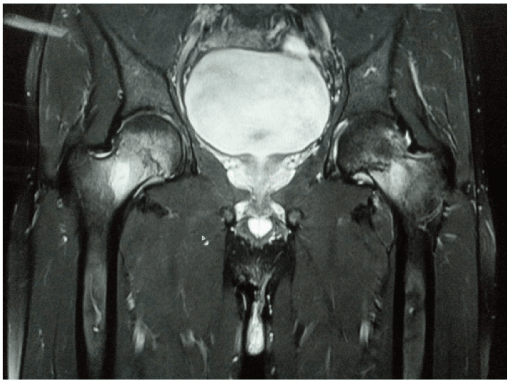
- MRI is gold standard - X-rays often negative initially
- Female athlete triad - amenorrhea, low energy availability, low BMD
- Military recruits and runners are highest risk populations
- “Groin pain in young athlete/military recruit = stress fracture until proven otherwise
- “X-rays often negative for 2-4 weeks - MRI for early diagnosis
- “Superior cortex involvement = surgical emergency (high displacement risk)
- “Return to sport requires MRI evidence of healing
This is THE exam question. Tension side (superior cortex) = surgical fixation required. Compression side (inferior cortex) = conservative management possible. Get this wrong and you fail.
X-rays are often negative for 2-4 weeks. MRI shows bone marrow edema early. Always order MRI if clinical suspicion high and X-rays negative.
Low energy availability, menstrual dysfunction, low BMD. Must screen female athletes with stress fractures. Endocrine referral if triad suspected.
Femoral neck is a high-risk stress fracture location due to displacement potential and AVN risk. More aggressive management than tibial stress fractures.
- Location
- Superior cortex involvement
- Treatment
- SURGICAL - prophylactic screw fixation
- Location
- Inferior cortex only
- Treatment
- Non-weight bearing 6-8 weeks, serial imaging
- Location
- Complete with displacement
- Treatment
- Urgent surgical fixation (cannulated screws or DHS)
- Location
- Progressive symptoms at 6 weeks
- Treatment
- Convert to surgical fixation
- Location
- Both hips affected
- Treatment
- Address underlying cause, extended rest
TRIADTRIAD - Female Athlete Risk
Hook:TRIAD in female athletes = Think stress fracture and bone health
Overview and Epidemiology
Femoral neck stress fractures are overuse injuries occurring from repetitive submaximal loading, most common in endurance athletes and military recruits. They represent a high-risk stress fracture location due to displacement potential and AVN risk.
Historical context:
- First described in military populations
- Recognition of tension vs compression distinction critical
- Female athlete triad identified as major risk factor
Femoral neck stress fractures are classified as high-risk stress fractures due to the risk of displacement leading to AVN and nonunion. They require more aggressive management than low-risk stress fractures (tibial shaft, metatarsal).
- Femoral neck stress fractures account for approximately 3% of all sport-related stress fractures (Robertson & Wood 2017)
- Distance/marathon runners are the commonest athletic population affected; military recruits in basic training are the other key high-risk group
- Female predominance, strongly linked to the female athlete triad / RED-S; in mixed surgical military cohorts roughly half of operatively treated cases are women (Shaw 2022)
- Ballet dancers and other high-volume, leanness-emphasis athletes are also over-represented
- Across military basic training, the baseline incidence of stress fracture of any site is several percent over an 8-week cycle (5.9% per 8 weeks in the female Navy recruit RCT; Lappe 2008) — the femoral neck is a small but high-consequence subset
- Training errors (too much, too soon)
- Female athlete triad (low energy availability, amenorrhea, low BMD)
- Low vitamin D
- Smoking
- Previous stress fracture
- Rapid increase in activity
Pathophysiology and Mechanisms
Femoral neck anatomy:
The femoral neck is vulnerable to stress fractures due to:
- High bending loads during weight-bearing activities
- Limited blood supply (risk of AVN)
- Thin cortical bone especially superiorly
Superior cortex - TENSION forces:
During single-leg stance, the femoral neck experiences bending moments:
- Superior cortex is under TENSION (pulling apart)
- Inferior cortex is under COMPRESSION (pushing together)
Tension forces cause:
- Cracks to propagate rather than close
- Higher risk of complete fracture
- Potential for sudden displacement
This is why tension-side stress fractures are surgical emergencies - the crack can propagate and displace suddenly.
