Midfoot Degenerative Joint Disease | Triple Joint Complex | Surgical Challenge
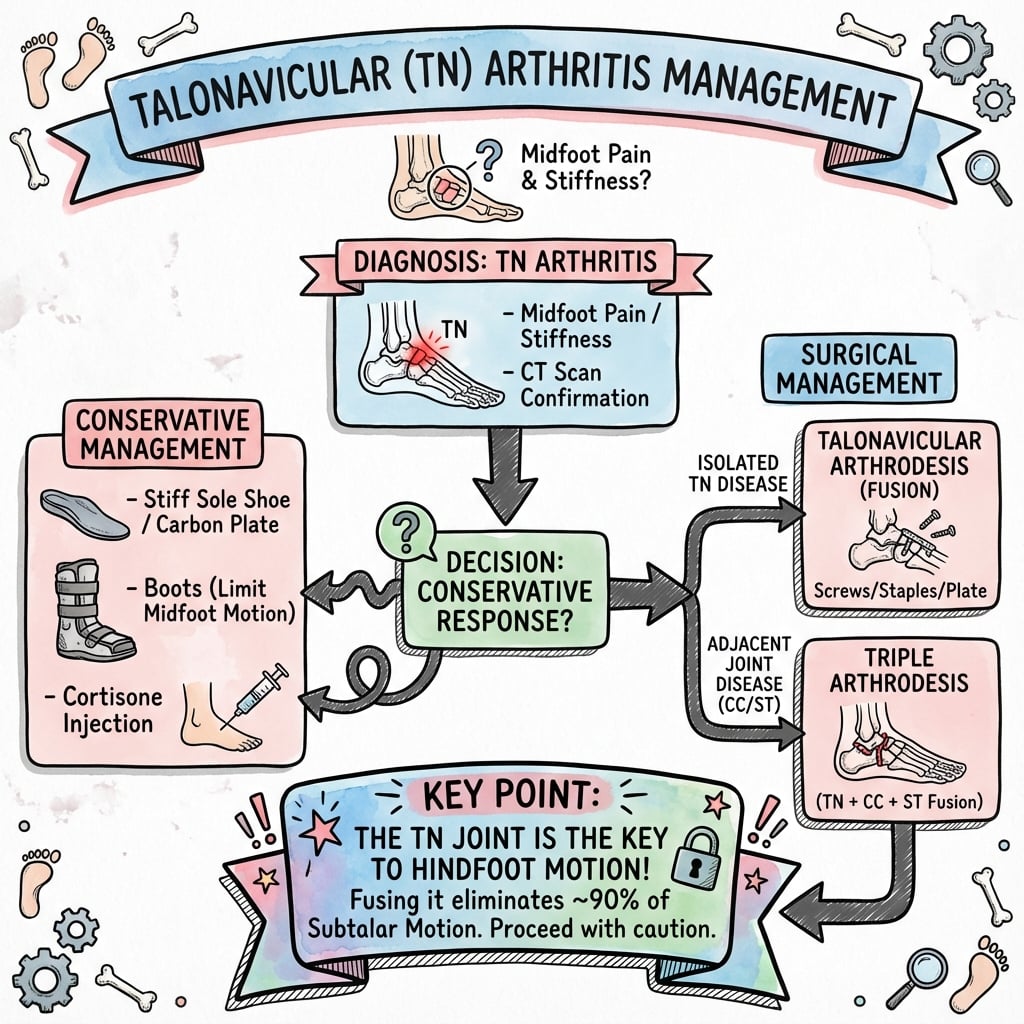
- TN joint is critical for hindfoot-forefoot motion and inversion/eversion
- Arthritis commonly involves adjacent joints - check subtalar and calcaneocuboid
- Isolated TN arthrodesis maintains 70-80% of hindfoot motion
- Triple arthrodesis indicated when multiple hindfoot joints involved
- Adult-acquired flatfoot (PTTD Stage 3) commonly leads to TN arthritis
- “TN joint contributes 50% of hindfoot inversion/eversion
- “Beaking on dorsal navicular = chronic TN arthritis hallmark
- “Beware posterior tibial tendon dysfunction coexistence
- “Isolated TN fusion: consider ball-and-socket ankle contraindication
- Imaging Findings
- Joint space narrowing only
- Treatment
- NSAIDs, orthoses, activity modification
- Key Pearl
- 6 months conservative trial mandatory
- Imaging Findings
- TN arthritis isolated, subtalar preserved
- Treatment
- Isolated TN arthrodesis
- Key Pearl
- Preserves 70-80% hindfoot motion
- Imaging Findings
- TN + subtalar + CC arthritis
- Treatment
- Triple arthrodesis
- Key Pearl
- Corrects deformity and pain simultaneously
- Imaging Findings
- Moderate arthritis, preserved bone stock
- Treatment
- Consider TN arthroplasty (emerging)
- Key Pearl
- Limited long-term data available
Overview and Epidemiology
Talonavicular arthritis represents degeneration of the critical articulation between the talar head and navicular. As the apex of the medial longitudinal arch, TN joint pathology profoundly affects foot biomechanics, leading to arch collapse, forefoot abduction, and altered gait patterns. Understanding TN arthritis is essential as it rarely exists in isolation and commonly coexists with posterior tibial tendon dysfunction and adjacent joint pathology.
