Hindfoot Degeneration | Loss of Inversion/Eversion | Posttraumatic Most Common
- Subtalar joint provides 20-30° of hindfoot inversion/eversion - critical for uneven ground
- 70-80% are posttraumatic - most from calcaneal fractures with Bohler angle loss
- Loss of motion causes compensatory midfoot stress - may develop adjacent arthritis
- Isolated subtalar arthrodesis maintains 70-80% normal hindfoot motion via other joints
- Triple arthrodesis gold standard for pantalocalcaneonavicular arthritis
- “Gait shows lack of hindfoot inversion on uneven ground - patient walks stiffly
- “Inject subtalar joint with local anesthetic under image guidance - diagnostic test
- “Broden views (40° pronation, 10-40° cephalad tilt) visualize posterior facet best
- “Isolated fusion preserves ankle and midfoot - better than triple for isolated disease
Three facets: anterior, middle, posterior. Posterior facet bears 70-80% load. Subtalar joint provides inversion/eversion for uneven ground adaptation. Loss causes compensatory midfoot stress and altered ankle mechanics.
70-80% are posttraumatic - most from calcaneal fractures. Bohler angle loss under 20° correlates with subtalar arthritis risk. Talar fractures involving posterior facet also high risk.
Fluoroscopy-guided subtalar injection with local anesthetic and steroid. If greater than 75% pain relief, confirms subtalar source. Essential to differentiate from ankle, midfoot, or sinus tarsi pathology.
Isolated arthrodesis for isolated disease. Triple arthrodesis for pantalocalcaneonavicular involvement. Preserve ankle joint at all costs. Malunion causes adjacent joint overload and deformity.
- Joints Involved
- Subtalar joint only
- Treatment
- Isolated subtalar arthrodesis
- Key Pearl
- Preserves midfoot and ankle - 70-80% normal motion maintained
- Joints Involved
- Two of triple joints
- Treatment
- Double arthrodesis (subtalar + TN)
- Key Pearl
- Consider triple if calcaneocuboid borderline - avoid isolated midfoot stress
- Joints Involved
- Subtalar with hindfoot malalignment
- Treatment
- Arthrodesis plus deformity correction
- Key Pearl
- MUST correct alignment - lateral column lengthening may be needed
- Joints Involved
- Pantalocalcaneonavicular
- Treatment
- Triple arthrodesis
- Key Pearl
- Coordinate with rheumatology - optimize disease control perioperatively
AMPSubtalar Joint Anatomy - Three Facets
Hook:AMP up the load - Posterior facet takes 70-80% of subtalar stress!
ISOLATEDIndications for Isolated Subtalar Arthrodesis
Hook:Keep subtalar fusion ISOLATED - preserve adjacent joints for better function!
Overview and Epidemiology
Subtalar arthritis is degenerative disease of the subtalar joint, most commonly arising after intra-articular calcaneal fractures. The subtalar joint complex consists of three facets (anterior, middle, posterior) between the talus and calcaneus, providing critical hindfoot inversion and eversion motion for walking on uneven ground.
The subtalar joint provides 20-30 degrees of hindfoot inversion and eversion, which is essential for adaptation to uneven terrain and normal gait mechanics. Loss of this motion causes compensatory stress at adjacent joints (ankle, midfoot) and significantly impairs function on slopes and irregular surfaces.
- Age: 40-60 years peak incidence (posttraumatic)
- Gender: Male greater than female (3:1) - reflects trauma pattern
- Posttraumatic: 70-80% of cases - calcaneal fractures most common
- Primary OA: Rare in isolation - usually associated with other hindfoot pathology
- Inflammatory: Rheumatoid, psoriatic, seronegative arthropathy
- Gait: Stiff hindfoot, reduced shock absorption
- Terrain: Difficulty on uneven ground, slopes, stairs
- Compensation: Increased midfoot and ankle stress
- Adjacent joints: Risk of secondary arthritis over time
- Activity limitation: Running, hiking significantly impaired
Pathophysiology and Mechanisms
The subtalar joint is anatomically complex with three articulating facets. The posterior facet bears 70-80% of the load and is most commonly involved in arthritis. The middle facet sits on the sustentaculum tali. The anterior facet is part of the talocalcaneonavicular joint complex. Understanding this anatomy is critical for surgical planning and approach selection.
