Two Articulations | Increased Jump Distance | Reduced Dislocation | Beware IPD
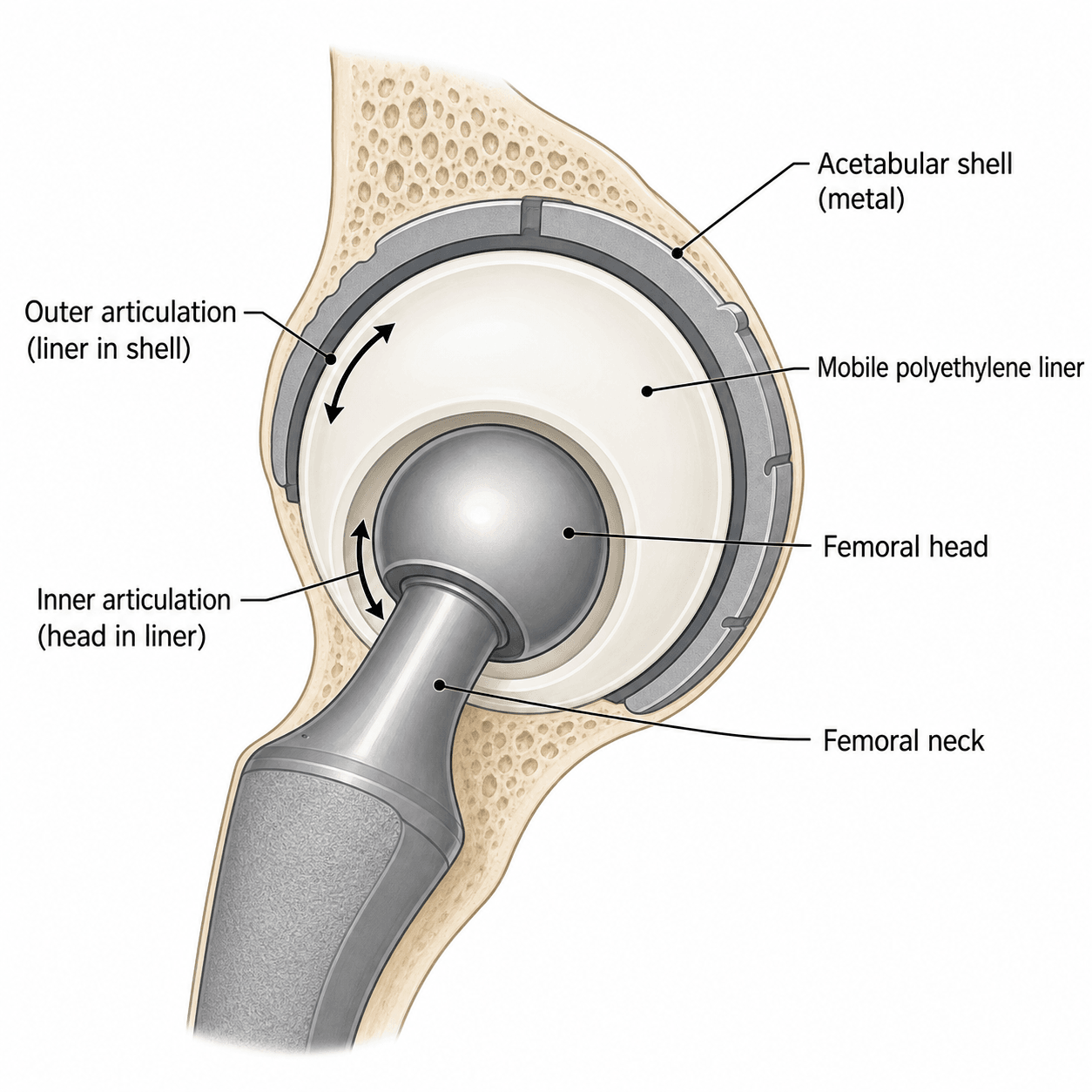
- Two articulations: small head within mobile polyethylene liner, liner articulates with metal shell
- Increased jump distance from larger effective head size reduces impingement and dislocation
- Intraprosthetic dislocation (IPD) is unique complication - liner dissociates from head
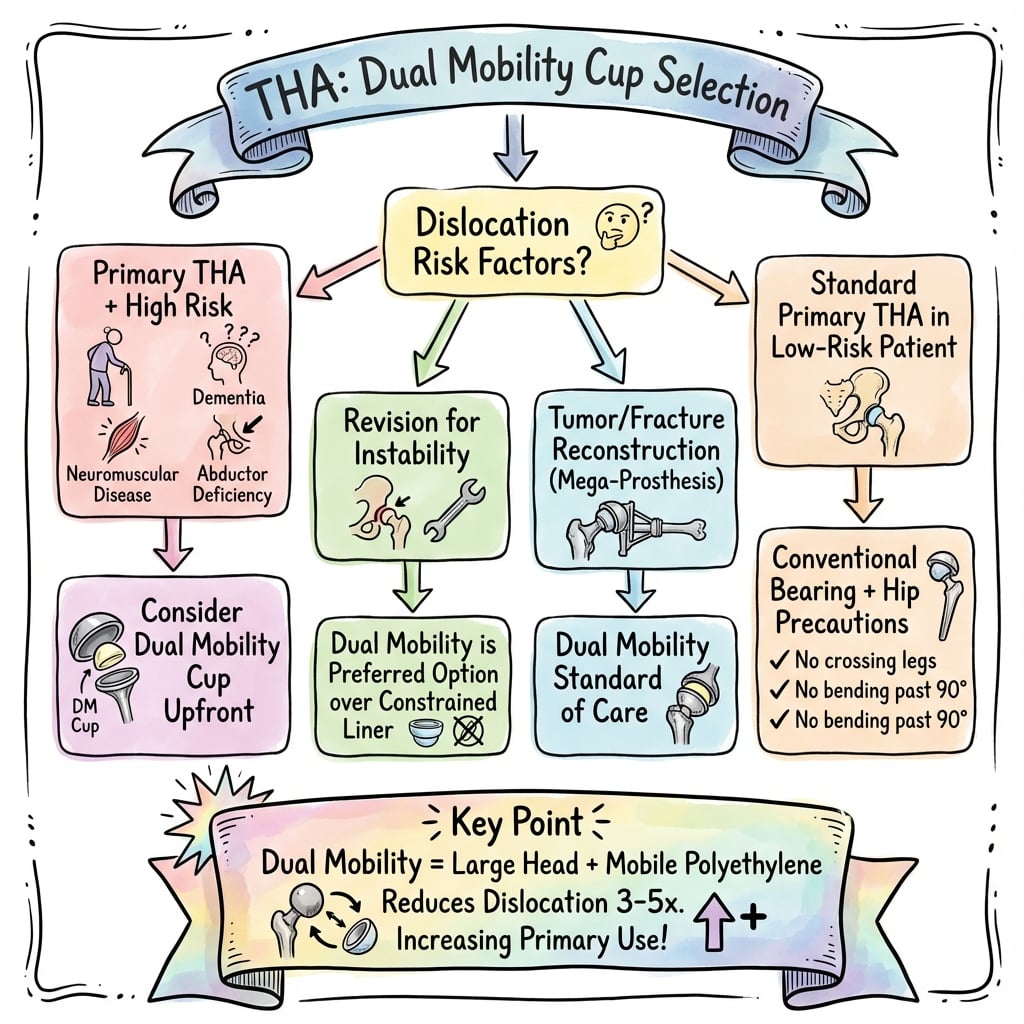
- Primary indications: high-risk primary THA and revision for instability
- AOANJRR data shows excellent survivorship and low revision rates for instability
- “Dual mobility has TWO bearing surfaces - not just a larger head
- “Jump distance is distance the head must travel to dislocate - larger with dual mobility
- “IPD occurs when mobile liner separates from femoral head (early vs late types)
- “Modern designs have improved liner retention reducing IPD risk
The dual mobility design creates two articulations: the small femoral head (typically 22-28mm) within a mobile polyethylene liner, and the liner articulating with the metal shell. This increases the effective head-to-neck ratio and jump distance.
IPD is the unique complication of dual mobility - the polyethylene liner dissociates from the femoral head. Early IPD (under 3 months) suggests technical error. Late IPD suggests liner wear or design issues.
Use dual mobility for high-risk patients: neuromuscular disorders (Parkinson's, cerebral palsy), abductor deficiency, cognitive impairment, prior stroke, high BMI, or revision for recurrent instability.
Registry data (AOANJRR) shows dual mobility has lower revision rates for dislocation compared to standard THA. Particularly beneficial in revision setting and femoral neck fracture treatment in elderly.
- Standard THA
- One (head-liner)
- Dual Mobility THA
- Two (head-liner and liner-shell)
- Standard THA
- Actual head diameter (28-40mm)
- Dual Mobility THA
- Outer liner diameter (typically 40-55mm)
- Standard THA
- Based on actual head/neck
- Dual Mobility THA
- Improved by larger effective head
- Standard THA
- Smaller (e.g., 5-8mm for 32mm head)
- Dual Mobility THA
- Larger (e.g., 12-18mm depending on liner)
- Standard THA
- 2-5% primary, 10-15% revision
- Dual Mobility THA