- Articular cartilage loss: Progressive degeneration
- Subchondral sclerosis: Abnormal loading patterns
- Osteophyte formation: Dorsal beaking characteristic
- Arch collapse: Loss of keystone support
- Forefoot abduction: Compensatory malalignment
- PTTD Stage 3: Most common association
- Subtalar arthritis: 60-70% coexistence
- Calcaneocuboid arthritis: 30-40% involvement
- Ankle valgus: Secondary deformity
- Hallux valgus: Forefoot compensation
The Ball-and-Socket Ankle: A Contraindication to Isolated TN Fusion
A ball-and-socket ankle - a rounded, domed talar body articulating with a congruent concave tibial plafond - is a compensatory adaptation that develops when native subtalar and transverse-tarsal (inversion/eversion) motion is congenitally absent or lost early in life. The ankle assumes the coronal-plane motion normally shared across the hindfoot. Spotting it on a mortise radiograph should trigger a search for its cause and stop you before offering an isolated talonavicular fusion.
The ball-and-socket ankle is most classically associated with tarsal coalition (especially talocalcaneal), congenital longitudinal limb deficiencies such as fibular hemimelia, and previously operated or fused hindfeet. Its relevance to talonavicular arthritis is a specific surgical trap that this topic flags but does not otherwise explain.
- The hindfoot already offloads onto the ankle for inversion/eversion; a stiffening TN fusion pushes even more demand onto that single joint, accelerating ankle degeneration
- The "spared" subtalar joint is not truly mobile when a coalition underlies the ball-and-socket adaptation, so the motion-sparing rationale for isolated fusion collapses
- The primary pathology (coalition or deficiency) is unaddressed by a TN fusion alone, so deformity and symptoms recur
- Treat a ball-and-socket ankle as a red flag for an underlying coalition and investigate accordingly (see the dedicated tarsal coalition topic)
- Plan around the whole abnormal hindfoot, not the TN joint in isolation
- Counsel that the ankle is the motion reserve and must be protected, not further loaded
Pathophysiology and Mechanisms
The TN joint is the apex of the medial longitudinal arch and contributes 50% of total hindfoot inversion and eversion. Loss of TN function shifts motion demands to adjacent joints (subtalar, ankle, calcaneocuboid), potentially accelerating degenerative changes. The posterior tibial tendon inserts on the navicular tuberosity and is intimately related to TN joint stability.
- Anatomical Details
- Ball (talar head) and socket (navicular concavity)
- Clinical Significance
- Primary site of midfoot motion - 50% inversion/eversion
- Anatomical Details
- Plantar support from calcaneus to navicular
- Clinical Significance
- Loss leads to talar head plantar subluxation
- Anatomical Details
- Inserts on navicular tuberosity
- Clinical Significance
- Dysfunction causes medial column collapse and TN stress
- Anatomical Details
- TN, subtalar, calcaneocuboid
- Clinical Significance
- Function as integrated unit - isolated pathology rare
Motion Contribution
The TN joint is part of the oblique axis of the hindfoot, allowing combined:
- Inversion: 50% contribution to total hindfoot inversion (20-30 degrees)
- Eversion: 50% contribution to total hindfoot eversion (10-15 degrees)
- Forefoot locking: Critical for rigid lever during push-off
- Shock absorption: Allows hindfoot adaptability on uneven ground
TRAUMASTalonavicular Arthritis Causes
Hook:Think of foot TRAUMAS that damage the TN joint over time!