Biomechanics
The subtalar joint provides primarily inversion and eversion motion (20-30 degrees total arc), which is coupled with:
- Ankle dorsiflexion: Subtalar eversion unlocks the midfoot
- Ankle plantarflexion: Subtalar inversion locks the midfoot
- Shock absorption: Dampens impact forces during heel strike
- Terrain adaptation: Allows foot to conform to uneven surfaces
- Location
- Large facet on posterior calcaneus
- Load Bearing
- 70-80% of subtalar load
- Clinical Significance
- Most commonly arthritic - primary surgical target
- Location
- Sustentaculum tali (medial)
- Load Bearing
- 15-20% of subtalar load
- Clinical Significance
- Support structure - involved in coalition and inflammatory disease
- Location
- Talar head (shares with TN joint)
- Load Bearing
- 5-10% of subtalar load
- Clinical Significance
- Continuous with talonavicular joint - may have combined pathology
Pathophysiology
- Calcaneal fracture: Intra-articular with joint surface incongruity
- Bohler angle loss: Less than 20° correlates with arthritis risk
- Cartilage damage: Direct injury plus abnormal loading
- Malunion: Altered mechanics accelerate degeneration
- Timeline: Symptoms typically develop 1-5 years post-injury
- Primary OA: Rare - usually associated with hindfoot malalignment
- Inflammatory: Rheumatoid, psoriatic, ankylosing spondylitis
- Coalition: Tarsal coalition with chronic abnormal stress
- Biomechanical: Cavus or planovalgus deformity overload
- Progression: Often involves multiple hindfoot joints
Classification and Grading
Etiological Classification
- Etiology
- Prior calcaneal or talar fracture
- Percentage
- 70-80%
- Treatment Considerations
- Most common - address malunion, correct alignment
- Etiology
- Idiopathic degeneration
- Percentage
- 10-15%
- Treatment Considerations
- Rare - rule out biomechanical causes
- Etiology
- Rheumatoid, psoriatic, seronegative
- Percentage
- 5-10%
- Treatment Considerations
- Systemic disease management essential
- Etiology
- Tarsal coalition with secondary changes
- Percentage
- 5%
- Treatment Considerations
- Consider coalition resection if appropriate age
Most cases are posttraumatic following calcaneal fractures.
The Rammelt-Zwipp Calcaneal-Malunion Classification
The alignment-correction tab and the Evidence Base (Zwipp; Rammelt) invoke this classification and the controversies debate "in-situ vs bone block", but the five deformity types that actually decide the operation are never set out - and they are the framework that matches deformity to procedure.
- Type I - arthritis, no malalignment → in-situ subtalar arthrodesis (the only type for which simple fusion suffices).
- Type II - arthritis plus a varus or valgus hindfoot deformity → distraction bone-block arthrodesis to realign and restore height.
- Type III - arthritis plus loss of height and dorsal tilting of the talus → distraction bone-block arthrodesis (restore talocalcaneal height and de-rotate the talus, relieving anterior ankle impingement).
- Type IV - additionally lateral translation of the calcaneus (causing hindfoot valgus and fibular abutment) → corrective calcaneal osteotomy through the old fracture plane, usually with a bone block.
- Type V - additionally talar tilt out of the ankle mortise → the rarest and most demanding; needs the osteotomy plus an anterior/anteromedial approach to the ankle.
- Zwipp also groups by bony status: A = malunion, B = nonunion, C = aseptic/septic osteonecrosis (Group C requires a preliminary radical necrectomy and a staged reconstruction).
Q: How does the Rammelt-Zwipp classification guide surgery for posttraumatic subtalar arthritis? A: Type I (no malalignment) → in-situ fusion; Types II-III (varus/valgus, lost height, dorsiflexed talus) → distraction bone-block arthrodesis; Type IV (lateral translation, fibular abutment) → corrective calcaneal osteotomy; Type V (talar tilt out of the mortise) → osteotomy + an anterior ankle approach. In-situ fusion is adequate only for Type I - the higher the type, the more correction (height, translation, osteotomy) is required.
Clinical Presentation
History
- Pain location: Sinus tarsi (lateral hindfoot), deep heel pain
- Worse with: Uneven ground, stairs, prolonged walking
- Stiffness: Morning stiffness, improves with activity initially
- Limp: Antalgic gait, avoids inversion/eversion
- History: Previous calcaneal or talar fracture (70-80%)
- Walking: Difficulty on slopes, uneven surfaces
- Running: Significantly limited or impossible
- Stairs: Pain with descent (loading in plantarflexion)
- Work: Difficulty with prolonged standing, manual labor
- Recreation: Hiking, sports participation limited
Physical Examination
Systematic Examination Approach
Standing: Assess hindfoot alignment (varus, valgus, neutral). Observe gait for stiffness and antalgic pattern. Look for prior surgical scars from calcaneal fracture fixation.