Stress fracture pathophysiology:
- Bone remodeling imbalance: Resorption exceeds formation
- Microdamage accumulation: Repetitive loading
- Stress reaction: Bone edema without fracture line
- Stress fracture: Fracture line develops
- Complete fracture: Full-thickness propagation
Early detection at stress reaction stage allows conservative management.
The tension on the superior femoral neck is not fixed - it is modulated by the hip abductors. In single-leg stance body weight creates a bending moment that tenses the superior cortex, but a contracting gluteus medius and minimus pull on the proximal femur and add a compressive, offsetting load across the neck, lowering the net superior tensile strain. This is why abductor fatigue matters: late in a marathon or a long march the tiring abductors stop neutralising the bending moment, superior tensile strain rises, and the fatigue fracture propagates - explaining the classic late-in-endurance-event onset. The practical consequences follow from the same idea: hip-abductor and core conditioning are part of prevention and of graded return to sport, and gait retraining that reduces excessive hip adduction (and contralateral pelvic drop) unloads the superior neck. It also reinforces the tension-side rule - once the protective muscle force is overwhelmed, the superior crack only ever sees distraction, so it cannot be trusted to heal without fixation.
Classification Systems
Tension vs Compression:
- Location
- Superior cortex
- Risk
- HIGH - displacement risk
- Treatment
- Surgical fixation
- Location
- Inferior cortex
- Risk
- Lower
- Treatment
- Conservative possible
- Location
- Both cortices
- Risk
- Highest
- Treatment
- Surgical - urgent
Location is THE key factor in management decisions. Always determine if the fracture involves the superior (tension) or inferior (compression) cortex.
A stress fracture is either a fatigue fracture - abnormal (excessive/repetitive) load on normal bone (the runner/recruit picture this topic centres on) - or an insufficiency fracture - normal physiological load on abnormal (weakened) bone. The distinction reframes the whole work-up. In a young athlete or recruit with a femoral neck stress fracture, the driver is training error plus RED-S, and you screen energy availability, menses, vitamin D and BMD. In a middle-aged or older patient (or any atypical host), an "insufficiency" FNSF should trigger a search for osteoporosis, osteomalacia (low vitamin D, raised ALP), coxa vara, prolonged corticosteroid use, inflammatory arthritis and bisphosphonate-related bone changes, because the bone - not the load - is the problem. Both occur on the tension or compression side and both follow the same fix-the-tension-side rule, but fatigue fractures need load and energy correction while insufficiency fractures need the underlying metabolic bone disease treated or they recur and fixation fails.
FULLERTONFULLERTON - Classification
Hook:FULLERTON classification guides treatment decisions
Clinical Assessment
- Young athlete or military recruit
- Insidious onset groin pain
- Activity-related symptoms
- Pain worse with impact activities
- May have preceding prodromal ache
- Training history (recent increases?)
- Menstrual history (females)
- Dietary intake and RED-S screening
- Previous stress fractures
- Medication history (steroids, bisphosphonates)
In any athlete with stress fracture, screen for Relative Energy Deficiency in Sport (RED-S) - the updated term for female athlete triad. This includes low energy availability, menstrual dysfunction, and bone health issues.
Physical examination:
Key tests:
- Technique
- Observe walking
- Finding
- Antalgic gait
- Technique
- Passive rotation in extension
- Finding
- Groin pain
- Technique
- Single leg hop
- Finding
- Pain reproduction
- Technique
- Femur over forearm as fulcrum
- Finding
- Pain with loading
- Technique
- Hip ROM tests
- Finding
- Groin pain, reduced ROM
Hop test:
- Should NOT be performed if high clinical suspicion
- Risk of displacing an incomplete fracture
- Use clinical judgment
The single-leg hop test can reproduce pain but risks displacing an incomplete fracture. If clinical suspicion is high, proceed directly to imaging rather than provocative testing.