Classification and Grading
Radiographic Classification
- Radiographic Findings
- Joint space narrowing under 50%, minimal osteophytes
- Clinical Correlation
- Mild pain with activity, preserved function
- Management
- Conservative management preferred
- Radiographic Findings
- 50-75% joint space loss, moderate osteophytes, subchondral sclerosis
- Clinical Correlation
- Moderate pain limiting activity
- Management
- Surgical candidates after failed conservative
- Radiographic Findings
- Bone-on-bone, large osteophytes, deformity, dorsal beaking
- Clinical Correlation
- Severe pain at rest, functional limitation
- Management
- Arthrodesis or arthroplasty indicated
Clinical Assessment
- Pain location: Dorsomedial midfoot, navicular region
- Pain character: Aching at rest, sharp with activity
- Aggravating factors: Walking, stairs, uneven ground
- Associated symptoms: Arch collapse, forefoot abduction
- Functional impact: Distance limitation, altered gait
- Previous injuries: Midfoot trauma, ankle sprains
- Inspection: Medial arch height, forefoot abduction
- Palpation: TN joint tenderness, dorsal osteophytes
- Range of motion: Hindfoot inversion/eversion reduced
- Posterior tibial function: Single heel rise test
- Gait analysis: Antalgic, loss of push-off power
- Adjacent joints: Subtalar, ankle, first ray mobility
Up to 70% of TN arthritis cases have coexisting PTTD. Failure to address PTT dysfunction leads to recurrent deformity after TN fusion. Always perform single heel rise test and assess for too-many-toes sign. Stage the PTTD appropriately as it may alter surgical planning.
Physical Examination Maneuvers
Systematic Examination Sequence
Arch height: Evaluate medial longitudinal arch - collapsed versus normal. Hindfoot alignment: Valgus suggests PTTD, varus suggests other pathology. Too-many-toes sign: Visible lateral toes when viewing from behind = flatfoot.
Technique: Patient stands on affected leg and rises onto toes. Positive finding: Inability to rise or maintain position = PTT dysfunction. Heel inversion: Normal heel inverts during heel rise; absent in PTTD.
TN joint motion: Stabilize talus, move navicular - crepitus and pain. Subtalar motion: Inversion/eversion - compare to contralateral. Flexibility: Rigid versus flexible deformity affects surgical options.
TN stress test: Direct pressure over TN joint reproduces pain. Forefoot abduction stress: Worsens pain if TN unstable. Tiptoe test: Unable to achieve or maintain due to pain.
Investigations

Imaging Protocol
Views: AP, lateral, oblique foot radiographs standing. TN joint assessment: Joint space, osteophytes, dorsal beaking. Alignment: Talar head coverage by navicular, forefoot abduction. Adjacent joints: Evaluate subtalar and calcaneocuboid.
Indications: Surgical planning, assess deformity severity. Information: Bone stock quality, subchondral cyst size, fusion preparation. 3D reconstruction: Helpful for complex deformity understanding.
Indications: Assess PTT integrity, spring ligament, articular cartilage. Findings: Cartilage loss, bone marrow edema, tendon pathology. Role: Pre-operative planning when soft tissue pathology suspected.
Radiographic Findings
- Description
- Reduction in TN joint space under 2mm
- Clinical Implication
- Primary sign of arthritis - correlates with symptoms
- Description
- Osteophyte formation on dorsal navicular
- Clinical Implication
- Pathognomonic for chronic TN arthritis
- Description
- Increased density at articular surfaces
- Clinical Implication
- Chronic abnormal loading pattern
- Description
- Lateral subluxation, under 60% coverage
- Clinical Implication
- Indicates flatfoot deformity and PTTD
Management Algorithm
Non-Operative Treatment
Indications:
- Mild to moderate symptoms
- Early-stage arthritis (Grade 1-2)
- Patient preference or medical comorbidities
- Minimum 6-month trial before considering surgery
Conservative Protocol
Reduce high-impact activities: Running, jumping, prolonged standing. Footwear: Supportive shoes with rocker-bottom sole, stiff midsole. Goal: Decrease stress on TN joint during daily activities.
Custom orthoses: Medial arch support, forefoot posting. Off-the-shelf: Arizona brace, UCBL orthosis for rigid support. Goal: Support arch, reduce TN motion, offload joint.
NSAIDs: First-line for pain and inflammation control. Corticosteroid injection: TN joint injection under image guidance. Duration: Maximum 2-3 injections per year.