Swelling: Sinus tarsi fullness, lateral hindfoot edema common.
Sinus tarsi: Focal tenderness lateral to talus and anterior to lateral malleolus.
Subtalar joint line: Palpable posteriorly - tenderness with deep palpation.
Calcaneal deformity: Widening from prior fracture, prominence laterally.
Subtalar motion: Assess inversion/eversion with ankle in neutral. Normal is 20-30° total arc. Arthritic joint shows marked restriction (often less than 10°) and crepitus.
Ankle motion: Test to ensure pathology is subtalar, not ankle.
Midfoot: Assess Chopart joint mobility to identify adjacent pathology.
Subtalar stress test: Stabilize talus, move calcaneus in inversion/eversion. Pain and restriction indicate pathology.
Anterior drawer: Rule out ankle instability as pain source.
Talonavicular stress: Assess for combined pathology requiring triple fusion.
Hindfoot pain can arise from ankle, subtalar, talonavicular, or sinus tarsi syndrome. Diagnostic injection of the subtalar joint under fluoroscopy with local anesthetic is essential to confirm the pain source before surgical planning. Greater than 75% pain relief confirms subtalar origin.
Investigations
Imaging Protocol
Systematic Imaging Approach
AP, lateral, and oblique foot: Assess subtalar joint space, calcaneal morphology, adjacent joints.
Broden views: 40° foot pronation with 10°, 20°, 30°, 40° cephalad tube tilt. Best visualizes posterior facet - gold standard for subtalar joint assessment.
Harris axial view: Calcaneal axial view shows varus/valgus alignment and width.
Non-contrast CT: Coronal and sagittal reconstructions show joint space narrowing, subchondral sclerosis, osteophytes, and deformity.
Coalition assessment: Rule out tarsal coalition as etiology.
Surgical planning: Bone stock assessment, screw trajectory planning.
Indications: Differentiate subtalar arthritis from sinus tarsi syndrome, soft tissue pathology, or occult fracture.
Findings: Bone marrow edema, synovitis, ligament pathology.
Fluoroscopy-guided: Inject 2-3 mL local anesthetic plus steroid into posterior facet.
Interpretation: Greater than 75% pain relief confirms subtalar source. No relief suggests alternate diagnosis.
Radiographic Findings
- Significance
- Cartilage loss - grade severity (mild, moderate, severe)
- Best View
- Broden views (posterior facet), lateral foot
- Significance
- Chronic stress and bone remodeling
- Best View
- CT scan shows best detail
- Significance
- Marginal bone formation - indicates advanced disease
- Best View
- Lateral foot, CT coronal views
- Significance
- Posttraumatic with loss of calcaneal height
- Best View
- Lateral foot radiograph
- Significance
- Malalignment requires correction during fusion
- Best View
- Harris axial view, weight-bearing AP ankle
Differential Diagnosis
Lateral and posterior hindfoot pain is non-specific. The single highest-yield step is a fluoroscopy-guided diagnostic block before any fusion - imaging severity correlates poorly with the true pain generator.
- Distinguishing Features
- Sinus tarsi pain, worse on uneven ground, restricted inversion/eversion
- Key Test
- Broden/CT plus subtalar block (greater than 75% relief)
- Pitfall
- Mild radiographic change can still be symptomatic
- Distinguishing Features
- Focal sinus tarsi tenderness, often after sprain, joint space preserved
- Key Test
- MRI (synovitis/fibrosis), sinus tarsi block
- Pitfall
- Mislabelled as arthritis - no joint-space loss on CT
- Distinguishing Features
- Anterior ankle pain, worse with dorsi/plantarflexion arc
- Key Test
- Weight-bearing ankle films, ankle block
- Pitfall
- Fusing the subtalar joint will not relieve ankle pain
- Distinguishing Features
- Retromalleolar pain/swelling, pain on resisted eversion
- Key Test
- MRI/dynamic ultrasound
- Pitfall
- Tendon tear coexists with calcaneal malunion (lateral wall)
- Distinguishing Features
- Diffuse deep pain, history of steroid/trauma
- Key Test
- MRI bone marrow oedema
- Pitfall
- Plain films often normal early
- Distinguishing Features
- Younger patient, rigid flatfoot, recurrent sprains
- Key Test
- CT/MRI (talocalcaneal middle facet)
- Pitfall
- May be the underlying cause, not a separate diagnosis
Calcaneal Malunion: the Sequelae That Make In-Situ Fusion Insufficient
Since 70-80% of subtalar arthritis is posttraumatic (calcaneal fracture), the topic repeatedly refers to malunion, lost height, lateral-column shortening, bone block and osteotomy - but never explains the cluster of secondary problems a calcaneal malunion causes beyond the arthritis itself, which is exactly why simply fusing the joint in situ often fails.