Differential diagnosis of activity-related groin/hip pain in the young athlete:
- Discriminating features
- Insidious load-related groin pain, worse with impact; pain on log roll/axial loading; high-risk population
- Key investigation
- MRI (bone marrow oedema, fracture line, tension vs compression)
- Discriminating features
- Sharp anterior groin pain with flexion-rotation; positive FADIR; clicking/catching
- Key investigation
- MRI arthrogram; X-ray for cam/pincer morphology
- Discriminating features
- Pain on resisted adduction or hip flexion; localised tenderness; acute onset
- Key investigation
- Clinical; ultrasound/MRI if persistent
- Discriminating features
- Lower abdominal and adductor-origin pain; pain on resisted sit-up and Valsalva
- Key investigation
- MRI of pubic symphysis and rectus/adductor aponeurosis
- Discriminating features
- Groin or buttock pain in runner; tender pubic ramus or sacrum
- Key investigation
- MRI of pelvis
- Discriminating features
- Groin pain, steroid/alcohol history; pain on extremes of rotation
- Key investigation
- MRI (subchondral crescent, double-line sign)
- Discriminating features
- Rest pain, fever, marked ROM restriction, raised inflammatory markers
- Key investigation
- Bloods, aspiration; MRI/US for effusion
Investigations
Clinical Imaging
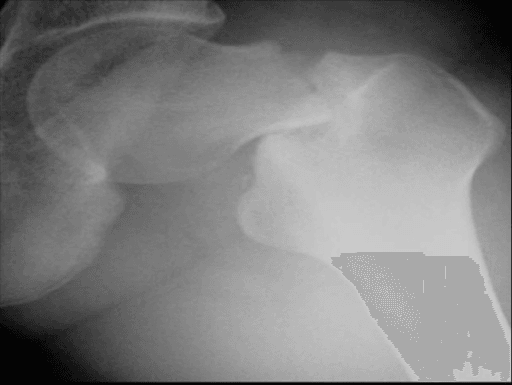
- Often negative for 2-4 weeks
- May show sclerotic line, periosteal reaction
- Full-length views recommended
- Compare to contralateral side
- Detects stress reaction before fracture line visible
- Shows bone marrow edema (T2/STIR hyperintense)
- Identifies fracture line if present
- Determines tension vs compression involvement
- Essential for early diagnosis
MRI shows bone marrow edema (bright on T2/STIR, dark on T1) in stress reactions. A fracture line appears as low signal on all sequences. Location of findings determines if tension or compression side involved.
- Clinical suspicion with negative X-rays
- Early diagnosis critical (athletes in-season)
- Determine extent and location
- Monitor healing progress
