AITFL + PITFL + IOL + ITL | External Rotation Mechanism | Subtle on Plain Films | Fix if Unstable
- External rotation is the primary mechanism - AITFL tears first, then IOL, then PITFL
- Clear space greater than 6mm on mortise view indicates instability
- Tibiofibular overlap less than 6mm (AP) or less than 1mm (mortise) suggests diastasis
- Clinical tests: squeeze test, external rotation stress test, Cotton test (fibular translation)
- Surgical fixation: position ankle in dorsiflexion and neutral rotation to avoid malreduction
- Screw vs suture button: both effective, suture button allows physiologic motion
- “High ankle sprain = syndesmotic injury requiring 2-3x longer recovery than lateral sprain
- “Always rule out syndesmotic injury in ankle fractures - Maisonneuve pattern has proximal fibula fracture
- “Squeeze test compresses tibia/fibula at mid-calf - reproduces pain at syndesmosis
- “External rotation stress view shows diastasis - compare to contralateral side
External rotation of the foot on a planted ankle is the key mechanism. This sequentially disrupts AITFL (first), interosseous ligament (second), and PITFL (last). Internal rotation injuries are rare and produce different patterns.
Clear space greater than 6mm on mortise view is the most reliable plain film sign of diastasis. Also check tibiofibular overlap: less than 6mm on AP or less than 1mm on mortise is abnormal. Need stress views if equivocal.
Squeeze test (compressing tibia and fibula at mid-calf) has the highest sensitivity for syndesmotic injury. Pain at the ankle (not at the squeeze site) indicates syndesmotic disruption. External rotation stress test is also highly specific.
Position the ankle in dorsiflexion during syndesmotic fixation. The talus is wider anteriorly - dorsiflexion locks the talus in the mortise and prevents over-compression. Check reduction on intraoperative fluoroscopy before fixation.
- Stability
- Stable on stress views
- Treatment
- Conservative: boot 2-4 weeks, progressive weight bearing
- Key Points
- Return to sport 6-8 weeks (longer than lateral sprain)
- Stability
- Latent instability
- Treatment
- Consider fixation if athletic demands high, otherwise trial conservative
- Key Points
- MRI can confirm extent of ligament injury
- Stability
- Unstable (West Point dislocation)
- Treatment
- Operative fixation mandatory
- Key Points
- 1-2 screws or suture button construct
- Stability
- Unstable if disrupted
- Treatment
- Fix fracture, then assess syndesmosis with Cotton test intraoperatively
- Key Points
- Fix if more than 2mm fibular translation or diastasis on stress
SCREWSCREW vs BUTTON Decision
Hook:SCREW highlights the traditional screw fixation approach and the need for removal
6126-1-2 Rule for Radiographic Assessment
Hook:Remember the critical measurements: 6-1-2 for clear space, overlap, and translation
Overview and Epidemiology
Syndesmotic instability, commonly called a high ankle sprain, refers to disruption of the ligamentous structures that bind the distal tibia and fibula together, allowing abnormal motion and widening (diastasis) of the ankle mortise.
- Accounts for 1-11% of all ankle sprains in the general population
- Much higher incidence in contact sports (American football, rugby, ice hockey)
- Present in 23% of operatively treated ankle fractures
- Associated with Maisonneuve fractures (proximal fibula fracture with syndesmotic disruption)
- Prolonged recovery: 8-12 weeks to return to sport vs 2-4 weeks for lateral ankle sprain
- High missed diagnosis rate: up to 20% initially missed on clinical examination
- Post-traumatic arthritis: even 1mm of malreduction increases contact pressures by 40%
- Chronic pain and instability if undertreated
The term "high ankle sprain" distinguishes syndesmotic injuries from the much more common lateral ankle sprain (ATFL/CFL). The syndesmotic ligaments are located above the ankle joint proper, between the tibia and fibula, rather than connecting the talus to the fibula (as in lateral sprains).
- External rotation of the foot relative to the leg (most common)
- Foot planted, body rotates over it
- Common in cutting sports, tackles, or getting foot caught in a hole
- Less commonly: hyperdorsiflexion or eversion
- AITFL (Anterior Inferior Tibiofibular Ligament) - tears first
