Wear Rates | Particle Disease | Material Properties | Patient Selection
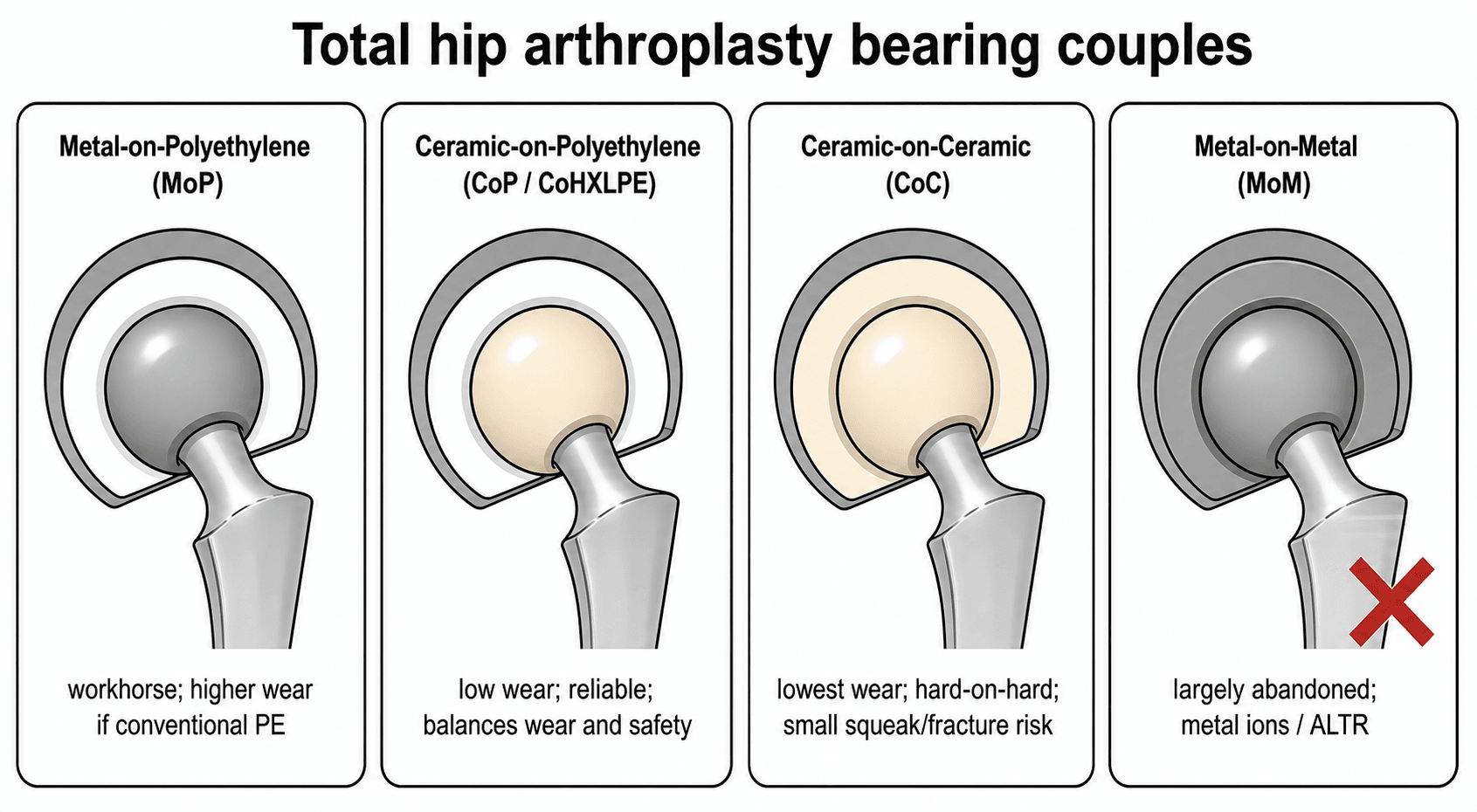
- HXLPE (highly cross-linked polyethylene) has replaced conventional PE - 90% reduction in wear
- Ceramic-on-ceramic has lowest wear but risk of squeaking (1-5%) and fracture (rare under 0.1%)
- Metal-on-metal failed due to ALVAL (pseudotumor), metallosis, high revision rates - essentially abandoned
- Dual mobility reduces dislocation by 50-75% - excellent for instability risk
- Particle disease (osteolysis) driven by volume and biologic activity of wear debris
- “HXLPE is standard - cross-linking reduces wear but decreases mechanical properties
- “Large heads (36mm+) reduce dislocation but increase volumetric wear in MoP
- “Ceramic has excellent wear but brittleness - avoid in high-impact activities
- “MoM abandoned due to ALVAL - chromium and cobalt ion release causes pseudotumor
Highly cross-linked polyethylene (HXLPE) has replaced conventional PE in over 90% of THAs. Irradiation cross-linking reduces wear by 90% but decreases fatigue strength. Not recommended for thinner liners (under 6mm). AOANJRR shows excellent survivorship.
Ceramic-on-ceramic has lowest wear (4-5 micrometers/year) but carries risk of squeaking (1-5%) and fracture (under 0.1%). Modern generation ceramics (alumina matrix composite, Biolox Delta) have lower fracture risk than older alumina.
Metal-on-metal failed catastrophically. Chromium/cobalt ion release causes ALVAL (aseptic lymphocytic vasculitis-associated lesion) with pseudotumor formation, soft tissue destruction. MHRA issued alerts 2010-2012. Essentially abandoned globally. Know surveillance protocols for legacy patients.
Osteolysis results from macrophage response to wear particles. Polyethylene particles (0.1-10 micrometers) are most osteolytic per particle, but volume matters. HXLPE dramatically reduced osteolysis rates. Size, number, and biologic activity all contribute.
- First Choice
- MoP (metal-on-HXLPE), 32-36mm head
- Alternative
- Ceramic-on-HXLPE if young end of range
- Avoid
- MoM (obsolete)
- First Choice
- Ceramic-on-ceramic or Ceramic-on-HXLPE
- Alternative
- MoP with large HXLPE head (36mm+)
- Avoid
- Conventional PE, thin liners
- First Choice
- Dual mobility (MoP or Ceramic-on-HXLPE)
- Alternative
- Large head MoP (36-40mm) with constraint
- Avoid
- Small heads (under 32mm)
- First Choice
- MoP (HXLPE), ceramic-on-HXLPE
- Alternative
- Reinforced ceramic-on-ceramic (Biolox Delta)
- Avoid
- Older generation ceramics, conventional PE
- First Choice
- Ceramic-on-ceramic or Ceramic-on-HXLPE
- Alternative
- Oxidized zirconium-on-HXLPE
- Avoid
- MoP (standard cobalt-chrome), MoM
HXLPEHXLPE - Properties of Highly Cross-Linked Polyethylene
Hook:HXLPE is the modern standard but remember the minimum thickness requirement
ALVALALVAL - Metal-on-Metal Failure Mechanism
Hook:ALVAL is the devastating complication that ended MoM - know it for legacy patient surveillance
Overview and Historical Context
Bearing surface selection is one of the most important decisions in total hip arthroplasty, directly impacting longevity, wear, particle disease, and revision risk. The evolution of bearing surfaces reflects advances in materials science and hard-earned lessons from clinical failures.