- Better for visualizing cortical fracture lines
- Less sensitive for early stress reaction
- Useful if MRI contraindicated or equivocal
- Highly sensitive but less specific
- Shows focal uptake at fracture site
- Less commonly used now due to MRI availability
- Cannot distinguish tension vs compression
- Vitamin D level
- Calcium
- TSH (if RED-S suspected)
- Consider DEXA for BMD (if triad/RED-S)
Management
SURGICAL MANAGEMENT REQUIRED:
Tension-side (superior cortex) stress fractures have high displacement risk and require prophylactic fixation.
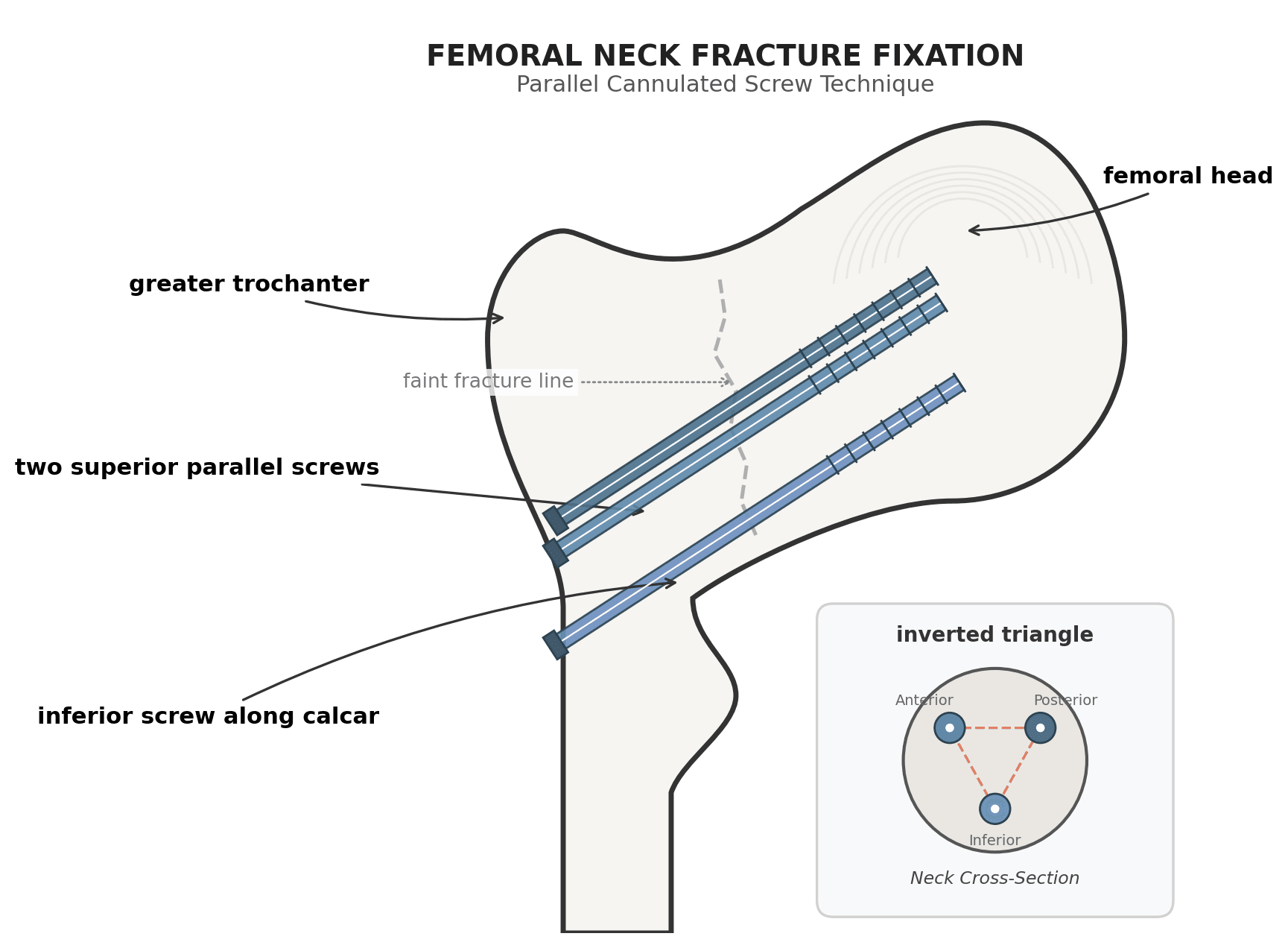
- Multiple cannulated screws (typically 3, inverted triangle) — historically standard in young athletes with good bone
- Sliding hip screw (SHS) or cephalomedullary nail — increasingly favoured, especially in poorer bone, larger fractures or non-compliant patients; a fixed-angle device better resists varus and the implant choice may reduce the subtrochanteric stress-riser risk seen after isolated cannulated screws (Hwang 2022)
- Valgus osteotomy or arthroplasty reserved for salvage/non-union/AVN
- Supine on fracture table
- Image intensifier guidance
- 3 cannulated screws in inverted triangle, or SHS as above
- Ensure no screw in weight-bearing dome
- Avoid a low (distal) starting point that creates a subtrochanteric stress riser
- Protected weight bearing initially
- Progress as healing confirmed
- Return to sport when united and pain-free
Do not delay surgery for tension-side fractures.
TENSIONTENSION - Superior Side Management
Hook:TENSION side = Top side = T for TROUBLE - needs surgery!
COMPRESSIONCOMPRESSION - Inferior Side Management
Hook:COMPRESS = Can usually Conservative Manage if only inferior cortex
Surgical Technique
- Supine on fracture table or radiolucent table
- Image intensifier access for AP and lateral
- Slight internal rotation of leg
- Unaffected leg in lithotomy position
- Confirm fracture location on imaging
- Mark skin incision
- Ensure adequate fluoroscopy images
- Prepare for closed vs open approach
Most cases can be done percutaneously with fluoroscopic guidance.