Strengthening: Posterior tibial tendon, intrinsic foot muscles. Stretching: Gastrocnemius-soleus complex to reduce forefoot load. Gait training: Optimize mechanics to reduce TN stress.
Approximately 40-50% of patients with mild to moderate TN arthritis achieve satisfactory symptom control with comprehensive conservative management. Predictors of success include flexible deformity, mild radiographic changes, and absence of significant PTTD.
FUSETalonavicular Arthritis Management
Hook:Conservative measures first, then FUSE the joint when they fail!
Surgical Technique: Isolated TN Arthrodesis
Dorsomedial Approach to Talonavicular Joint
Surgical Steps
Position: Supine with bump under ipsilateral hip. Tourniquet: Thigh tourniquet recommended. C-arm: Position for AP, lateral, and oblique foot views.
Location: Dorsomedial foot, centered over TN joint. Landmarks: Start 2cm proximal to navicular tuberosity, extend distally 6-8cm. Orientation: Curvilinear following course of TN joint.
Identify: Extensor hallucis longus (EHL) tendon medially. Protect: Superficial peroneal nerve branches laterally. Develop: Interval lateral to EHL tendon.
Capsulotomy: Incise TN joint capsule dorsally. Exposure: Reflect capsule to expose articular surfaces completely. Identify: Talar head and navicular articular cartilage.
Superficial peroneal nerve: Dorsolateral to incision - identify and protect. Dorsalis pedis artery: Deep to extensor tendons - avoid excessive lateral retraction. Deep peroneal nerve: Adjacent to dorsalis pedis - preserve vascular supply.
Complications
- Incidence
- 10-15% isolated TN, 15-20% double/triple
- Risk Factors
- Smoking, diabetes, osteoporosis, poor bone contact
- Management
- Revision fusion with bone graft and improved fixation
- Incidence
- 20-30% at 10 years post-fusion
- Risk Factors
- Increased motion demand, malalignment
- Management
- Activity modification, orthoses, possible future fusion
- Incidence
- 5-10% superficial infection, under 2% deep
- Risk Factors
- Diabetes, smoking, poor soft tissue handling
- Management
- Antibiotics for superficial, debridement for deep
- Incidence
- 2-5% temporary, under 1% permanent
- Risk Factors
- Superficial peroneal nerve at risk
- Management
- Usually resolves; neurolysis if persistent
- Incidence
- 5-10% malalignment
- Risk Factors
- Poor intraoperative alignment, inadequate fixation
- Management
- May require corrective osteotomy or revision
Nonunion is the most common major complication. Prevention strategies: (1) Complete cartilage removal to bleeding bone, (2) Maximize bone contact surface area, (3) Rigid fixation with crossed screws or plate, (4) Bone graft for defects, (5) Post-op non-weight-bearing for 6-8 weeks, (6) Smoking cessation mandatory, (7) Optimize diabetes control.
Postoperative Care and Rehabilitation
Rehabilitation Timeline - Isolated TN Fusion
Immobilization: Below-knee cast or CAM boot. Weight-bearing: Non-weight-bearing with crutches. Elevation: Strict elevation to minimize swelling. Monitoring: Wound check at 2 weeks, suture removal.
Immobilization: Continue cast or boot. Weight-bearing: Non-weight-bearing continued. Radiographs: 6-week X-rays to assess fusion progress. DVT prophylaxis: Consider if risk factors present.
Weight-bearing: Transition to partial then full weight-bearing in boot. Criteria: Radiographic evidence of fusion (bridging trabeculae). Physical therapy: ROM exercises for adjacent joints. Monitoring: 12-week X-rays to confirm fusion.
Transition: Wean from boot to supportive shoe with orthosis. Activities: Gradual return to normal activities. Goals: Full weight-bearing, pain-free ambulation. Final assessment: 6-month clinical and radiographic evaluation.
