PIPJ Hyperextension + DIPJ Flexion
- Characterized by PIPJ Hyperextension and DIPJ Flexion.
- Driven by dorsal subluxation of the lateral bands (opposite of Boutonniere).
- Can be Primary (Volar plate laxity/Intrinsic tightness) or Secondary (Mallet finger).
- Bunnell's Intrinsic Tightness Test discriminates Type I from Type II.
- Conservative management involves blocking PIPJ hyperextension (Figure-of-8 splint).
- Surgery ranges from soft tissue balancing (FDS tenodesis) to salvage (Fusion).
- “If the PIPJ is stiff, tenodesis will NOT work. You must release the contracture first.
- “In Mallet-induced Swan Neck, treating the DIPJ often corrects the PIPJ (if flexible).
- “Intrinsic tightness is defined as less PIP flexion when the MCP is extended vs flexed.
Intrinsic Tightness In Rheumatoid Arthritis, the intrinsic muscles often become fibrotic and tight. This pulls the lateral bands taut and hyper-extends the PIPJ. If you simply perform a capsulodesis or tenodesis without releasing the intrinsics, the deformity will recur or the finger will be stiff.
Bunnell's Test You MUST assess intrinsic tightness. Passive PIP flexion is checked with MCP Extended (tightens intrinsics) and MCP Flexed (relaxes intrinsics). If Flexion with Extended MCP is LESS than Flexion with Flexed MCP, the test is POSITIVE.

- PIPJ
- Hyperextended
- DIPJ
- Flexed
- Lateral Bands
- Dorsal Subluxed
- Volar Plate
- Lax/Ruptured
- PIPJ
- Flexed
- DIPJ
- Hyperextended
- Lateral Bands
- Volar Subluxed
- Volar Plate
- Normal/Contracted
- PIPJ
- Normal
- DIPJ
- Flexed
- Lateral Bands
- Normal
- Volar Plate
- Normal
- PIPJ
- Normal
- DIPJ
- Extended (cannot flex)
- Lateral Bands
- Normal
- Volar Plate
- Normal
DOVEPathomechanics
Hook:The Swan flies like a DOVE.
Overview
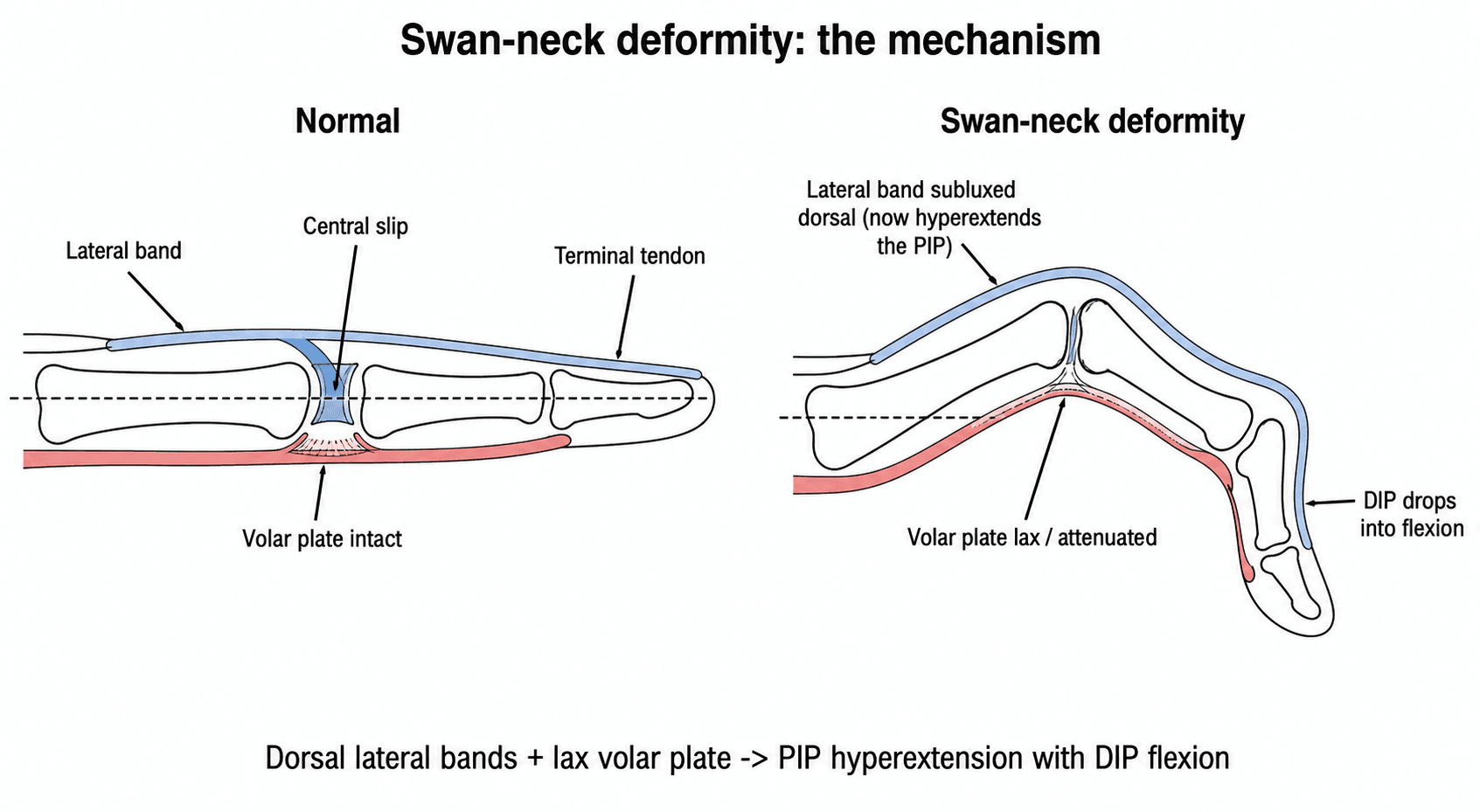
Swan Neck deformity consists of hyperextension of the PIPJ and reciprocal flexion of the DIPJ. It is caused by an imbalance where the extensor mechanism subluxates dorsally at the PIPJ.
