Flexion (Burst) vs Extension (Avulsion) | SLIC Classification | Anterior Corpectomy | Spinal Cord Injury
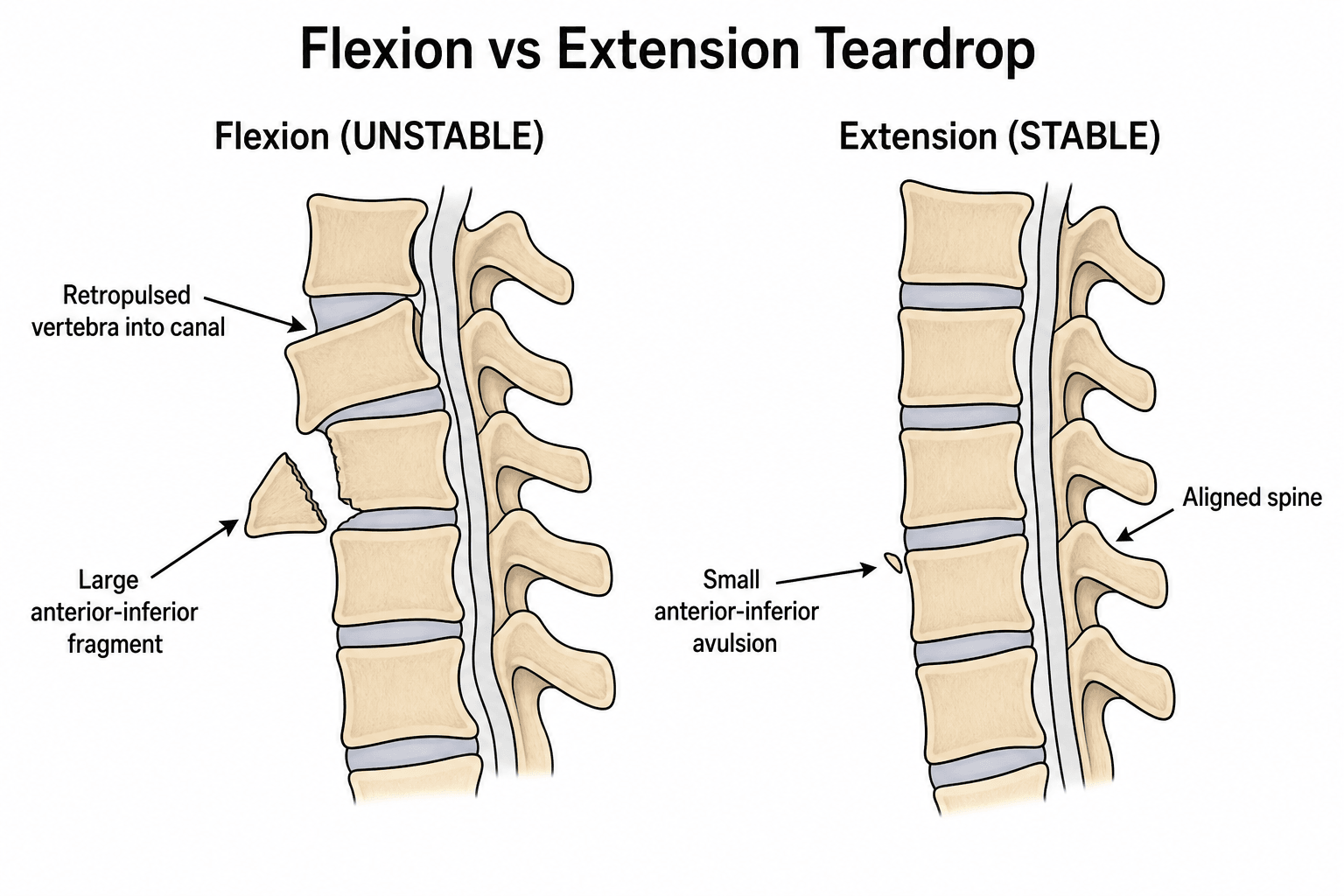
- Two Types: Flexion Teardrop (Unstable, Burst) vs Extension Teardrop (Usually Stable, Avulsion).
- Flexion Teardrop: Catastrophic injury. Kyphosis, retropulsed fragment, ALL ligaments disrupted. Quadriplegia common.