- Loss of talocalcaneal height → a dorsiflexed ("horizontal") talus. When the calcaneus collapses, the talus is pushed into a more horizontal, dorsiflexed position (reduced talar declination). This jams the front of the ankle (anterior tibiotalar impingement) and blocks ankle dorsiflexion - the classic "flat-topped/horizontal talus" effect. Fusing the subtalar joint in situ leaves this untouched; restoring height with a distraction bone block re-tilts the talus and relieves the impingement (Rammelt: talar-declination corrected ~38%, height ~62%).
- Lateral-wall blow-out and lateral translation → subfibular/peroneal impingement. The widened, laterally-displaced calcaneus abuts the fibula (subfibular impingement) and impinges or tears the peroneal tendons - a common coexisting cause of lateral hindfoot pain (the peroneal row in the differential). This needs decompression of the lateral wall (± peroneal tenolysis) and, if the calcaneus is translated, a corrective osteotomy - not fusion alone.
- Heel widening, shortening and hindfoot malalignment (usually varus, sometimes valgus) cause shoe-fitting problems and altered load transfer.
- Bottom line: on CT and weight-bearing films, specifically look for lost height, a dorsiflexed talus, lateral-wall abutment and malalignment - their presence means in-situ fusion is insufficient, and you must restore height (bone block) and/or correct translation (osteotomy) and address the peroneal tendons.
Q: What does a calcaneal malunion cause beyond subtalar arthritis, and why does it matter? A: Lost talocalcaneal height dorsiflexes the talus → anterior ankle impingement and loss of dorsiflexion; the lateral-wall blow-out/translation → subfibular impingement and peroneal tendon pathology; plus heel widening and varus/valgus malalignment. In-situ subtalar fusion fixes none of these - so you restore height with a distraction bone block, decompress the lateral wall/peroneals, and correct translation with an osteotomy as the deformity dictates.
Management Algorithm
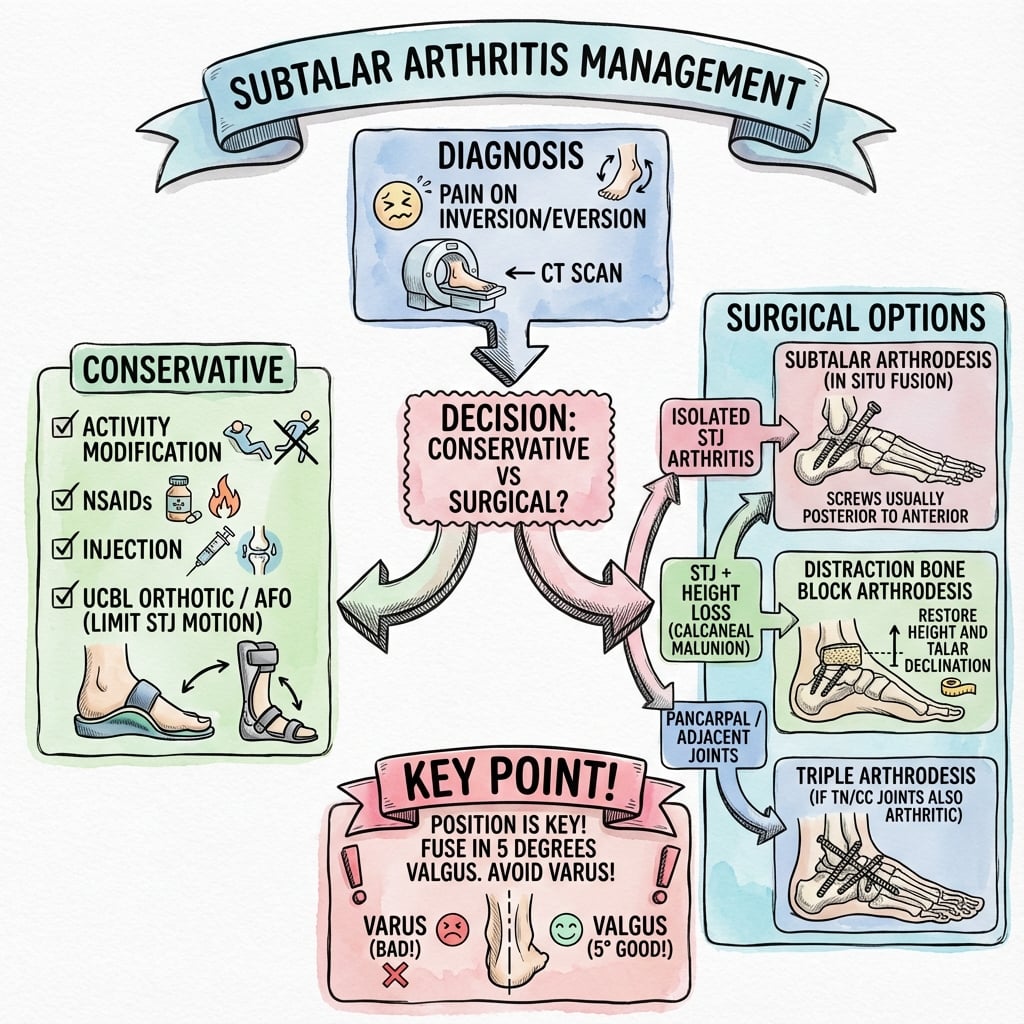
Non-Operative Treatment
Goal: Reduce pain, improve function, delay or avoid surgery.
Conservative Treatment Protocol
- Avoid uneven ground, reduce impact activities
- Low-impact exercise (swimming, cycling) encouraged
- Weight management if BMI over 30
- Avoid prolonged standing or walking
- Custom AFO: Ankle-foot orthosis with medial/lateral posting
- UCBL orthosis: University of California Biomechanics Lab insert
