Benign Synovial Cartilage Metaplasia | Multiple Loose Bodies | Usually Monoarticular
- Benign metaplasia of synovium producing multiple cartilage nodules that detach as loose bodies - usually a single large joint (knee most common)
- Primary (idiopathic, true metaplastic disease) vs secondary (loose bodies from OA, trauma, osteochondritis dissecans, Charcot)
- Milgram staging drives surgery: stage 1-2 need synovectomy because active synovium is the source of recurrence
- Radiographs show multiple similar-sized calcified loose bodies; ~1/3 are non-calcified and only seen on MRI/arthroscopy
- Malignant transformation to secondary chondrosarcoma in ~5% - suspect with rapid recurrence, symptom progression, or bone/marrow invasion
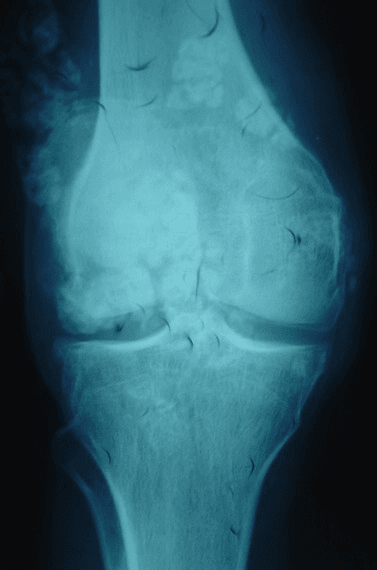
- “Classic radiograph: numerous loose bodies of roughly equal size with ring-and-arc ('popcorn') chondroid calcification
- “Non-calcified disease can be radiographically occult - a normal X-ray does NOT exclude it; image with MRI
- “Primary disease is monoarticular and the nodules are uniform; secondary disease has fewer, variably-sized bodies plus a clear underlying joint disorder
- “Recurrence after simple loose-body removal alone is common in stage 1-2; remove the diseased synovium
Primary synovial chondromatosis is a benign clonal metaplastic process of the synovium, not simply mechanical loose bodies. The active synovium continually generates new nodules - which is why loose-body removal alone (without synovectomy) frequently recurs in active (Milgram stage 1-2) disease.
Primary = idiopathic synovial metaplasia, monoarticular, uniform-sized bodies, otherwise healthy joint. Secondary = loose bodies generated by an underlying disorder (osteoarthritis, trauma, osteochondritis dissecans, neuropathic/Charcot joint) - fewer, variably-sized bodies with obvious background joint disease.
Roughly one third of cases have non-mineralised cartilage nodules that are invisible on plain radiographs. A normal X-ray does NOT exclude the diagnosis. MRI demonstrates the lobulated synovial masses and non-calcified bodies and defines extra-articular extension.
Secondary synovial chondrosarcoma develops in approximately 5%. Red flags: rapidly recurrent disease after adequate surgery, progressive symptoms over months, cortical/medullary bone invasion, and an enlarging dominant mass. Refer suspicious cases to a sarcoma unit.
Overview and Epidemiology
Synovial chondromatosis (also called synovial osteochondromatosis when the nodules ossify) is an uncommon benign disorder in which the synovial membrane of a joint, tendon sheath, or bursa undergoes cartilaginous metaplasia, forming multiple nodules that detach to become loose bodies. It is usually monoarticular, most often affects the knee, and presents with chronic pain, swelling, stiffness, and mechanical symptoms (locking, catching). Although benign, it can damage the joint over time and carries a small but real risk (~5%) of malignant transformation to secondary synovial chondrosarcoma.
- Age: Most present in the 3rd-5th decades (30-50 years)
- Sex: Male predominance, roughly 2:1 in most series
- Pattern: Almost always monoarticular
- Rarity: Uncommon; large joints of adults
- Knee: Most common (over 50% of cases)
- Hip, elbow, shoulder: Next most frequent large joints
- Ankle, wrist, TMJ: Less common but reported
- Over 30 anatomical sites described, including bursae and tendon sheaths
Primary versus Secondary
Primary synovial chondromatosis is a true idiopathic metaplastic/neoplastic disease of the synovium - the joint is otherwise normal, the disease is monoarticular, and the loose bodies are numerous and uniform in size.
Secondary synovial chondromatosis describes loose bodies generated by an underlying joint disorder - osteoarthritis, trauma/osteochondral fracture, osteochondritis dissecans, neuropathic (Charcot) joint, or osteonecrosis. Here the bodies are fewer and variable in size, and there is obvious background joint pathology. Distinguishing the two changes prognosis and counselling.
