Stulberg Classification of Perthes Outcome
Examiners expect you to define each Stulberg class by the femoral head shape AND the head-acetabulum relationship — sphericity alone is not enough. A Class III (ovoid head in an ovoid socket) is congruent, not incongruent. A Class V (flat head in a round socket) is the one that is truly incongruent and carries the worst prognosis. Class V patients often develop symptomatic OA in their thirties or forties, whereas Classes I–II may never develop significant arthritis. State the class, define the morphology, and give the prognosis in one sentence.
The Stulberg Classification — Five Classes
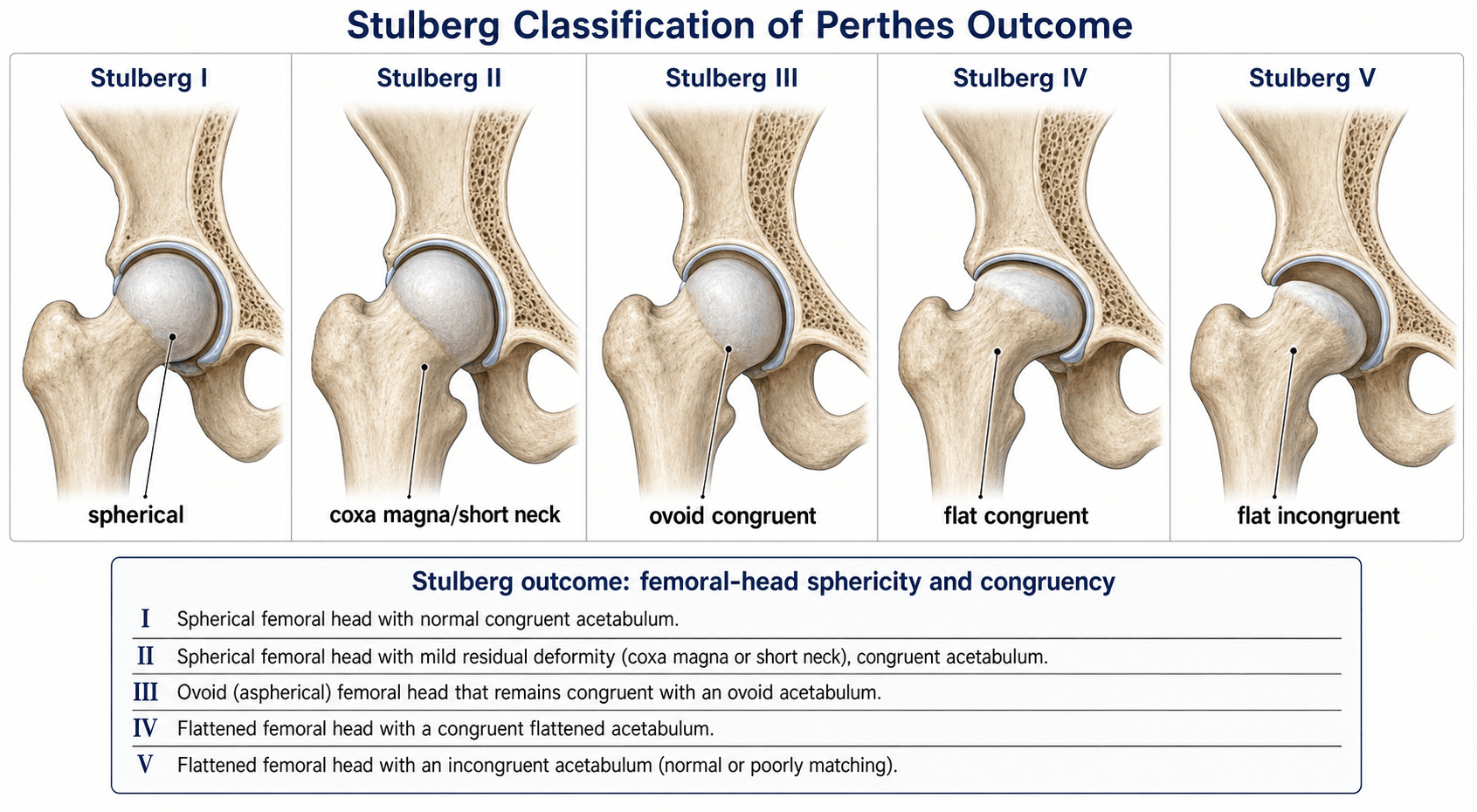

The Stulberg classification (Stulberg, Cooperman & Wallensten, 1981) grades the radiographic appearance of the hip at skeletal maturity after Perthes disease, assessing femoral head sphericity and head-acetabulum congruency on the AP (and frog-leg lateral) pelvic radiographs.