- IOL (Interosseous Ligament) - distal extension of interosseous membrane
- PITFL (Posterior Inferior Tibiofibular Ligament) - strongest, tears last
- ITL (Inferior Transverse Ligament) - deep portion of PITFL
Anatomy and Biomechanics of the Syndesmosis
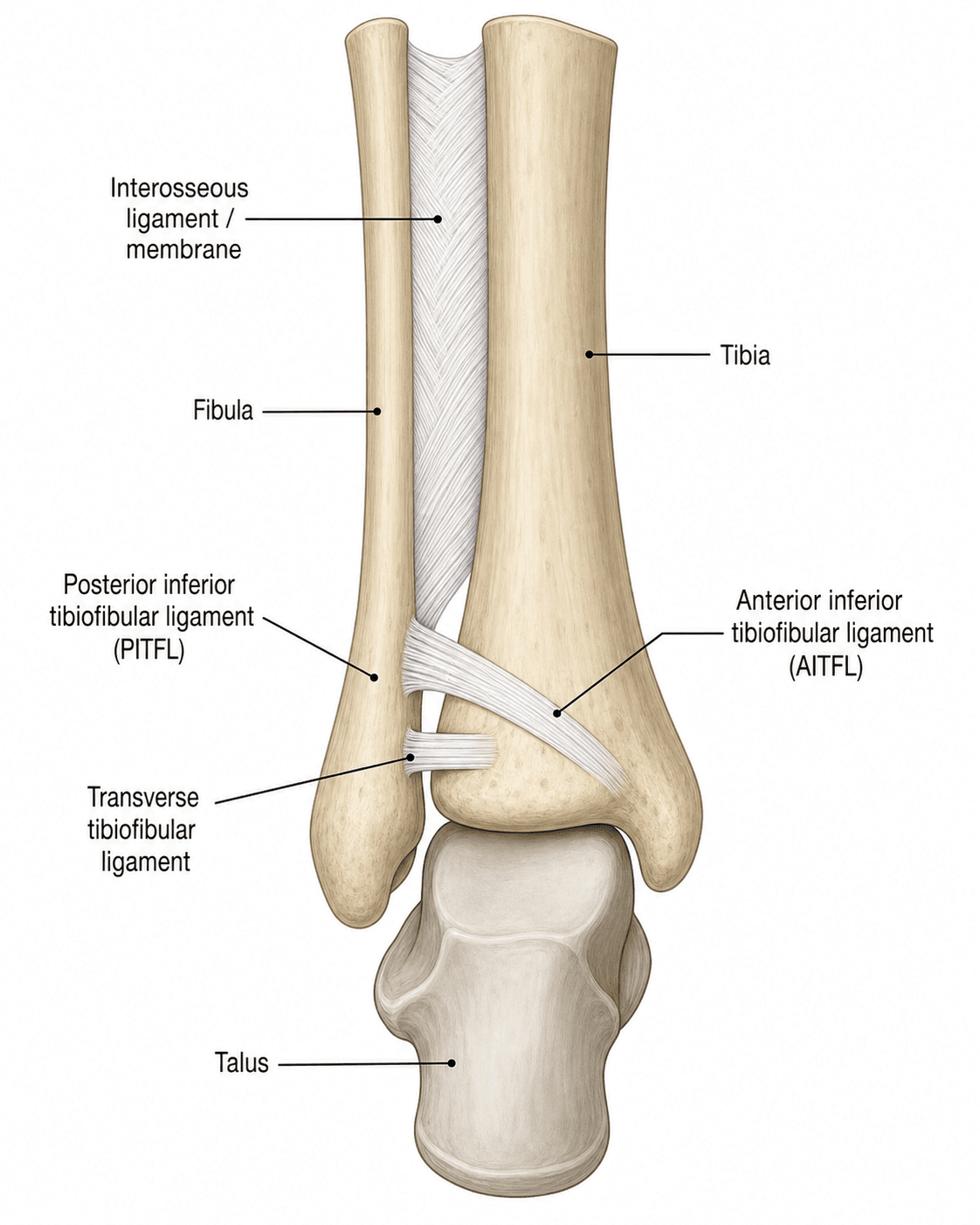
Syndesmotic ligament complex:
The distal tibiofibular joint (syndesmosis) is a fibrous joint stabilized by four primary ligament structures:
- Origin: anterior tubercle of tibia (Chaput tubercle)
- Insertion: anterior aspect of fibula
- Most commonly injured (tears first in external rotation)
- Oriented obliquely downward from tibia to fibula
- Provides 35% of syndesmotic stability
- Distal continuation of the interosseous membrane
- Provides 22% of syndesmotic stability
- Disrupts after AITFL in sequential injury pattern
- Origin: posterior tubercle of tibia (Volkmann tubercle)
- Insertion: posterior aspect of fibula
- Strongest component (42% of stability)
- Tears last in external rotation injuries
- Superficial and deep components
- Deep portion of PITFL
- Creates a labrum-like extension posteriorly
- Contacts the posterior talus
In external rotation injuries, the ligaments fail in a predictable sequence: AITFL first, then IOL, then PITFL. Complete syndesmotic disruption requires failure of all three. The PITFL is the strongest and is the key stabilizer - if intact, the syndesmosis is usually stable.
Biomechanics of the ankle mortise:
- Talar dome is wider anteriorly by 2-3mm
- During dorsiflexion, the wider anterior talus pushes the fibula laterally, causing physiologic widening (up to 1-2mm)
- The syndesmotic ligaments allow this normal physiologic motion while preventing excessive separation
- Contact area: syndesmotic ligaments contribute to tibiotalar contact mechanics
Functional anatomy:
Even 1mm of lateral fibular displacement increases tibiotalar contact pressures by 40% and significantly increases risk of post-traumatic arthritis. Anatomic reduction is essential - "close enough" is not acceptable for syndesmotic injuries.
- Fibular length: shortening of more than 2mm causes altered ankle biomechanics
- Fibular rotation: external rotation malreduction narrows the mortise posteriorly
- Syndesmotic width: must restore anatomic tibiofibular relationship
PITFALLPITFALL - Syndesmotic Ligament Anatomy
Hook:PITFALL reminds you of the ligaments (PITFL, IOL, AITFL) and the pitfalls of missing or undertreating syndesmotic injury
Pathophysiology
Injury mechanism and sequential failure:
Syndesmotic injuries occur through a predictable biomechanical sequence when external rotation force is applied to the foot while the leg is fixed:
Stage 1: AITFL disruption
- External rotation force first tensions the AITFL
- AITFL is relatively weaker than PITFL
- Partial or complete tear occurs depending on force magnitude
- Allows initial widening of anterior syndesmosis
Stage 2: Interosseous ligament failure
- Continued external rotation propagates injury proximally
- Interosseous ligament tears from distal to proximal
- May extend several centimeters up the interosseous membrane
- Creates potential space for fibular displacement
Stage 3: PITFL disruption
- PITFL is the strongest component (42% of stability)
- Last to fail in complete syndesmotic disruption
- May avulse with posterior malleolus fracture (Volkmann fragment)
- Complete disruption allows frank diastasis
- Normal tibiofibular clear space: 2-5mm
- Even 1mm lateral displacement of fibula reduces tibiotalar contact area by 42%
- Contact pressure increases by 40% with 1mm malreduction
- Creates asymmetric loading pattern on tibial plafond
- Loss of normal syndesmotic motion during dorsiflexion
- Fibula cannot translate laterally as talus widens anteriorly
- Abnormal talar position in mortise during gait cycle
- Increased shear stress on articular cartilage
- Chronic overload of medial or lateral tibial plafond
- Subchondral bone stress and microfracture
- Cartilage breakdown over months to years
- Post-traumatic osteoarthritis develops
Cadaver studies show that 1mm of lateral fibular displacement reduces tibiotalar contact area by 42% and increases peak contact pressure by 40%. This explains why anatomic reduction is essential - even small degrees of malreduction lead to accelerated arthritis.