Complications
- Risk Factors
- Tension side, delayed diagnosis
- Prevention/Management
- Early surgery for tension side, non-weight bearing
- Risk Factors
- Displacement, delayed fixation
- Prevention/Management
- Urgent treatment, anatomic reduction
- Risk Factors
- Displacement, inadequate fixation, metabolic factors
- Prevention/Management
- Revision surgery, bone grafting
- Risk Factors
- Inadequate fixation, early loading
- Prevention/Management
- Proper technique, protected weight bearing
- Risk Factors
- Failure to address risk factors
- Prevention/Management
- Treat underlying causes, gradual return
- Risk Factors
- Metabolic factors, inadequate rest
- Prevention/Management
- Extended non-weight bearing, optimize bone health
- Most feared complication
- Risk increases with displacement
- Time to treatment matters
- May occur despite optimal care
- Monitor long-term
- More common if displaced
- Risk factors: smoking, metabolic bone disease, poor fixation
- Treatment: revision with bone graft, valgus osteotomy, or arthroplasty
AVN risk is directly related to degree of displacement and time to treatment. Tension-side fractures have higher AVN risk because they are more likely to displace. Urgent surgical fixation minimizes this risk.
Postoperative Care and Rehabilitation
Postoperative protocol:
- Protected weight bearing (toe-touch or partial)
- Hip ROM exercises
- Core and upper body conditioning
- Aquatic therapy when wound healed
- Serial X-rays at 2 and 6 weeks
- Progress weight bearing as healing allows
- X-ray to confirm early union
- Stationary bike
- Progressive hip strengthening
- Continue cross-training
- Full weight bearing when united
- Progress to impact activities
- Running progression (if athlete)
- Sport-specific training
- Final MRI to confirm healing
- Union confirmed on imaging
- Full, pain-free ROM
- Strength symmetry
- Functional testing passed
- Underlying risk factors addressed
- Compression side (conservative): 3-4 months
- Tension side (surgical): 4-6 months
- Displaced fracture: 6-12 months (depends on AVN)
Outcomes and Prognosis
Prognostic factors:
- Better Prognosis
- Compression side
- Worse Prognosis
- Tension side
- Better Prognosis
- Early (stress reaction)
- Worse Prognosis
- Late (complete fracture)
- Better Prognosis
- Non-displaced
- Worse Prognosis
- Displaced
- Better Prognosis
- Urgent appropriate care
- Worse Prognosis
- Delayed treatment
- Better Prognosis
- Addressed
- Worse Prognosis
- Unaddressed
Expected outcomes by type (figures are approximate; outcome is dominated by displacement and time-to-diagnosis):
- High union rate with compliant non-weight bearing and serial imaging
- Return to sport typically 3-4 months
- Long-term prognosis excellent once healed, provided RED-S/metabolic drivers are corrected
- Good union with timely fixation
- Return to sport typically 4-6 months
- AVN risk increases with any displacement or delay
- Markedly worse: high AVN and non-union risk; sporting outcomes considerably worse once displaced (Robertson & Wood 2017)
- May require arthroplasty if AVN develops
Athletic case series report encouraging return-to-sport rates when FNSF is caught early. However, in operatively treated military trainees, 58% were ultimately separated from service despite surgery, and 39% showed fracture-line progression (Shaw 2022). The lesson for the viva: outcome hinges on early diagnosis before displacement, the demand of the population, and correcting the underlying cause — not on the operation alone.
Prevention and Return to Sport
- Gradual load progression (10% rule)
- Adequate rest days
- Cross-training to reduce impact
- Proper footwear
- Appropriate running surfaces
- Adequate caloric intake
- Calcium: 1000-1500mg daily
- Vitamin D: maintain greater than 75 nmol/L
- Avoid relative energy deficiency
- Menstrual history in all female athletes
- RED-S screening questionnaire
- Low threshold for endocrine referral
- Bone health assessment if abnormalities
- Address all modifiable risk factors
- Gradual return to sport
- Cross-training during recovery
- Long-term bone health monitoring
Guidelines, Registries & Global Practice
Femoral neck stress fracture (FNSF) is a globally consistent diagnosis with a single overriding management principle — location (tension vs compression) and displacement drive treatment — that holds across every major board and health system.
