Medial Calcaneus | FHL at Risk | Stable Reference
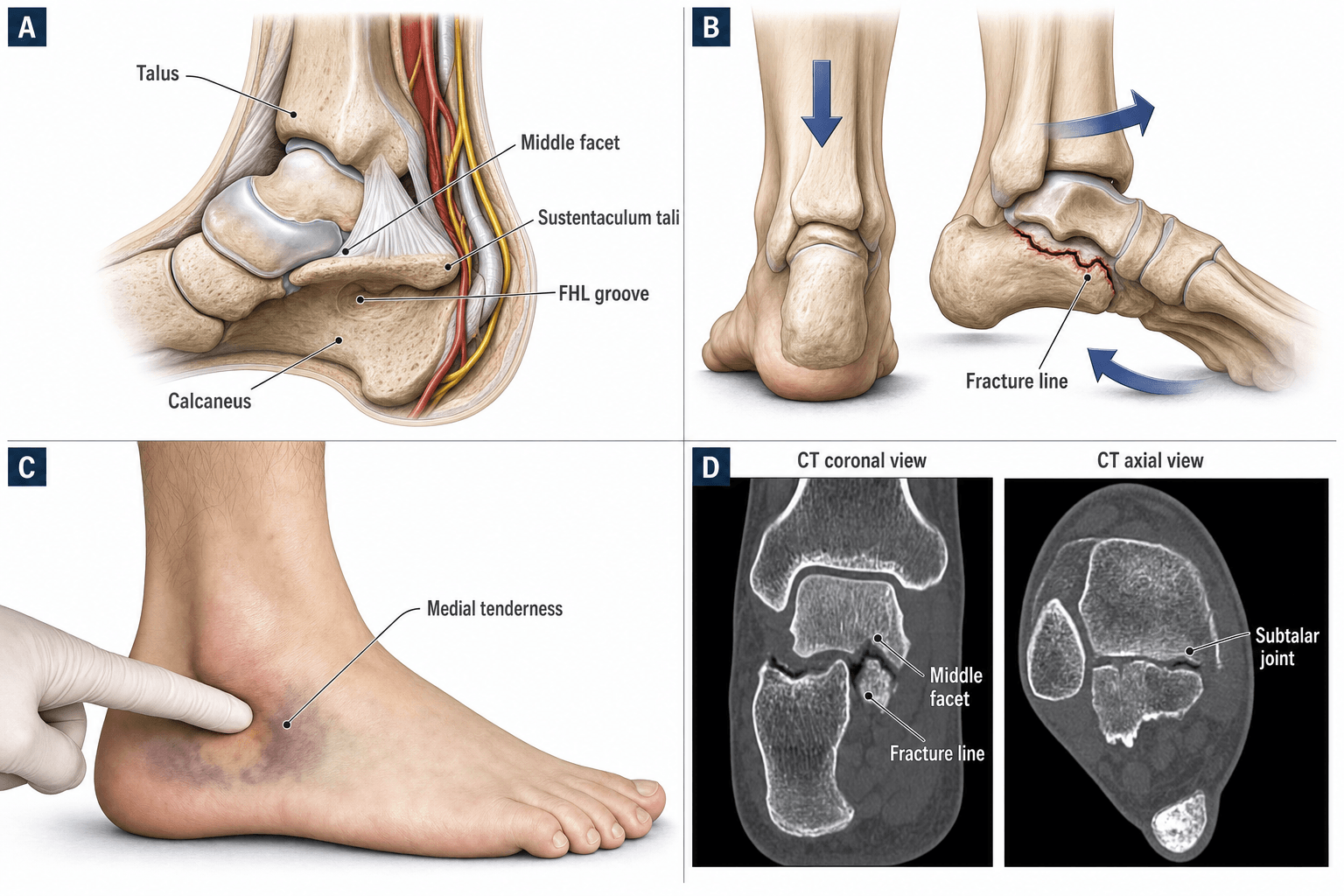
- Sustentaculum tali = medial shelf of calcaneus, attachment site for spring ligament and deltoid ligament
- FHL tendon at risk - Runs beneath sustentaculum, injury causes loss of great toe flexion
- Medial plantar nerve at risk - Runs medial to sustentaculum, injury causes medial foot numbness
- Stable reference for reduction - Sustentaculum usually stays attached to talus via interosseous ligament, serves as template for calcaneal fracture reduction
- ORIF if displaced - Prevents subtalar arthritis and FHL dysfunction
- “Sustentaculum tali = medial shelf, stable reference for calcaneal fracture reduction
- “FHL tendon runs beneath sustentaculum - at risk in medial approach
- “Medial plantar nerve at risk - runs medial to sustentaculum
- “ORIF if displaced - prevents subtalar arthritis
FHL (Flexor Hallucis Longus) tendon runs beneath sustentaculum tali - Injury causes loss of great toe flexion. Medial approach requires careful dissection to protect FHL. Medial plantar nerve also at risk.