Outcomes and Prognosis
- Isolated TN Fusion
- 85-90%
- Triple Arthrodesis
- 90-95%
- Notes
- Higher with plate fixation
- Isolated TN Fusion
- 80-85%
- Triple Arthrodesis
- 75-85%
- Notes
- Pain relief primary driver
- Isolated TN Fusion
- 70-80% return to pre-injury level
- Triple Arthrodesis
- 60-70%
- Notes
- Younger, healthier patients do better
- Isolated TN Fusion
- 20-30% at 10 years
- Triple Arthrodesis
- 30-40% at 10 years
- Notes
- Increased with malalignment
Predictors of Good Outcome
- Successful fusion without complications
- Correct alignment restoration
- Isolated TN arthritis (no adjacent disease)
- Non-smoker, well-controlled diabetes
- Moderate activity expectations
- Nonunion requiring revision
- Malalignment or malunion
- Pre-existing adjacent joint arthritis
- Smoking, uncontrolled diabetes
- High-impact activity demands
Guidelines, Registries & Global Practice
- Midfoot OA is common but under-recognised; symptomatic midfoot OA affects roughly 1 in 8 adults over 50 in population imaging studies
- Isolated TN involvement is uncommon (~10-15%); the TN joint is most often affected as part of a triple-complex or planovalgus pattern
- Leading drivers globally: post-traumatic (Lisfranc / navicular injury), inflammatory (RA), and stage III progressive flatfoot
- Müller-Weiss disease clusters in middle-aged women and in regions with historic childhood under-nutrition
- Nonunion risk: 10-15%, higher in smokers and diabetics
- Adjacent joint arthritis: 20-30% at 10 years
- Nerve injury: 2-5% superficial peroneal nerve
- Infection: 5-10% superficial, under 2% deep
- Prolonged recovery: 3-6 months to fusion, 6-12 months full recovery
- Position Relevant to TN Arthritis
- Stage-based management; joint-sparing reconstruction before fusion where flexible
- Practical Implication
- Reserve TN fusion for rigid/arthritic stage III disease
- Position Relevant to TN Arthritis
- Trial of structured non-operative care and orthoses before arthrodesis
- Practical Implication
- Document conservative trial; podiatry-led pathway emphasised
- Position Relevant to TN Arthritis
- Rigid fixation, complete cartilage debridement to bleeding bone, dual-implant compression
- Practical Implication
- Technique standard underpinning high union rates
- Position Relevant to TN Arthritis
- Favour limited (joint-sparing) fusion to preserve hindfoot motion when feasible
- Practical Implication
- Isolated/double fusion over triple when CC and STJ are healthy
- Position Relevant to TN Arthritis
- No dedicated TN implant tracking — no registry-validated TN arthroplasty exists
- Practical Implication
- TN arthroplasty remains investigational; fusion is the registry-supported standard
- Weight-bearing CT and MRI for staging and PTT/spring-ligament assessment
- Cannulated compression screws, locking dorsal plates, headless compression implants
- Adjuncts: bone stimulators, biologics for high-risk fusions
- Reliance on weight-bearing plain radiographs alone; clinical staging of PTTD
- Standard cancellous screws and staples; local autograft (calcaneus) over iliac crest
- Extended cast immobilisation where boots/early ROM rehab unavailable
Key documentation requirements:
- Document comprehensive conservative trial (minimum 6 months) before surgery
- Assessment of adjacent joint status and reasoning for procedure selection
- Discussion of smoking cessation and diabetes optimization
- Detailed informed consent including nonunion and adjacent joint degeneration risks
- Post-operative non-compliance with weight-bearing restrictions can lead to failure - document instructions clearly
Controversies and Areas of Uncertainty
- Arguments For
- Modified double spares CC joint and lateral column
- Arguments Against
- Higher TN nonunion after modified double (44% vs 0% in Burrus et al)
- Current Position
- Triple still favoured for rigid deformity; double in selected mobile lateral columns
- Arguments For
- CC fusion theoretically improves correction and stability
- Arguments Against
- Symptomatic CC nonunion is rare; sparing it shortens surgery
- Current Position
- Increasing support for sparing CC when not arthritic (Moore et al)
- Arguments For
- Preserves midfoot motion in young, high-demand patients
- Arguments Against
- No registry data, unknown implant survival, technically demanding
- Current Position
- Investigational only — fusion remains the standard of care
- Arguments For
- Plates/dual implants give rigid compression in poor bone
- Arguments Against
- Crossed screws are lower-profile with less dissection
- Current Position
- Dual-implant (screw + staple/plate) favoured over single screw
- Arguments For
- Isolated TN/tension-band preserves motion (Fornaciari et al)
- Arguments Against
- Perinavicular OA may demand TN-cuneiform extension
- Current Position
- MRI-guided extent decision; isolate when peri-navicular joints spared
MCQ Practice Points
Q: What percentage of total hindfoot inversion and eversion motion occurs at the talonavicular joint? A: 50% - The TN joint contributes approximately 50% of hindfoot inversion/eversion through its role in the oblique axis. Loss of TN motion shifts demands to subtalar and ankle joints.