- Extension Teardrop: Elderly/Osteoporotic. Avulsion of anteroinferior vertebral body by ALL. Usually stable.
- Imaging: CT to assess fragment and canal. MRI for discs/ligaments/cord.
- Treatment: Flexion teardrop needs surgical stabilization. Extension teardrop often non-op.
- “The 'Teardrop' fragment is misleading - Flexion type is a BURST injury, not just an avulsion.
- “Flexion Teardrop has ALL THREE column disruption (Unstable).
- “Extension Teardrop is an avulsion at the ALL attachment (Stable unless severe).
- “Check for Sagittal Vertebral Body Fracture (Flexion Teardrop splits the body).
Flexion vs Extension. They have opposite stability profiles. Flexion = Unstable. Extension = Usually Stable. Know the difference.
It's a BURST Injury. The fragment is just the tip of the iceberg. There is posterior ligamentous disruption and retropulsion.
Expect Cord Injury. Flexion teardrop often presents with quadriplegia or anterior cord syndrome.
Extension Teardrop Can Progress. If severe, may have delayed instability. Follow-up imaging.
- Flexion Teardrop
- Axial Load + Flexion (Diving)
- Extension Teardrop
- Hyperextension + Axial Load
- Flexion Teardrop
- Young, High Energy
- Extension Teardrop
- Elderly, Osteoporotic
- Flexion Teardrop
- Burst (3-Column)
- Extension Teardrop
- Avulsion (Anterior Column)
- Flexion Teardrop
- UNSTABLE
- Extension Teardrop
- Usually STABLE
- Flexion Teardrop
- Common (Quad/Anterior Cord)
- Extension Teardrop
- Rare
- Flexion Teardrop
- Surgery (ACDF/Corpectomy)
- Extension Teardrop
- Collar / Halo
BURSTFlexion Teardrop Features
Hook:Flexion Teardrop is a BURST injury.
AVULSIONExtension Teardrop Features
Hook:Extension Teardrop is an AVULSION.
Dive InDiving Injury Pattern
Hook:Diving causes Flexion Teardrop.
Overview and Epidemiology
Teardrop fractures are cervical spine injuries with a triangular fragment from the anteroinferior vertebral body. There are TWO distinct types with opposite stability profiles: Flexion Teardrop (unstable burst injury, surgery needed) and Extension Teardrop (stable avulsion, usually conservative). Understanding the distinction is critical - flexion teardrop is a catastrophic 3-column injury often causing quadriplegia, while extension teardrop is usually stable with excellent prognosis.
- Flexion Teardrop: Young adults, high-energy trauma (diving, MVC, sports)
- Extension Teardrop: Elderly, low-energy falls with hyperextension
- Level: Most commonly C5 or C6
- Gender: No specific predilection
- Flexion: Catastrophic injury, high rate of quadriplegia, poor prognosis
- Extension: Usually stable, excellent prognosis with conservative treatment
- Neurological: Flexion teardrop often causes anterior cord syndrome or complete injury
- Surgery: Flexion teardrop requires anterior corpectomy, extension rarely needs surgery
Anatomy and Pathophysiology
- Axial Load: Force transmitted down the spine (head strike).
- Flexion: Cervical spine flexed at moment of impact.
- Burst: Vertebral body comminutes. Sagittal split common.
- Posterior Element Disruption: Posterior ligamentous complex fails in tension.
- Retropulsion: Posterior body fragment retropulses into canal.
- Result: Three-column injury. Grossly unstable. Cord compression.
- Hyperextension: Cervical spine hyperextends.
- Axial Load: Some axial component.
- ALL Tension: Anterior Longitudinal Ligament fails, avulsing a fragment.
- Result: Anterior column injury only. Stable (unless severe disc disruption).
- Flexion: Look for sagittal body fracture, posterior ligament injury, kyphosis.
- Extension: Fragment is from anteroinferior body. Body otherwise intact. No kyphosis.