Historical evolution:
- 1960s-1990s: Charnley's metal-on-conventional polyethylene (MoP) established the gold standard
- 1970s-1980s: First ceramic bearings introduced (alumina-on-alumina)
- 1990s-2000s: Metal-on-metal (MoM) resurgence for large heads and young patients
- 2000s: Introduction of highly cross-linked polyethylene (HXLPE)
- 2010-2012: MoM catastrophic failure - MHRA alerts, widespread abandonment
- 2010s-present: HXLPE becomes standard, ceramic refinements, dual mobility expansion
Sir John Charnley's low-friction arthroplasty using metal femoral head on polyethylene acetabular component with bone cement established THA as a reliable procedure. His principle of low friction (small 22mm head) minimized wear but increased dislocation risk - modern surgery balances these competing factors.
- Metal-on-HXLPE: 70-80% of primary THAs globally (most common)
- Ceramic-on-HXLPE: 10-15% (growing in young patients)
- Ceramic-on-ceramic: 5-10% (selected young patients)
- Dual mobility: 5-10% in primary THA, higher in revision (20-30%)
- Metal-on-metal: Less than 1% (legacy cases, essentially abandoned)
The AOANJRR provides world-leading registry data on bearing surface performance. Key findings inform global practice patterns and exam answers.
Anatomy and Biomechanics - Tribology Fundamentals
Tribology fundamentals:
Tribology is the science of friction, wear, and lubrication. In THA, the bearing surface operates under:
- Loads: 2-8x body weight during gait
- Cycles: 1-2 million cycles per year for active patient
- Lubrication: Synovial fluid (boundary and fluid film lubrication)
Wear mechanisms:
- Adhesive wear: Material transfer between surfaces
- Abrasive wear: Hard particles (cement, bone, metal) scratch softer surface
- Fatigue wear: Cyclic loading causes subsurface crack propagation
- Corrosion: Electrochemical degradation (especially in MoM)
The Stribeck curve describes lubrication regimes. THA operates in mixed lubrication (boundary + fluid film). Large heads with good clearance promote fluid film lubrication, reducing wear. This explains why proper component positioning and head size selection matter.
Material properties critical for bearings:
- Hardness (HV)
- Low (20-30)
- Elastic Modulus (GPa)
- 1
- Fracture Toughness
- High (ductile)
- Hardness (HV)
- High (400-500)
- Elastic Modulus (GPa)
- 210
- Fracture Toughness
- Moderate
- Hardness (HV)
- Very High (2000+)
- Elastic Modulus (GPa)
- 380
- Fracture Toughness
- Low (brittle)
- Hardness (HV)
- Very High (2000+)
- Elastic Modulus (GPa)
- 358
- Fracture Toughness
- Moderate (improved)
- Hardness (HV)
- High (1300+)
- Elastic Modulus (GPa)
- 200
- Fracture Toughness
- Moderate
Head size effects:
- Small heads (22-28mm): Low volumetric wear, high dislocation risk, limited ROM
- Large heads (36-40mm+): Low dislocation risk, high ROM, increased volumetric wear in MoP
- Optimal balance: 32-36mm for most patients with HXLPE
The relationship between head size and wear is complex - linear wear rate may increase slightly but dislocation risk decreases significantly.
Linear versus Volumetric Wear - and Why Head Size Matters
Two different measures of wear are quoted throughout this topic, and they behave very differently with head size:
- Definition
- Depth the head sinks into the liner
- Units
- mm per year
- Relationship to head size
- Roughly independent of head diameter
- Definition
- Total volume of debris removed
- Units
- cubic mm per year
- Relationship to head size
- Rises with the square of the head radius
For a given linear penetration, volumetric wear is proportional to the square of the femoral head radius (the swept worn area scales with radius squared). Doubling the head size therefore generates far more debris for the same depth of penetration. Because osteolysis is driven by the volume and number of particles, this single geometric fact explains the central head-size dilemma:
- With conventional polyethylene, large heads produced prohibitive volumetric wear and osteolysis - which is why historic practice favoured small (22-28mm) heads despite their dislocation risk.
- With HXLPE, linear wear is so low (roughly 0.01 to 0.05mm per year) that even a 36mm head generates an acceptable debris volume - which is exactly why modern surgery can use 32-36mm heads to gain stability without paying a wear penalty.
This geometry reconciles the whole topic: large heads improve stability but, for a given linear wear rate, generate volumetric debris in proportion to the square of the radius. Conventional PE could not tolerate this, so heads were kept small; HXLPE's order-of-magnitude lower linear wear is what made 32-36mm heads safe. Always frame head-size selection as a stability-versus-volumetric-wear trade-off.
The Stability Side of Head Size: Jump Distance and Head-Neck Ratio
If volumetric wear is the cost of a larger head, stability is the benefit, and it too is geometric:
- Jump distance is the distance the head centre must travel to escape the cup - approximately the head radius (about half the diameter) for a hemispherical cup. A larger head has a larger jump distance, so it must sublux further before it dislocates. This is the primary reason larger heads, and the large effective outer head of a dual-mobility bearing, resist dislocation.
- Head-neck ratio (head diameter divided by neck diameter) governs the primary arc of motion - the range of movement before the neck impinges on the rim. A higher ratio allows more impingement-free motion before the neck levers the head out (the secondary, impingement mechanism of dislocation). Larger heads and skirtless, reduced-diameter necks raise this ratio.
Two geometric mechanisms: a larger head has a greater jump distance (approximately one head radius must be traversed to dislocate) and a higher head-neck ratio, giving a wider impingement-free arc before the neck levers the head out. Dual mobility exploits both by creating a very large effective outer head. This is the stability counterpart to the volumetric-wear penalty - and the reason 32-36mm HXLPE heads are the modern compromise.
Classification Systems - Bearing Surface Types
- Ultra-high molecular weight polyethylene (UHMWPE)
- Gamma sterilization in air
- Wear rate: 0.1-0.2mm per year (linear)
- Volumetric wear increases with head size
- Particle disease: 0.1-10 micrometer particles highly osteolytic
- Osteolysis: 10-40% at 10-15 years
- Revision for wear: Leading cause of late THA failure
- Oxidative degradation: Free radicals from sterilization cause aging
- Essentially obsolete in primary THA
- May still be used in constrained liners (better mechanical properties)
- Historical importance for understanding particle disease
Conventional PE taught us about particle disease but has been superseded by HXLPE.
Clinical Assessment - Patient Evaluation for Bearing Selection
Pre-operative assessment for bearing choice:
The selection of bearing surface is a critical decision that should be individualized based on comprehensive patient assessment. This is typically done during pre-operative consultation once THA is indicated.