- Femoral Head Shape
- Spherical
- Head–Acetabulum Relationship
- Congruent (spherical head in spherical socket)
- Prognosis
- Excellent — near-normal hip, low OA risk
- Femoral Head Shape
- Spherical
- Head–Acetabulum Relationship
- Congruent (spherical head, spherical socket; slight enlargement or coxa magna)
- Prognosis
- Good — low OA risk, may have mild symptoms late
- Femoral Head Shape
- Non-spherical (ovoid or mushroom-shaped)
- Head–Acetabulum Relationship
- Congruent (ovoid head in ovoid socket, not spherical)
- Prognosis
- Fair — moderate OA risk by age 50–60
- Femoral Head Shape
- Non-spherical (flat)
- Head–Acetabulum Relationship
- Congruent (flat head in flat socket)
- Prognosis
- Fair-to-poor — significant OA risk by middle age
- Femoral Head Shape
- Non-spherical (flat)
- Head–Acetabulum Relationship
- Incongruent (flat head in spherical socket)
- Prognosis
- Poor — early OA, often symptomatic by 30s–40s
Spherical · Spherical · Ovoid · Flat · IncongruentRemember the five Stulberg classes
Hook:The key divider is II vs III (spherical vs non-spherical); the second is IV vs V (congruent flat vs incongruent flat — V is the worst).
Coxa magna (enlargement of the femoral head) is common after Perthes and, by itself, does NOT indicate a worse Stulberg class — a large but spherical head in a congruent socket is Class II. Examiners test this distinction.
Principles Behind the Classification
The Stulberg system is rooted in two biomechanical principles:
- Sphericity of the femoral head determines contact area. A spherical head distributes load over the maximum articular surface, minimising peak contact stress. Loss of sphericity concentrates load on a smaller area, accelerating cartilage wear.
- Congruency between the femoral head and acetabulum determines whether the joint surfaces match. Congruent aspheric joints (Classes III–IV) redistribute load imperfectly but symmetrically, so OA develops more slowly. Incongruent joints (Class V) create edge-loading and rapid cartilage degeneration.
A flat femoral head articulating against a spherical acetabulum creates point-loading at the edges of contact. This mechanical mismatch accelerates cartilage loss far more than a flat-on-flat congruent joint (Class IV), even though both are non-spherical.
A spherical head — whether normal-sized (I) or enlarged/coxa magna (II) — maintains normal biomechanics. The acetabulum remodels to match a coxa magna head during growth, preserving congruency. Long-term OA risk approximates that of the general population.
In children, the acetabulum has substantial remodelling capacity. If the femoral head remains contained during the Perthes disease process, the acetabulum remodels to match the head shape — this is why containment treatment aims to preserve sphericity and congruency.
GAGEL — head-at-risk signsHead-at-risk signs (predict poor Stulberg outcome)
Hook:The more head-at-risk signs present during the active phase, the worse the expected Stulberg class — they drive the decision to contain (femoral/Salter osteotomy or shelf).
Everything in active treatment is in service of a better Stulberg class, and the unifying concept is containment:
- The principle: during the biologically plastic fragmentation/reossification phase, keeping the soft femoral head deep and covered within the acetabulum lets the head remodel toward a sphere and the acetabulum mould around it — the acetabulum is the mould. A contained head trends toward Stulberg I–II; an uncovered, subluxing head deforms toward IV–V.