Classification Systems
Teardrop Fracture Types
- Mechanism
- Axial load + flexion (diving)
- Pathology
- Burst (3-column injury)
- Stability
- UNSTABLE
- Neurology
- Common (quad/anterior cord)
- Treatment
- Surgery (ACCF)
- Mechanism
- Hyperextension + axial load
- Pathology
- Avulsion (anterior column)
- Stability
- Usually STABLE
- Neurology
- Rare
- Treatment
- Collar/halo (conservative)
Flexion Teardrop is a BURST injury (3-column, unstable, surgery needed) - the teardrop fragment is just the tip of the iceberg. Extension Teardrop is an AVULSION (anterior column only, usually stable, conservative). The teardrop fragment looks similar but the injuries are vastly different.
Clinical Assessment
- Mechanism: Diving (classic for flexion), MVC, fall with hyperextension (extension)
- Neurology: Weakness, numbness, bowel/bladder issues
- Pain: Neck pain, may radiate
- Age: Young (flexion), elderly (extension)
- Immobilization: Maintain C-spine precautions (collar)
- Neurological: Full motor/sensory exam, rectal tone, anal wink
- Cord syndromes: Anterior cord, central cord, complete injury
- Stability: Do not test range of motion - maintain immobilization
Flexion teardrop often causes:
- Anterior Cord Syndrome: Motor loss, pain/temperature loss, preserved proprioception/vibration
- Central Cord Syndrome: Upper limbs greater than lower limbs weakness
- Complete Cord Injury: No motor/sensory below level
Extension teardrop rarely causes neurological injury.
- Motor
- Complete loss below level
- Sensory
- Pain/temp lost, proprioception preserved
- Prognosis
- Poor - anterior spinal artery
- Motor
- Upper limbs greater than lower
- Sensory
- Variable
- Prognosis
- Better - may recover function
- Motor
- No motor below level
- Sensory
- No sensation below level
- Prognosis
- Poor - unlikely recovery
Spinal Shock vs Neurogenic Shock
Spinal shock is a neurological phenomenon: transient loss of all reflex activity below the injury (flaccid paralysis, areflexia, loss of bulbocavernosus and anal reflexes) immediately after cord injury, resolving over hours to days. Return of the bulbocavernosus reflex (S2-S4) marks the end of spinal shock - and you cannot accurately classify an injury as ASIA A (complete) while the patient is still in spinal shock, because apparent total loss may partly recover. Neurogenic shock is a haemodynamic phenomenon seen in cervical/high-thoracic (above T6) cord injury: loss of sympathetic outflow causes hypotension WITH bradycardia and warm, vasodilated peripheries - the opposite of the tachycardic, vasoconstricted picture of haemorrhagic shock.
In a trauma patient, always exclude haemorrhagic shock before attributing hypotension to neurogenic shock - the two can coexist. Once haemorrhage is excluded, manage neurogenic shock with judicious fluids, vasopressors (e.g. noradrenaline) and atropine for symptomatic bradycardia, targeting a MAP of ~85-90 mmHg for the first ~7 days to optimise spinal cord perfusion.
- Distinguishing Feature
- Sagittal body split, comminution, retropulsion, kyphosis, PLC disruption
- Stability / Action
- Unstable - surgery
- Distinguishing Feature
- Small fragment, body intact, no sagittal split, fragment height greater than width
- Stability / Action
- Usually stable - collar
- Distinguishing Feature
- Loss of anterior height without discrete teardrop fragment or retropulsion
- Stability / Action
- Usually stable
- Distinguishing Feature
- Central comminution and retropulsion without the classic anteroinferior triangular fragment
- Stability / Action
- Often unstable
- Distinguishing Feature
- Well-corticated, rounded, smooth margins, no oedema on MRI, incidental
- Stability / Action
- Stable - do not treat as acute
- Distinguishing Feature
- Fused, brittle spine; trivial mechanism; transverse fracture through ankylosed segment
- Stability / Action
- Highly unstable - very low threshold for surgery
A small anteroinferior fragment in a fused, ankylosed spine (ankylosing spondylitis or DISH) is not a benign avulsion - the rigid spine behaves like a long bone and these are unstable, three-column shear fractures with a high rate of delayed neurological deterioration. CT the whole cervical spine and have a very low threshold for cross-sectional imaging.