Patient factors to assess:
- Assessment
- Longevity requirements, life expectancy
- Bearing Implications
- Under 50: ceramic options. Over 65: MoP standard
- Assessment
- Sports, occupation, daily demands
- Bearing Implications
- High activity: ceramic-on-HXLPE or CoC. Standard: MoP
- Assessment
- Prior dislocation, abductor deficiency, neurologic
- Bearing Implications
- High risk: dual mobility first choice
- Assessment
- Previous reactions, implant sensitivity
- Bearing Implications
- Avoid MoP if severe. Choose ceramic-on-ceramic or CoP
- Assessment
- Weight optimization, liner thickness concerns
- Bearing Implications
- Obesity: ensure adequate liner thickness (over 6mm)
- Assessment
- Acceptance of squeak risk, cost considerations
- Bearing Implications
- Discuss ceramic squeak risk. Balance expectations
- Age and life expectancy: Critical for longevity planning
- Activity goals: What activities does patient want to return to?
- Prior joint replacements: Experience with previous bearings
- Allergy history: Metal sensitivity, implant reactions
- Neuromuscular conditions: Parkinson's, stroke, dementia (dual mobility indication)
- Falls risk: Cognitive impairment, balance disorders
- Expectations: What has patient heard about different bearings?
- BMI: Obesity affects liner thickness calculations
- Hip pathology: Dysplasia, bone loss may affect cup size
- Abductor function: Weakness indicates dual mobility consideration
- Neuromuscular examination: Spasticity, tremor, weakness
- Spinopelvic alignment: Fixed deformities affect stability (dual mobility)
- X-rays: Bone quality, acetabular anatomy, dysplasia
- CT if complex anatomy: For accurate component sizing
- Acetabular dimensions: Estimate cup size for liner thickness calculations
- Metal allergy → Exclude MoP
- High dislocation risk → Dual mobility
- Very young (under 40) → Avoid conventional PE
- MoM → Never use (obsolete)
- Under 50 years → Ceramic options (CoC or CoP)
- 50-65 years → Ceramic-on-HXLPE or MoP
- Over 65 years → MoP standard (cost-effective)
- Ceramic: Squeak risk (1-5%), fracture risk (under 0.1%), best wear
- HXLPE: Proven standard, no special risks, excellent outcomes
- Dual mobility: IPD risk (under 1%), excellent stability
- Cost considerations (ceramic 2-3x more expensive)
- Tolerance for squeak risk
- Activity goals
- Revision aversion (ceramic best longevity for young)
Bearing selection should be shared decision-making between surgeon and patient. Present options appropriate for the patient's profile, discuss risks/benefits, incorporate patient values. Document discussion and rationale in medical record. This is especially important for ceramic bearings (squeak risk) and dual mobility (IPD risk).
- HXLPE standard: "This is the proven standard bearing with excellent long-term results"
- Ceramic options: "Lower wear for your young age, but 1-5% risk of squeaking which is usually benign"
- Dual mobility: "Dramatically reduces your dislocation risk given your risk factors"
- Activity modification: All bearings require avoiding high-impact sports
- Bearing choice and rationale
- Discussion of alternatives
- Patient understanding and agreement
- Special considerations (allergy, dislocation risk)
Clinical assessment for bearing selection is a systematic process balancing patient factors, surgeon experience, and evidence-based outcomes.
Ceramic Bearing Options - Hard-on-Hard Surfaces
- 1st generation (1970s): Pure alumina - high fracture risk (up to 1%)
- 2nd generation (1990s): Improved alumina - fracture risk 0.2-0.5%
- 3rd generation (2000s): High-purity alumina (Biolox Forte) - fracture under 0.1%
- 4th generation (2010s+): Alumina matrix composite (Biolox Delta) - fracture under 0.01%
- Alumina matrix with zirconia platelets for crack resistance
- 20-25% higher strength than pure alumina
- Maintains low wear characteristics
- Lowest wear rate: 4-5 micrometers/year (10-20x less than HXLPE)
- Minimal particle disease: Ceramic particles less biologically active
- Hydrophilic surface: Better fluid film lubrication
- Excellent longevity potential: Ideal for young patients (under 50)
- Squeaking: 1-5% incidence (multifactorial)
- Fracture risk: Under 0.1% with modern ceramics but catastrophic if occurs
- Stripe wear: With component malposition or microseparation
- Cost: 2-3x more expensive than MoP
- Surgical technique demands: Impaction technique critical, no ceramic damage
Ceramic fracture is rare but devastating. Metal particles embedded in surrounding tissue make revision extremely difficult. All ceramic debris must be removed, usually requiring ceramic-on-HXLPE or MoP at revision. Prevention: avoid high-impact activities (rugby, martial arts), ensure perfect impaction technique.
- Stripe wear from edge loading (component malposition)
- Microseparation during gait
- Impingement causing lever-out
- Patient factors: Thin patients, high activity
- Most squeaking is benign - not associated with higher revision rates
- Young patients (under 50) with high longevity requirements
- High activity level but not extreme impact sports
- Patient accepts squeak risk after counseling
- High-impact sports (rugby, parachuting, martial arts)
- Significant component malposition anticipated
- Patient unwilling to accept squeak risk
CoC offers the best wear performance but demands perfect technique and patient selection.
CERAMICCERAMIC - Ceramic Bearing Considerations
Hook:CERAMIC benefits and risks - lowest wear but squeaking and fracture potential
Investigations - Bearing Performance Assessment
The rise and catastrophic fall of metal-on-metal:
Historical rationale (1990s-2000s):
- Large head sizes possible (up to 60mm+) for stability
- Low volumetric wear (self-polishing with use)
- Young active patients with metal-on-metal resurfacing
- Appeared to solve PE particle disease problem
Why MoM failed - the ALVAL disaster:
Metal-on-metal is essentially abandoned due to devastating soft tissue reactions. This is one of the greatest failures in modern arthroplasty. Know this for exam - what went wrong, how to surveil legacy patients, and why it failed despite promising early wear data.