- 0.5-2% primary, 2-5% revision
- Standard THA
- None
- Dual Mobility THA
- Intraprosthetic dislocation (0.5-1%)
- Standard THA
- None (standard) or constrained
- Dual Mobility THA
- Mobile polyethylene liner
- Key Information
- Two articulations: small head (22-28mm) in mobile PE liner, liner articulates with metal shell
- Key Information
- Increased jump distance (12-18mm) and effective head size (40-55mm) reduce dislocation
- Key Information
- High-risk primary THA (neuromuscular, cognitive, abductor deficiency), revision for instability
- Key Information
- 0.5-2% primary (vs 3-5% standard), 2-5% revision (vs 10-15% standard)
- Key Information
- Intraprosthetic dislocation (IPD) 0.5-1% - liner dissociates from head
- Key Information
- 70% reduction in dislocation revision, comparable overall survivorship (95-98% at 5 years)
- Key Information
- Bousquet (France, 1974), FDA approved USA 2009, modern HXLPE designs low IPD
- Key Information
- Gold standard treatment - superior to constrained liner or large head revision
Overview and Historical Development
Dual mobility total hip arthroplasty uses a unique bearing design with two articulation surfaces to reduce the risk of hip dislocation. The concept was developed by Professor Gilles Bousquet in France in the 1970s in response to high dislocation rates with early THA designs.
Historical context:
- 1974: Bousquet introduced the concept at the University Hospital of Saint-Etienne, France
- Initial design: 22mm cobalt-chrome head within large mobile polyethylene liner
- Goal: Increase effective head size and range of motion before impingement
- European adoption: Widely used in France and Europe from 1980s onwards
- USA adoption: FDA approval in 2009, increasing use since then
- Modern designs: Multiple manufacturers with improved liner retention mechanisms
The biomechanical principle is that hip dislocation requires the femoral head to "jump" over the acetabular rim. Dual mobility increases this jump distance by creating a larger effective head size (the outer diameter of the mobile liner, typically 40-55mm) compared to the actual femoral head (22-28mm). This larger effective head increases the range of motion before impingement and makes dislocation mechanically more difficult.