- Containability — the arthrogram question: a dynamic arthrogram shows whether the head reduces congruently in abduction or hinges on the lateral acetabular edge (hinge abduction = a deformed, non-containable head). A hinging hip is NOT helped by simple abduction/containment and needs a different plan (e.g. a valgus osteotomy to swing a congruent segment into the joint).
- Non-operative: maintain range of motion (physiotherapy); abduction bracing has been used but high-level evidence is weak (the Herring study found no benefit of bracing over observation).
- Femoral varus derotation osteotomy — contains the head by redirecting the neck; watch for limb shortening, trochanteric overgrowth and residual varus.
- Pelvic osteotomy (Salter innominate, or triple) — improves anterolateral coverage; the meta-analysis found pelvic procedures did better than femoral in the under-6s.
- Combined femoral + pelvic for severe under-coverage.
- Salvage for the non-containable/hinging or late-presenting hip: shelf acetabuloplasty or Chiari osteotomy to augment coverage, or a valgus (± extension) osteotomy to relieve hinge abduction.
- Who benefits (evidence): age over 8 (skeletal age over 6) with lateral pillar B or B/C does better with surgery; under-6 or lateral pillar A do well with observation; lateral pillar C does poorly regardless.
Clinical Application — From Active Disease to Stulberg Outcome
The Stulberg classification is applied retrospectively at maturity, but treatment during the active phase of Perthes disease aims to achieve the best possible Stulberg class. The clinical pathway is:
- Timing
- Age 4–8 typically
- Key Decision
- Confirm diagnosis; exclude differential (septic arthritis, epiphyseal dysplasia)
- Goal for Stulberg Outcome
- Establish baseline and lateral pillar class
- Timing
- Months 6–12
- Key Decision
- Assess head-at-risk signs; decide on containment
- Goal for Stulberg Outcome
- Prevent lateral subluxation and femoral head deformity
- Timing
- 1–3 years
- Key Decision
- Maintain containment; monitor head sphericity
- Goal for Stulberg Outcome
- Preserve or restore sphericity (target Class I–II)
- Timing
- Skeletal maturity
- Key Decision
- Apply Stulberg classification; counsel on prognosis
- Goal for Stulberg Outcome
- Predict OA risk; plan long-term surveillance
The Herring lateral pillar classification (assessed during the fragmentation phase) is the strongest predictor of the final Stulberg class. Lateral pillar Group A almost always achieves Stulberg I or II. Group C has a high likelihood of Stulberg IV or V. Group B and B/C border groups are the ones where containment treatment makes the biggest difference. Always mention Herring when discussing Stulberg prognosis in a viva.
Stulberg is the OUTCOME measure; examiners expect you to place it among the systems used DURING the disease and to know when each applies:
- Salter-Thompson (A/B) — earliest, based on the extent of the subchondral fracture (crescent sign): Group A (under half the dome involved, better) versus Group B (over half, worse). Its value is that it can be applied early, at the crescent-sign stage.
- Catterall (4 groups) — by the extent of epiphyseal involvement on AP and frog-leg lateral: I (anterior involvement only, no sequestrum), II (sequestrum with intact lateral margin), III (most of the head, only a small intact part), IV (whole head). Higher group plus "head-at-risk" signs predicts a worse result; limited by being a relatively late, less-reliable assessment.
- Herring lateral pillar (A / B / B-C border / C) — at the fragmentation phase, by the height of the lateral pillar: A (no height loss, almost always good), B (more than half the height maintained), B/C border (about half, narrowed or poorly ossified), C (less than half the height, worst). The strongest treatment-guiding predictor of the final Stulberg class.
- Mose — an outcome measure (concentric-circle template): deviation of the head from a true circle under 2 mm is good, about 2 mm fair, over 2 mm poor. Older sphericity tool, still used in some outcome studies (e.g. alongside Stulberg in meta-analyses).