Factors affecting healing:
- Ligament vascularity: syndesmotic ligaments have lower blood supply than lateral ankle ligaments
- Constant stress: weight bearing continuously stresses the healing syndesmosis
- Fibrous vs anatomic healing: without fixation, ligaments may heal in elongated position
- Scar tissue formation: interposition prevents anatomic healing
Classification Systems
West Point Ankle Grading System
This is the most commonly used classification for syndesmotic instability:
- Description
- Ligament disruption but no diastasis on static or stress films
- Stability
- Stable
- Treatment
- Conservative
- Description
- Diastasis only with stress testing, reduces spontaneously
- Stability
- Unstable
- Treatment
- Consider fixation (depends on activity level)
- Description
- Frank diastasis on static radiographs
- Stability
- Unstable
- Treatment
- Operative fixation mandatory
The West Point classification guides treatment. Latent injuries can be treated conservatively with protected weight bearing. Subluxation injuries may be managed conservatively in low-demand patients but often require fixation in athletes. Dislocation injuries always require operative fixation.
This classification is based on the clinical finding and assists in treatment decisions.
Clinical Presentation and Examination
- Mechanism: external rotation injury, twisting on planted foot, direct blow
- Pain location: anterior ankle, just above the joint line (compared to lateral ankle sprain which is more distal)
- Inability to bear weight immediately after injury
- Prolonged symptoms: pain lasting weeks (vs days for typical lateral sprain)
- High-energy mechanism
- Persistent pain despite treatment for "ankle sprain"
- Proximal fibular tenderness (Maisonneuve)
- Pain with ambulation more than 2 weeks post-injury
- Compress tibia and fibula together at mid-calf level
- Positive: pain at the ankle (distal syndesmosis), not at the compression site
- Sensitivity: 30-92%, Specificity: 88-95%
- Most sensitive clinical test for syndesmotic injury
- Stabilize leg, externally rotate foot with knee flexed to 90 degrees
- Positive: pain at anterior or posterior syndesmosis
- Sensitivity: 20-71%, Specificity: 85-97%
- Most specific clinical test
- Grasp calcaneus and talus, translate laterally
- Positive: greater than 2mm lateral shift of fibula relative to tibia
- More commonly performed intraoperatively under anesthesia
- Compares to contralateral side
- Dorsiflex ankle and apply external rotation force
- Positive: pain at syndesmosis
- May be difficult to perform acutely due to pain
No single clinical test is perfectly sensitive. If the mechanism and presentation suggest syndesmotic injury, proceed with imaging even if tests are negative. Combine clinical tests to improve diagnostic accuracy.
This section covers the examination findings used to assess syndesmotic stability.
- Distinguishing features
- Pain ABOVE the joint line over the anterior syndesmosis; positive squeeze and dorsiflexion-external rotation tests; prolonged recovery
- Key investigation
- Mortise/stress radiographs (clear space greater than 6mm), MRI
- Distinguishing features
- Pain and swelling distal/anterolateral over the lateral ligaments; anterior drawer positive; rapid recovery
- Key investigation
- Clinical; radiograph if Ottawa rules positive
- Distinguishing features
- Proximal fibular tenderness with medial-side injury; distal fibula may look normal
- Key investigation
- Full-length tibia-fibula radiographs; mortise view
- Distinguishing features
- Focal lateral malleolar bony tenderness and deformity
- Key investigation
- AP, mortise, lateral radiographs
- Distinguishing features
- Medial tenderness and widened medial clear space; often accompanies syndesmotic injury
- Key investigation
- Mortise view (medial clear space), stress views, MRI
- Distinguishing features
- Deep ankle pain, mechanical catching or effusion, often after an inversion injury
- Key investigation
- MRI or CT
- Distinguishing features
- Posterolateral pain behind the fibula, painful resisted eversion, snapping
- Key investigation
- Dynamic ultrasound or MRI
EXTERNALEXTERNAL - Mechanism and Clinical Assessment
Hook:EXTERNAL reminds you of the external rotation mechanism and the key assessment and treatment principles
Investigations and Imaging
Clinical Imaging Atlas


- Tibiofibular overlap: should be greater than 6mm
- Less than 6mm suggests diastasis
- Tibiofibular clear space: measure 1cm above plafond
- Greater than 6mm suggests instability
- Medial clear space: distance between medial malleolus and talus
- Should be equal to superior clear space (ankle joint space)
- Widening greater than 1mm compared to superior = deltoid injury
- Tibiofibular clear space: greater than 6mm abnormal
- Tibiofibular overlap: less than 1mm abnormal
- Talocrural angle: should be symmetric
- Assess for posterior malleolus fracture (associated with PITFL injury)
- Greater than 25% articular surface involvement may need fixation
On the mortise view, a tibiofibular clear space greater than 6mm is the most reliable plain radiograph sign of syndesmotic diastasis. Also check tibiofibular overlap: less than 6mm on AP or less than 1mm on mortise is abnormal.