Current usage patterns:
- Europe: 10-25% of primary THA in some countries (France highest)
- Australasia: 15-20% of primary THA (AOANJRR data)
- USA: Increasing adoption, particularly for high-risk cases
- Indications: High-risk primary THA and revision for instability
BOUSQUETBOUSQUET - Historical Development
Hook:BOUSQUET developed the concept in France - know the history for exam discussions
Indications and Patient Selection
- Parkinson's disease (impaired proprioception, rigidity)
- Cerebral palsy (spasticity, muscle imbalance)
- Multiple sclerosis (weakness, spasticity)
- Prior stroke with residual weakness or spasticity
- Muscular dystrophy
- Dementia or Alzheimer's disease
- Inability to follow hip precautions
- Psychiatric disorders affecting compliance
- Abductor muscle deficiency or tears
- Prior hip surgery with soft tissue damage
- Spinopelvic imbalance (flat lumbar spine, fixed sagittal imbalance)
- High BMI (over 35) with increased soft tissue laxity
- Developmental dysplasia of the hip (DDH) with abnormal anatomy
- High fall risk (multiple comorbidities, frailty)
- Poor compliance anticipated
- Substance abuse affecting adherence
- Displaced intracapsular fracture in frail elderly
- High dislocation risk (cognitive impairment, prior falls)
- Either hemiarthroplasty or THA with dual mobility
These indications reflect patients with elevated baseline dislocation risk where dual mobility offers protective benefit.
HIGHHIGH RISK - Primary THA Indications
Hook:HIGH RISK patients benefit most from dual mobility - know when to choose it
Anatomy and Biomechanics
- Metal shell: Typically titanium with porous coating for bone ingrowth
- Mobile polyethylene liner: Highly cross-linked polyethylene (HXLPE)
- Liner retention mechanism: Enhanced design features to prevent dissociation
- Shell sizes: Typically 44mm to 66mm diameter
- Standard femoral stem: Same as conventional THA (cemented or uncemented)
- Small femoral head: Typically 22mm or 28mm diameter
- Materials: Cobalt-chrome or ceramic (ceramic less common)
- Primary articulation: Small head rotating within mobile liner (intraprosthetic)
- Secondary articulation: Mobile liner rotating within metal shell (extraprosthetic)
- Standard 32mm Head
- 32mm
- Dual Mobility (28mm head, 50mm liner)
- 50mm (outer liner)
- Standard 32mm Head
- Approximately 1.8:1
- Dual Mobility (28mm head, 50mm liner)
- Approximately 3.5:1
- Standard 32mm Head
- Approximately 7mm
- Dual Mobility (28mm head, 50mm liner)
- Approximately 15mm
- Standard 32mm Head
- Standard (limited by neck)
- Dual Mobility (28mm head, 50mm liner)
- Increased (improved ratio)
- Standard 32mm Head
- Lower (smaller bearing)
- Dual Mobility (28mm head, 50mm liner)
- Higher (larger polyethylene surface)
Jump distance concept:
- Definition: Distance the femoral head center must travel perpendicular to the acetabular opening to dislocate
- Formula: Jump distance = (effective head radius) - (neck radius) × sin(inclination angle)
- Larger jump distance = more stable: Requires greater force and displacement to dislocate
- Clinical relevance: Dual mobility jump distance typically 12-18mm vs 5-8mm for standard THA
Both articulations can move, but the distribution of motion varies. Initially, the intraprosthetic articulation (head within liner) predominates. Over time, as the liner seats into the shell, the extraprosthetic articulation (liner within shell) increases. The ratio typically stabilizes at 60-70% intraprosthetic and 30-40% extraprosthetic motion.
Wear considerations:
- Two bearing surfaces: Polyethylene wear at both articulations
- Volumetric wear: Greater total polyethylene surface area than standard THA
- HXLPE: Highly cross-linked polyethylene reduces wear rate
- Modern evidence: Acceptable wear rates with current generation designs
- Long-term concern: More polyethylene debris than metal-on-HXLPE standard THA
Classification Systems
Historical evolution of dual mobility designs:
- Era
- 1970s-1990s
- Key Features
- Bousquet design, cemented metal-backed cup, standard polyethylene
- Limitations
- High wear rates, frequent IPD (5-10%)
- Era
- 1990s-2000s
- Key Features
- Improved liner retention, cementless options, enhanced polyethylene
- Limitations
- Reduced IPD but still concerns about wear
- Era
- 2000s-present
- Key Features
- HXLPE, advanced retention mechanisms, multiple bearing options
- Limitations
- Low IPD (under 1%), acceptable wear rates
Key improvements over time:
- Liner retention mechanisms reduced IPD from 5-10% to under 1%
- HXLPE reduced volumetric wear rates significantly
- Uncemented options improved long-term fixation
- Modular designs allow revision flexibility
Evolution from first to third generation transformed dual mobility from experimental to mainstream.
Clinical Assessment and Patient Evaluation
- Primary diagnosis: Osteoarthritis, AVN, femoral neck fracture, inflammatory arthritis
- Dislocation risk factors: Prior dislocation, neuromuscular disorder, cognitive status, fall history
- Medical comorbidities: Parkinson's disease, stroke, dementia, epilepsy, substance use
- Functional status: Mobility aids, independence, living situation
- Prior hip surgery: Previous THA, osteotomy, fracture fixation, arthroscopy
- Medications: Medications affecting balance, anticoagulation
- Gait assessment: Trendelenburg sign (abductor weakness), neuromuscular abnormalities
- Hip range of motion: Flexion, extension, abduction, adduction, rotation
- Abductor strength: Resisted abduction testing, single leg stance
- Leg length: Measure discrepancy if present
- Neurovascular: Document baseline function
- Cognitive assessment: Orientation, ability to follow instructions
- Spinal alignment: Sagittal balance, lumbar lordosis, flexibility
- Standing lateral spine radiograph: Measure lumbar lordosis, sacral slope, pelvic tilt
- Sitting lateral radiograph: Assess spinopelvic mobility
- Flat lumbar spine: High risk for posterior dislocation when sitting (pelvic retroversion)
- Stiff spine: Limited compensatory motion increases hip demands
- Patient Factors
- Young, active, no risk factors, primary OA, good bone/soft tissue
- Consider Dual Mobility?