- Metal ion release: Chromium and cobalt ions from tribocorrosion and wear
- ALVAL (Aseptic Lymphocytic Vasculitis-Associated Lesion):
- Type IV delayed hypersensitivity reaction
- Lymphocytic infiltration, tissue necrosis
- Pseudotumor formation (fluid-filled or solid mass)
- Soft tissue destruction: Muscles, tendons, nerves destroyed by pseudotumor
- Metallosis: Metal staining of tissues
- Pseudotumor on MRI or ultrasound
- Pain disproportionate to radiographic findings
- Elevated metal ions: Cobalt and chromium in blood
- Soft tissue mass may be palpable
- Implant may appear well-fixed on X-ray - soft tissue problem
- Medical Device Alert issued warning of high failure rates
- Surveillance protocols mandated for all MoM patients
- Many systems recalled or withdrawn from market
- Class action lawsuits (DePuy ASR, Smith & Nephew BHR)
- Investigations
- Metal ions (Co, Cr), clinical assessment
- Threshold for Action
- Ions over 7 ppb (parts per billion)
- Investigations
- MRI MARS (metal artifact reduction sequence)
- Threshold for Action
- Pseudotumor present, or growing
- Investigations
- Metal ions annually + MRI if symptomatic
- Threshold for Action
- Lower threshold for imaging
- Investigations
- Symptomatic + pseudotumor, or ions over 20 ppb
- Threshold for Action
- Revision even if asymptomatic with large/growing tumor
Revision surgery for MoM failure:
- Complete debridement of all necrotic tissue and metallosis
- Ceramic or polyethylene liner (never metal again)
- Large head removal - may need smaller head for adequate liner thickness
- Soft tissue reconstruction may be needed (abductor repair common)
- Outcomes poor if severe tissue destruction
Viva scenario: "A patient with MoM THA from 2008 presents with hip pain and cobalt ion level of 15 ppb. Management?" Answer: (1) This MoM bearing is at risk for ALVAL. (2) Order MRI MARS protocol to assess for pseudotumor. (3) If pseudotumor present, proceed to revision with complete debridement and bearing change. (4) If no tumor, close surveillance and consider revision if symptoms progress or ions increase. (5) Counsel re: failed technology.
- Demonstrates importance of long-term surveillance and registry data
- Example of biologic response mattering more than wear volume
- Know ALVAL pathophysiology and surveillance protocols
- Legacy patient management - many still have MoM implants
- Less than 1% of new THAs (essentially obsolete)
- Used only in rare circumstances (metal allergy with ceramic unavailable)
- Focus now on managing legacy patients with surveillance and revision
Metal-on-metal is a cautionary tale of technology adoption without adequate long-term data.
Dual Mobility Bearings
- Small femoral head (22-28mm) articulates with polyethylene liner
- Large outer diameter (typically 36-42mm+) articulates with metal shell
- Two articulations: Small inner (primary), large outer (secondary)
- Results in large effective head size for stability
- Large head-to-neck ratio: Increased ROM before impingement
- Two centers of rotation: Impingement causes rotation, not dislocation
- Effective head diameter: 36-44mm equivalent for jump distance
- Retained ROM: Better than constrained liners
- High dislocation risk patients:
- Revision THA (50-75% dislocation reduction)
- Prior dislocation
- Neuromuscular disorders (Parkinson's, stroke, dementia)
- Abductor deficiency
- Tumor resection
- Spinal deformity or fusion
- Primary THA in selected patients:
- Elderly with cognitive impairment
- High fall risk
- Unable to comply with precautions
Dual mobility reduces dislocation rates by 50-75% in high-risk patients. AOANJRR shows 1-2% dislocation rate with dual mobility vs 3-5% with standard bearings in revision THA. This is the primary indication - instability prevention, not treatment of all patients.
- Standard: Cobalt-chrome head on HXLPE liner
- Ceramic-on-HXLPE: Ceramic head for lower wear
- All have metal shell outer bearing (shell-liner interface)
-
Intraprosthetic dislocation (IPD):
- Liner dissociates from head (rare, under 1%)
- Usually from impingement or liner manufacturing issue
- Requires open reduction (closed fails)
- May need revision if recurrent
-
Dual wear surfaces:
- Inner bearing (head-liner): Low wear with HXLPE
- Outer bearing (liner-shell): Concerns about wear
- Total wear slightly higher than single bearing
- Long-term data reassuring (over 20 years European experience)
-
Metallosis from outer bearing:
- Early designs had metal-on-metal outer bearing issues
- Modern designs with retentive rim reduce motion at outer bearing
- Most wear occurs at inner bearing
- Revision THA: Dual mobility significantly lower dislocation and revision rates
- Primary THA: Growing use, excellent outcomes in high-risk patients
- No increase in aseptic loosening or late complications
- Trend toward increased adoption (currently 5-10% of primary, 20-30% revision)
- Avoid impingement (main cause of IPD)
- Ensure snap-fit of liner into head (manufacturer-specific technique)
- Component position standard targets (cup 40 degrees abduction, 15-20 anteversion)
- Can't use constrained liner with dual mobility (different concept)
- Some surgeons advocate routine use in all elderly patients
- Ceramic-on-HXLPE dual mobility may further reduce wear
- Improved outer bearing surfaces under development
Dual mobility is a major advance for instability prevention - know indications and IPD complication.
Wear Mechanisms and Particle Disease
Wear debris generation:
Particle size and biologic response:
- Size Range
- 0.1-10 micrometers
- Biological Response
- Highly osteolytic per particle
- Clinical Effect
- Osteolysis (main concern with conventional PE)
- Size Range
- Under 0.1 micrometers (nanometer)
- Biological Response
- Low biological activity
- Clinical Effect
- Minimal osteolysis
- Size Range
- 20-100 nanometers
- Biological Response
- ALVAL/hypersensitivity (ions)
- Clinical Effect
- Pseudotumor, tissue destruction
- Size Range
- 1-100 micrometers
- Biological Response
- Moderate inflammatory
- Clinical Effect
- Interface osteolysis
The osteolysis cascade:
- Wear particles enter periprosthetic tissue through joint capsule, screw holes, thin implant-bone interface
- Macrophage activation: Particles phagocytosed by macrophages
- Cytokine release: TNF-alpha, IL-1, IL-6, RANKL
- Osteoclast activation: RANK-RANKL pathway
- Bone resorption: Progressive osteolysis
- Implant loosening: Loss of fixation from bone loss
The effective joint space is the path particles can travel - joint capsule, screw holes, thin bone-implant interface. Particles accumulate at weak points (stress risers, thin cement mantle, uncemented ingrowth surfaces). Granuloma formation causes progressive osteolysis and eventual loosening.
- Particle volume: Total amount of wear debris (HXLPE dramatically reduces this)
- Particle size: 0.1-10 micrometers most osteolytic
- Particle shape: Elongated worse than round
- Patient biology: Some patients more susceptible (genetic factors)
- Time: Cumulative exposure (why young patients at highest risk historically)
- Implant design: Access of particles to bone
- 95% reduction in osteolysis at 10-year follow-up vs conventional PE
- Osteolysis rates now under 5% at 15 years (vs 30-40% historical)
- Transformed THA outcomes in young patients
- Most osteolysis now from other sources: cement, metal debris, backside wear
- Occurs when liner micromotion against metal shell
- Locking mechanism critical
- Diagnosis: Increasing metallosis without obvious bearing wear
- Prevention: Adequate liner locking, avoid thin liners (under 3-4mm backside thickness)
- Cement particles, bone chips, metal debris from components
- Scratch polyethylene surface
- Accelerate wear dramatically
- Prevention: Meticulous surgical technique, thorough lavage, avoid cement extrusion
WEARWEAR - Factors Affecting Bearing Surface Wear
Hook:WEAR factors - remember it's not just the material but also mechanical environment
Management Algorithm
Standard patient (over 65, average activity):
First choice: Metal-on-HXLPE (32-36mm head)
- Most proven long-term data (HXLPE over 15 years)
- Lowest revision rates in registry data
- Excellent wear performance (0.01-0.05mm/year)
- Cost-effective
- Forgiving of minor malposition
- 32mm: Good balance, most common
- 36mm: Slightly more stability, acceptable wear with HXLPE
- Avoid under 28mm (dislocation risk) or over 40mm (potential wear concerns)
Alternative: Ceramic-on-HXLPE
- If patient younger end of range (65-70)
- If long life expectancy
- Slightly better wear than MoP
- No squeak risk vs CoC
Avoid:
- Conventional PE (obsolete)
- MoM (failed technology)
- CoC (unnecessary in this age group)
- Dual mobility (unless instability risk factors)
For most patients over 65, MoP (HXLPE) with 32-36mm head is the gold standard.