Weight-bearing radiographs:
- May reveal diastasis not apparent on non-weight-bearing films
- Useful in chronic or subtle cases
Plain radiographs are the initial imaging modality and often diagnostic.
- Advantages
- Fast, low cost, readily available. Clear space and overlap measurements
- Limitations
- May miss latent instability
- Best Use
- Initial screening, frank diastasis
- Advantages
- Gold standard for latent instability. Bilateral comparison
- Limitations
- Requires contralateral views, can be painful
- Best Use
- Equivocal cases, isolated syndesmotic injury
- Advantages
- Visualizes ligaments, assesses associated injuries
- Limitations
- Expensive, longer acquisition time
- Best Use
- Chronic pain, pre-operative planning
- Advantages
- Excellent for bony detail, post-operative reduction assessment
- Limitations
- Radiation, poor soft tissue detail
- Best Use
- Posterior malleolus, assess reduction quality
Management Algorithm
- West Point latent (stable on stress testing)
- Isolated AITFL sprain without diastasis
- No associated fractures
- Patient can bear weight without significant pain
- RICE protocol: rest, ice, compression, elevation
- Controlled Ankle Motion (CAM) boot or below-knee cast
- Non-weight bearing initially, progress as tolerated
- NSAIDs for pain (short course to avoid delayed healing)
- Crutches until comfortable single-leg standing
- Progress to protected weight bearing in boot
- Begin gentle range of motion exercises
- Alphabet exercises
- Plantarflexion and dorsiflexion
- Avoid inversion/eversion initially
- Progressive resistance exercises
- Continue boot for 4-6 weeks total
- Wean from boot to lace-up ankle brace
- Proprioceptive training: balance exercises, single leg stance
- Strengthening: gastrocnemius, tibialis anterior, peroneals
- Sport-specific drills (if athlete)
- Gradual return to activity
- No pain with weight bearing or running
- Full range of motion compared to contralateral
- Single leg hop test 90% of contralateral
- Typically 8-12 weeks (2-3x longer than lateral ankle sprain)
High ankle sprains take significantly longer to heal than lateral ankle sprains because: (1) the syndesmotic ligaments are under constant stress with weight bearing; (2) the mortise must remain stable during dynamic activities; (3) incomplete healing leads to chronic instability and pain.
Follow-up radiographs at 2-4 weeks to ensure no delayed diastasis develops.
Surgical Technique
Traditional syndesmotic screw fixation:
Setup:
- Patient supine, bump under ipsilateral hip
- Thigh tourniquet (optional)
- Fluoroscopy available (AP, mortise, lateral views)
Step 1: Reduction of syndesmosis
- Ensure fibular length restored (if fracture present)
- Position ankle in dorsiflexion and neutral rotation
- Dorsiflexion widens anterior talus, preventing over-compression
- Apply reduction clamp from fibula to tibia
- Place clamp 2cm above joint line
- Apply gentle compression (avoid over-compression)
- Confirm reduction on fluoroscopy:
- AP: tibiofibular overlap greater than 6mm
- Mortise: clear space less than 6mm, overlap greater than 1mm
- Lateral: fibula centered in incisura
Step 2: Screw insertion
- Insert screw 2-3cm above tibial plafond
- Direction: 30 degrees anterior to posterior (parallel to joint line)
- Size: 3.5mm or 4.5mm cortical screw
- Drill perpendicular to long axis of fibula
- Purchase: 3 cortices (both fibular cortices + near tibial cortex) or 4 cortices (all four)
- 3 cortices: allows some motion, screw less likely to break
- 4 cortices: more rigid, higher breakage rate
- Do not lag the screw (use non-lag technique)
Step 3: Optional second screw
- Some surgeons place 2 screws for increased stability
- Second screw 1-2cm proximal to first
- Same trajectory and technique
Step 4: Confirm reduction
- Remove clamp
- Obtain final fluoroscopy images (AP, mortise, lateral)
- Ensure clear space, overlap, and fibular position anatomic
Screw removal:
- Remove at 8-12 weeks if non-bioabsorbable
- Prevents screw breakage with weight bearing
- Protected weight bearing until screw removed or bioabsorbable screw incorporated
Tricortical fixation (3 cortices) is increasingly favored because it provides adequate stability while allowing some physiologic motion and has a lower screw breakage rate. Quadricortical fixation is more rigid but requires screw removal before full weight bearing.
This is the traditional technique with proven long-term results.
Complications
- Over-compression of syndesmosis
- Fibular malposition (rotation, translation)
- Recognition: intraoperative fluoroscopy on multiple views
- Prevention: ankle in dorsiflexion, neutral rotation, gentle clamp application
- Screw placed too distal or wrong trajectory
- Recognition: pain, limited motion, radiographic signs
- Prevention: stay 2cm above plafond, confirm on lateral view
- Superficial peroneal nerve (at fibular incision site)
- Deep peroneal nerve or anterior tibial vessels (rare, with anterior approach)
- Prevention: careful dissection, knowledge of anatomy
- Incidence: 5-10% in ankle fracture surgery
- Risk factors: diabetes, smoking, soft tissue injury
- Prevention: delay surgery if blisters present, careful soft tissue handling
- If weight bearing too early with rigid fixation
- Usually asymptomatic if syndesmosis healed
- Prevention: protected weight bearing until screw removal or union
- Syndesmosis re-widens despite fixation
- May indicate inadequate fixation or continued instability
- Management: revision fixation if detected early
These complications can often be prevented with careful technique and appropriate post-operative protocols.