Pathophysiology and Pathology
Pathogenesis
In primary disease the synovial lining undergoes chondroid metaplasia, forming foci of hyaline cartilage within the subsynovial connective tissue. These cartilage nodules enlarge, may calcify and then ossify (synovial osteochondromatosis), and ultimately pedunculate and detach into the joint as loose bodies. Detached bodies survive by nutrient diffusion from synovial fluid and may continue to grow, sometimes coalescing into large lobulated masses. The process is now regarded as a benign clonal neoplastic condition rather than purely reactive, which explains its tendency to recur from residual active synovium.
- Metaplasia: Synovial connective tissue forms cartilage nodules
- Growth: Nodules enlarge within synovium (Milgram 1)
- Detachment: Nodules pedunculate and shed as loose bodies (Milgram 2)
- Quiescence: Synovium settles, free bodies remain (Milgram 3)
- Joint damage: Mechanical wear and secondary osteoarthritis
- Extra-articular spread: Through capsule/bursae in extensive disease
- Recurrence: From retained active synovium
- Malignant change: Secondary chondrosarcoma in approximately 5%
Gross and Histological Features
Pathology
Multiple pearly-white to bluish cartilage nodules, ranging from millimetres to centimetres, of broadly similar size in primary disease. Bodies may be embedded in synovium or lying free; calcified/ossified bodies feel gritty or bony.
Nodules of hyaline cartilage with chondrocytes arranged in clusters. Mild cytological atypia and binucleate cells can be present in benign disease - a known pitfall for over-diagnosing malignancy.
Enchondral ossification produces the osteochondromatosis variant; calcification gives the ring-and-arc radiographic pattern. Roughly one third remain non-mineralised.
Spindling at the periphery, sheets of cells losing the clustered (chondroid lobule) architecture, myxoid change, necrosis, and especially permeative bone/marrow invasion raise concern for secondary chondrosarcoma. Cellular atypia alone is unreliable.
Benign synovial chondromatosis can show mild chondrocyte atypia and binucleation that overlaps with low-grade chondrosarcoma. The most reliable discriminators of malignancy are architectural - loss of the clustered nodular pattern, sheet-like growth, myxoid matrix, necrosis, and invasion of bone/marrow - rather than cytology alone. This is why diagnosis on small biopsy is error-prone and suspicious cases belong in a sarcoma unit.
The Molecular Basis: FN1-ACVR2A and Why It Is 'Neoplastic'
The topic repeatedly calls primary synovial chondromatosis a "benign clonal neoplastic" process rather than a reactive one — here is the evidence behind that statement.
- It is clonal, not reactive. Cytogenetic and molecular studies show the metaplastic chondrocytes are a clonal population (chromosome-12 abnormalities have been reported), so the disease behaves like a true neoplasm — it regenerates from residual active synovium rather than simply resolving once a trigger is removed.
- The recurrent gene fusion. Primary synovial chondromatosis characteristically harbours a recurrent FN1-ACVR2A gene fusion (and its reciprocal ACVR2A-FN1), joining the fibronectin (FN1) promoter to the activin-receptor ACVR2A — a molecular hallmark confirming its neoplastic (not degenerative) nature.
- Why it matters clinically. This self-renewing, clonal biology is the molecular reason the topic keeps stressing synovectomy in active (Milgram 1-2) disease — leaving fusion-driven clonal synovium behind is what drives recurrence — and it frames progression to secondary chondrosarcoma as malignant transformation of an already-neoplastic lesion.
Q: Why is primary synovial chondromatosis called a neoplasm rather than a reactive/degenerative process? A: The metaplastic chondrocytes are clonal and carry a recurrent FN1-ACVR2A gene fusion — molecular proof it is a true (benign) neoplasm. This is why it regenerates from residual synovium (mandating synovectomy in Milgram 1-2 disease) and why ~5% can undergo malignant transformation to secondary chondrosarcoma.
Classification
- Metaplasia within synovium, no loose bodies
- Synovium is the entire disease
- Active synovial disease plus free loose bodies
- Multiple free bodies, synovium quiescent
- Stage 1-2: The synovium is still generating nodules - synovectomy is needed to reduce recurrence, in addition to removing any loose bodies.
- Stage 3: The synovium is inactive - loose-body removal may suffice, with lower recurrence.