- Rocker-bottom shoe: Reduces subtalar motion demand
- Heel lift: If leg length discrepancy from malunion
- NSAIDs: First-line for inflammation (naproxen 500mg twice daily)
- Acetaminophen: For pain without inflammation
- Topical agents: NSAIDgels for localized pain
- Avoid opioids: Not indicated for chronic arthritis
- Corticosteroid injection: 40mg triamcinolone plus local anesthetic
- Fluoroscopy-guided: Essential for accurate placement
- Response: Greater than 75% relief confirms diagnosis
- Duration: 3-6 months relief typical, can repeat once
Surgical consideration is appropriate after at least 6 months of comprehensive conservative management including orthotics, activity modification, NSAIDs, and at least one diagnostic/therapeutic injection. Surgery is indicated when pain significantly limits function despite optimal non-operative treatment.
Surgical Technique
Subtalar Arthrodesis - Standard Technique
Indications: Isolated subtalar arthritis with preserved ankle and midfoot joints.
Operative Steps
- Position: Lateral decubitus with affected side up, OR supine with bump under ipsilateral hip
- Tourniquet: Thigh tourniquet at 300 mmHg
- Image: C-arm positioned for lateral and Broden views
- Prep and drape: Circumferential leg preparation
- Incision: Oblique incision over sinus tarsi, from tip of fibula toward talonavicular joint (4-5 cm)
- Dissection: Incise through sinus tarsi fat, expose subtalar joint
- Retraction: Protect peroneal tendons anteriorly, sural nerve posteriorly
- Visualization: Identify posterior facet - main arthrodesis target
- Cartilage removal: Use curettes, osteotomes, or burr to remove ALL cartilage down to bleeding subchondral bone
- Surfaces: Ensure congruent apposition of talus and calcaneus
- Maintain height: Avoid excessive bone resection - preserve calcaneal height
- Fish-scale surfaces: Create irregular surface for biological fusion
- Screws: Two 7.0mm or 7.3mm cannulated screws standard
- Trajectory: One screw from posterolateral calcaneus into talar body, second from posterior calcaneus into talar neck
- Imaging: Confirm position on lateral and Broden views
- Compression: Ensure good compression across joint surfaces
- Alignment check: Ensure 5° hindfoot valgus maintained
- Drain: Usually not required
- Deep closure: Repair sinus tarsi tissue if possible
- Skin: Subcuticular or interrupted sutures
- Splint: Short leg posterior splint in neutral ankle, 5° valgus hindfoot
Meticulous joint preparation is the key to successful fusion.