Postoperative Care and Rehabilitation
Post-operative protocol for screw fixation:
Phase 1: Protection (0-2 weeks)
- Splint or boot with non-weight bearing
- Elevate leg above heart level
- Ice for swelling control
- DVT prophylaxis if indicated
- Suture removal at 10-14 days
Phase 2: Early mobilization (2-6 weeks)
- Transition to CAM boot
- Non-weight bearing continues (if quadricortical screw)
- Partial weight bearing (if tricortical screw, some protocols)
- Begin gentle ROM exercises (plantarflexion/dorsiflexion)
- Avoid inversion/eversion
Phase 3: Screw removal and progressive loading (6-12 weeks)
- Screw removal at 8-12 weeks (if not bioabsorbable)
- After removal, progress to full weight bearing over 2 weeks
- Wean from boot to ankle brace
- ROM exercises progress to include inversion/eversion
- Begin strengthening exercises
Phase 4: Return to activity (12+ weeks)
- Progress strengthening
- Proprioceptive training: balance board, single leg exercises
- Sport-specific drills
- Gradual return to sport at 12-16 weeks post-screw removal
Total timeline: 20-28 weeks (5-7 months) from surgery to full sport
Screws are removed to prevent breakage and allow resumption of full activity. Screw breakage rate is 25-50% if left in place beyond 12 weeks with weight bearing. Broken screws are usually asymptomatic but can be difficult to remove later if needed.
This protocol protects the syndesmosis during ligament healing.
Prevention and Return to Sport
- Proprioceptive exercises in pre-season training
- Balance and agility drills
- Core and hip strengthening (improves lower extremity control)
- Prophylactic bracing in high-risk sports (football, basketball)
- Reduces incidence of ankle injuries by 30-50%
- Lace-up braces or high-top shoes provide lateral support
- Avoid holes, uneven surfaces
- Proper footwear for surface type
- Adequate warm-up before activity
- Gradual increase in training intensity
- Avoid fatigue (injury risk increases when fatigued)
- Pain-free: no pain with weight bearing, running, cutting
- ROM: full dorsiflexion (critical for push-off), equal to contralateral
- Strength: 90% of contralateral on single leg heel raise, hop test
- Functional testing: single leg hop greater than 90% of contralateral
- Radiographic stability: no diastasis on stress views
- Athlete confidence with cutting and jumping
- No apprehension or fear of re-injury
- Week 1: straight-line jogging (50% effort)
- Week 2: increased pace, longer distances (75% effort)
- Week 3: change of direction, cutting at 50% speed
- Week 4: sport-specific drills at increasing intensity
- Week 5: non-contact practice
- Week 6+: full contact practice, then return to competition
- Conservative treatment: 8-12 weeks
- Screw fixation: 20-28 weeks (including screw removal time)
- Suture button: 12-16 weeks
- Continue proprioceptive training indefinitely
- Use ankle brace for 6-12 months after return
- Maintain strength and conditioning
Athletes who return to sport before meeting objective criteria have a significantly higher re-injury rate. The prolonged recovery time for syndesmotic injuries is frustrating for athletes but essential for proper healing. Premature return leads to chronic instability.
Guidelines, Registries & Global Practice
Global epidemiology:
Syndesmotic injuries account for roughly 1-11% of all ankle sprains but are markedly over-represented in collision and cutting sports played worldwide (American football, rugby league and union, soccer, ice hockey and Australian Rules football). In the United States Military Academy cohort the syndesmosis was involved in a substantial minority of ankle sprains, and elite-football injury surveillance confirms a prolonged return-to-play burden relative to lateral sprains. According to PubMed, the JAAOS review by Hunt and colleagues emphasises that the historic paucity of high-level data has produced genuine practice variation in diagnosis and fixation choice across regions (DOI, PMID 26498585).
Side-by-side guidance:
- Diagnosis emphasis
- Stress testing and arthroscopy to grade isolated injuries; unstable injuries need stabilisation
- Fixation guidance
- Anatomic reduction is paramount; screw or dynamic fixation both acceptable
- Evidence level
- Expert consensus / Level V
- Diagnosis emphasis
- Mortise clear space and stress views; CT for reduction assessment
- Fixation guidance
- Trend toward dynamic (suture button) fixation; screw still standard, removal optional
- Evidence level
- Level I-II RCT/meta-analysis
- Diagnosis emphasis
- Restore fibular length and rotation first, then assess syndesmosis (Cotton/hook test)
- Fixation guidance
- Anatomic reduction under direct or CT control; avoid over-compression and malrotation
- Evidence level
- Principle-based / Level V
- Diagnosis emphasis
- Early senior assessment; CT where reduction is uncertain
- Fixation guidance
- Stabilise unstable syndesmosis; implant choice surgeon-led
- Evidence level
- Standard of care / Level V
- No national joint registry tracks syndesmotic implants specifically; the best comparative data come from RCTs and meta-analyses rather than registries
- Level I meta-analysis (Grassi et al., AJSM 2019) shows dynamic fixation reduces malreduction and reoperation versus screws (DOI, PMID 31188642)
- CT-based RCT evidence (Kortekangas et al., Injury 2015) shows dynamic constructs maintain reduction better at 2 years (DOI, PMID 25769201)
- Implant choice: screw fixation remains common globally for cost reasons; suture button uptake is higher in athletic and well-resourced centres
- Screw removal: routine removal practised in some centres, retain-until-symptomatic in others; evidence does not mandate routine removal
- Reduction assessment: increasing use of intraoperative or postoperative CT (vs plain films alone) where available
MCQ Practice Points
Answer: AITFL (Anterior Inferior Tibiofibular Ligament)
The sequential failure pattern is: AITFL → IOL → PITFL. The AITFL is relatively weaker and positioned anteriorly where it receives maximal tension during external rotation. The PITFL is the strongest component (42% of stability) and tears last.