Surgical Technique - Bearing-Specific Considerations
- Calculate minimum liner thickness: (cup ID - head OD) / 2 = must be over 6mm
- Example: 54mm cup, 36mm head = (54-36)/2 = 9mm thickness (safe)
- Example: 48mm cup, 36mm head = (48-36)/2 = 6mm thickness (marginal)
- Choose smaller head or larger cup if thickness under 6mm
- Ensure complete seating (listen for snap/feel for stable rim lock)
- Check locking mechanism integrity
- Avoid backside damage (scratches accelerate backside wear)
- Some systems require specific impaction technique
- Clean Morse taper thoroughly (no blood, debris)
- Align head with taper, single firm strike
- Avoid repeated impaction (damages taper)
- Test stability before closure
- Liner won't seat: Check for debris, shell deformation
- Head won't lock: Check taper damage, blood contamination
- Backside scratches: Consider liner replacement if severe
Standard HXLPE technique is straightforward and forgiving.
Complications Specific to Bearing Surfaces
- Specific Complication
- Osteolysis/particle disease
- Incidence
- 30-40% at 15 years
- Management
- Revision with HXLPE, bone grafting
- Specific Complication
- Liner fracture (thin liners)
- Incidence
- Under 1% if adequate thickness
- Management
- Revision, ensure minimum 6mm
- Specific Complication
- Squeaking
- Incidence
- 1-5%
- Management
- Usually benign, revision if severe/painful
- Specific Complication
- Fracture (modern)
- Incidence
- Under 0.1%
- Management
- Revision, all debris removal, MoP or CoP
- Specific Complication
- Stripe wear
- Incidence
- 1-3% with malposition
- Management
- May progress to fracture, revise if progressive
- Specific Complication
- ALVAL/pseudotumor
- Incidence
- 10-30% at 10 years
- Management
- Revision with debridement, bearing change
- Specific Complication
- Intraprosthetic dislocation
- Incidence
- Under 1%
- Management
- Open reduction, may need revision
- Specific Complication
- Dislocation
- Incidence
- 1-5% (lower with DM/large heads)
- Management
- Closed reduction, address instability
Differential diagnosis of the painful or noisy THA by bearing-related cause:
- Typical Bearing/Setting
- Metal-on-metal (legacy)
- Key Distinguishing Features
- Pain out of proportion to X-ray, soft-tissue mass, well-fixed components
- Confirmatory Test
- Cobalt/chromium ions raised, MARS MRI shows pseudotumour
- Typical Bearing/Setting
- Conventional PE (and late HXLPE)
- Key Distinguishing Features
- Often asymptomatic until late; expansile periprosthetic lucencies
- Confirmatory Test
- Serial radiographs / CT showing lytic lesions
- Typical Bearing/Setting
- Ceramic-on-ceramic
- Key Distinguishing Features
- Audible noise on specific movements, usually pain-free
- Confirmatory Test
- Component-position analysis (CT), often benign
- Typical Bearing/Setting
- Ceramic-on-ceramic / ceramic head
- Key Distinguishing Features
- Acute pain, grinding, sudden noise, metallosis
- Confirmatory Test
- Radiograph/CT showing fractured component
- Typical Bearing/Setting
- Dual mobility
- Key Distinguishing Features
- Dislocation that cannot be closed-reduced
- Confirmatory Test
- Radiograph shows liner displaced from head
- Typical Bearing/Setting
- HXLPE (thin liner)
- Key Distinguishing Features
- Acute pain, instability, eccentric head, metallosis
- Confirmatory Test
- Radiograph showing asymmetric/loose liner
- Typical Bearing/Setting
- Any bearing (key mimic)
- Key Distinguishing Features
- Rest/night pain, effusion, raised inflammatory markers
- Confirmatory Test
- CRP/ESR, aspiration with culture and synovial markers
- Typical Bearing/Setting
- Any bearing
- Key Distinguishing Features
- Start-up/load-related pain, progressive migration
- Confirmatory Test
- Radiolucent lines, component migration on serial films
- Risk factors: Thin liners (under 6mm), large heads, obese patients, trauma
- Presentation: Acute pain, instability, metallosis from exposed shell
- Prevention: Calculate liner thickness, minimum 6mm rule
- Treatment: Revision, ensure adequate thickness (may need smaller head)
- Mechanism: Microseparation, stripe wear, edge loading from malposition
- Risk factors: Thin patients, high activity, component malposition, smaller cups
- Presentation: Audible squeak with specific movements (sitting to standing, stairs)
- Natural history: Most remain stable, not associated with higher revision
- Management: Reassurance if benign, revision only if painful or patient distress severe
- Incidence: Under 0.1% with Biolox Delta
- Causes: Impaction technique error, severe trauma, pre-existing damage
- Presentation: Acute pain, grinding sensation, metallosis (embedded particles)
- Treatment: Urgent revision, complete debridement (metal particles), convert to MoP or CoP
- Prevention: Careful impaction, avoid ceramic damage, patient counseling on activity
- Pathophysiology: Type IV hypersensitivity to metal ions, tissue destruction
- Presentation: Pain, soft tissue mass, elevated metal ions, abnormal MRI
- Diagnosis: MRI MARS protocol, metal ion levels (Co, Cr)
- Grading: Pseudotumor size and tissue involvement
- Treatment: Revision with complete debridement, bearing change (ceramic or PE), soft tissue reconstruction
- Outcomes: Poor if severe tissue destruction, abductor deficiency common
- Mechanism: Liner disengages from femoral head (not traditional dislocation)
- Causes: Impingement, liner design/manufacturing, inadequate snap-fit
- Presentation: Dislocation that cannot be closed reduced (key feature)
- Diagnosis: X-ray shows liner outside head
- Treatment: Open reduction required, assess for impingement, may need revision
- Prevention: Avoid impingement, ensure proper liner seating intraoperatively
Postoperative Care and Surveillance
Standard bearing surveillance:
- Standard THA rehabilitation protocol (bearing-independent)
- No bearing-specific restrictions for HXLPE or ceramic
- Dual mobility: Standard precautions (not more restrictive)
- Ceramic: Avoid direct trauma to hip (warn about falls)
- Clinical assessment, X-rays
- All bearings: Assess position, stability, early complications
- Ceramic: Listen for squeaking (if present, document and counsel)
- Dual mobility: Assess for early IPD (rare)
- Clinical and radiographic assessment
- Standard bearings (MoP, CoC, CoP): Routine surveillance
- MoM legacy patients: Metal ions annually, MRI if symptomatic or high ions
- Ceramic: Document squeaking if present, assess if changing
- Every 1-2 years clinical/radiographic
- HXLPE: Monitor for late osteolysis (rare but possible)
- Ceramic: Long-term squeak assessment, wear evaluation
- MoM: Lifetime surveillance required (metal ions, MRI if indicated)
- All: Monitor for aseptic loosening, infection, periprosthetic fracture
MoM-specific surveillance (MHRA 2012 guidelines):
All patients with metal-on-metal bearings require lifetime surveillance. This includes hip resurfacing and large head (over 36mm) MoM THAs. Follow MHRA 2012 guidance or equivalent local protocol. Failure to surveil is medicolegal risk.