- Staging is histological, but imaging and arthroscopic appearance help estimate activity pre-operatively.
Milgram staging is the classic exam framework because it directly links pathology to surgery: active synovium (stage 1-2) means do a synovectomy, quiescent disease (stage 3) means remove the bodies.
Clinical Presentation
- Chronic joint pain and swelling, often for years
- Stiffness and reduced range of motion
- Mechanical symptoms: locking, catching, clicking, giving way
- Insidious onset; often a long delay to diagnosis
- Effusion and diffuse synovial thickening/fullness
- Palpable loose bodies that move ("joint mice")
- Crepitus and restricted motion
- Mass effect / nerve compression in extra-articular extension (e.g. ulnar nerve at elbow, peri-articular masses)
A young-to-middle-aged adult (often male) with months-to-years of one swollen, painful, occasionally locking knee and radiographs showing multiple similar-sized calcified loose bodies is the textbook presentation. If the X-ray is normal but symptoms persist, get an MRI - non-calcified disease is radiographically silent.
Extra-Articular Disease: Tenosynovial and Bursal Chondromatosis
The overview notes the synovium of a "tendon sheath or bursa" can be involved and that over 30 sites are described — the extra-articular (para-articular) variant behaves differently enough to be worth separating.
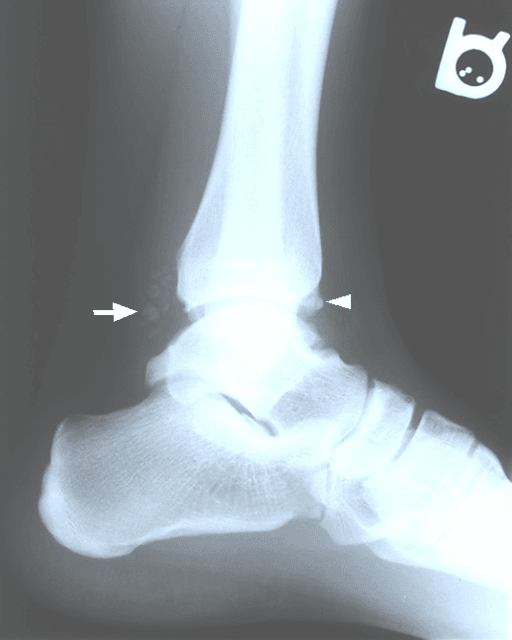
- The extra-articular counterpart. The same cartilaginous metaplasia can arise in the synovium of a tendon sheath (tenosynovial chondromatosis) or a bursa (bursal chondromatosis) rather than inside a joint — most often in the hand, wrist, foot and ankle.
- A mass, not a locking joint. Instead of the intra-articular story of effusion and mechanical locking, extra-articular disease presents as a firm, slowly-growing para-articular soft-tissue mass (with calcified nodules on imaging), which can erode adjacent bone by pressure and, near the elbow or wrist, compress a nerve.
- Diagnosis and treatment. MRI shows lobulated cartilage-signal nodules within the sheath or bursa; treatment is excision of the involved tenosynovium/bursa together with the nodules (the sheath equivalent of a joint synovectomy), and — as intra-articularly — incomplete excision recurs.
- Do not mistake it for its neighbours. In the hand or finger a nodular tendon-sheath lesion is more often a giant cell tumour of the tendon sheath (developed in its own topic); tenosynovial chondromatosis is distinguished by its chondroid (ring-and-arc) calcification and cartilage-signal nodules.
Q: A firm, slowly-enlarging soft-tissue mass over the wrist/hand tendons shows lobulated calcified nodules - what is it and how is it treated? A: Extra-articular (tenosynovial) synovial chondromatosis - the tendon-sheath/bursa counterpart of the joint disease, presenting as a para-articular mass (which can erode bone or compress a nerve) rather than a locking joint. Treat by excising the involved sheath/bursa with the nodules; distinguish it from a giant cell tumour of the tendon sheath by its chondroid ring-and-arc calcification.
Investigations
Plain Radiographs
- Multiple intra-articular calcified/ossified bodies of broadly similar size, classically with ring-and-arc ("popcorn") chondroid calcification.
- Preserved or only mildly narrowed joint space in primary disease (versus the marked changes of secondary OA-related disease).
- Pressure erosion of adjacent bone may occur in long-standing/extensive disease.
- Up to one third are non-calcified and therefore radiographically occult - a normal film does not exclude the diagnosis.