Sustentaculum tali is stable reference for calcaneal fracture reduction - Usually stays attached to talus via interosseous ligament. Serves as template for reducing other calcaneal fragments. Critical in calcaneal fracture ORIF.
Medial plantar nerve at risk in medial approach - Runs medial to sustentaculum, between abductor hallucis and flexor digitorum brevis. Injury causes medial foot numbness and intrinsic muscle weakness.
Displacement greater than 2mm requires ORIF - Prevents subtalar arthritis and FHL dysfunction. Medial approach with protection of FHL and medial plantar nerve. Screw fixation from medial to lateral.
- Displacement
- Non-displaced, isolated
- Treatment
- Conservative (cast)
- Outcome
- 85-90% good results
- Displacement
- Displaced, isolated
- Treatment
- ORIF
- Outcome
- 80-85% good results
- Displacement
- Part of calcaneal fracture
- Treatment
- ORIF as part of calcaneal
- Outcome
- 75-85% good results
STABLEStable Reference
Hook:STABLE: Sustentaculum attached to Talus via interosseous ligament, Anatomic position, Bone reference, Ligament intact, Essential for calcaneal fracture reduction!
FMPStructures at Risk
Hook:FMP: FHL and Medial plantar nerve - Protect both in medial approach!
Overview and Epidemiology
Sustentaculum tali fractures are rare injuries involving the medial shelf of the calcaneus, which serves as a stable reference for calcaneal fracture reduction and has important structures (FHL tendon and medial plantar nerve) at risk during surgical approach.
Definition
Sustentaculum tali fracture: Fracture of the sustentaculum tali, which:
- Location: Medial shelf of calcaneus
- Function: Forms part of subtalar joint (middle facet)
- Attachment: Spring ligament and deltoid ligament
- Stability: Usually stays attached to talus via interosseous ligament
Sustentaculum tali anatomy:
- Medial shelf: Projects medially from calcaneus
- Subtalar joint: Forms middle facet (articulates with talus)
- FHL groove: FHL tendon runs beneath sustentaculum
- Stable reference: For calcaneal fracture reduction
Epidemiology
- Incidence: Less than 1% of calcaneus fractures
- Age: Peak 20-40 years (trauma population)
- Gender: No clear predominance
- Mechanism: High-energy trauma, inversion injury, or part of calcaneal fracture
- Associated injuries: Calcaneal fractures, ankle injuries
Sustentaculum tali is stable reference for calcaneal fracture reduction - Usually stays attached to talus via interosseous ligament. Serves as template for reducing other calcaneal fragments. Critical in calcaneal fracture ORIF.
Flexor Tendon Entrapment: an Absolute Operative Indication
Beneath and medial to the sustentaculum run the long flexors: the flexor hallucis longus (FHL) in its fibro-osseous groove directly on the undersurface of the shelf, and the flexor digitorum longus (FDL) passing more medially, superficial to the FHL. Either tendon can become incarcerated within a displaced sustentaculum fracture line - a complication the reference operative series (Dürr, Zwipp and Rammelt) lists explicitly, alongside articular incongruity, as a formal indication to operate.