It is the mechanical reverse of a Boutonniere deformity. Hyperextension of the PIPJ can only occur once the volar plate (the primary static restraint) becomes lax, ruptured or attenuated. When this happens, the lateral bands migrate dorsal to the axis of rotation of the PIPJ. Once dorsal, they function purely as PIPJ extensors and the joint becomes locked in hyperextension.
The reciprocal DIPJ flexion is the second half of the deformity. Because the extensor mechanism is now "tethered" proximally at the hyperextended PIPJ, the terminal tendon loses effective excursion and the unopposed pull of the flexor digitorum profundus (FDP) draws the DIPJ into flexion. The result is the classic zig-zag collapse: PIPJ hyperextension with DIPJ flexion. Crucially, the deformity is a mechanical imbalance, not a single structural failure, which is why successful treatment must restore balance (block PIPJ hyperextension and/or re-anchor the distal extensor) rather than simply releasing one structure.
Pathophysiology and Mechanisms
Extensor Apparatus
- Lateral Bands: Normally lie dorsal to the axis of rotation of the PIPJ (extensors).
- Transverse Retinacular Ligament: Prevents dorsal migration. In Swan Neck, this ligament stretches or fails.
- Triangular Ligament: Becomes tight / shortened.
The interplay of these ligaments creates the balance.
In the rheumatoid hand the swan neck is rarely an isolated PIPJ problem - it is one link in a zig-zag (concertina) collapse that the examiner wants you to trace:
- Wrist: radial deviation and carpal supination/collapse shift the load distally.
- MCP joint: synovitis stretches the radial sagittal band and leads to volar subluxation and ulnar drift; the intrinsics then shorten and pull the lateral bands.
- PIP joint: the tightened intrinsics plus a stretched volar plate produce PIPJ hyperextension - the swan neck - with reciprocal DIPJ flexion.