Complications
- Incidence
- 5-10%
- Risk Factors
- Smoking, diabetes, inadequate preparation, inflammatory arthritis
- Management
- Revision fusion with bone graft, optimize biology, smoking cessation essential
- Incidence
- 3-5%
- Risk Factors
- Inadequate intraoperative positioning, loss of fixation
- Management
- If symptomatic, revision osteotomy plus fusion. Prevention is key.
- Incidence
- 2-5%
- Risk Factors
- Lateral approach traction, direct injury
- Management
- Paresthesia common, permanent numbness rare. Prevention: careful retraction
- Incidence
- 2-3%
- Risk Factors
- Diabetes, smoking, lateral approach
- Management
- Wound care, antibiotics if infected. Delay weight-bearing until healed
- Incidence
- 10-15% at 10 years
- Risk Factors
- Pre-existing disease, malalignment, high activity
- Management
- Monitor clinically, may require future ankle or midfoot fusion
Key factors to minimize nonunion risk: (1) Complete cartilage removal to bleeding bone, (2) Congruent joint surfaces with good contact, (3) Rigid fixation with compression, (4) Smoking cessation for at least 6 weeks pre-op and 12 weeks post-op, (5) Optimize medical comorbidities (diabetes, nutrition), (6) Non-weight-bearing for 6-8 weeks post-op.
NONUNIONComplications of Subtalar Arthrodesis
Hook:Avoid NONUNION - prepare surfaces well, correct alignment, preserve nerves!
Postoperative Care and Rehabilitation
Rehabilitation Protocol - Isolated Subtalar Arthrodesis
- Immobilization: Short leg splint, strict non-weight-bearing
- Elevation: Leg elevated above heart to minimize swelling
- Ice: Cryotherapy as tolerated
- Pain control: Multimodal analgesia (acetaminophen, NSAIDs if no fusion concern, opioids minimal)
- DVT prophylaxis: Aspirin 81mg daily or LMWH if high risk
- Cast change: Transition to short leg cast at suture removal (2 weeks)
- Weight-bearing: Continue non-weight-bearing
- X-rays: 6-week radiographs to assess fusion progress
- Smoking: Continue strict cessation
- Bone stimulator: Consider if high-risk patient (diabetes, smoking history)
- CT scan: At 8-10 weeks if fusion status uncertain on X-ray
- Weight-bearing: Progress to partial weight-bearing in boot if fusion progressing
- Advancement: Full weight-bearing by 12 weeks if solid fusion
- Physical therapy: Start ankle and midfoot range of motion, gait training
- Transition to shoe: Supportive athletic shoe once full weight-bearing tolerated
- Strengthening: Progressive resistance exercises for ankle and foot
- Proprioception: Balance and stability training
- Return to activity: Gradual return to desired activities, avoid high-impact initially
- Final X-rays: 6-month radiographs confirm solid fusion
Outcomes and Prognosis
Functional Outcomes
Isolated subtalar arthrodesis provides excellent pain relief in 85-90% of patients with isolated subtalar arthritis. Patients regain ability to walk on level ground without pain, though difficulty persists on uneven terrain due to loss of inversion/eversion.
- Isolated Subtalar Fusion
- 85-90% significant improvement
- Triple Arthrodesis
- 90-95% significant improvement
- Isolated Subtalar Fusion
- 90-95% union
- Triple Arthrodesis
- 85-90% union (lower due to three joints)
- Isolated Subtalar Fusion
- Maintains 70-80% normal hindfoot motion via adjacent joints
- Triple Arthrodesis
- Complete hindfoot fusion - no inversion/eversion
- Isolated Subtalar Fusion
- Most return to low-impact activity by 6 months
- Triple Arthrodesis
- Longer recovery, more limitation on uneven ground
- Isolated Subtalar Fusion
- 10-15% at 10 years (ankle, midfoot)
- Triple Arthrodesis
- Higher ankle arthritis risk (20-30% at 10 years)
Factors associated with suboptimal results after subtalar arthrodesis: (1) Nonunion (most common cause of failure), (2) Malunion in varus or valgus (causes adjacent joint overload), (3) Pre-existing adjacent joint arthritis that progresses, (4) Unrealistic patient expectations about motion and activity, (5) Workers' compensation or litigation status, (6) Continued smoking or poor medical optimization.