Why entrapment changes the plan
- It blocks reduction. An interposed tendon acts as a soft-tissue block; the fragment cannot be seated congruently until the tendon is retrieved, so any closed or percutaneous attempt will fail.
- It abolishes active toe flexion. Incarceration of the FHL tethers the great-toe flexor and abolishes active hallux flexion; FDL entrapment does the same for the lesser toes. This is the mechanical basis for the classic "cannot flex the great toe" sign, and is far more often entrapment than a primary tendon rupture.
- It removes the millimetre debate. Because interposition both blocks reduction and disables the tendon, entrapment is an absolute operative indication whatever the amount of displacement - the usual step-off threshold simply does not apply.
Recognising and dealing with it
- Clinically: test active great-toe and lesser-toe flexion in every medial hindfoot injury; loss of hallux flexion after a fall demands scrutiny rather than reassurance.
- On CT: look for the tendon lying within the fracture gap and for a fragment that will not seat; MRI confirms tendon incarceration and distinguishes entrapment from rupture.
- Intra-operatively: through the direct medial approach, identify, retract and free the FHL (and FDL where involved) from the fracture before reduction, then reduce to the medial facet and cortical outline and fix with two small-fragment screws directed medial to lateral. A tendon left entrapped risks adhesion, a flexion contracture or clawing of the hallux, and late attritional rupture.
Loss of active great-toe flexion with a sustentaculum fracture is FHL entrapment until proven otherwise, not simply "FHL bruising." Entrapment of the FHL or FDL blocks reduction and is an absolute indication for open surgery whatever the displacement - free the tendon first, then reduce and fix.
Anatomy and Pathophysiology
Sustentaculum Tali Anatomy
Sustentaculum tali:
- Location: Medial shelf of calcaneus
- Size: 1-2cm projection medially
- Function: Forms part of subtalar joint (middle facet)
- Attachments: Spring ligament, deltoid ligament
Subtalar joint:
- Three facets: Anterior, middle (sustentaculum), posterior
- Sustentaculum: Middle facet, articulates with talus
- Function: Inversion/eversion, stability
FHL (Flexor Hallucis Longus) tendon:
- Course: Runs beneath sustentaculum tali
- Function: Flexes great toe
- Risk: At risk in medial approach
Medial plantar nerve:
- Location: Medial to sustentaculum
- Course: Between abductor hallucis and flexor digitorum brevis
- Function: Sensory to medial foot, motor to intrinsic muscles
- Risk: At risk in medial approach
Pathophysiology
Injury mechanism:
- High-energy trauma: Part of calcaneal fracture
- Inversion injury: Isolated sustentaculum fracture
- Direct trauma: To medial heel
Why sustentaculum is stable:
- Interosseous ligament: Attaches sustentaculum to talus
- Strong attachment: Ligament usually intact
- Template: Serves as reference for reduction
Why displacement matters:
- Subtalar joint: Sustentaculum is part of subtalar joint
- Articular surface: Displacement causes joint incongruity
- Arthritis risk: Malunion leads to subtalar arthritis
Classification Systems
Pattern-Based Classification
Type I (Non-displaced, isolated):
- Isolated sustentaculum fracture
- Non-displaced
- Treatment: Conservative (cast)
- Outcome: 85-90% good results
Type II (Displaced, isolated):
- Isolated sustentaculum fracture
- Displaced
- Treatment: ORIF
- Outcome: 80-85% good results
Type III (Part of calcaneal fracture):
- Sustentaculum fracture as part of calcaneal fracture
- Treatment: ORIF as part of calcaneal fixation
- Outcome: 75-85% good results
Pattern guides treatment approach.