Investigations
Imaging Protocol
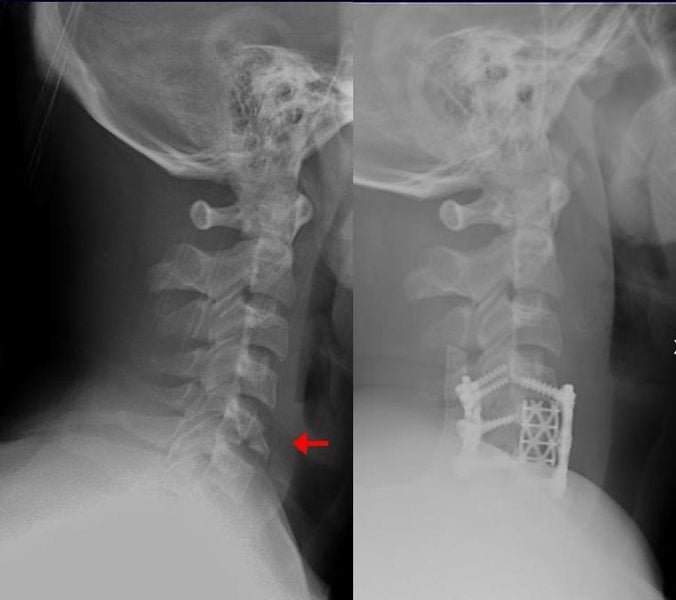
AP, lateral, odontoid views - may show teardrop fragment.
Findings:
- Teardrop fragment (anteroinferior corner)
- Kyphosis (flexion teardrop)
- Widening of interspinous distance (flexion teardrop)
- Loss of vertebral body height (flexion teardrop)
Essential for assessment - 1mm cuts with reconstructions.
Assess:
- Fragment size and location
- Vertebral body comminution (flexion) vs intact (extension)
- Sagittal split (flexion teardrop - key finding)
- Retropulsed fragment (flexion teardrop)
- Facet alignment
- Canal compromise
Required for soft tissue assessment.
Assess:
- Spinal cord (edema, contusion, compression)
- Disc herniation
- Posterior ligamentous complex (PLC) integrity
- Anterior longitudinal ligament (ALL)
- DLC (disco-ligamentous complex) status
Flexion Teardrop: Sagittal vertebral body fracture (key!), body comminution, kyphosis, retropulsed fragment, PLC disruption. Extension Teardrop: Small fragment, body otherwise intact, no sagittal split, no kyphosis, posterior elements intact. CT is essential to differentiate - sagittal split is the key finding for flexion teardrop.
Screen for Vertebral Artery Injury (Blunt Cerebrovascular Injury)
Cervical spine fractures - particularly those with translation, facet subluxation/dislocation, or extension into the foramen transversarium (as a displaced flexion teardrop may have) - carry a real risk of blunt cerebrovascular injury (BCVI) to the vertebral (or carotid) artery, which can cause posterior-circulation stroke. Apply screening criteria (e.g. the modified Denver criteria - which include any cervical spine fracture with subluxation, fracture through the transverse foramen, or upper C1-C3 fractures) and obtain CT angiography of the neck. Confirmed BCVI is usually managed with antithrombotic therapy (antiplatelet or anticoagulation), balanced against the patient's bleeding/injury profile, to reduce stroke risk. This is an easy mark to drop in a cervical-trauma viva.
Management Algorithm

Flexion Teardrop Management
Surgical Stabilization Required.
- Immediate: C-spine immobilization. ICU admission.
- Traction: May be used for initial alignment (Gardner-Wells tongs).
- Imaging: CT + MRI.
- Surgery:
- Approach: Anterior (Corpectomy + Cage + Plate) OR Combined Anterior-Posterior.
- Anterior Corpectomy: Remove fractured vertebra. Structural graft. Plate fixation.
- Posterior Stabilization: Lateral mass screws/rods if significant kyphosis or posterior instability.
- Post-op: ICU monitoring. Collar.
Anterior approach addresses the main pathology (burst body + disc). Posterior added if severe kyphosis.
Surgical Technique
Anterior Cervical Corpectomy and Fusion (ACCF)
For Flexion Teardrop.
- Positioning: Supine, head neutral. Inline traction.
- Approach: Standard anterior cervical (left-sided). Platysma, longus colli.
- Discectomy: Remove discs above and below fractured level.
- Corpectomy: Remove fractured vertebral body. Decompress canal.