Guidelines, Registries & Global Practice
- Posttraumatic dominance: 70-80% of subtalar arthritis follows calcaneal (and posterior-facet talar) fractures worldwide
- Calcaneal fracture burden: Up to ~2% of all fractures; predominantly young working-age men after falls from height
- Late arthrodesis: A recognised endpoint after both operative and non-operative calcaneal fracture care (Cochrane 2023)
- Resource link: Higher rates of severe malunion where displaced fractures are managed non-operatively without follow-up
- Arthroplasty registries (NJR, AJRR, AOANJRR, SHAR, NZJR) track joint replacement, not hindfoot fusion - so subtalar arthrodesis has no dedicated implant-survival registry
- Ankle fusion data from national datasets are the nearest comparator for union/complication benchmarking
- SSI surveillance: Foot and ankle procedures are captured in national surgical-site-infection programmes (e.g. UKHSA, US NHSN)
- Focus
- Perioperative VTE and SSI in foot/ankle surgery
- Practical Point
- Risk-stratified VTE prophylaxis; routine pharmacologic prophylaxis not mandated for all foot/ankle cases
- Focus
- Calcaneal and hindfoot trauma pathways
- Practical Point
- Specialist foot-and-ankle input and CT for intra-articular calcaneal fractures to plan reconstruction vs later fusion
- Focus
- Fracture and malunion reconstruction principles
- Practical Point
- Restore alignment first; deformity-matched correction (in-situ vs osteotomy vs bone block) before/with fusion
- Focus
- Smoking cessation and surgical safety
- Practical Point
- Perioperative smoking cessation and the WHO surgical checklist apply across resource settings
In high-resource settings, CT, fluoroscopic diagnostic blocks, and arthroscopic or deformity-correcting fusion are routine. In limited-resource settings, plain radiographs and in-situ fusion predominate, and displaced calcaneal fractures more often present late as fixed malunions requiring bone-block or osteotomy reconstruction.
fusion versus joint preservation, expected loss of inversion/eversion (difficulty on uneven ground), nonunion (5-10%), adjacent-joint arthritis (10-15% at 10 years), sural nerve injury (2-5%), and infection (1-3%). Document the trial of conservative care (minimum 6 months) and a positive diagnostic block before fusion - the commonest avoidable errors are fusing the wrong joint, malalignment, and inadequate smoking-cessation counselling.
Controversies and Areas of Uncertainty
The Buckley RCT (Sanders IV) showed no functional difference between ORIF and ORIF plus primary subtalar arthrodesis. Whether to fuse the subtalar joint up front in the highest-grade fractures - accepting motion loss to avoid a likely second operation - remains surgeon- and patient-specific rather than evidence-mandated.
Arthroscopic subtalar fusion reports union rates around 95% with less wound morbidity, but no RCT compares it with open fusion, and it is unsuitable for significant deformity requiring realignment or bone block. Open surgery remains the default where alignment must be corrected.
For calcaneal malunion with lost height and talar dorsiflexion, distraction bone-block arthrodesis restores hindfoot geometry but carries higher nonunion and wound risk than simple in-situ fusion. The threshold of height loss that justifies a bone block is not standardised.
Autograft, allograft, BMP and external/implanted bone stimulators are used to reduce nonunion, especially in revision or high-risk (smoker, diabetic) patients, but high-level evidence specific to subtalar fusion is lacking and use is largely extrapolated.
MCQ Practice Points
Q: What is the gold standard diagnostic test to confirm subtalar joint as pain source before surgery? A: Fluoroscopy-guided subtalar injection with local anesthetic. Greater than 75% pain relief confirms the subtalar joint as the primary pain generator and validates surgical planning.
Q: Which radiographic view best visualizes the posterior facet of the subtalar joint? A: Broden views - Foot in 40° pronation with 10°, 20°, 30°, 40° cephalad tube tilt. Provides tangential views of the posterior facet. Harris axial view shows calcaneal alignment.
Q: What is the expected fusion rate and pain relief after isolated subtalar arthrodesis? A: Fusion rate 90-95%, pain relief in 85-90% of patients. Higher success than triple arthrodesis for isolated disease. Adjacent joint motion is preserved (70-80% normal hindfoot motion).