- Optional - standard THA acceptable
- Patient Factors
- Elderly, high BMI, mild cognitive impairment, prior hip surgery
- Consider Dual Mobility?
- Consider dual mobility - discuss risks/benefits
- Patient Factors
- Neuromuscular disease, dementia, recurrent dislocation, abductor deficiency
- Consider Dual Mobility?
- Strong indication for dual mobility
- Patient Factors
- Revision for instability, multiple prior dislocations, combined risk factors
- Consider Dual Mobility?
- Dual mobility gold standard
Decision-making framework:
- Low risk primary: Standard THA reasonable, dual mobility optional
- Moderate risk: Shared decision-making with patient about dual mobility benefits
- High risk: Strong recommendation for dual mobility
- Revision instability: Dual mobility is standard of care
Proper patient assessment and risk stratification guide appropriate dual mobility use.
Investigations and Imaging
- AP pelvis: Assess both hips, bone quality, dysplasia, prior hardware
- Lateral hip: Assess femoral offset, version estimate
- Assess for: Bone loss, dysplasia, protrusio, prior surgery, acetabular defects
- Revision cases: Assess bone stock, component position, osteolysis
- Complex primary: Severe dysplasia, prior fracture, bone loss
- Version assessment: Acetabular and femoral version measurement
- 3D reconstruction: Surgical planning for complex anatomy
- Abductor assessment: Suspected gluteus medius/minimus tear
- AVN staging: MRI is gold standard for early AVN
- Soft tissue evaluation: Infection suspicion, tumor
- Standing lateral spine radiograph: Lumbar lordosis, pelvic incidence, sacral slope
- Sitting lateral radiograph: Assess pelvic tilt change (spinopelvic mobility)
- Indications: Prior dislocation, spinal fusion, flat back syndrome, elderly
- FBC, UEC, coagulation profile
- Blood group and antibody screen
- ECG, CXR as per anesthetic assessment
- ESR, CRP (elevated suggests infection)
- Aspiration with culture if revision or concern for infection
- PJI workup if revision case
- Bone density scan if concern for osteoporosis (affects fixation choice)
- Cardiac/respiratory workup as needed for comorbidities
- Digital templating: Plan component sizes (acetabular shell, femoral stem)
- Offset and leg length: Plan restoration of hip biomechanics
- Component position: Plan target inclination and anteversion
Appropriate imaging guides surgical planning and dual mobility component selection.
Management Algorithm
Algorithm for dual mobility in primary THA:
Step 1: Assess dislocation risk
- Low risk: Young, active, no comorbidities → Standard THA appropriate
- Moderate risk: Elderly, high BMI, mild cognitive issues → Discuss options
- High risk: Neuromuscular, dementia, abductor deficiency → Recommend dual mobility
- Very high risk: Multiple risk factors combined → Strong dual mobility indication
Step 2: Patient counseling
- Explain dual mobility benefits (reduced dislocation 0.5-2% vs 3-5%)
- Discuss unique complication (IPD under 1%)
- Review recovery and precautions (may be relaxed with dual mobility)
- Shared decision-making for moderate risk patients
Step 3: Component selection
- Choose appropriate dual mobility system
- Size acetabular shell based on native acetabulum
- Select femoral stem based on canal geometry
- Plan combined anteversion (cup + stem = 25-40 degrees)
Step 4: Surgical approach
- Select approach based on surgeon experience
- Posterior most common for dual mobility
- Anterior or anterolateral also suitable
- Standard soft tissue protection regardless of approach
This structured approach ensures appropriate dual mobility use in primary THA.
Surgical Technique
- Most commonly used approach for dual mobility
- Excellent acetabular exposure for shell positioning
- Capsular repair important for stability (as with all THA)
- Standard posterior soft tissue repair techniques
- Good visualization of acetabulum
- Preserves posterior capsule
- Abductor split or detachment techniques
- Increasingly popular for dual mobility
- Intermuscular interval, no muscle cutting
- Good component positioning
- May be more challenging for larger shells
Approach selection based on surgeon experience and patient anatomy, not determined by dual mobility choice.
Dual Mobility vs the Constrained Liner
The constrained liner is repeatedly cited as the inferior alternative for instability, but its design and failure mechanism are worth understanding. A constrained liner achieves stability by mechanically capturing the femoral head - typically with a metal locking or reinforcing ring around the polyethylene rim (or a captured tripolar bearing) - so the head cannot leave the liner without overcoming the ring. Dual mobility, by contrast, achieves stability biomechanically through a larger effective head and a greater jump distance.
- Dual mobility
- Larger effective head and increased jump distance (biomechanical)
- Constrained liner
- Mechanical capture of the head by a locking/reinforcing ring
- Dual mobility
- Increased (large head-to-neck ratio)
- Constrained liner
- Reduced - the constraining rim limits motion and increases impingement
- Dual mobility
- Head moves within the mobile liner and the force is dissipated
- Constrained liner
- Force is transmitted as torque to the fixation interfaces
- Dual mobility
- Intraprosthetic dislocation (rare with modern designs)
- Constrained liner
- Locking-ring failure, liner-shell dissociation, acetabular loosening
- Dual mobility
- Higher survivorship, lower re-dislocation (94.7% vs 81.0%; 2.6% vs 11.0%)
- Constrained liner
- Inferior survivorship and higher dislocation/loosening
- Dual mobility
- First-line for recurrent instability and high-risk hips
- Constrained liner
- Salvage only when capture is the sole option (e.g. irreparable abductor loss, very low demand)
A constrained liner achieves stability by mechanically capturing the head with a locking or reinforcing ring, whereas dual mobility does so biomechanically through a larger effective head and greater jump distance. The price of mechanical capture is that any dislocating force is transmitted as torque to the fixation interfaces - so constrained liners fail by locking-ring failure, liner-shell dissociation or acetabular loosening, and they also restrict motion and increase impingement. This is why dual mobility outperforms the constrained liner for recurrent instability (in the pooled review, survivorship 94.7% vs 81.0% and dislocation 2.6% vs 11.0%), and the constrained liner is now reserved for salvage situations where capture is the only option, such as irreparable abductor deficiency in a very low-demand patient.