- Graft: Structural cage (titanium or PEEK) filled with bone graft.
- Plate: Anterior cervical plate spanning levels above and below.
- Closure: Hemostasis. Drain optional. Layered closure.
May add posterior stabilization if severe ligamentous injury.
Complications
- Risk Factor
- Missed instability / Surgical
- Management
- ICU monitoring / Revision
- Risk Factor
- Osteoporosis / Poor fixation
- Management
- Revision surgery
- Risk Factor
- Inadequate correction
- Management
- Extension osteotomy / Revision
- Risk Factor
- Fusion
- Management
- Surveillance / Revision
- Risk Factor
- Anterior approach
- Management
- Usually transient / SLP
Postoperative Care and Rehabilitation
Rehabilitation Timeline
ICU monitoring: Especially if cord injury, MAP goals
Collar: Rigid cervical collar
DVT prophylaxis: Mechanical + chemical (if no contraindication)
Mobilization: Early mobilization if neurologically intact
Collar: Continue rigid collar
X-ray: 6-week check for fusion
Rehabilitation: Spinal cord rehab if injury
Activity: Avoid heavy lifting, contact sports
If fusion: May remove collar
X-ray: Confirm fusion
Activity: Gradual return to activities
Follow-up: Flexion-extension X-rays
Outcomes and Prognosis
- Key Outcomes
- Guarded prognosis, high permanent neurological deficit
- Notes
- Poor recovery even with surgery, anterior cord syndrome common
- Key Outcomes
- Excellent prognosis with conservative care
- Notes
- 95%+ heal with collar, rarely need surgery
- Key Outcomes
- 90%+ with modern instrumentation (ACCF)
- Notes
- High success with anterior corpectomy and fusion
Neurological status at presentation is the strongest predictor of outcome. Flexion teardrop has guarded prognosis with high rate of permanent neurological deficit. Extension teardrop has excellent prognosis with conservative treatment. Fusion rates are high (90%+) with modern anterior corpectomy and fusion techniques.
Guidelines, Registries & Global Practice
- Diving/shallow-water injuries: Pooled series report spinal cord injury in over 90% of cases, with roughly two-thirds left with permanent neurological deficit (Griepp 2022)
- Demographics: Flexion teardrop predominantly young males in high-energy trauma; extension teardrop in elderly, often osteoporotic or with cervical spondylosis
- Incidence: Diving-related cord injury estimated at approximately 1 per million population per year in temperate climates (Schwarz, Austria)
- Level: C5 and C6 are the most commonly affected segments for both types
- SLIC (Vaccaro 2007): score of 4 or more favours surgery; threshold widely adopted globally
- AOSpine subaxial (2016): A/B/C morphology, facet descriptor and neurology - the common international language alongside SLIC
- C-spine clearance: NEXUS and Canadian C-Spine Rule guide imaging triage; CT is the standard in obtunded or high-risk patients
- MRI: Required to assess DLC, disc and cord before declaring an injury stable
- Position on Subaxial Cervical Trauma
- Morphology-based A/B/C classification; encourages structured severity scoring to guide operative decisions
- Position on Subaxial Cervical Trauma
- Closed reduction and timing guidance for cervical SCI; supports early reduction of malalignment in awake patients
- Position on Subaxial Cervical Trauma
- Suggests decompression within 24 hours for acute traumatic cervical SCI where feasible (informed by STASCIS)
- Position on Subaxial Cervical Trauma
- Spinal injury major-trauma pathway: CT first-line for significant mechanism, MRI for cord/ligament assessment, transfer to spinal-capable centre
- Position on Subaxial Cervical Trauma
- Endorses SLIC and AOSpine for communication and surgical triage of subaxial injuries
- Rapid CT/MRI access, ICU with MAP-targeted cord perfusion
- Early (within 24h) decompression and instrumented anterior/posterior fusion
- Specialist spinal cord rehabilitation pathways
- Imaging may rely on plain films plus limited CT; MRI access constrained
- Traction (Gardner-Wells tongs) and halo/orthosis play a larger role when timely surgery is unavailable
- Emphasis on transfer to a spine-capable centre and prevention of secondary cord injury during handling
Key clinical-governance points (apply globally):
- Document mechanism (diving, fall, MVC) and a full ASIA/ISNCSCI neurological assessment at presentation
- State the teardrop type (flexion vs extension), the SLIC/AOSpine grade, and the rationale
- Counsel on surgical vs conservative options, expected outcomes and the guarded prognosis of cord injury
- Record informed consent including dysphagia, recurrent laryngeal/hypoglossal nerve injury, vascular injury, dural tear, non-union and the small risk of neurological deterioration
Controversies and Areas of Uncertainty
STASCIS supports decompression within 24 hours, but it was a non-randomised cohort and the benefit is clearest in incomplete injuries. The practical "ultra-early" (under 12h) target and its benefit in complete injuries remain debated, and logistics often dominate real-world timing.