Clinical Assessment
History
Symptoms:
- Medial heel pain: Pain on medial side of heel
- FHL dysfunction: Loss of great toe flexion (if FHL injured)
- Swelling: Localised to medial heel
- Difficulty weight bearing: Pain with weight bearing
Mechanism:
- High-energy trauma (calcaneal fracture)
- Inversion injury (isolated)
- Direct trauma to medial heel
Physical Examination
Inspection:
- Swelling on medial heel
- Ecchymosis (may be delayed)
- Deformity (rare)
Palpation:
- Tenderness over sustentaculum (medial to calcaneus)
- FHL dysfunction (loss of great toe flexion if injured)
- Subtalar joint tenderness
Range of Motion:
- Subtalar ROM limited and painful
- Great toe flexion limited (if FHL injured)
- Inversion/eversion painful
Special tests:
- FHL function: Test active great toe flexion
- Medial plantar nerve: Test sensation to medial foot
- Subtalar joint stress: Pain with inversion/eversion
FHL function and medial plantar nerve sensation are key findings - FHL runs beneath sustentaculum, injury causes loss of great toe flexion. Medial plantar nerve runs medial to sustentaculum, injury causes medial foot numbness.
Investigations
Standard X-ray Protocol
Lateral view:
- May show sustentaculum fracture
- Less reliable than CT
Axial view (Harris view):
- Shows sustentaculum from below
- Better view than lateral
AP view:
- May show fracture
- Less reliable
Key point: CT is often needed for diagnosis and planning.
Differential Diagnosis
Medial hindfoot pain after trauma is easily mislabelled as an ankle sprain. CT distinguishes a sustentaculum fracture from its mimics.
- Key clinical clue
- Tenderness 2 cm below medial malleolus, painful FHL excursion
- Best investigation
- CT (coronal/axial)
- Discriminator
- Fracture through medial calcaneal shelf and middle facet
- Key clinical clue
- Lateral or anterolateral subtalar tenderness
- Best investigation
- CT
- Discriminator
- Fracture line in talus, not calcaneus
- Key clinical clue
- Tenderness over medial malleolus, no bony point pain
- Best investigation
- MRI / stress views
- Discriminator
- Ligamentous signal, no cortical break
- Key clinical clue
- Pain along tendon, no acute high-energy mechanism
- Best investigation
- MRI / ultrasound
- Discriminator
- Tendon signal change, normal bone
- Key clinical clue
- Heel widening, reduced Bohler angle, marked swelling
- Best investigation
- Lateral X-ray + CT
- Discriminator
- Posterior facet depression on CT
- Key clinical clue
- Incidental, smooth corticated margin, often bilateral
- Best investigation
- CT / compare contralateral side
- Discriminator
- Smooth cortex, no oedema, asymptomatic
Up to a third of sustentaculum fractures are initially missed and treated as ankle sprains. Any patient with medial hindfoot point tenderness, an inability to actively flex the great toe, or pain on resisted hallux flexion after a fall or inversion injury needs CT - plain films are unreliable. A smooth, corticated, often bilateral os sustentaculi is a normal variant and must not be mistaken for an acute fracture.
Os Sustentaculi: the Sustentaculum-Specific Fracture Mimic
The single most important normal variant to separate from an acute sustentaculum fracture is the os sustentaculi, an accessory ossicle at the posterior margin of the sustentaculum tali. It arises from a secondary ossification centre that fails to fuse and is joined to the sustentaculum by a fibrocartilaginous synchondrosis. It is frequently bilateral - a feature that is itself a valuable clue.
- Os sustentaculi (variant)
- Smooth, rounded, well corticated on both sides
- Acute fracture
- Sharp, irregular, non-corticated lucency
- Os sustentaculi (variant)
- Absent
- Acute fracture
- Present, often with soft-tissue swelling
- Os sustentaculi (variant)
- Frequently bilateral - image the other foot
- Acute fracture
- Unilateral, matches the injured side
- Os sustentaculi (variant)
- Incidental, no high-energy history
- Acute fracture
- Point tenderness, lost hallux flexion after trauma
When the ossicle is the problem
An os sustentaculi is usually an asymptomatic incidental finding, but it is not always innocent. A painful synchondrosis - whether degenerate or disrupted by an acute injury - can itself generate medial subtalar pain that mimics a fracture, and the variant has been linked to symptomatic middle-facet subtalar pathology. The rule is therefore two-way: do not label a smooth, bilateral, non-oedematous ossicle as a fresh fracture, but equally do not dismiss persistent medial hindfoot pain in a patient who happens to have one - the junction can be the pain generator.