Answer: Greater than 6mm
Harper and Keller (1989) established that a clear space greater than 6mm on mortise view has 100% sensitivity and 94% specificity for syndesmotic diastasis. This is measured 1cm above the tibial plafond on the mortise radiograph.
Answer: Maisonneuve fracture - YES, syndesmosis requires fixation
This is a Maisonneuve fracture pattern (Lauge-Hansen PER IV). The entire syndesmosis is disrupted from the proximal fibula fracture down to the ankle. The distal fibula appears intact but the syndesmotic ligaments are completely torn. Fix the medial malleolus, then perform Cotton test to confirm syndesmotic instability, then fix syndesmosis. Do NOT fix the proximal fibula fracture.
Answer: Dorsiflexion
The talus is wider anteriorly by 2-3mm. Positioning the ankle in dorsiflexion locks the wider anterior talus in the mortise, preventing over-compression of the syndesmosis. If the ankle is in plantarflexion during fixation, the narrower posterior talus allows over-compression, and when the patient dorsiflexes post-operatively, the ankle will be too tight.
Answer: Lateral fibular translation test - greater than 2mm requires fixation
The Cotton test assesses lateral translation of the fibula relative to the tibia. The examiner grasps the calcaneus and talus and translates laterally while palpating the fibula. Greater than 2mm of translation (compared to contralateral side) indicates syndesmotic instability requiring fixation. This is often performed intraoperatively under anesthesia after fibula or medial malleolus fixation.
Answer: Allows physiologic motion and faster return to sport (no removal needed)
Suture button (TightRope) allows 1-2mm of physiologic syndesmotic motion, permits earlier weight bearing and range of motion, and does not require removal. This translates to faster return to sport: 12-16 weeks vs 20-28 weeks with screw fixation. RCTs show equivalent functional outcomes but lower re-operation rate with suture button.
Answer: 40% increase in contact pressure
Biomechanical cadaver studies show that even 1mm of lateral fibular displacement reduces tibiotalar contact area by 42% and increases peak contact pressure by 40%. This explains the high rate of post-traumatic arthritis with malreduction and why anatomic reduction is essential.
Answer: Squeeze test (sensitivity 30-92%)
The squeeze test involves compressing the tibia and fibula together at mid-calf level. Pain at the ankle (not at the compression site) indicates syndesmotic disruption. It has the highest sensitivity of the clinical tests, though no single test is perfectly sensitive. External rotation stress test is more specific.
- AITFL tears first in external rotation injuries
- PITFL is the strongest component (42% of stability)
- Inferior transverse ligament is the deep portion of PITFL
- Sequential failure: AITFL → IOL → PITFL
- Squeeze test: most sensitive (compress at mid-calf, pain at ankle)
- External rotation stress test: most specific
- Cotton test: assess lateral fibular translation (greater than 2mm = unstable)
- All tests should be compared to contralateral side
- Clear space greater than 6mm on mortise view = diastasis
- Tibiofibular overlap less than 6mm on AP or less than 1mm on mortise = abnormal
- Medial clear space should equal superior clear space
- Stress views needed if static films equivocal
- West Point: latent (stable), subluxation (unstable with stress), dislocation (frank diastasis)
- Maisonneuve: PER IV injury - proximal fibula fracture + complete syndesmotic disruption
- Position ankle in dorsiflexion and neutral rotation during fixation
- Screw placed 2-3cm above plafond, 30 degrees anterior to posterior
- Tricortical vs quadricortical: both effective, tricortical lower breakage rate
- Suture button allows physiologic motion and faster return to sport
- 1mm malreduction increases contact pressure by 40%
- Screw vs suture button: equivalent outcomes, suture button faster return to sport
- Return to sport: 8-12 weeks conservative, 12-16 weeks suture button, 20-28 weeks screw
- Arthritis risk 10-30% at 5-10 years, higher with malreduction
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old male rugby player presents 3 days after sustaining an external rotation injury to his ankle during a tackle. He describes immediate pain above the ankle joint and difficulty bearing weight. Ottawa ankle rules applied - radiographs show no fracture. Squeeze test is positive. Mortise view shows clear space of 5.5mm. External rotation stress views show clear space widening to 7mm, with 2mm difference compared to contralateral side. What is your diagnosis and management?”
“A 35-year-old female presents with an ankle injury after a fall. She has swelling and tenderness over the medial malleolus and proximal fibula. Ankle radiographs show a medial malleolus fracture and widened medial clear space, but the fibula appears intact distally. Proximal tibia-fibula radiographs show a proximal fibula fracture. What is your diagnosis and surgical plan?”
“You are asked to review a patient in clinic 2 weeks after syndesmotic screw fixation for an ankle fracture. The patient reports persistent pain and difficulty mobilizing. You obtain radiographs and notice the tibiofibular clear space is 7mm on the mortise view. What is your assessment and management?”