DUALDUAL - Core Design Principles
Hook:DUAL reminds you this is about TWO articulations, not just a big head
Complications
- Incidence
- 0.5-1% (modern designs)
- Management
- Closed reduction possible if early, open reduction and liner exchange if recurrent
- Incidence
- 0.5-2% primary, 2-5% revision
- Management
- Closed reduction, assess for malposition or impingement
- Incidence
- 1-3% (more with ceramic heads)
- Management
- Usually benign, rarely requires revision
- Incidence
- Theoretical concern, rare clinically
- Management
- Surveillance radiographs, revision if osteolysis
- Incidence
- Very rare with modern designs (under 0.5%)
- Management
- Revision with liner exchange, assess shell stability
Intraprosthetic dislocation (IPD) - unique to dual mobility:
Definition: Dissociation of the polyethylene liner from the femoral head, while the liner remains in the metal shell.
-
Early IPD (under 3 months postop):
- Usually due to technical error
- Incomplete liner seating during surgery
- Impingement (neck-on-liner) levering liner off head
- Component malposition
-
Late IPD (over 3 months postop):
- Polyethylene liner wear
- Liner deformation over time
- Older generation liner retention designs
- Patient feels hip "go out" but different sensation than typical dislocation
- Hip may appear reduced on X-ray (liner still in shell, head medial)
- Eccentric position of femoral head within acetabulum on X-ray
- May have pain or clicking sensation
- AP pelvis X-ray: Femoral head appears medialized or eccentric in cup
- Lateral X-ray: Head not concentrically positioned in liner
- "Double-density" sign: Overlapping shadows of head and liner rim
- Acute presentation: Attempt closed reduction (may succeed if liner not damaged)
- Recurrent IPD: Open reduction, liner exchange, assess for impingement or malposition
- Late IPD with wear: Liner exchange, consider shell revision if worn or malpositioned
- Meticulous surgical technique ensuring complete liner seating
- Proper component positioning to avoid impingement
- Modern liner designs with enhanced retention mechanisms
- Infection (same risk as standard THA)
- Periprosthetic fracture (same risk)
- Loosening (potentially higher polyethylene wear load)
- Neurovascular injury (same risk)
- Leg length discrepancy (same risk)
- Distinguishing features
- Liner separates from head; less deformity than true dislocation; head appears medialised/eccentric in shell, double-density sign
- Key investigation / next step
- AP + lateral radiograph; closed reduction attempt, open reduction + liner exchange if recurrent
- Distinguishing features
- Whole liner-and-head construct out of shell; classic shortened/rotated limb, frank deformity
- Key investigation / next step
- Radiograph; closed reduction, assess component position and impingement
- Distinguishing features
- Recurrent instability despite reduction; cup outside safe zone or abnormal combined anteversion
- Key investigation / next step
- CT for version; revise malpositioned component
- Distinguishing features
- Rest/night pain, warmth, effusion, raised inflammatory markers; can mimic loosening
- Key investigation / next step
- ESR/CRP, aspiration with culture and cell count
- Distinguishing features
- Activity-related start-up pain, progressive radiolucent lines, component migration
- Key investigation / next step
- Serial radiographs; revision if symptomatic or progressive
- Distinguishing features
- Acute pain after fall/load, inability to weight-bear, fracture on imaging
- Key investigation / next step
- Radiograph (Vancouver classification); fixation versus revision
- Distinguishing features
- Groin pain on active hip flexion / resisted straight-leg raise; prominent cup rim
- Key investigation / next step
- Examination, image-guided injection; rarely revision/release
Closed Reduction Pitfall: Iatrogenic Intraprosthetic Dislocation
A true (extra-articular) dual-mobility dislocation can usually be reduced closed, but there is a specific trap: a forceful closed reduction can lever the polyethylene liner off the femoral head and convert a true dislocation into an intraprosthetic dislocation (iatrogenic IPD). The retentive rim of the liner is levered off the head during the manoeuvre, leaving the liner in the shell and the head bare.
- Concentric head in liner (true reduction)
- Centred within the acetabular component on AP and lateral
- Eccentric/medialised head (iatrogenic IPD)
- Medialised/eccentric; double-density sign (overlapping head and liner-rim shadows)
- Concentric head in liner (true reduction)
- Liner-and-head reduced together into the shell
- Eccentric/medialised head (iatrogenic IPD)
- Reduction levered the liner off the head - liner in shell, head out of liner
- Concentric head in liner (true reduction)
- Confirm stability; manage as a reduced true dislocation
- Eccentric/medialised head (iatrogenic IPD)
- Open reduction and liner exchange - the liner cannot be re-captured closed
A forceful closed reduction of a true dual-mobility dislocation can lever the liner off the head and convert it into an intraprosthetic dislocation (iatrogenic IPD). Reduce gently, under full muscle relaxation (general anaesthesia) and with image-intensifier guidance, and never assume success from limb position alone: confirm a CONCENTRIC head-within-liner position on post-reduction radiographs. A head that sits medialised or eccentric in the shell after 'reduction' (the double-density sign) is an IPD, not a reduced hip, and needs open reduction with liner exchange because the liner cannot be re-captured closed.