The practical rule is to correct the deformity proximal-to-distal: a swan-neck reconstruction done while leaving a subluxed, ulnar-drifted MCP joint uncorrected will recur, because the proximal driver is untreated. Address wrist and MCP malalignment (and systemic disease control) as part of the plan, not the PIPJ in isolation.
Classification Systems

Nalebuff Classification (Rheumatoid)
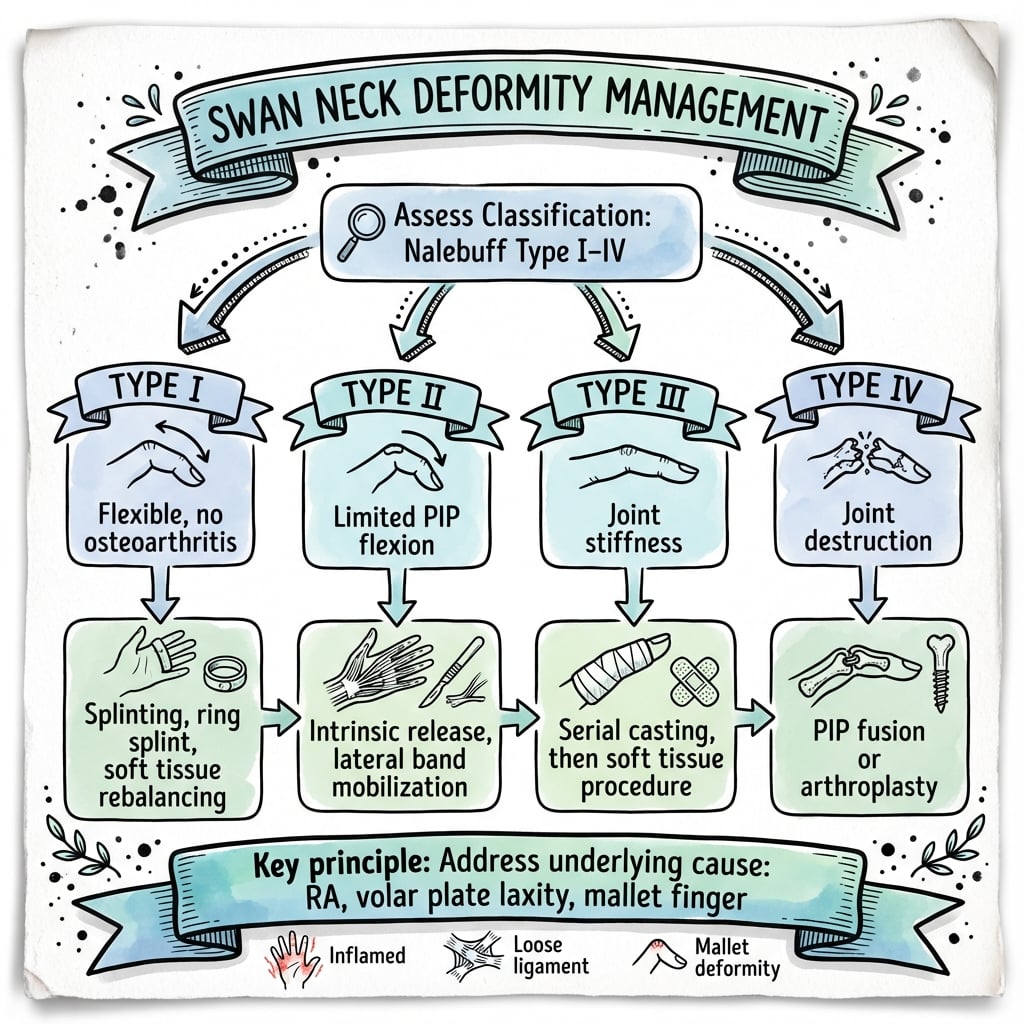
- Type I: PIPJ is flexible in all positions. No intrinsic tightness. Splinting and soft-tissue tenodesis are effective.
- Type II: PIPJ is flexible, but intrinsic tightness is present (Bunnell +ve). Requires intrinsic release before/with balancing.