MHRA protocol summary:
- Annual clinical assessment - pain, function, soft tissue mass
- Annual metal ion levels - cobalt and chromium
- MRI if:
- Symptomatic (pain, mass)
- Metal ions over 7 ppb
- ASR or other recalled system
- Large head (over 36mm)
- Revision if:
- Symptomatic with pseudotumor
- Asymptomatic but large/growing pseudotumor
- Metal ions persistently over 20 ppb
Activity restrictions by bearing:
- Recommended Activities
- Walking, cycling, golf, swimming
- Caution Activities
- Jogging, doubles tennis
- Avoid Activities
- Impact sports, marathon running
- Recommended Activities
- Walking, cycling, golf, swimming, jogging
- Caution Activities
- Singles tennis, skiing
- Avoid Activities
- Contact sports, high-impact
- Recommended Activities
- Walking, cycling, golf, swimming
- Caution Activities
- Jogging, skiing, tennis
- Avoid Activities
- Rugby, martial arts, parachuting, extreme impact
- Recommended Activities
- All standard activities
- Caution Activities
- High-impact sports
- Avoid Activities
- Extreme ROM sports (yoga, gymnastics may risk IPD)
- HXLPE: Proven standard, excellent longevity, no special restrictions
- Ceramic: Avoid high trauma risk, report squeaking (usually benign)
- Dual mobility: Excellent stability, rare IPD risk
- MoM legacy: Lifetime surveillance required, report any symptoms immediately
- Registry data (AOANJRR in Australia) provides population-level outcomes
- Individual patient: Clinical symptoms most important
- Radiographic loosening: Progressive radiolucent lines, migration
- Osteolysis: Expansile lucencies, cortical thinning
Outcomes and Prognosis - Long-term Performance
- 15-year survivorship: 94-96% (AOANJRR data)
- Wear rate: 0.01-0.05mm/year linear
- Osteolysis: Under 5% at 15 years (vs 30-40% conventional PE)
- Excellent outcomes across all age groups
- Most predictable long-term performance
- 15-year survivorship: 95-96% (highest of common bearings)
- Wear rate: 30-50% less than metal-on-HXLPE
- Best outcomes in under 55 age group (AOANJRR)
- Growing body of 10-15 year data
- May become future standard
- 15-year survivorship: 92-95%
- Lowest wear rate: 4-5 micrometers/year
- Squeak: 1-5%, most benign (not associated with higher revision)
- Fracture: Under 0.1% with modern ceramics (Biolox Delta)
- Young patients: Best wear performance over decades
- Revision for squeak: Under 1% (rare indication)
- Dislocation reduction: 50-75% vs conventional bearings
- Revision THA: 1-2% dislocation rate (vs 5-15% standard)
- Primary THA high-risk: 1-3% dislocation rate
- IPD rate: Under 1%
- No increase in loosening vs standard bearings
- Excellent outcomes in appropriate indications
- 10-15 year revision rate: 15-30% (catastrophic failure)
- ALVAL/pseudotumor: 10-30% at 10 years
- Essentially abandoned globally
- Legacy patients require ongoing surveillance
- Impact on Outcomes
- Young patients higher wear (more cycles)
- Optimization Strategy
- Use lowest-wear bearing (ceramic options)
- Impact on Outcomes
- High activity increases wear
- Optimization Strategy
- Counsel activity modification, choose durable bearing
- Impact on Outcomes
- Malposition accelerates wear, increases complication risk
- Optimization Strategy
- Precision positioning, avoid outliers
- Impact on Outcomes
- Larger heads: more stability, more volumetric wear
- Optimization Strategy
- Balance at 32-36mm for most patients
- Impact on Outcomes
- Obesity increases loads and wear
- Optimization Strategy
- Weight optimization pre-operatively
- Impact on Outcomes
- HXLPE dramatically better than conventional PE
- Optimization Strategy
- Use modern bearings (HXLPE standard)
- Ceramic-on-HXLPE: Lowest revision rate (4-5% at 15 years)
- Metal-on-HXLPE: Acceptable (5-7% at 15 years)
- Longevity critical (may need 40+ year implant life)
- Recommendation: Ceramic options when possible
- Ceramic-on-HXLPE and Metal-on-HXLPE: Similar excellent outcomes
- Individual factors guide choice (activity, preference, cost)
- Both excellent options
- Metal-on-HXLPE: Standard of care, excellent outcomes
- Cost-effective
- Longevity less critical (20-25 year life expectancy)
- Ceramic options reasonable but not necessary for most
- Overall satisfaction: Over 90% with modern bearings
- Squeak impact: Variable - some patients unbothered, others distressed
- Function: Excellent with all modern bearings
- Pain relief: 90-95% significant improvement
- Return to activities: Most patients achieve desired activity level
- HXLPE: High satisfaction, no bearing-specific concerns
- Ceramic: High satisfaction if no squeak, decreased if squeak present
- Dual mobility: Excellent satisfaction, confidence in stability
- MoM: Low satisfaction due to surveillance burden and complications
- HXLPE revolution transformed THA outcomes
- Ceramic options further improve outcomes in young patients
- Dual mobility solves instability problem
- Modern bearings achieve 95%+ survivorship at 15 years
These excellent outcomes are why THA is considered one of the most successful surgical procedures in medicine.
Guidelines, Registries & Global Practice
Global epidemiology and demand:
Hip osteoarthritis is the principal indication for THA, and its burden is rising worldwide. According to PubMed, Global Burden of Disease 2019 analysis for Australia showed hip OA prevalence grew 171% between 1990 and 2019, with population ageing and high BMI as key drivers, and OA-related disability now exceeding that of ischaemic heart disease and type 2 diabetes (Ackerman et al, Intern Med J 2022, DOI). GBD analyses report parallel growth in other large populations - for example, OA prevalence in India rose from 23.5 million (1990) to 62.4 million (2019) (Singh et al, Osteoarthritis Cartilage 2022, DOI). This expanding, ageing and increasingly younger patient base makes durable, low-wear bearing selection a lifetime issue rather than a short-term one.