IPDIPD - Intraprosthetic Dislocation Types
Hook:IPD is the unique dual mobility complication - early vs late has different causes
Postoperative Care and Rehabilitation
Postoperative protocol for dual mobility THA:
- Standard THA postoperative care
- Mobilization day of surgery or day 1 (per institutional protocol)
- Hip precautions may be relaxed compared to standard THA
- Weight bearing as tolerated (unless femoral/acetabular bone concerns)
- DVT prophylaxis per guidelines
- Progressive mobilization with physiotherapy
- Stairs training before discharge
- Hip precautions: Many surgeons use reduced or no formal precautions with dual mobility
- Wound care education
- Discharge planning for home support if needed
- Wound check and suture/staple removal (day 10-14)
- Progressive walking distance and activities
- Weaning from walking aids as tolerated
- Return to driving (4-6 weeks, when off opioids and good control)
- Light activities of daily living
- X-ray at 6 weeks (AP pelvis and lateral hip)
- Assess component position and bone ingrowth
- Progressive strengthening exercises
- Return to sedentary work
- Recreational activities as tolerated
- Full functional recovery expected by 3-6 months
- Return to full activities including sports (discuss with surgeon)
- Annual follow-up with X-rays for surveillance
- Watch for late complications or wear
Hip precautions debate:
- Traditional approach: Standard THA precautions (no flexion over 90 degrees, no adduction past midline, no internal rotation)
- Dual mobility advantage: Increased stability may allow reduced or no formal precautions
- Current trend: Many surgeons reduce or eliminate precautions for dual mobility patients
- Patient-specific: Consider patient's cognitive status, compliance, fall risk
The benefit of dual mobility is that many surgeons feel comfortable eliminating or significantly reducing hip precautions. The increased jump distance and range of motion before impingement provide inherent stability. However, this remains surgeon-dependent, and high-risk patients (cognitive impairment, prior dislocation) may still benefit from precautions.
Long-term surveillance:
- Annual X-rays: AP pelvis and lateral hip for first 2-5 years
- Watch for: Osteolysis, component migration, wear
- Symptomatic review: Pain, clicking, instability sensation
- After 5 years: Consider X-rays every 2-3 years if asymptomatic
Guidelines, Registries & Global Practice
Hip instability is the leading early cause of revision THA worldwide, and dual mobility has become a globally accepted strategy to address it. The picture below is evidence-led rather than tied to any single health system.
Global epidemiology and burden of instability
- Dislocation is among the commonest indications for early revision THA; pooled comparative data show dual-mobility cups cut dislocation roughly six-fold versus fixed-bearing cups (dislocation risk ratio 0.16) (Romagnoli et al. Int Orthop 2018; DOI).
- Dual mobility was conceived by Gilles Bousquet in Saint-Etienne, France (early 1970s); long-term modern-generation cementless cups now show no intraprosthetic dislocation or osteolysis at 10-16 years (Gaillard/Batailler et al. J Arthroplasty 2019; DOI).
- Use is highest in France and continental Europe, rising in Australasia and North America (FDA clearance for modular dual mobility, 2009).
Major guidance, side by side
- Position on dual mobility
- Recognises dual mobility as an option to reduce instability, especially in revision and high-risk primary THA; emphasises individualised selection
- Evidence level / note
- Consensus / moderate-quality evidence
- Position on dual mobility
- Implant choice guided by ODEP benchmarking and NJR outcome data; dual mobility used for instability-risk and recurrent dislocation rather than as a default primary bearing
- Evidence level / note
- Registry-anchored guidance
- Position on dual mobility
- Supports dual mobility (and large heads) as constructs that raise jump distance and head-neck ratio for unstable or revision hips
- Evidence level / note
- Expert / principle-based
- Position on dual mobility
- Endorses dual mobility for high-dislocation-risk primary THA, femoral neck fracture in the elderly and revision for instability
- Evidence level / note
- Consensus, Level III evidence base
Registry evidence (instability and survivorship)
- Signal
- Lower revision for dislocation than fixed-bearing THA; comparable overall cumulative revision; rising utilisation
- Practice point
- Favoured for revision instability and frail FNF
- Signal
- Used with ODEP benchmarking; instability/revision indications predominate over routine primary use
- Practice point
- Bearing choice tied to outcome data
- Signal
- Steadily increasing dual-mobility use in primary and revision THA
- Practice point
- Adoption reflects instability-prevention strategy
- Signal
- Support dual mobility for elderly femoral neck fracture and instability-risk hips
- Practice point
- Strong trauma-arthroplasty signal
Global practice variation
- High-resource settings: dual mobility increasingly routine for revision instability and elderly femoral neck fracture; debate persists about routine use in young, high-demand primary THA owing to polyethylene wear concerns.
- Limited-resource settings: higher implant cost and supply constraints limit uptake; standard fixed-bearing THA with optimised component position and head size remains the mainstay, with dual mobility reserved for highest-risk hips.
- Bearing trends: modern HXLPE liners and improved retention mechanisms have largely resolved the first-generation IPD/wear problem; ceramic-head dual mobility is under evaluation but carries limited long-term data.
For any board, the world standard is consistent: dual mobility is the construct of choice for revision instability and a strong option for high-dislocation-risk primary THA and elderly femoral neck fracture. Registries (AOANJRR, NJR, AJRR, Nordic) show reduced instability revision with comparable overall survivorship; the main unresolved question is wear in young, high-demand patients.
MCQ Practice Points
Q: What is the primary biomechanical advantage of dual mobility THA that reduces dislocation risk? A: Increased jump distance due to larger effective head size. The outer diameter of the mobile polyethylene liner (typically 40-55mm) acts as the effective head, creating a larger head-to-neck ratio and requiring greater displacement to dislocate (12-18mm jump distance vs 5-8mm for standard 32mm head).