- Type III: PIPJ flexion is limited (Stiff) but the joint surface is preserved. X-ray often normal. Mobilise first (serial casting, manipulation, capsulotomy).
- Type IV: PIPJ is stiff AND X-ray shows joint destruction. Salvage by arthrodesis or arthroplasty.
This classification guides treatment from splinting (I), release (II), mobilisation (III), to salvage (IV). The crucial division is flexible (I/II) — amenable to soft-tissue surgery — versus fixed (III/IV) — where soft-tissue procedures fail and the joint itself must be addressed.
- Typical Patient
- Older female, polyarticular
- Joint Erosion
- Yes (late)
- First-Line Treatment
- DMARD control + splint, then staged surgery
- Typical Patient
- Any age, prior DIP injury
- Joint Erosion
- No
- First-Line Treatment
- Treat the DIPJ (splint/fusion) first
- Typical Patient
- Young, spastic hand
- Joint Erosion
- No
- First-Line Treatment
- Tone management, selective release; guarded
- Typical Patient
- Female, non-erosive lupus
- Joint Erosion
- No (reducible)
- First-Line Treatment
- Conservative; reducible deformity
- Typical Patient
- Young, hyperextension injury
- Joint Erosion
- No
- First-Line Treatment
- Block hyperextension; tenodesis/SORL
FLIDNalebuff Classification
Hook:The lid (FLID) is on the deformity.
Clinical Assessment
Examination
- Deformity: Obvious PIP Hyperextension / DIP Flexion.
- Passive Correctability: Can you reduce the PIPJ easily? (Type I/II vs III).
- Impact: Does the finger initiate flexion? Locking?
- Mallet: Check if the DIPJ can extend passively.
Always document the passive range of motion.
Investigations
Radiology
- Views: AP and Lateral.
- Findings:
- Joint Space: Look for narrowing/erosions (Type IV).
- Alignment: Degree of hyperextension.
- Fracture: Mallet fracture at DIPJ?
Crucial to rule out joint destruction before offering soft tissue reconstruction.
Management Algorithm
Splinting (Type I)
- Device: Figure-of-8 Splint / Oval-8 / Silver Ring Splint.
- Mechanism: Blocks the last 10-20 degrees of extension (prevents hyperextension) but allows full flexion.
- Outcome: Highly effective for mobile deformities. Patients often wear silver rings permanently as jewelry.
Compliance is very high with silver rings compared to plastic.
Surgical Considerations
FDS Tenodesis (Swallow Tail)
- Indication: Type I (Mobile).
- Technique: One hemislip of the FDS tendon is divided proximally (in palm or P1).
- Routing: It is passed through the flexor sheath and anchored into P2 bone or looped.
- Effect: Creates a check-rein that prevents PIP hyperextension.
- Rehab: Dorsal block splint to protect the tenodesis.
The tenodesis must be tensioned with the PIPJ flexed 20-30 degrees.
The topic invokes the Fowler mechanism (a chronic mallet concentrating extensor force at the PIPJ) - the matching operation is the Fowler central slip tenotomy, which examiners expect you to name:
- Indication: a chronic mallet finger / mallet-driven (DIPJ) swan neck with a persistent DIPJ extensor lag and a supple PIPJ.
- Principle: divide the central slip (and the dorsal apparatus) over the proximal part of the middle phalanx. This releases the proximal tether so extensor force is transmitted distally to the terminal tendon, restoring active DIPJ extension and correcting the mallet/swan-neck imbalance.
- Caveat: a small (around 10 to 15 degree) PIPJ extensor lag is accepted, and a true boutonniere is the feared over-correction if too much is divided - so the PIPJ volar restraints must be competent.
It is a neat, joint-sparing alternative to DIPJ fusion when a chronic mallet is the driver.
SOFTSurgical Options
Hook:Keep the finger SOFT.
Complications
Surgical Complications
- Recurrence: Common in RA due to progressive disease; occurs in up to 30% at 5 years.
- Stiffness: Correction of hyperextension often results in loss of full flexion; trade-off between stability and motion.
- Infection: Increased risk with silicone implants or immunosuppressive RA medications.