Because non-mineralised cartilage is invisible on plain films, persistent monoarticular symptoms with a normal radiograph still warrant MRI. Many cases are missed on X-ray alone.

Differential Diagnosis
- Key Distinguishing Features
- Monoarticular, numerous uniform bodies, otherwise normal joint
- Imaging Clues
- Ring-and-arc calcified bodies; lobulated synovial cartilage on MRI
- Key Distinguishing Features
- Fewer, variable-sized bodies with obvious background joint disease
- Imaging Clues
- Joint-space loss, osteophytes, donor defect (OCD)
- Key Distinguishing Features
- Hemosiderin-laden proliferative synovitis, recurrent haemarthrosis
- Imaging Clues
- Low T1 and T2 signal with GRE 'blooming' (no cartilage bodies)
- Key Distinguishing Features
- Rapid recurrence, progressive pain, dominant enlarging mass
- Imaging Clues
- Cortical/medullary bone invasion, soft-tissue extension
- Key Distinguishing Features
- Numerous tiny fibrinous bodies, inflammatory background
- Imaging Clues
- Small uniform low-signal bodies, no chondroid calcification
The pivotal exam distinction is benign synovial chondromatosis versus secondary synovial chondrosarcoma - aggressive bone invasion and rapid recurrence point to malignancy.
Management
Treatment Principles
Goal: relieve mechanical symptoms, remove loose bodies, address the active synovium when present, and protect the joint - while remaining alert to malignant transformation.
- Stage 3 (quiescent): removal of loose bodies may be sufficient.
- Stage 1-2 (active): add synovectomy to remove the source of recurrence.
- Extent and location (intra- vs extra-articular, accessibility) determine arthroscopic vs open approach.
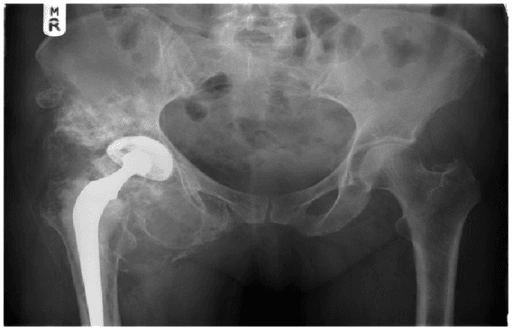
- End-stage joint destruction: consider arthroplasty in appropriate joints (e.g. hip) once disease is controlled.
- Suspected malignancy: refer to a sarcoma unit for staging and oncological resection.
Recurrence after simple loose-body removal in active (Milgram 1-2) disease is well recognised because the synovium keeps producing nodules. Removing the diseased synovium is the rationale for synovectomy in active disease.
Complications
- Recurrence (residual active synovium)
- Secondary osteoarthritis from chronic mechanical damage
- Joint destruction / deformity in advanced disease
- Nerve compression from extra-articular masses (e.g. ulnar nerve at the elbow)
- Secondary synovial chondrosarcoma in approximately 5%
- Typically arises many years after onset, after one or more recurrences
- Worse prognosis than conventional chondrosarcoma (intra-articular site, delayed diagnosis)
- May require wide resection or amputation
Guidelines, Registries and Global Practice
- The WHO Classification of Soft Tissue and Bone Tumours lists synovial chondromatosis among benign chondrogenic tumours and recognises rare malignant transformation.
- Milgram staging is the internationally used histological framework linking activity to surgical strategy.
- MRI is the consensus cross-sectional modality worldwide for non-calcified disease and extent mapping.
- Arthroscopic synovectomy is increasingly favoured in well-resourced centres for accessible joints; open surgery remains standard for extensive or deep disease.
- In resource-limited settings, plain radiographs and open surgery predominate; non-calcified disease may be under-diagnosed without MRI access.
- Suspected malignant transformation is managed within sarcoma referral networks (e.g. national bone and soft-tissue tumour services) rather than locally.
Wherever you practise, the principles are constant: stage by Milgram, image with MRI when non-calcified disease is suspected, remove the active synovium to limit recurrence, and escalate rapidly changing or bone-invading disease to a sarcoma service. Exact surgical access (arthroscopic vs open) varies with resources and disease extent, not with geography.
Memory Aids
123Milgram Staging
Hook:Count up 1-2-3: synovium alone, then synovium plus bodies, then bodies alone. Stage tells you whether you must do a synovectomy.