A single anterior corpectomy addresses the burst body and retropulsion, but the threshold for adding posterior fixation (degree of kyphosis, facet injury, PLC failure, osteoporosis) is not standardised and varies by surgeon and registry.
There is no validated cut-off separating a benign avulsion from an unstable hyperextension injury. MRI assessment of the disc and ALL is operator-dependent, and delayed instability is occasionally reported, justifying interval flexion-extension films.
High-dose methylprednisolone remains contentious. Several guidelines no longer recommend it routinely because the marginal neurological benefit is outweighed by infective and metabolic complications; practice varies widely between regions.
MCQ Practice Points
Q: What is the key difference between flexion and extension teardrop fractures? A: Flexion teardrop is a BURST injury (3-column, unstable, surgery needed). Extension teardrop is an AVULSION (anterior column only, usually stable, conservative). The teardrop fragment looks similar but the injuries are vastly different.
Q: What is the classic mechanism for flexion teardrop fracture? A: Diving into shallow water - axial load through the vertex with the neck in flexion. This mechanism causes the burst injury pattern.
Q: What CT finding differentiates flexion from extension teardrop? A: Sagittal split through the vertebral body in flexion teardrop (key finding!). The body is comminuted/burst. In extension, the body is intact with just an avulsion fragment.
Q: What is the typical SLIC score for flexion teardrop fractures? A: 6-10 points (morphology 3-4 + DLC 2 + neurology 2-4) - well above the surgical threshold of 4. Extension teardrop typically scores 1-3 (usually conservative).
Q: What is the surgical treatment for flexion teardrop fractures? A: Anterior cervical corpectomy and fusion (ACCF) - remove fractured vertebra, decompress canal, structural graft, anterior plate. May add posterior stabilization if severe kyphosis or posterior instability.
Q: What cord syndrome is commonly associated with flexion teardrop? A: Anterior cord syndrome - loss of motor, pain, and temperature below the level, preserved proprioception and vibration. Complete cord injury is also common.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old male is brought in after diving into shallow water. He is quadriplegic with no motor or sensory function below C5. GCS 15, breathing spontaneously. What is your assessment and management?”
“A 78-year-old female presents after a fall with hyperextension of her neck. She has neck pain but no weakness or numbness. X-ray shows a small teardrop fragment at C5. What is your diagnosis and management?”
“You are shown two lateral C-spine X-rays both showing a teardrop fragment. One is from a 25-year-old diver, the other from a 75-year-old who fell. How do you differentiate flexion from extension teardrop?”