The os sustentaculi is a corticated, frequently bilateral accessory ossicle joined to the sustentaculum by a synchondrosis. Smooth cortication, absence of marrow oedema, and a matching appearance on the opposite foot separate it from an acute fracture, whose lucency is sharp, non-corticated, and surrounded by oedema. When medial hindfoot pain persists, remember the synchondrosis itself can be the source.
FHLSustentaculum Tali Features
Hook:FHL: Flexor Hallucis Longus - runs beneath sustentaculum, at risk in medial approach!
Management Algorithm
Management Pathway
Sustentaculum Tali Fracture Management
CT is usually required for diagnosis - sustentaculum fractures are difficult to see on X-ray alone. Assess displacement, fragment size, and FHL relationship. Part of calcaneal fracture or isolated.
If non-displaced (less than 2mm step-off) and isolated, conservative treatment with cast and non-weight bearing for 6-8 weeks. Success rate 85-90%.
If displaced (greater than 2mm) or part of calcaneal fracture, ORIF required. Medial approach with protection of FHL and medial plantar nerve. Screw fixation from medial to lateral. Success rate 80-85%.
If part of calcaneal fracture, address sustentaculum as part of calcaneal ORIF. Sustentaculum serves as stable reference for reduction. Fix with screws from lateral plate or medial screws. Success rate 75-85%.
Surgical Technique
Medial Approach ORIF (Isolated Fractures)
Indications:
- Isolated sustentaculum fracture
- Displaced (greater than 2mm)
Approach:
- Medial approach to calcaneus
- Expose sustentaculum
- Protect FHL and medial plantar nerve
Technique:
- Exposure: Medial approach, identify and protect FHL tendon (runs beneath sustentaculum)
- Protection: Identify and protect medial plantar nerve (runs medial to sustentaculum)
- Reduction: Anatomic reduction of sustentaculum to calcaneus
- Fixation: Screws (2.7-3.5mm) from medial to lateral
- Verification: Confirm reduction and hardware position fluoroscopically
Advantages:
- Direct access to sustentaculum
- Preserves subtalar joint
- Prevents arthritis
Medial approach for isolated fractures.
Complications
- Incidence
- 5-10%
- Risk Factors
- Medial approach
- Prevention/Management
- Protect FHL, identify early
- Incidence
- 5-10%
- Risk Factors
- Medial approach
- Prevention/Management
- Protect nerve, identify early
- Incidence
- 10-15%
- Risk Factors
- Malunion, displacement
- Prevention/Management
- Anatomic reduction, early treatment
- Incidence
- 5-10%
- Risk Factors
- Displacement, inadequate fixation
- Prevention/Management
- Rigid fixation, bone graft if needed
FHL Injury
5-10% incidence:
- Cause: Medial approach, FHL runs beneath sustentaculum
- Prevention: Identify and protect FHL tendon during approach
- Management: Repair if injured, may need FHL transfer if severe
Medial Plantar Nerve Injury
5-10% incidence:
- Cause: Medial approach, nerve runs medial to sustentaculum
- Prevention: Identify and protect medial plantar nerve during approach
- Management: Neuroma excision if symptomatic
Postoperative Care
Immediate Postoperative
- Immobilisation: Short leg cast or boot
- Weight bearing: Non-weight bearing (6-8 weeks)
- ROM: Ankle ROM after cast removal
- PT: Subtalar ROM and FHL strengthening
Rehabilitation Protocol
Weeks 0-6:
- Short leg cast, non-weight bearing
- Elevation to reduce swelling
- Ankle ROM exercises (if stable)
Weeks 6-8:
- Cast removal
- Transition to walking boot
- Progressive weight bearing
Weeks 8-12:
- Full weight bearing
- Progressive activity
- Return to sport (3-4 months)
Outcomes and Prognosis
Overall Outcomes
ORIF (isolated):
- Success rate: 80-85% (union, pain relief)
- Functional outcomes: 75-80% return to pre-injury level
- Subtalar arthritis: 10-15% develop arthritis
ORIF (part of calcaneal):
- Success rate: 75-85% (union, pain relief)
- Functional outcomes: 70-75% return to pre-injury level
- Subtalar arthritis: 15-20% develop arthritis
Conservative (non-displaced):
- Success rate: 85-90% (union, pain relief)
- Functional outcomes: 80-85% return to pre-injury level
- Subtalar arthritis: 5-10% develop arthritis
Long-Term Prognosis
Subtalar arthritis progression:
- With proper treatment: 10-15% develop subtalar arthritis
- Without treatment: 20-30% develop subtalar arthritis
- Risk factors: Displacement, malunion, delayed treatment
Guidelines, Registries & Global Practice
Global Epidemiology
- Rarity: Isolated sustentaculum tali fractures are reported globally as under 1% of all calcaneal fractures.