Registry evidence (Level II observational, very large numbers):
National registries are the strongest real-world evidence on bearing performance. The largest dataset is the National Joint Registry of England and Wales, which demonstrated unequivocally that stemmed metal-on-metal articulations fail at high rates and should not be implanted, with failure worsening as head diameter increased (Smith et al, Lancet 2012, DOI). The AOANJRR, capturing over 98% of Australian arthroplasties since 1999, shows cross-linked polyethylene markedly outperforming non-cross-linked polyethylene, ceramic and cross-linked bearings dominating contemporary use, and 32-36mm heads as the most common size. Major registries (AOANJRR, NJR, the American AJRR, and the Nordic registries) are broadly concordant on these conclusions.
- Population/Coverage
- Over 98% capture since 1999
- Key Bearing Signal
- Cross-linked PE much lower revision than non-cross-linked; ceramic/XLPE dominate; 32-36mm heads standard
- Population/Coverage
- Over 3 million procedures
- Key Bearing Signal
- Stemmed MoM high failure (head-size dependent); larger ceramic-on-ceramic heads perform well
- Population/Coverage
- Largest US arthroplasty registry
- Key Bearing Signal
- Ceramic-on-XLPE and metal-on-XLPE predominate; MoM essentially abandoned
- Population/Coverage
- Pooled Scandinavian data
- Key Bearing Signal
- Cross-linked PE reduces revision for wear/osteolysis vs conventional PE
International guidance, regulators and professional bodies:
- Position on Bearings
- Cross-linked PE supported to reduce wear/osteolysis; no single hard-on-hard bearing mandated; individualise by age/activity
- Strength/Basis
- Evidence-based guideline / registry-informed
- Position on Bearings
- Implants should meet the 10A benchmark (over 95% survival at 10 years); cross-linked PE accepted as standard
- Strength/Basis
- Benchmark-based commissioning
- Position on Bearings
- Stemmed MoM not recommended; lifelong surveillance of legacy MoM; dual mobility endorsed for instability risk
- Strength/Basis
- Consensus + MHRA alerts
- Position on Bearings
- Mandatory surveillance of MoM (Co/Cr ions, MARS MRI); recalls of high-failure MoM systems (e.g. ASR)
- Strength/Basis
- Device safety regulation
- Position on Bearings
- Cross-linked PE and ceramic articulations as mainstays; bearing choice tailored to age, activity and instability risk
- Strength/Basis
- Educational consensus
Practice variation across regions:
- Ceramic-on-ceramic: High uptake in parts of Europe and Asia (notably South Korea, France); lower in North America where ceramic-on-XLPE and metal-on-XLPE predominate.
- Dual mobility: Long-established in France (origin of the concept); rapid recent growth elsewhere for instability prophylaxis in primary and revision THA.
- Cross-linked polyethylene: Near-universal as the standard liner across all high-income registries; conventional PE largely obsolete.
- Metal-on-metal: Abandoned globally for stemmed THA following Lancet/NJR data and regulator alerts; only legacy-patient surveillance remains.
Anchor bearing answers to registry and guideline evidence: "The NJR (Smith et al, Lancet 2012) showed stemmed metal-on-metal fails at high, head-size-dependent rates and should not be used, while the AOANJRR confirms cross-linked polyethylene and ceramic bearings as durable mainstays with 32-36mm heads as standard." Cite the latest AOANJRR Annual Report (Australia) for current figures.
Regulatory and consent essentials:
- TGA (Australia) / FDA / MHRA / CE-mark approval required for all bearing components.
- MoM legacy surveillance is mandated (annual cobalt/chromium ions, MARS MRI if symptomatic or ions elevated; revise if symptomatic with pseudotumour or persistently very high ions).
- Informed consent must include bearing-specific risks (ceramic squeak and fracture; HXLPE liner fracture if thin; intraprosthetic dislocation with dual mobility; metal sensitivity).
MCQ Practice Points
Q: How does highly cross-linked polyethylene reduce wear compared to conventional polyethylene? A: Irradiation (gamma or e-beam) creates cross-links between polymer chains, increasing wear resistance. Post-irradiation treatment (remelting or annealing) eliminates free radicals. This results in 90% wear reduction but decreased mechanical properties (fatigue strength). Minimum 6mm thickness required.
Q: What is the fracture risk of modern fourth-generation ceramic bearings (Biolox Delta)? A: Under 0.1% (less than 1 in 1000). Biolox Delta is alumina matrix composite with zirconia platelets for increased fracture toughness. This is much lower than first-generation pure alumina (1%) and second-generation (0.2-0.5%). Still, fracture is catastrophic requiring extensive debridement.
Q: What is ALVAL and how does it lead to metal-on-metal THA failure? A: ALVAL (Aseptic Lymphocytic Vasculitis-Associated Lesion) is a Type IV delayed hypersensitivity reaction to chromium and cobalt ions released from MoM bearings. Results in lymphocytic infiltration, tissue necrosis, and pseudotumor formation with progressive soft tissue destruction. Diagnosed by elevated metal ions (over 7 ppb) and MRI showing pseudotumor.
Q: How does dual mobility reduce dislocation risk compared to standard bearings? A: Dual mobility has two articulations: small inner head (22-28mm) in polyethylene liner, and large outer liner (36-42mm+) in metal shell. This creates large effective head size for stability while maintaining small inner bearing. Results in 50-75% dislocation reduction in high-risk patients. Main complication is intraprosthetic dislocation (IPD) under 1%.
Q: According to AOANJRR, which bearing has the lowest revision rate in patients under 55? A: Ceramic-on-HXLPE shows the lowest revision rates in the under-55 age group at 15-year follow-up (approximately 4-5%), followed by ceramic-on-ceramic and metal-on-HXLPE (5-7%). Metal-on-metal has highest revision rates (15-30%) and is obsolete. In patients over 65, metal-on-HXLPE is excellent and cost-effective.
Q: What particle size range is most osteolytic in polyethylene wear debris? A: 0.1-10 micrometers is the most biologically active size range. These particles are phagocytosed by macrophages, triggering cytokine release (TNF-alpha, IL-1, RANKL) and osteoclast activation. HXLPE dramatically reduces particle generation, resulting in 95% reduction in osteolysis vs conventional PE at 10-year follow-up.
Q: What is the optimal femoral head size for metal-on-HXLPE bearing in standard patient? A: 32-36mm represents optimal balance. Larger heads reduce dislocation risk and increase ROM, but increase volumetric wear. Heads under 28mm have unacceptably high dislocation rates. Heads over 40mm provide no additional stability benefit and may increase wear. Must ensure minimum 6mm liner thickness with larger heads.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old engineer presents with end-stage hip arthritis from prior acetabular fracture. He is very active (cycling, golf, occasional tennis). BMI 26. He asks about bearing surfaces and wants the best option for longevity. What do you recommend and why?”