- Tendon Rupture: FDS tenodesis can fail if tensioned too tightly or if manipulation is forceful.
- Implant Failure: Silicone arthroplasty fractures over time (7-10 year lifespan).
- Neuroma: Risk of digital nerve injury with lateral approaches.
- Flexion Contracture: Over-correction can limit extension; reported in 15% of tenodesis cases.
Careful patient selection and setting realistic expectations are essential.
Rehabilitation
- Splint: Dorsal block splint (prevents extension past 20 deg).
- Motion: Active flexion allowed.
- Wean: Start gentle active extension.
- Check: Ensure no recurrence of hyperextension "snap".
- Strength: Grip strengthening using putty and Theraputty exercises.
- Splint: Night splinting often continued for 3-6 months to prevent recurrence.
- Dexterity: Fine motor tasks (picking up coins, buttons, writing).
- Goals: Functional ROM (30-80 degrees) is better than Full ROM.
- Work Simulation: Occupation-specific tasks to prepare for return to work.
- Long-term Splinting: Silver ring splints worn permanently in some cases.
- Monitoring: Regular hand therapy reviews to detect recurrence early.
- Disease Control: In RA, coordination with rheumatology for DMARD optimisation.
Prognosis
Expected Outcomes by Treatment
- Splinting (Type I): Excellent functional outcomes; 80-90% symptom control with ring splints.
- FDS Tenodesis: Good results in 70-80%; some loss of full flexion expected (10-20 degrees).
- Intrinsic Release: Effective for Type II; may need combined with tenodesis.
- Fusion (Type III/IV): Reliable pain relief; functional position (30-45 degrees) preferred.
- Arthroplasty: Fair function for 7-10 years; silicone fracture is inevitable long-term.
Patient satisfaction depends on realistic expectations and appropriate procedure selection.
Guidelines, Registries & Global Practice
Global Epidemiology
- Rheumatoid arthritis is the dominant systemic cause of swan-neck deformity, with a global prevalence of roughly 0.5-1% of adults and a 2-3:1 female predominance; deformity risk rises with disease duration and inadequate disease control.
- Finger deformities (swan-neck, boutonniere, ulnar drift) develop in a substantial proportion of long-standing, poorly controlled RA, but their incidence has fallen markedly in the biologic/DMARD era.
- Non-rheumatoid causes are seen worldwide: post-traumatic (chronic mallet, volar plate injury), connective-tissue disease (SLE / Jaccoud arthropathy, Ehlers-Danlos with constitutional laxity), and neuromuscular spasticity (cerebral palsy, post-stroke).
Side-by-Side Guideline Positions (no level-1 surgical RCTs exist; principles are consensus-based)
- Emphasis
- Classification-driven management; non-operative splinting first for flexible deformity; arthrodesis for unstable/destroyed joints in high-demand hands
- Emphasis
- Treat the underlying mechanism (intrinsic vs joint vs distal mallet); hand therapy and ring splinting before surgery; staged reconstruction in multi-digit RA
- Emphasis
- Restore mechanical balance (block PIPJ hyperextension, re-establish distal anchor) rather than isolated release; protect repairs in dorsal-block splinting
- Emphasis
- Optimise systemic disease control (DMARD/biologic) before elective hand reconstruction to reduce recurrence
Registry & Evidence Notes
- No dedicated swan-neck registry exists; PIPJ implant arthroplasty data are captured within national arthroplasty/implant registries and small institutional series.
- Best comparative evidence is the splint crossover RCT (silver ring vs thermoplastic) showing equivalence, and medium-term tenodesis cohorts; surgical correction rests largely on Level IV evidence.
Disease Control as the Foundation
- In RA, the single most important determinant of long-term outcome is systemic disease activity; uncontrolled synovitis predicts recurrence after any reconstruction.
- Coordinated rheumatology, hand surgery and hand therapy input is the global standard of care.
High- vs Limited-Resource Practice Variation
- High-resource settings: early DMARD/biologic therapy, custom silver-ring or thermoplastic splints, specialist hand therapy, and selective soft-tissue reconstruction; deformity is increasingly prevented rather than corrected.