- Pattern: The sustentaculum is fractured in roughly a third (around 34 to 36%) of intra-articular calcaneal fractures, rising with Sanders grade.
- Demographics: Typically young-to-middle-aged adults (peak ~20 to 45 years) after a fall from height or road-traffic trauma; a male predominance mirrors the wider calcaneal-fracture population.
- Resource link: Incidence tracks high falls and motorcycle/road trauma, so the burden is proportionally higher in regions with high road-injury rates and occupational falls.
Guidelines and Society Positions — Side by Side
No orthopaedic society publishes a sustentaculum-specific guideline; practice is extrapolated from calcaneal-fracture and intra-articular fracture principles.
- Position relevant to this fracture
- Anatomical reduction of articular facets; sustentaculum is the reduction key for the calcaneus; defined screw corridors
- Practical takeaway
- Restore middle-facet congruity; capture the constant fragment
- Position relevant to this fracture
- Hindfoot/calcaneal injuries managed in centres with CT and foot-and-ankle expertise; soft-tissue-led timing
- Practical takeaway
- Image with CT, refer complex/associated injuries, respect soft tissues
- Position relevant to this fracture
- No dedicated guideline; emphasis on individualised, evidence-informed decision-making for calcaneal fractures
- Practical takeaway
- Selective surgery, shared decision-making
- Position relevant to this fracture
- Supports operative care for displaced articular incongruity in selected patients by experienced surgeons
- Practical takeaway
- Surgeon experience and patient selection drive outcome
Registry and Trial Evidence
- Registries: Arthroplasty/implant registries (NJR, AJRR, AOANJRR, Swedish/Norwegian) do not capture sustentaculum or calcaneal fracture fixation, so there is no implant-survival data for this injury - a point worth stating explicitly in a viva.
- Best trial evidence: The UK Heel Fracture Trial (Griffin, BMJ 2014) found no two-year functional advantage of ORIF over non-operative care for typical displaced intra-articular calcaneal fractures, with far higher complication and reoperation rates after surgery. It frames the global caution around routine calcaneal surgery but does not address isolated sustentaculum fractures, where middle-facet incongruity and tendon entrapment remain operative indications.
High- vs Limited-Resource Practice
- High-resource: Routine CT for diagnosis and planning, fluoroscopy-guided or open anatomical fixation, foot-and-ankle subspecialist input, structured rehabilitation.
- Limited-resource: CT may be unavailable, so missed diagnoses are commoner; non-displaced and many displaced fractures are managed in a cast with non-weight-bearing; percutaneous screw fixation is favoured over extensile approaches to limit wound and infection risk where soft-tissue and perioperative support are constrained.