“A 58-year-old man had metal-on-metal THA (DePuy ASR) in 2007. He now presents with progressive hip pain over the past 6 months. Examination shows a palpable soft tissue mass laterally. X-rays show well-fixed components. Blood tests show cobalt 18 ppb, chromium 16 ppb. What is your management?”
“A 38-year-old woman had ceramic-on-ceramic THA 18 months ago. She now complains of loud squeaking with sitting to standing and climbing stairs. The hip is otherwise pain-free and functional. X-rays show well-positioned components. She is very distressed by the noise. How do you manage this?”
BEARING OPTIONS OVERVIEW
- Metal-on-HXLPE: 70-80% of THAs, standard of care, excellent outcomes
- Ceramic-on-HXLPE: 10-15%, best for young patients, no squeak
- Ceramic-on-Ceramic: 5-10%, lowest wear, 1-5% squeak risk
- Dual Mobility: 5-10% primary (higher in revision), 50-75% dislocation reduction
- Metal-on-Metal: Obsolete (under 0.1%), ALVAL/pseudotumor failure
HXLPE (HIGHLY CROSS-LINKED PE)
- Manufacturing: Irradiation (50-100 kGy) + remelting/annealing
- Benefits: 90% wear reduction vs conventional PE, 95% less osteolysis
- Trade-off: Decreased mechanical properties (fatigue strength)
- Minimum thickness: 6mm to prevent fracture
- Used in over 90% of modern THAs globally
CERAMIC BEARINGS
- CoC: Lowest wear (4-5 micrometers/year), 1-5% squeak, under 0.1% fracture (Biolox Delta)
- CoP (ceramic-on-HXLPE): 30-50% less wear than MoP, no squeak, excellent for young
- Indications: Young patients (under 50), high longevity requirements
- Avoid: High-impact sports (rugby, martial arts), extreme trauma risk
- AOANJRR: CoP lowest revision rate in under 55 age group
MOM FAILURE (LEGACY SURVEILLANCE)
- ALVAL: Type IV hypersensitivity to Co/Cr ions → pseudotumor
- Surveillance (MHRA 2012): Annual metal ions, MRI if symptomatic or ions over 7 ppb
- Revision if: Symptomatic + pseudotumor, or ions over 20 ppb
- At revision: Complete debridement, bearing change (never MoM again)
- Essentially abandoned globally - under 0.1% current usage
DUAL MOBILITY
- Design: Small inner head (22-28mm) in PE liner, large outer (36-42mm+) effective
- Dislocation reduction: 50-75% in high-risk patients
- Indications: Revision THA, abductor deficiency, neurologic/cognitive impairment
- Complication: Intraprosthetic dislocation (IPD) under 1%, requires open reduction
- AOANJRR: 1-2% dislocation rate vs 3-5% conventional in revision THA
SELECTION BY PATIENT
- Standard (over 65): MoP (HXLPE) 32-36mm head - proven, cost-effective
- Young active (under 50): CoP or CoC - longevity priority, counsel squeak risk
- Instability risk: Dual mobility first choice - dramatic dislocation reduction
- Metal allergy: CoC or CoP - avoid metal bearing surfaces
- Obesity: MoP or CoP, ensure adequate liner thickness (over 6mm)
AOANJRR KEY DATA
- Ceramic-on-HXLPE: Lowest revision rate (4-5% at 15 years), especially under 55
- Metal-on-HXLPE: Excellent all ages (5-6% at 15 years), cost-effective
- Head size: 32-36mm optimal balance (dislocation vs wear)
- Dual mobility: Significantly lower dislocation in revision THA
- Always reference registry data in Australian exam answers
COMPLICATIONS
- HXLPE: Liner fracture if under 6mm thickness
- CoC: Squeaking 1-5% (usually benign), fracture under 0.1% (catastrophic)
- CoC: Stripe wear from malposition (can progress to fracture)
- MoM: ALVAL/pseudotumor 10-30% at 10 years, surveillance mandatory
- Dual mobility: IPD under 1%, requires open reduction
EXAM PEARLS
- HXLPE solved the particle disease problem - 90% wear reduction
- Ceramic-on-HXLPE best balance for young patients (low wear, no squeak)
- MoM failed due to ALVAL - know MHRA 2012 surveillance protocol
- Dual mobility transforms instability outcomes - 50-75% dislocation reduction
- Reference AOANJRR registry data for evidence-based practice
Evidence Base
- Single-centre cohort of 134 primary THAs (mean age 50.7 years) followed at least 15 years. HXLPE showed significantly lower linear and volumetric wear than conventional polyethylene, with no radiographic loosening or osteolysis in the HXLPE group. Wear-related reoperation-free survival was 100% for HXLPE versus 90.9% for conventional PE at 15-18 years.
- Systematic review and meta-analysis of 13 studies (2,278 hips, mean age 44 years). Modern ceramic-on-ceramic THA achieved 96% 10-year survival, with a squeaking rate of 2.7%, ceramic fracture 0.6%, and aseptic loosening 0.5%. Versus polyethylene cups, risk ratio for revision favoured CoC (RR 0.27).
- Series of 660 metal-on-metal resurfacings and large-bearing ASR THAs. 3.4% required revision for adverse reaction to metal debris (all ASR), associated with significantly higher whole-blood chromium and cobalt ion concentrations, smaller components and increased acetabular anteversion. Excess bearing wear, not hypersensitivity alone, drove most failures.
- Analysis of 402,051 primary THAs (31,171 stemmed MoM) from the National Joint Registry of England and Wales. MoM failed at high rates that increased with head size (5-year revision 3.2% for 28mm vs 5.1% for 52mm in men). In young women, 46mm MoM had a 6.1% 5-year revision rate versus 1.6% for 28mm metal-on-polyethylene. Larger ceramic-on-ceramic heads, by contrast, performed better.
- Systematic review of 54 studies. In 10,783 primary dual mobility THAs, intraprosthetic dislocation occurred in 1.1% and extra-articular dislocation in 0.46%, with 98.0% component survivorship at mean 8.5 years. In 3,008 revision dual mobility THAs, survivorship was 96.6% at 5.4 years. Intraprosthetic dislocation was largely confined to earlier designs.
- GBD 2019 data for Australia showed hip OA prevalence grew 171% from 1990 to 2019 (3.20 million Australians with any OA in 2019), driven by population ageing and high BMI. Age-standardised OA years-lived-with-disability rates (313 per 100,000) exceeded those of ischaemic heart disease, stroke and type 2 diabetes.
- The AOANJRR captures over 98% of arthroplasty procedures in Australia. Cross-linked polyethylene bearings have markedly lower revision rates than non-cross-linked polyethylene. Ceramic and cross-linked-polyethylene articulations dominate contemporary practice, while large-head metal-on-metal and conventional polyethylene have been associated with the highest revision rates and are now rarely used. Femoral heads of 32-36mm are the most commonly used size.