Key Anatomy
- Teardrop fragment = triangular anteroinferior vertebral body fragment
- Flexion = burst injury (3-column), extension = avulsion (anterior column)
- C5-C6 = most common level for both types
- Posterior ligamentous complex (PLC) = determines stability
Classification
- Flexion teardrop = BURST (unstable, surgery), extension = AVULSION (stable, conservative)
- SLIC score: Flexion 6+ (surgery), extension 1-3 (conservative)
- Sagittal split on CT = key finding for flexion teardrop
- Body intact on CT = extension teardrop
Treatment Algorithm
- Flexion teardrop: Anterior corpectomy and fusion (ACCF), may add posterior
- Extension teardrop: Rigid collar 6-8 weeks, excellent prognosis
- SLIC greater than 4 = surgery recommended
- MRI essential to assess DLC and cord
Surgical Pearls
- ACCF: Remove fractured vertebra, decompress canal, structural graft, anterior plate
- May add posterior stabilization if severe kyphosis or posterior instability
- Protect during positioning - Mayfield clamp, neutral alignment
- High fusion rates (90%+) with modern instrumentation
Complications
- Neurological deterioration: Missed instability, surgical complication
- Nonunion: Osteoporosis, poor fixation - revision surgery
- Kyphosis: Inadequate correction - extension osteotomy
- Dysphagia: Anterior approach - usually transient
Evidence Base and Key Trials
SLIC - Original Classification (Spine Trauma Study Group)
- Defined the Subaxial Injury Classification and Severity Scale (SLIC) from three weighted categories: injury morphology, disco-ligamentous complex (DLC), and neurological status
- Multicentre reliability study, 20 spine surgeons scoring 11 trauma cases on two occasions
- Interrater intraclass correlation: morphology 0.57, DLC 0.49, neurology 0.87; raters agreed with the algorithm treatment recommendation in 93.3% of cases
- Reliability compared favourably with the older Harris and Allen-Ferguson mechanistic systems
SLIC-Based Surgical Approach Algorithm
- Evidence-based algorithm linking SLIC injury type to surgical approach (anterior, posterior, or combined)
- Burst/compression and distraction injuries are more often amenable to a single anterior approach
- Severe translation/rotation injuries more commonly require a posterior or combined antero-posterior approach
- Designed to answer the two core questions: should I operate, and which approach do I choose?
SLIC Scored Injuries - Literature Analysis
- Systematic review (2007-2014) mapping specific injury patterns onto SLIC scores and resulting treatment
- SLIC 1-3: neurologically intact spinous-process, laminar, small facet, compression and burst fractures - non-operative
- SLIC 4: indeterminate zone, e.g. central cord syndrome, incomplete deficits, burst with complete deficit
- SLIC 5-10: distraction/rotational injuries, traumatic disc herniation with deficit, burst with incomplete deficit - operative
AOSpine Subaxial Cervical Classification
- Morphology-based system mirroring the thoracolumbar scheme: A (compression), B (tension band), C (translational), plus facet (F) descriptors, patient modifiers and neurology
- Substantial intra- and interobserver reliability (kappa 0.75 intraobserver, 0.64 interobserver)
- A flexion teardrop is typically an A3/A4 compression-burst, often with a tension-band (B) or translational (C) component when posteriorly unstable
- An extension teardrop avulsion is usually a low-grade A0/A1 anterior compression injury
STASCIS - Early vs Delayed Decompression
- Prospective multicentre cohort of 313 acute cervical SCI patients comparing decompression before vs after 24 hours
- 19.8% of the early-surgery group improved by 2 or more ASIA grades at 6 months vs 8.8% in the late group
- Adjusted odds of a 2-grade AIS improvement were 2.8 times higher with early surgery (OR 2.83, 95% CI 1.10-7.28)
- Complication rates were similar (24.2% early vs 30.5% late)
ISNCSCI - International Standards for Neurological Classification
- Defines the ASIA/ISNCSCI examination: motor and sensory levels, neurological level of injury, and the ASIA Impairment Scale (AIS A-E)
- Distinguishes complete (AIS A) from incomplete injuries and codifies the zone of partial preservation
- Provides the standard framework underpinning prognostic and trial endpoints in SCI
- Anterior cord syndrome and central cord syndrome are defined incomplete clinical patterns within this standard
Diving and Breaking-Wave Cervical Injuries
- Single-centre series plus PRISMA systematic review (534 pooled patients, mean age 45.4 years) of shallow-water cervical injuries
- 94.2% of pooled patients sustained a spinal cord injury
- An estimated 64.8% had permanent neurological injury and 12.5% permanent quadriplegia on follow-up
- Diving mechanism, AOSpine subaxial injury score over 10, and cord signal change all predicted disability or death at 12 months
Flexion Teardrop - Imaging and Radiological Features
- Illustrated case of multilevel flexion teardrop fractures (C3, C5, C6) in an 82-year-old after a fall
- MRI showed anteroinferior endplate-corner fractures with focal kyphosis, marrow oedema, anterior longitudinal ligament disruption and canal stenosis
- Emphasises that the teardrop fragment is a marker of a more extensive flexion-compression injury
- Highlights the role of MRI in defining ligamentous and cord involvement