Key Anatomy
- AITFL: tears first, 35% of stability
- IOL: interosseous ligament, 22% stability
- PITFL: strongest, 42% stability, tears last
- ITL: deep PITFL, labrum-like function
- Sequential failure: AITFL → IOL → PITFL
Mechanism and Epidemiology
- External rotation of foot on planted ankle
- 1-11% of all ankle sprains, 23% of ankle fractures
- Common in contact sports: rugby, AFL, football
- Maisonneuve: proximal fibula fracture + complete syndesmotic disruption
Clinical Tests (Compare to Contralateral)
- Squeeze test: most sensitive (compress mid-calf, pain at ankle)
- External rotation stress: most specific
- Cotton test: greater than 2mm fibular translation = unstable
- Palpate entire fibula (rule out Maisonneuve)
Radiographic Assessment
- Mortise view: clear space greater than 6mm = diastasis (MOST IMPORTANT)
- AP: tibiofibular overlap less than 6mm abnormal
- Mortise: overlap less than 1mm abnormal
- Stress views if equivocal (bilateral for comparison)
- Medial clear space = superior clear space (if wider = deltoid injury)
West Point Classification
- Latent: stable on stress → conservative
- Subluxation: unstable on stress → consider fixation (athlete)
- Dislocation: frank diastasis → operative mandatory
Surgical Technique Principles
- Ankle in DORSIFLEXION and NEUTRAL rotation (critical)
- Screw 2-3cm above plafond, 30° anterior-posterior
- Tricortical (3 cortices) vs quadricortical (4 cortices) - both work, tricortical less breakage
- Cotton test intraop: greater than 2mm translation = fix
- Check reduction: AP, mortise, lateral fluoroscopy
Screw vs Suture Button
- Screw: rigid, remove at 8-12 weeks, RTP 20-28 weeks
- Button: allows motion, no removal, RTP 12-16 weeks
- Both equivalent outcomes, button faster rehab
- Button higher cost but lower re-operation rate
Complications
- Malreduction (20-50%): even 1mm → 40% increased contact pressure
- Screw breakage: 25-50% if not removed by 12 weeks
- Post-traumatic arthritis: 10-30% at 5-10 years (higher with malreduction)
- Chronic instability: inadequate initial fixation, premature removal
Return to Sport
- Conservative: 8-12 weeks (latent injuries)
- Suture button: 12-16 weeks
- Screw: 20-28 weeks (includes removal time)
- Criteria: pain-free, full ROM, 90% strength, functional testing
- Use ankle brace for 6-12 months after return
Critical Numbers to Remember
- 6mm: clear space threshold on mortise view
- 1mm: malreduction increases pressure by 40%
- 2mm: Cotton test translation threshold
- 2-3cm: screw distance above plafond
- 30°: screw trajectory (anterior-posterior)
- 8-12 weeks: screw removal timing
Evidence Base
Dynamic vs Static Fixation: Level I Meta-analysis of RCTs
- Meta-analysis of randomised controlled trials comparing dynamic (suture button) versus static (screw) syndesmotic fixation
- Dynamic fixation significantly reduced overall complications (RR 0.55) and inadequate reduction at final follow-up (RR 0.36)
- Lower risk of recurrent diastasis or clinical instability with dynamic fixation (RR 0.10)
- Reoperation risk reduced with dynamic fixation versus permanent screws (RR 0.24)
- AOFAS score modestly higher with dynamic fixation (+8.6 points at 24 months); overall quality of evidence moderate to very low
Clear Space Measurement: Radiographic Criteria
- Cadaveric radiographic study (12 lower limbs) defining the normal distal tibiofibular relationship on AP and mortise views
- Tibiofibular clear space on AP and mortise views should be less than approximately 6mm
- Tibiofibular overlap on AP view should be greater than approximately 6mm (or 42% of fibular width)
- Tibiofibular overlap on mortise view should be greater than approximately 1mm
- Tibiofibular clear space was the single most reliable parameter for detecting early syndesmotic widening
Syndesmotic Ligament Biomechanics
- Ex vivo tensile testing of anterior and posterior tibiofibular ligaments and the posterior tibiotalar deltoid in 10 cadaveric limbs
- Posterior tibiofibular ligament (PITFL) showed the greatest tensile strength of the structures tested
- Anterior tibiofibular ligament (AITFL) typically failed by mid-substance rupture near its fibular insertion
- PITFL failures were split between mid-substance rupture and fibular avulsion
- Tibiofibular ligaments were stronger than the lateral collateral and deltoid ligaments, underscoring their constraining role
Reduction Quality Predicts Functional Outcome
- Multicentre retrospective review of 51 ankle fractures treated with syndesmotic screw fixation across three university hospitals
- On postoperative radiographs, 16% of syndesmoses were not anatomically reduced
- Quality of syndesmotic reduction was the ONLY significant predictor of functional outcome (p = 0.04)
- Reduction alone accounted for 15-18% of the variance in validated functional scores (SMFA, Olerud-Molander)
- 8 of 51 screws were judged to have had inadequate indications, highlighting technique and indication variability
Suture Button vs Single Screw: Randomised Trial
- 97 patients randomised to suture button (n=48) or a single quadricortical syndesmotic screw (n=49), with 90% followed to 2 years
- Higher median AOFAS (96 vs 86) and Olerud-Molander (100 vs 90) scores in the suture button group at 2 years
- Less pain on walking and at rest, and higher EQ-5D index, with suture button
- Tibiofibular side-to-side difference of 2mm or more on CT at 2 years in 20/40 screw versus 8/40 suture button patients (p = 0.009)
- 7 screw patients developed symptomatic recurrent diastasis versus none with suture button
Reduction Accuracy on Bilateral CT: TightRope vs Screw