The map: Salter-Thompson (early/crescent) → Catterall and Herring (fragmentation, to guide treatment) → Mose and Stulberg (healing/maturity, to grade the result). Don't apply Herring/Catterall at maturity or Stulberg during the active phase.
Prognostic Implications and Long-Term Outcomes

- OA Risk by Age 50
- Very low (similar to general population)
- Typical Age of Symptom Onset
- Unlikely
- Likely Intervention Needed
- None or conservative
- OA Risk by Age 50
- Low
- Typical Age of Symptom Onset
- Late (if ever)
- Likely Intervention Needed
- Conservative; rare THR after age 60
- OA Risk by Age 50
- Moderate (roughly 30–50 percent)
- Typical Age of Symptom Onset
- 50s–60s
- Likely Intervention Needed
- Conservative initially; THR in 50s–60s
- OA Risk by Age 50
- Moderate-to-high (roughly 50–75 percent)
- Typical Age of Symptom Onset
- 40s–50s
- Likely Intervention Needed
- THR likely by 50s
- OA Risk by Age 50
- High (over 75 percent)
- Typical Age of Symptom Onset
- 30s–40s
- Likely Intervention Needed
- THR often needed by 40s
A patient who had Perthes disease as a child and presents with hip pain in their thirties or forties should raise suspicion for a poor Stulberg outcome (Class IV or V). Request an AP pelvis radiograph and classify the morphology before attributing symptoms to soft-tissue causes. These patients may need early referral to an arthroplasty surgeon.
Herring DURING · Stulberg AT THE ENDStulberg versus Herring — when to use each
Hook:One predicts (Herring, mid-disease), one measures (Stulberg, at the end) — don't mix them up.
Limitations and Modern Context
- Inter-observer reliability is moderate, particularly distinguishing Classes III from IV (both are non-spherical and congruent — the difference is ovoid versus flat). Some authors propose collapsing III and IV into a single category.
- Radiographic assessment only. The classification does not account for cartilage integrity (MRI-determined), labral pathology, or patient-reported outcomes — a patient with a Stulberg III hip may be asymptomatic while a Stulberg II patient may have pain from labral tearing.
- Age at onset matters independently. Children with onset before age 6 tend to achieve better Stulberg classes regardless of treatment, while those with onset after age 8 tend to do worse — the classification does not stratify by age.
- Stulberg was developed in the pre-MRI era and relies on plain radiographs. Modern MRI-based assessment of femoral head sphericity and cartilage health may provide more granular prognostication, but Stulberg remains the standard for outcome studies and exam purposes.
- Bilateral Perthes (in roughly 10–15 percent of cases) complicates classification because acetabular remodelling may be bilateral, and each hip must be classified independently.
Guidelines, Registries and Global Practice
- Perthes disease has no single universal guideline comparable to the NICE or AAOS pathways for arthroplasty. Management is guided by institutional protocols and expert consensus, primarily derived from the multicentre POSNA (Pediatric Orthopaedic Society of North America) studies and the European Paediatric Orthopaedic Society (EPOS) recommendations.
- Containment versus non-containment debate varies globally. North American practice historically favoured surgical containment (femoral varus osteotomy, Salter osteotomy) for head-at-risk patients, while some European centres (notably the UK and Scandinavia) have advocated non-operative management with physiotherapy and abduction bracing, citing that many lateral pillar B hips do well without surgery. The POSNA multicentre trial helped define the subgroup that benefits most from surgery.
- Age at onset drives practice variation. Most centres agree that children under age 6 with lateral pillar A or B disease can be managed non-operatively, while children over age 8 with lateral pillar B/C or C disease benefit from containment. The grey zone (age 6–8, lateral pillar B) is where practice varies most.
- Long-term follow-up recommendations differ: UK practice typically follows Perthes patients to skeletal maturity and then discharges if Stulberg I–II, while some centres in the US and Japan recommend lifelong periodic review for all Perthes patients regardless of outcome class, given the late OA risk.