Q: What is the most common cause of talonavicular arthritis? A: Post-traumatic arthritis - Midfoot fractures and dislocations are the leading cause. Adult-acquired flatfoot (PTTD Stage 3) is the second most common etiology.
Q: What clinical sign is pathognomonic for chronic talonavicular arthritis on radiographs? A: Dorsal beaking of the navicular - Dorsal osteophyte formation on the navicular is characteristic of chronic TN arthritis and indicates longstanding degenerative changes.
Q: What is the fusion rate for isolated talonavicular arthrodesis? A: 85-90% - Isolated TN fusion has high success rates. Nonunion occurs in 10-15% and is more common in smokers, diabetics, and cases with inadequate fixation.
Q: What is the standard fixation for isolated TN arthrodesis? A: Two crossed 3.5mm or 4.0mm cannulated screws - One screw from dorsal navicular to plantar talus, second from plantar navicular to dorsal talus. Crossed configuration provides rotational stability.
Q: What is the incidence of adjacent joint arthritis following isolated TN fusion at 10-year follow-up? A: 20-30% - Adjacent joint degeneration (subtalar, calcaneocuboid) occurs due to increased motion demands. Risk increased with malalignment and high activity levels.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old woman presents with progressive medial midfoot pain over 2 years. She has difficulty walking more than 500 meters and notes that her arch has collapsed. On examination, she has tenderness over the TN joint, a flatfoot deformity, and can perform a single heel rise with difficulty. Weight-bearing radiographs show moderate TN joint space narrowing with dorsal beaking but preserved subtalar joint. How would you manage this patient?”
“You have decided to proceed with isolated talonavicular arthrodesis in a 60-year-old diabetic patient with failed conservative management. Walk me through your surgical technique and key technical considerations.”
“At 6-month follow-up, your patient who underwent TN arthrodesis continues to have pain at the fusion site. Radiographs show a lucent gap at the TN joint with no bridging trabeculae. How do you manage this nonunion?”
Evidence Base and Key Trials
Isolated TN Arthrodesis in Rheumatoid Arthritis with PTTD
- Prospective series of 26 patients (20 women, 6 men), mean age 43.6 years
- Mean AOFAS hindfoot score improved from 48.2 to 88.6 at mean 4.5-year follow-up
- Only one nonunion and two superficial wound infections across the cohort
- Fusion achieved with screws, memory staples, or a combination
Screw-and-Staple Technique for Isolated TN Arthrodesis
- Single-surgeon series of 20 feet with inflammatory talonavicular arthritis
- Solid arthrodesis in 19 of 20 feet (95%) at an average of 11 weeks
- Combined screw plus staple fixation with indirect joint distraction
- Complications: one nonunion, one DVT, one superficial wound infection
Triple Arthrodesis: 25- and 44-Year Follow-up
- 67 feet in 57 young patients, mostly neuromuscular (poliomyelitis predominant)
- 54 patients (95%) remained satisfied despite progressive degeneration
- By second follow-up ALL ankles showed degenerative change; midfoot joints also affected
- Pseudarthrosis in 13 feet; need for walking support rose from 32% to 68%
Modified Double versus Triple Arthrodesis for Rigid Planovalgus
- Retrospective comparison: modified double (n=9) versus triple (n=7) for stage 3 planovalgus
- TN nonunion rate 44% (4 of 9) after modified double versus 0% after triple (p=0.042)
- FAAM and FAOS activity and quality-of-life scores significantly worse after double
- No difference in preoperative radiographic parameters between groups
Isolated TN Tension-Band Fusion for Müller-Weiss Syndrome
- Prospective series of 10 feet with advanced Müller-Weiss (Maceira stage III-IV)
- AOFAS score improved from 33 to 88.3 (p under 0.0001) at minimum 24-month follow-up
- Trabecular bridging by 2-3 months in 9 of 10 feet using a static tension-band construct
- One implant failure required revision with additional screw fixation
Single- versus Double-Incision Triple Arthrodesis
- Retrospective comparison of 70 patients (37 single-incision lateral, 33 double-incision)
- No difference in deformity correction, union, complications, or VAS pain improvement
- Operative time shorter with single lateral incision (86 vs 95 minutes, p=0.04)
- Only calcaneocuboid joints showed radiographic nonunion in either group