A common viva topic. Know that the sustentaculum = medial shelf and the classic (but no longer absolute) reduction reference for the calcaneus; the FHL runs beneath it and the medial neurovascular bundle lies medial - both at risk in the medial approach. Operate for middle-facet incongruity or tendon entrapment rather than a single millimetre figure. Quote the verified fragment-specific outcomes (mean AOFAS ~83.6 after medial-approach screw fixation; intact vs fractured sustentaculum AOFAS 84.4 vs 74.3) and cite the UK Heel Trial to show command of the wider debate.
Controversies and Areas of Uncertainty
The evidence base is thin (small series, biomechanical and anatomical studies, no fracture-specific RCT), so several questions remain genuinely open.
The classic teaching that the sustentaculum reliably stays attached to the talus is challenged by modern CT series showing it is fractured in roughly a third of intra-articular calcaneal fractures and displaced ('inconstant') in up to 34.5%. Fragment width under about 20.5 mm, comminution and diabetes predict an unreliable fragment. The pragmatic position: verify constancy on CT before using it as your reduction reference.
The widely quoted 2 mm articular step-off is extrapolated from intra-articular fracture principles rather than proven for the sustentaculum specifically. Most authors operate for any incongruity of the middle facet, depression, an intra-articular line, or tendon entrapment - the displacement number alone is a guide, not a hard rule.
The direct medial approach gives controlled reduction and protects the FHL and neurovascular bundle under vision, but adds soft-tissue dissection. Fractures where the medial facet depresses as a single block can be reduced and fixed percutaneously. Choice is fragment- and surgeon-dependent; no comparative trial exists.
Isolated fractures are typically fixed medial-to-lateral through the medial window. When the sustentaculum is captured as part of a lateral calcaneal-plate construct, screws run lateral-to-medial along a narrow safe corridor. Both are accepted; the risk with lateral-to-medial screws is medial cortical perforation injuring the FHL and neurovascular structures.
Acknowledge the constant-fragment dogma, then show you know it is no longer absolute: modern CT data put sustentacular involvement at about a third of calcaneal fractures, and a narrow or comminuted fragment is an unreliable template. Operative indication is best stated as middle-facet incongruity or tendon entrapment rather than a single millimetre figure, and the wider calcaneal-fracture literature (UK Heel Trial) cautions against over-operating the surrounding joint-depression injury.
MCQ Practice Points
Q: What is the sustentaculum tali and why is it important in calcaneal fractures? A: Sustentaculum tali = medial shelf of calcaneus - Usually stays attached to talus via interosseous ligament, so it remains in anatomic position. Serves as stable reference for reducing other calcaneal fragments. Critical in calcaneal fracture ORIF.
Q: What structure is at risk beneath the sustentaculum tali? A: FHL (Flexor Hallucis Longus) tendon - Runs beneath sustentaculum. Injury causes loss of great toe flexion. Medial approach requires careful dissection to protect FHL. Injury occurs in 5-10% of medial approaches.
Q: What nerve is at risk medial to the sustentaculum tali? A: Medial plantar nerve - Runs medial to sustentaculum, between abductor hallucis and flexor digitorum brevis. Injury causes medial foot numbness and intrinsic muscle weakness. Protect during medial approach (5-10% injury rate).
Q: How is sustentaculum tali used in calcaneal fracture reduction? A: Serves as stable reference - Usually stays attached to talus via interosseous ligament, so remains in anatomic position. All other calcaneal fragments are reduced TO the sustentaculum. Posterior facet aligned to sustentaculum middle facet.
Q: When is ORIF required for sustentaculum tali fractures? A: Displacement greater than 2mm or part of calcaneal fracture - Prevents subtalar arthritis and FHL dysfunction. Medial approach with protection of FHL and medial plantar nerve. Screw fixation from medial to lateral. Success rate 80-85%.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old patient presents with medial heel pain after inversion injury. CT shows isolated displaced sustentaculum tali fracture with 3mm displacement. Clinical examination shows loss of great toe flexion (FHL dysfunction).”
“A 30-year-old patient has a displaced calcaneal fracture (Sanders Type II). The examiner asks you to explain how you use the sustentaculum tali in the reduction.”