Global epidemiology:
- Setting
- Athletic
- Relative risk / notes
- Commonest civilian group; FNSF approximately 3% of sport-related stress fractures (Robertson & Wood 2017)
- Setting
- Occupational
- Relative risk / notes
- High-volume new loading; baseline all-site stress fracture ~5-6% per training cycle (Lappe 2008); FNSF a high-consequence subset
- Setting
- Athletic
- Relative risk / notes
- Risk rises with cumulative triad factors; high-risk runners ~4.4x trabecular-rich BSI (Roche 2023, Barrack 2014)
- Setting
- Athletic
- Relative risk / notes
- Over-represented via low energy availability
- Setting
- General
- Relative risk / notes
- Insufficiency-type FNSF; consider osteomalacia, osteoporosis, coxa vara (Tomar 2020)
Major guidance, side by side:
- Position on FNSF
- Femoral neck (tension side) classed as a HIGH-RISK stress fracture: image early, low threshold for fixation; tension-sided and displaced → surgery
- Evidence basis
- Expert consensus + cohort data (Level III-IV)
- Position on FNSF
- Treat as fragility/at-risk presentation where relevant; urgent senior review and theatre for displaced neck fractures; metabolic work-up
- Evidence basis
- Consensus / standards
- Position on FNSF
- Fixation principles: stable internal fixation for unstable/tension or displaced patterns; fixed-angle implants where bone quality is poor
- Evidence basis
- Mechanistic + cohort
- Position on FNSF
- Mandatory screening and treatment of low energy availability in any athlete with a bone stress injury
- Evidence basis
- Consensus (Level II-III supporting data)
There is no genuine international disagreement on the core algorithm: the tension/compression split and the imperative to fix tension-sided and displaced injuries are universal. Practice variation lies mainly in implant choice (cannulated screws vs sliding hip screw / cephalomedullary nail) and in the surgical threshold for compression-sided injuries — a commonly cited operative trigger is involvement of more than ~50% of the neck width or any fracture-line progression (Shaw 2022).
FNSF is not separately tracked in arthroplasty registries (NJR, AJRR, AOANJRR, SHAR), but those registries do inform salvage outcomes when AVN or non-union leads to arthroplasty in a young patient — generally good implant survival but a high revision burden over a long expected lifespan, reinforcing the priority of joint-preserving early fixation.
- High-resource settings: ready MRI access enables early diagnosis at the stress-reaction stage; multidisciplinary RED-S pathways (sports physician, dietitian, endocrinologist).
- Limited-resource settings: reliance on radiographs and bone scan delays diagnosis, increasing displacement and AVN; a higher index of suspicion and earlier protected weight-bearing partly offset limited cross-sectional imaging.
sports/orthopaedic assessment → urgent MRI → operative vs protected non-operative care by location → metabolic and RED-S work-up → staged return to load with bone-health optimisation.
MCQ Practice Points
Q: Which side of the femoral neck requires prophylactic fixation? A: The tension side (superior cortex). It carries a high risk of progression and displacement with subsequent AVN, so prophylactic fixation is advised even when minimally displaced. Compression side (inferior cortex) fractures are more stable and can often be managed conservatively with close imaging follow-up.
Q: What is the gold standard imaging for suspected stress fracture with negative X-rays? A: MRI. It has 100 percent sensitivity and detects bone marrow edema weeks before a fracture line is visible on X-ray (which has only 10-40 percent sensitivity early on).
Q: What are the components of the Female Athlete Triad? A: Low energy availability, menstrual dysfunction, and low bone mineral density. This increases stress fracture risk by 2-4x and must be screened for in all female athletes.
Q: What is the recommended screw configuration for femoral neck fixation? A: Three cannulated screws in an inverted triangle pattern. This provides optimal stability. Screws must assume a position along the calcar and avoid the weight-bearing dome.
Q: What is the target Vitamin D level for stress fracture healing? A: Greater than 75 nmol/L. Levels below this impair bone healing and increase recurrence risk. Supplementation is part of standard management.
Q: which factor most strongly correlates with AVN risk? A: Displacement. The degree of displacement and time to reduction/fixation determines the risk of vascular disruption to the femoral head.