- Limited-resource settings: later presentation with fixed (Nalebuff III/IV) deformity is common; durable, low-maintenance solutions (figure-of-8 splints, arthrodesis) are favoured over implant arthroplasty where implants, imaging or revision capacity are scarce.
- Untreated trauma (chronic mallet progressing to secondary swan neck) remains a preventable cause where access to early hand care is limited.
Controversies & Areas of Uncertainty
Swan-neck management is built almost entirely on Level IV cohorts and expert opinion. There are no surgical RCTs and no head-to-head comparison of reconstruction techniques, so most "best procedure" debates remain unresolved.
- Tenodesis vs SORL vs intrinsic release: No comparative trial defines the superior soft-tissue procedure. Half-FDS tenodesis has the most supportive medium-term data; SORL reconstruction is elegant but prone to graft attenuation over time, particularly in rheumatoid tissue.
- Splint type: Often debated as silver-ring "superior" to thermoplastic, but the only RCT found them equivalent in dexterity gain. Choice should be driven by patient preference, comfort and cosmesis, not assumed superiority.
- Timing of surgery in RA: Whether to reconstruct flexible deformities early (before fixed contracture) or defer until function is clearly compromised is unsettled; aggressive early surgery risks stiffness, while delay risks progression to fixed Type III/IV disease.
- Multi-digit surgery: The trade-off between correcting several digits in one stage versus staging to protect against global hand stiffness has no trial evidence and remains a judgement call.
- Arthrodesis vs arthroplasty for the destroyed joint: Fusion gives reliable, durable stability for high-demand hands; pyrocarbon/silicone arthroplasty preserves motion but carries implant failure and revision concerns. The balance shifts with patient demand, digit involved and resource setting.
MCQ Practice Points
Q: What constitutes a positive Bunnell test? A: Decreased PIP flexion when the MCP joint is extended (vs flexed).
Q: Which ligament normally prevents dorsal subluxation of the lateral bands? A: Transverse Retinacular Ligament.
Q: In Nalebuff Type II, what is the defining feature? A: Intrinsic muscle tightness.
Q: What is the primary function of a Figure-of-8 splint in Swan Neck? A: To block PIP hyperextension while allowing flexion.
Q: What is the surgical treatment for Nalebuff Type II Swan Neck? A: Intrinsic release (Littler procedure) to address the underlying intrinsic muscle tightness.
Q: How does a Mallet finger cause Swan Neck deformity? A: Loss of the terminal tendon anchor causes proximal retraction of the extensor mechanism, concentrating extension force at the PIPJ.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 60-year-old with RA has Swan Neck deformities in fingers 3, 4, 5. She wants surgery because they 'lock'. What is your assessment?”
“A patient presents with a chronic Mallet finger and a secondary Swan Neck deformity. The PIPJ is flexible. How do you treat the Swan Neck?”
“A young carpenter had a hyperextension injury. Now has a fixed Swan Neck (Type III). X-ray is normal. He needs strength.”
“A 55-year-old woman with well-controlled rheumatoid arthritis presents with Swan Neck deformities in all fingers of her dominant hand. She is an artist and cannot hold a brush. Radiographs show preserved joint spaces. What is your approach?”
Classification (Nalebuff)
- Type I: Mobile
- Type II: Intrinsic Tight
- Type III: Stiff
- Type IV: Arthritis
Management
- Splint: Oval-8 / Ring
- Sx I: Tenodesis
- Sx II: Intrinsic Release
- Sx III/IV: Fusion
Mechanics
- Volar Plate Laxity
- Lateral Bands Dorsal
- Bunnell Test Positive
- Mallet drive
Evidence Base
Nalebuff Classification (Foundational Paper)
- Original paper grouping rheumatoid swan-neck deformities into four types based on PIPJ flexibility in different MCP positions plus radiographic joint status
- Defined a treatment algorithm matched to each type, from soft-tissue balancing to salvage arthrodesis
- Established intrinsic tightness as the discriminator between flexible types