“A 28-year-old fell from a ladder six weeks ago and was diagnosed with an ankle sprain. He returns with persistent medial heel pain and cannot actively flex his great toe. X-rays were reported as normal. How do you proceed, and what is the likely diagnosis?”
Key Concepts
- Sustentaculum tali = medial shelf of calcaneus
- Usually stays attached to talus via interosseous ligament
- Serves as stable reference for calcaneal fracture reduction
- FHL tendon runs beneath sustentaculum (at risk)
Classification
- Type I: Non-displaced, isolated - conservative (85-90% good results)
- Type II: Displaced, isolated - ORIF (80-85% good results)
- Type III: Part of calcaneal fracture - ORIF as part of calcaneal (75-85% good results)
- Classification guides treatment approach
Treatment
- Non-displaced, isolated: Conservative (cast, NWB 6-8 weeks)
- Displaced, isolated: ORIF via medial approach (80-85% good results)
- Part of calcaneal: ORIF as part of calcaneal fixation (75-85% good results)
- Displacement greater than 2mm: ORIF required
Surgical Technique
- Medial approach: Protect FHL (beneath sustentaculum) and medial plantar nerve (medial to sustentaculum)
- Screws: 2.7-3.5mm from medial to lateral
- Part of calcaneal: Use sustentaculum as stable reference, reduce other fragments to it
- Verify reduction fluoroscopically
Complications
- FHL injury: 5-10% (prevent by protecting FHL)
- Medial plantar nerve injury: 5-10% (prevent by protecting nerve)
- Subtalar arthritis: 10-15% if untreated, 10-15% with proper treatment
- Nonunion: 5-10% (prevent with rigid fixation)
Evidence Base
Every cited statistic below is taken directly from the linked paper. Where source data exists, fragment-specific outcome figures (AOFAS, Foot Function Index) are quoted rather than generic "80-85% good results" estimates. Sustentaculum tali fractures are rare, so the literature is dominated by small operative series, anatomical/biomechanical studies, and the broader calcaneal-fracture trial evidence.
Direct medial approach ORIF — the reference operative series
- 87% had additional foot/ankle fractures - rarely truly isolated
- Mean AOFAS 83.6, FFI 21.6 at 80 months after screw fixation
- Isolated fractures outperform those with associated injuries
- Look for lateral talar process (23%) and midtarsal (45%) injuries
Sustentaculum integrity predicts outcome in calcaneal fractures
- Sustentaculum fractured in 36% of intra-articular calcaneal fractures
- Higher Sanders grade = higher chance of sustentacular involvement
- Intact sustentaculum: AOFAS 84.4 vs 74.3 if fractured (p less than 0.001)
- The 'constant fragment' is not always constant
When is the sustentaculum NOT a constant fragment?
- Sustentaculum fragment 'inconstant' in 34.5% of calcaneal fractures
- Predictors: small width, comminution, intra-articular line, diabetes
- Cut-off fragment width 20.5 mm for inconstancy
- Verify the fragment on CT before using it as a template
Sustentaculum (constant-fragment) screw improves construct stability
- Sustentaculum screw reduces fracture-line displacement vs plate alone
- Lower peak stress in bone and implant with sustentacular screw
- More even stress distribution across the construct
- Supports routine 'constant-fragment' screw in Sanders II
Safe corridor for the sustentaculum screw — anatomical study
- Entry ~14 mm posterior, ~3 mm above lowest tarsal-sinus point
- Screw anteversion ~16 degrees (males) / ~15 degrees (females)
- Mean screw length ~41.6 mm
- A defined corridor reduces malposition and FHL/neurovascular risk
UK Heel Fracture Trial — operative vs non-operative calcaneal fractures
- No functional advantage of ORIF for typical displaced calcaneal fractures
- Complications/reoperations far higher with surgery (OR 7.5)
- Tempers enthusiasm for routine operative calcaneal fixation
- Reduction quality and patient selection matter more than the incision