Q: What is the strongest evidence-based indication for dual mobility THA? A: Revision THA for recurrent instability. Meta-analyses and registry data show dual mobility reduces re-dislocation from 10-15% to 2-5% and has superior outcomes compared to constrained liners or large head revision. This is the gold standard approach for recurrent THA dislocation.
Q: A patient presents 4 weeks after dual mobility THA with hip pain and X-ray showing the femoral head medialized and eccentric within the acetabular component. What is the diagnosis? A: Intraprosthetic dislocation (IPD). The polyethylene liner has dissociated from the femoral head while remaining in the shell. Early IPD (under 3 months) suggests technical error such as incomplete liner seating or impingement. Management includes attempted closed reduction and if unsuccessful or recurrent, open reduction with liner exchange.
Q: How many articulation surfaces does a dual mobility THA have and what are they? A: Two articulations: (1) Primary/intraprosthetic articulation - small femoral head (22-28mm) rotating within mobile polyethylene liner, (2) Secondary/extraprosthetic articulation - mobile liner rotating within metal shell. Both articulations contribute to overall motion with typically 60-70% occurring at the intraprosthetic and 30-40% at the extraprosthetic surface.
Q: According to AOANJRR data, what is the revision rate for dislocation with dual mobility THA compared to standard THA? A: Dual mobility has significantly lower revision for dislocation - approximately 0.3% at 5 years compared to 1.1% for standard THA. This represents a 70% reduction in dislocation revision risk. Overall survivorship is comparable between dual mobility and standard THA.
Q: Which patient populations are considered high-risk for THA dislocation and may benefit from dual mobility? A: High-risk populations include: (1) Neuromuscular disorders (Parkinson's, cerebral palsy, prior stroke, MS), (2) Cognitive impairment (dementia, psychiatric disorders), (3) Anatomical factors (abductor deficiency, spinopelvic imbalance, DDH), (4) Medical factors (high fall risk, obesity, prior dislocation history), (5) Femoral neck fracture in frail elderly.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 72-year-old woman with severe hip osteoarthritis is scheduled for primary THA. She has a history of Parkinson's disease with moderate tremor and rigidity, but is cognitively intact and independently mobile with a walking stick. Her daughter asks if there's anything you can do to reduce the risk of hip dislocation, which happened to a friend. How would you counsel this patient about dual mobility THA?”
“A 68-year-old man underwent primary THA via posterior approach 3 years ago for osteoarthritis. He has had four posterior dislocations, all reduced in the emergency department. The last dislocation was 2 weeks ago. CT scan shows well-positioned components (cup 40 degrees inclination, 20 degrees anteversion, stem in 15 degrees anteversion). What are your options for managing his recurrent instability and why would you choose dual mobility?”
“You performed a dual mobility THA 6 weeks ago using a posterior approach. The patient presents to ED reporting the hip 'went out' while bending to tie shoes. On examination, the leg is slightly shortened and internally rotated, but less deformity than a typical dislocation. AP pelvis X-ray shows the femoral head appears eccentric within the acetabular component, medialized relative to the shell. What has happened and how do you manage this?”
CORE DESIGN PRINCIPLES
- Two articulations: head-in-liner (intraprosthetic) + liner-in-shell (extraprosthetic)
- Small head (22-28mm) in mobile polyethylene liner
- Effective head size = outer liner diameter (40-55mm)
- Increased jump distance (12-18mm vs 5-8mm standard)
- Larger head-to-neck ratio reduces impingement
- Both articulations contribute to motion (60% intra, 40% extra)
KEY INDICATIONS
- Primary THA: Neuromuscular (Parkinson's, CP, stroke), cognitive impairment, abductor deficiency
- Primary THA: High fall risk, femoral neck fracture in elderly, prior hip surgery
- Revision THA: Recurrent instability (GOLD STANDARD), complex revision with bone loss
- Other: Oncologic reconstruction, radiation pelvis, prior infection with soft tissue compromise
- Relative: BMI over 35, spinopelvic pathology, hypermobility syndromes
OUTCOMES AND EVIDENCE
- Dislocation rate: 0.5-2% primary, 2-5% revision (vs 3-5% and 10-15% standard)
- AOANJRR: 0.3% revision for dislocation at 5 years (vs 1.1% standard)
- Survivorship: 95-98% at 5 years (comparable to standard THA)
- Re-dislocation in revision: 2-5% dual mobility vs 10-15% other options
- Meta-analyses: Dual mobility superior to constrained liner for revision instability
INTRAPROSTHETIC DISLOCATION (IPD)
- Unique complication: Liner dissociates from head (head medializes, liner stays in shell)
- Incidence: 0.5-1% with modern designs (higher with older designs)
- Early IPD (under 3 months): Technical error (incomplete seating, impingement)
- Late IPD (over 3 months): Polyethylene wear, liner deformation
- X-ray signs: Eccentric head, medialized position, double density sign
- Management: Attempt closed reduction; if fails or recurrent, open reduction + liner exchange
SURGICAL TECHNIQUE
- Any standard approach (posterior most common)
- Acetabular shell: Standard positioning (40 degrees inclination, 15-25 degrees anteversion)
- Critical: Meticulous liner insertion (clean/dry shell, ensure full seating, audible click)
- Femoral component: Standard technique, 10-15 degrees stem anteversion
- Combined anteversion: 25-40 degrees (Ranawat safe zone)
- Intraoperative stability test: Full ROM, no impingement
AOANJRR KEY DATA
- Usage: rising in high-income settings; 18% of primary THA in Australia per AOANJRR (2023), up from 5% in 2010
- Dislocation revision: 70% reduction vs standard THA
- Femoral neck fracture: Lower revision than hemiarthroplasty or standard THA
- Revision instability: Lowest re-revision rate among all options
- Overall survivorship: Comparable to standard THA (no increase in other failures)
EXAM TRAPS AND PEARLS
- Don't confuse dual mobility with just a large head - it has TWO articulations
- IPD is specific to dual mobility - know diagnosis (X-ray signs) and management
- Revision for instability: Dual mobility is gold standard (superior to constrained)
- Can often eliminate or reduce hip precautions with dual mobility
- Modern HXLPE has acceptable wear rates despite larger surface area
- Bousquet developed in France 1970s - know the history
Outcomes and Evidence Synthesis
- Dislocation: roughly six-fold lower than fixed-bearing cups (dislocation risk ratio 0.16) (Romagnoli et al. Int Orthop 2018; DOI).