- Prospective RCT (43 patients) comparing TightRope versus a single 3.5mm tricortical screw in PER/Weber-C fractures, assessed with bilateral CT
- Postoperative malreduction rates were similar between groups
- Intraoperative CT of dynamically fixed ankles was misleading unless the ankle was supported at 90 degrees, mimicking malreduction
- At 2 years, reduction was better maintained with TightRope; malreduction tended to increase with the screw
- No significant difference in functional scores or osteoarthritis incidence
Diagnostic Accuracy of Clinical Tests (MRI Reference)
- Cross-sectional diagnostic accuracy study of 87 acute ankle sprains across 9 Australian clinics, with MRI as the reference standard
- Squeeze test was the most specific clinical test (specificity 88%, positive LR 2.15)
- Dorsiflexion-external rotation stress test: sensitivity 71%, negative LR 0.46
- Syndesmosis ligament tenderness was highly sensitive (92%); inability to single-leg hop had 89% sensitivity
- No single test was sufficiently accurate alone; combining sensitive and specific tests improved diagnosis
References
-
Hermans JJ, Beumer A, de Jong TA, Kleinrensink GJ. Anatomy of the distal tibiofibular syndesmosis in adults: a pictorial essay with a multimodality approach. J Anat. 2010;217(6):633-645. doi:10.1111/j.1469-7580.2010.01302.x
-
Waterman BR, Belmont PJ, Cameron KL, Deberardino TM, Owens BD. Epidemiology of ankle sprain at the United States Military Academy. Am J Sports Med. 2010;38(4):797-803. doi:10.1177/0363546509350757
-
Nussbaum ED, Hosea TM, Sieler SD, Incremona BR, Kessler DE. Prospective evaluation of syndesmotic ankle sprains without diastasis. Am J Sports Med. 2001;29(1):31-35. doi:10.1177/03635465010290010301
-
Hunt KJ, Phisitkul P, Pirolo J, Amendola A. High ankle sprains and syndesmotic injuries in athletes. J Am Acad Orthop Surg. 2015;23(11):661-673. doi:10.5435/JAAOS-D-13-00135
-
van Dijk CN, Longo UG, Loppini M, Florio P, Maltese L, Ciuffreda M, Denaro V. Classification and diagnosis of acute isolated syndesmotic injuries: ESSKA-AFAS consensus and guidelines. Knee Surg Sports Traumatol Arthrosc. 2016;24(4):1200-1216. doi:10.1007/s00167-015-3942-8
-
Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989;10(3):156-160. doi:10.1177/107110078901000308
-
Beumer A, van Hemert WL, Swierstra BA, Jasper LE, Belkoff SM. A biomechanical evaluation of the tibiofibular and tibiotalar ligaments of the ankle. Foot Ankle Int. 2003;24(5):426-429. doi:10.1177/107110070302400509
-
Alonso A, Khoury L, Adams R. Clinical tests for ankle syndesmosis injury: reliability and prediction of return to function. J Orthop Sports Phys Ther. 1998;27(4):276-284. doi:10.2519/jospt.1998.27.4.276
-
Sman AD, Hiller CE, Rae K, Linklater J, Black DA, Nicholson LL, Refshauge KM. Diagnostic accuracy of clinical tests for ankle syndesmosis injury. Br J Sports Med. 2015;49(5):323-329. doi:10.1136/bjsports-2013-092787
-
Sikka RS, Fetzer GB, Sugarman E, Wright RW, Fritts H, Boyd JL, Fischer DA. Correlating MRI findings with disability in syndesmotic sprains of NFL players. Foot Ankle Int. 2012;33(5):371-378. doi:10.3113/FAI.2012.0371
-
Lubberts B, Verhaven E, D'Hooghe P, Vereecke E, van Dijk CN. Epidemiology and return to play following isolated syndesmotic injuries of the ankle: a prospective cohort study of 3677 male professional footballers in the UEFA Elite Club Injury Study. Br J Sports Med. 2019;53(15):959-964. doi:10.1136/bjsports-2017-097710
-
Weening B, Bhandari M. Predictors of functional outcome following transsyndesmotic screw fixation of ankle fractures. J Orthop Trauma. 2005;19(2):102-108. doi:10.1097/00005131-200502000-00006
-
Kukreti S, Faraj A, Miles JN. Does position of syndesmotic screw affect functional and radiological outcome in ankle fractures? Injury. 2005;36(9):1121-1124. doi:10.1016/j.injury.2005.02.015
-
Lubberts B, Vopat BG, Wolf JC, Linn MS, Guss D, Nahed R, DiGiovanni CW. Arthroscopically assisted syndesmotic reduction: a systematic review of biomechanical and clinical outcomes. Arthroscopy. 2017;33(8):1585-1594. doi:10.1016/j.arthro.2017.03.005
-
Grass R, Rammelt S, Biewener A, Zwipp H. Peroneus longus ligamentoplasty for chronic instability of the distal tibiofibular syndesmosis. Foot Ankle Int. 2003;24(5):392-397. doi:10.1177/107110070302400504
-
Schepers T, Van Lieshout EM, de Vries MR, Van der Elst M. Increased rates of wound complications with locking plates in distal fibular fractures. Injury. 2011;42(10):1125-1129. doi:10.1016/j.injury.2011.01.009
-
Manjoo A, Sanders DW, Tieszer C, MacLeod MD. Functional and radiographic results of patients with syndesmotic screw fixation: implications for screw removal. J Orthop Trauma. 2010;24(1):2-6. doi:10.1097/BOT.0b013e3181a9f7a5
-
Laflamme M, Belzile EL, Bédard L, van den Bekerom MP, Glazebrook M, Pelet S. A prospective randomized multicenter trial comparing clinical outcomes of patients treated surgically with a static or dynamic implant for acute ankle syndesmosis rupture. J Orthop Trauma. 2015;29(5):216-223. doi:10.1097/BOT.0000000000000245
-
Andersen MR, Frihagen F, Hellund JC, Madsen JE, Figved W. Randomized trial comparing suture button with single syndesmotic screw for syndesmosis injury. J Bone Joint Surg Am. 2018;100(1):2-12. doi:10.2106/JBJS.16.01011
-
Kortekangas TH, Flinkkilä T, Niinimäki J, Leskelä HV, Savolainen V, Pakarinen H, Ohtonen P, Ristiniemi J. A prospective randomised study comparing TightRope and syndesmotic screw fixation for accuracy and maintenance of syndesmotic reduction assessed with bilateral computed tomography. Injury. 2015;46(6):1119-1126. doi:10.1016/j.injury.2015.02.004