CHONDROFeatures of Primary Disease
Hook:CHONDRO - cartilage nodules in one joint that detach, recur, and rarely turn malignant.
RAPIDRed Flags for Malignant Transformation
Hook:RAPID change in a long-standing 'benign' joint = think secondary chondrosarcoma and refer.
Exam Day Cheat Sheet
Core Concept
- Benign cartilaginous metaplasia of synovium producing multiple loose bodies
- Usually monoarticular; knee is the most common joint (over 50%)
- Primary (idiopathic, uniform bodies, normal joint) vs secondary (underlying OA/trauma/OCD, variable bodies)
- Now regarded as a benign clonal neoplastic process, not purely reactive
Milgram Staging (drives surgery)
- Stage 1: active synovium, NO loose bodies - synovectomy
- Stage 2: active synovium PLUS loose bodies - synovectomy + body removal
- Stage 3: free bodies, synovium quiescent - loose-body removal may suffice
- Active disease (1-2) recurs if synovium is left behind
Imaging
- X-ray: multiple similar-sized calcified bodies, ring-and-arc ('popcorn') calcification, preserved space
- About one third are non-calcified and X-ray occult - normal film does NOT exclude
- MRI: investigation of choice; lobulated cartilage-signal bodies in thickened synovium; maps extent
- CT best for calcified bodies and cortical erosion
Management
- Arthroscopic synovectomy + loose-body removal when accessible (low recurrence in selected cases)
- Open arthrotomy for large bodies, extra-articular extension, or inaccessible recesses
- Arthroplasty for end-stage secondary OA (e.g. hip)
- Suspected malignancy: stage and refer to a sarcoma unit
Malignant Transformation (~5%)
- Secondary synovial chondrosarcoma, typically ~a decade later, often after recurrence
- Red flags: rapid recurrence, progressive pain, enlarging dominant mass, bone/marrow invasion
- Atypia alone is unreliable - judge by clinical course and architecture
- Wide resection at a sarcoma centre; historically high amputation rates, guarded prognosis
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old man presents with a 2-year history of a swollen, intermittently painful right knee with episodes of locking and catching. Radiographs show multiple rounded calcified bodies of similar size around the knee with a relatively preserved joint space. How do you make the diagnosis and what is your management?”
“A 40-year-old woman has a chronically swollen, occasionally catching knee, but her plain radiographs are reported as normal. How do you proceed and what conditions are you considering?”
“A 58-year-old patient previously treated with open synovectomy for hip synovial chondromatosis returns within months with worsening pain, a rapidly enlarging mass, and a radiograph showing cortical bone destruction. How do you manage this?”
Evidence Base
Malignant Transformation of Synovial Chondromatosis: Systematic Review
- Systematic review identified 48 cases of secondary synovial chondrosarcoma reported since 1957
- Pathognomonic signs (such as intramedullary infiltration) were present in only a minority - infiltration in 43%
- Progression of symptoms, rapid local recurrence after complete resection, and muscle infiltration were more suggestive of malignancy than atypia
- Biopsy and partial resection were prone to diagnostic error; tumour size is a strong indicator of malignancy
Synovial Chondrosarcoma: Systematic Review of Outcomes
- 67 cases of synovial chondrosarcoma pooled; most arose as transformation of pre-existing synovial chondromatosis
- Mean age 56.9 years; knee most affected (47.7%), then hip (34.3%)
- Mean time to malignant transformation was 11.2 years; local recurrence rate 28.3%
- Surgery resulted in amputation in 59.7% of cases, reflecting difficult intra-articular tumours and diagnostic delay
Arthroscopic Management of Ankle Synovial Chondromatosis
- Systematic review of arthroscopic treatment of ankle synovial chondromatosis; 15 studies, 22 patients
- Cases were almost entirely Milgram stage III, treated with arthroscopic synovectomy plus loose-body excision
- Complication and recurrence rates after arthroscopic management were very low on available data
- Notes that malignant transformation to chondrosarcoma occurs in approximately 5% of cases overall
Primary Synovial Chondromatosis of the Hip: Cohort and Review
- Retrospective two-centre cohort of 15 cases of primary synovial chondromatosis of the hip over 15 years
- Mean age 36.5 years with a male preponderance and predominantly unilateral, insidious presentation
- MRI was the key cross-sectional modality for diagnosis and for assessing articular involvement
- Management ranged across observation, arthroscopic or open synovectomy, and hip arthroplasty; no malignant transformation in this cohort