- Intraprosthetic dislocation: about 1.1% across 10,783 primary dual-mobility THAs, mostly first-generation designs (Darrith et al. Bone Joint J 2018; DOI).
- Survivorship: approximately 98% at mean 8.5 years pooled, and approximately 98% at 10 years with no IPD/osteolysis for a modern cementless cup at 10-16 years (Gaillard/Batailler et al. J Arthroplasty 2019; DOI).
- Versus constrained liners: higher survivorship (94.7% vs 81.0%) and lower dislocation (2.6% vs 11.0%) (Van Eecke et al. Hip Pelvis 2020; DOI).
- Versus large femoral heads: no significant dislocation difference in the only RCT to date, both strategies giving low rates (Weintraub/Darrith et al. J Arthroplasty 2023; DOI).
- Dislocation roughly halved (RR 0.47) and revision reduced (RR 0.77) versus conventional THA, with a small increase in heterotopic ossification (Santiago et al. J Orthop Surg Res 2025; DOI).
Real-world joint registries (AOANJRR, NJR, AJRR and the Nordic registries) corroborate these findings - lower revision for instability with comparable overall survivorship - and are summarised in the Guidelines, Registries & Global Practice section below.
- Volumetric wear: Higher than standard metal-on-HXLPE THA (larger surface area)
- Linear wear rates: Acceptable with modern HXLPE (0.05-0.1mm/year)
- Osteolysis: Rare with modern HXLPE dual mobility (under 2% at 10 years)
- Revision for wear: Very low (under 1% at 10 years)
- Function scores: Comparable to standard THA (Oxford Hip Score, HOOS)
- Satisfaction: High satisfaction rates (85-95%)
- Return to activity: Similar to standard THA
- Quality of life: Improved from preoperative baseline, similar to standard THA
- Dual mobility reduces dislocation vs standard hemiarthroplasty or THA
- Particularly beneficial in frail elderly with cognitive impairment
- AOANJRR shows lower revision rate for instability
- Re-dislocation reduced from 10-15% to 2-5%
- Patient satisfaction high when instability resolved
- Most cost-effective approach for recurrent dislocation
Evidence Base
- Systematic review of 54 studies. For 10,783 PRIMARY dual mobility THAs: intraprosthetic dislocation (IPD) 1.1%, extra-articular dislocation 0.46%, aseptic loosening 1.3%, overall survivorship 98.0% at mean 8.5 years.
- For 3008 REVISION dual mobility THAs: IPD 0.3%, extra-articular dislocation 2.2%, survivorship 96.6% at 5.4 years.
- IPD was low and largely limited to earlier (first-generation) designs.
- Meta-analysis of 15 comparative studies, 2408 THAs (50.6% dual-mobility, 49.4% fixed-bearing).
- Dislocation risk ratio 0.16 (95% CI 0.09-0.28) favouring dual mobility - roughly a six-fold reduction in dislocation risk.
- Benefit held across primary, revision, trauma and elective subgroups and in high-risk patients.
- National registry capturing essentially all hip arthroplasties performed in Australia, used here as a representative example of registry evidence.
- Dual-mobility bearings are associated with lower revision for dislocation/instability than fixed-bearing THA, particularly in revision and femoral-neck-fracture settings, with comparable overall cumulative revision.
- Registry use of dual mobility has risen over the last decade, reflecting growing surgeon confidence.
- 3 RCTs plus 10 cohort studies, 21,585 patients (4887 dual mobility, 16,698 conventional THA).
- Dual mobility lowered dislocation (RR 0.47, 95% CI 0.34-0.65) and revision (RR 0.77, 95% CI 0.67-0.89) versus conventional THA.
- Trade-offs: higher heterotopic ossification (RR 1.98) and slightly worse early functional scores at 6-9 months; posterior approach did not alter the dislocation benefit.
- 310 primary cementless dual-mobility THAs (Saturne cup), mean follow-up 152 months (minimum 10 years).
- No prosthetic dislocation, no intraprosthetic dislocation and no acetabular osteolysis or cup loosening at final review.
- Acetabular component survivorship approximately 98% at 10 years - only stem revisions were for periprosthetic femoral fracture.
- Review of 46 reports, 5617 revision hips: 31 dual-mobility series, 15 constrained-liner (CAL) series.
- Dual mobility outperformed constrained liners: overall survivorship 94.7% vs 81.0%, dislocation 2.6% vs 11.0%, acetabular loosening 1.0% vs 2.0%.
- Mean IPD rate 0.6%; residual concern is polyethylene wear in younger, high-demand patients.
- Multicentre randomized controlled trial, 146 patients undergoing posterior-approach revision THA (76 dual mobility, 70 large head greater than or equal to 36 mm).
- At mean 18 months, dislocation was 2.6% (dual mobility) versus 4.3% (large head) - no statistically significant difference (p = 0.67), with lower-than-anticipated event rates.
- Both modern strategies markedly reduce instability; longer follow-up and full recruitment are needed to detect a difference.