Exam Cheat Sheet
Key Decision - Tension vs Compression
- TENSION (superior cortex) = SURGERY
- COMPRESSION (inferior cortex) = Conservative possible
- Tension side: high progression/displacement risk - fix even if minimally displaced
- Compression side: more stable - non-weight bearing with serial imaging
- Surgical threshold for compression side: progression or involvement of more than half the neck width
- This is THE exam question - get it right!
Diagnosis
- MRI is gold standard (X-rays often negative)
- Bone marrow edema on T2/STIR (early sign)
- Fracture line visible in higher grades
- Full-length femur X-ray to rule out shaft involvement
- Determine tension vs compression involvement
Surgical Technique
- Three cannulated screws (6.5-7.3mm)
- Inverted triangle configuration
- Fluoroscopic guidance (AP and Lateral)
- No screw in weight-bearing dome
- Posterior cortex engagement essential
Female Athlete Triad/RED-S
- Low energy availability (dietary)
- Menstrual dysfunction (amenorrhea)
- Low bone mineral density (osteopenia)
- Screen ALL female athletes with stress fractures
- involve sports dietitian and endocrinologist
Complications
- AVN - related to displacement degree
- Nonunion - metabolic factors/smoking
- Recurrence - if risk factors not addressed
- Hardware failure if early weight bearing
- Coxa vara deformity if reduction lost
Return to Sport
- Union confirmed on imaging (MRI/CT)
- Pain-free with activity and hop test
- Underlying causes addressed (Vitamin D)
- Gradual return with cross-training
- Typically 3-6 months depending on severity
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old female marathon runner presents with 4 weeks of activity-related groin pain. She has increased her training significantly in the past 2 months. X-rays are negative. How do you proceed?”
“MRI shows bone marrow edema involving the superior cortex with a fracture line. How do you manage this?”
“A 25-year-old male military recruit was diagnosed with compression-side femoral neck stress fracture and has been non-weight bearing for 6 weeks. Follow-up imaging shows fracture line progression. What do you do?”
Evidence Base
Fullerton & Snowdy — Original Classification and Treatment Series
- 54 femoral neck stress fractures identified prospectively over 4 years
- Generated the tension / compression / displaced treatment classification
- Notably reported NON-progression of tension-side fractures under careful protocols, but displacement remains the catastrophic risk that justifies fixation
Robertson & Wood — Current Concepts Review (Sport)
- FNSF ~3% of sport-related stress fractures
- MRI is the key second-line investigation when radiographs are normal
- Delayed diagnosis drives displacement; sporting outcomes are considerably worse once displaced
- Early detection yields good return-to-sport rates
Shaw et al. — Operative FNSF in Military Trainees (CORR)
- Surgical threshold used: complete, tension-sided, or compression-sided involving more than 50% of neck width
- 39% showed fracture-line progression on repeat imaging
- T1 oedema extent plus effusion predicted final fracture size
- 58% separated from military service despite surgery
Hwang et al. — Implant Choice and Stress-Riser Risk
- Cannulated screws can create a subtrochanteric stress riser, particularly with low starting points or poor bone
- Sliding hip screw or cephalomedullary nail recommended over cannulated screws in many cases
- Mandatory metabolic work-up for all FNSF patients
Lappe et al. — Calcium and Vitamin D RCT (Stress-Fracture Prevention)
- Large double-blind RCT (n=5,201)
- 20% relative reduction in stress-fracture incidence with calcium + vitamin D
- Supports nutritional optimisation in high-risk loading populations
Barrack et al. — Cumulative Female Athlete Triad Risk (AJSM)
- BSI incidence scales with the NUMBER of Triad risk factors
- Single factor ~15-20%; combined factors 30-50%
- Low BMD + high training volume: OR 5.1
- Cumulative-risk model underpins the Triad Cumulative Risk Assessment
Roche/Nattiv et al. — Triad Risk and Trabecular-Rich BSI
- High Triad risk: 4.40x trabecular-rich BSI (e.g. femoral neck)
- Each 1-point Triad CRA increase: +26% trabecular-rich BSI risk
- Trabecular-rich sites are especially sensitive to biological/energy risk factors
AAOS / BOA / consensus guidance on high-risk stress fractures
- Femoral neck (tension side) is a recognised HIGH-RISK stress-fracture site
- High-risk sites warrant earlier imaging, protected weight-bearing and a lower surgical threshold
- Guidance is consistent across major societies on the tension/compression operative split