Viva practice
Exam Viva
Practise clinical reasoning and management decisions out loud
“A 34-year-old man presents with progressive right hip pain. He had Perthes disease of the right hip as a child, treated conservatively. An AP pelvis radiograph shows a flat femoral head with a preserved spherical acetabular socket. What is the Stulberg classification, what is the prognosis, and how would you counsel him?”
“A 9-year-old girl presents with left hip pain and a limp. Radiographs show early fragmentation of the left capital femoral epiphysis with lateral pillar involvement estimated at approximately 50 percent of pillar height. She has Gage sign positive, lateral subluxation, and a horizontal physeal line. How would you classify her, what is the predicted Stulberg outcome without treatment, and what is your management plan?”
Exam cheat sheet
The five classes at maturity
- Class I: spherical head, congruent — excellent prognosis
- Class II: spherical head (coxa magna allowed), congruent — good prognosis
- Class III: ovoid or mushroom head, congruent (ovoid socket) — fair, moderate OA risk
- Class IV: flat head, congruent (flat socket) — fair-to-poor, significant OA risk
- Class V: flat head in spherical socket, incongruent — poor, early OA
Key prognostic divider
- Spherical (I–II) versus non-spherical (III–V) is the critical divide
- Congruent (I–IV) versus incongruent (V) determines OA timing
- Class V carries the worst prognosis: flat-on-round, early symptomatic OA
- Coxa magna alone does not worsen class if the head is spherical
Head-at-risk signs (predict poor Stulberg outcome)
- Gage sign — lateral epiphyseal V-shaped lucency
- Age over 6 at onset
- Growth plate involvement (horizontal physis or metaphyseal changes)
- Lateral pillar involvement (Herring B/C or C)
- Lateral subluxation of the femoral head
Clinical pearls
- Herring lateral pillar predicts Stulberg — apply Herring during fragmentation, Stulberg at maturity
- Multiple head-at-risk signs in a child over 8: offer containment surgery
- Class V patient in their thirties with hip pain: think early OA, get radiographs, refer early
- Distinguish Class III/IV (congruent, slower OA) from Class V (incongruent, faster OA)
Evidence
The natural history of Legg-Calvé-Perthes disease
- Landmark long-term study (88 patients/99 hips followed ~40 years, plus 68 patients/72 hips with complete serial films followed ~30 years) defining the five-class system on the maturity radiograph.
- Defined the THREE congruency categories that drive prognosis: spherical congruency (Classes I–II) → arthritis does NOT develop; aspherical congruency (III–IV) → mild-to-moderate arthritis in late adulthood; aspherical incongruency (V) → severe arthritis before age 50.
- Each class showed a characteristic pattern during the active disease and a specific long-term clinical/radiographic course.
Legg-Calvé-Perthes disease. Part II: prospective multicenter study of the effect of treatment on outcome
- Prospective multicentre study (438 patients/451 hips, age 6–12) using the lateral pillar classification and the Stulberg outcome.
- Lateral pillar group and age at onset were strong independent prognostic factors; over-8s with lateral pillar B or B/C border did significantly better with surgery than non-operatively.
- Group C did poorly and group B under age 8 did well regardless of treatment.
According to PubMed, the classification and the three-congruency concept are from Stulberg, Cooperman & Wallensten 1981 (J Bone Joint Surg Am 1981;63(7):1095-108; PMID 7276045). The lateral-pillar-predicts-Stulberg evidence is Herring et al. 2004 (PMID 15466720); the operative-versus-nonoperative meta-analysis is Nguyen et al. 2012 (DOI 10.1097/BPO.0b013e318269c55d); the 20-year predictive validity of the modified Stulberg is Huhnstock et al. 2021 (DOI 10.1302/0301-620X.103B12.BJJ-2021-0515.R1); and the inter-observer reliability (kappa 0.65) is Wiig et al. 2007 (DOI 10.1007/s11832-007-0020-x).