Q: What is the most significant modifiable risk factor for nonunion after subtalar arthrodesis? A: Smoking - Roughly triples nonunion risk after hindfoot/ankle fusion (pooled OR around 2.9, 95% CI 1.2-6.8). Documented cessation counselling at least 6 weeks preoperatively is standard of care.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old male presents with chronic lateral hindfoot pain 3 years after a fall from height resulting in a displaced intra-articular calcaneal fracture treated non-operatively. He has trialed orthotics, NSAIDs, and one corticosteroid injection with temporary relief. CT scan shows Grade 3 subtalar arthritis with joint space narrowing and subchondral sclerosis. Ankle and midfoot joints appear preserved. What is your assessment and management?”
“A 48-year-old female has lateral hindfoot pain. X-rays show mild subtalar joint space narrowing. She also has ankle pain. How do you differentiate the pain source and plan treatment?”
“A patient is 9 months post isolated subtalar arthrodesis with persistent pain and motion at the fusion site. CT shows nonunion with screw loosening. He is a smoker. How do you manage this?”
Key Anatomy
- Three facets: Anterior, Middle, Posterior (Posterior bears 70-80% load)
- Subtalar joint provides 20-30° inversion/eversion for uneven ground
- Sinus tarsi = space between talus and calcaneus laterally
- Sural nerve at risk with lateral approach - posterior to peroneals
Classification
- Posttraumatic = 70-80% (calcaneal fractures most common)
- Primary OA = 10-15% (rare in isolation)
- Inflammatory = 5-10% (rheumatoid, psoriatic, seronegative)
- Coalition-related = 5% (tarsal coalition with secondary changes)
Diagnosis and Treatment Algorithm
- Broden views = gold standard X-ray for posterior facet
- CT scan = assess severity, surgical planning, rule out adjacent joints
- Diagnostic injection = greater than 75% relief confirms source
- Conservative first = orthotics, NSAIDs, injection for 6+ months
- Isolated fusion = for isolated disease, preserves 70-80% hindfoot motion
- Triple fusion = if talonavicular or calcaneocuboid also involved
Surgical Pearls
- Sinus tarsi approach = lateral oblique incision 4-5cm
- Complete cartilage removal = critical for fusion success
- Two 7.0-7.3mm screws = standard fixation with compression
- Maintain 5° hindfoot valgus = prevent varus malunion
- Non-weight-bearing 6-8 weeks = protect fusion healing
Complications
- Nonunion = 5-10% (smoking roughly triples risk, OR ~2.9)
- Malunion = 3-5% (varus or valgus causes adjacent joint stress)
- Sural nerve injury = 2-5% (paresthesia common, permanent rare)
- Adjacent joint arthritis = 10-15% at 10 years (ankle, midfoot)
- Infection = 1-3% overall
Evidence Base and Key Studies
Arthroscopic Subtalar Arthrodesis for Subtalar Arthritis - Systematic Review
- Ten studies, 234 patients (240 feet) - posttraumatic arthritis the commonest indication
- Weighted mean fusion rate 95%, average time to fusion 10.2 weeks
- AOFAS hindfoot score improved from a weighted 47 pre-op to 80.7 post-op
- Nonunion and pain from prominent hardware were the most common complications
- Posterior approach trended toward better function; lateral approach toward higher union
Subtalar Distraction Bone-Block Arthrodesis for Calcaneal Malunion
- Prospective series of 31 patients with malunited calcaneal fractures (mean age 38.5y)
- No nonunions; one bone-block dislocation requiring revision and one soft-tissue infection
- AOFAS hindfoot score improved from 23.5 pre-op to 73.2 at mean 33-month follow-up
- Talocalcaneal height restored by ~62%, with normalised pedobarographic load transfer
- Degree of heel-height correction correlated with a normal heel loading pattern
ORIF vs ORIF plus Primary Subtalar Arthrodesis - Sanders IV RCT
- Randomised multicentre trial, 31 Sanders type IV displaced intra-articular calcaneal fractures
- ORIF (n=17) vs ORIF plus primary subtalar arthrodesis (n=14); 26 followed minimum 2 years
- No significant difference in SF-36, MFA, AOFAS hindfoot or VAS scores between groups
- AOFAS hindfoot 62.5 (ORIF) vs 65.8 (ORIF+PSTA), p=0.68
- Primary arthrodesis may avoid the need for delayed secondary subtalar fusion