Prevention Protocol | Brooker Classification | NSAIDs vs Radiation | High-Risk Groups
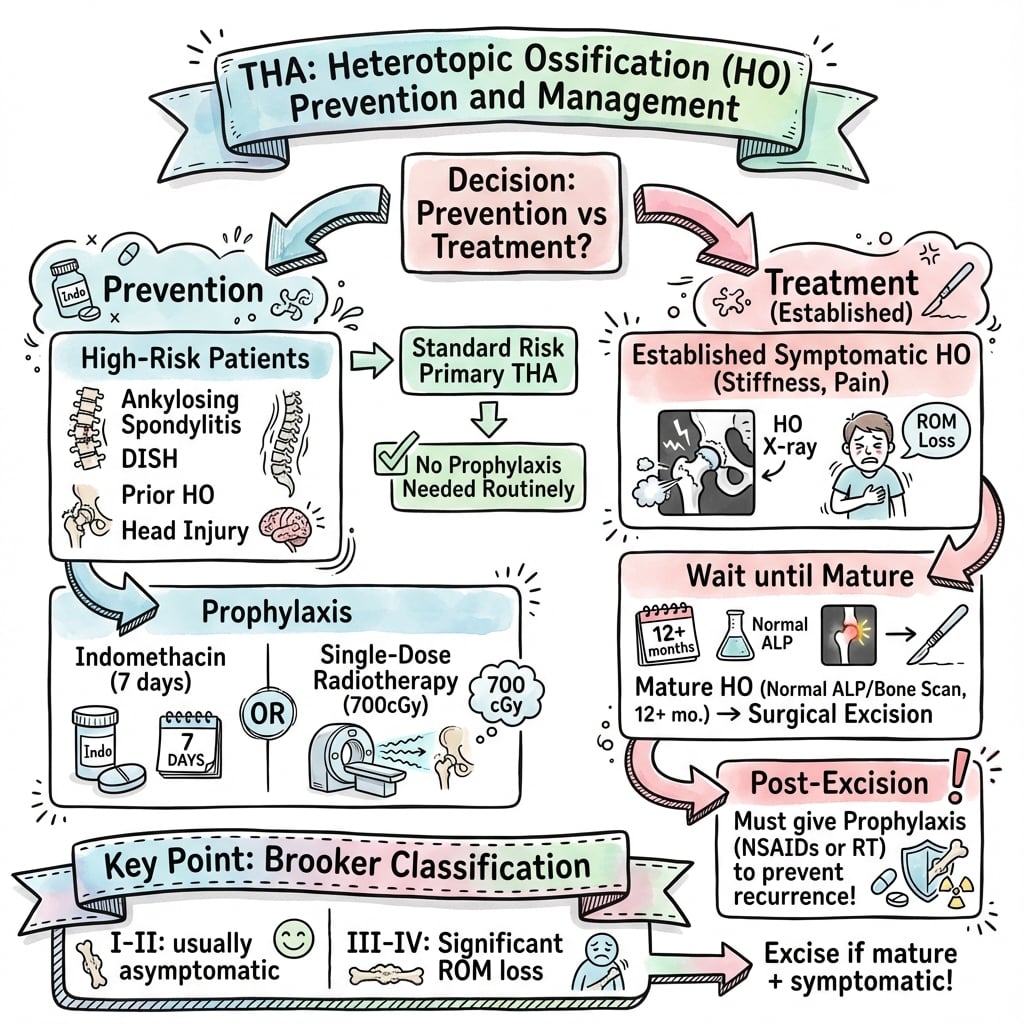
- Indomethacin 75mg daily for 6 weeks is standard NSAID prophylaxis (start within 24 hours of surgery)
- Single-dose radiation (700cGy) within 24-72 hours if NSAIDs contraindicated or high-risk revision
- Major risk factors: previous HO, ankylosing spondylitis, DISH, post-traumatic arthritis, hypertrophic OA, male gender
- DO NOT excise HO before 12-18 months maturation - high recurrence if excised early
- Brooker III-IV causes functional limitation - pain, restricted ROM, difficulty with ADLs
- “NSAIDs work by inhibiting prostaglandin synthesis preventing osteoblast differentiation
- “Radiation works by inhibiting mesenchymal stem cell differentiation and osteoblast proliferation
- “Combination NSAIDs + radiation NO additional benefit over single modality alone
- “Largest RCT (HIPAID): NSAIDs cut radiographic HO (RR 0.69) but did not improve pain/function and raised bleeding - hence selective, not universal, prophylaxis
Previous HO = 90% recurrence without prophylaxis. Ankylosing spondylitis, DISH, post-traumatic OA (especially acetabular fractures), hypertrophic OA, male gender, approach-dependent risk (anterolateral higher than posterior).
NSAIDs: Start within 24 hours, continue 6 weeks. Radiation: Single dose 700cGy within 24-72 hours post-op OR single dose pre-op (4 hours before incision). Late prophylaxis ineffective.
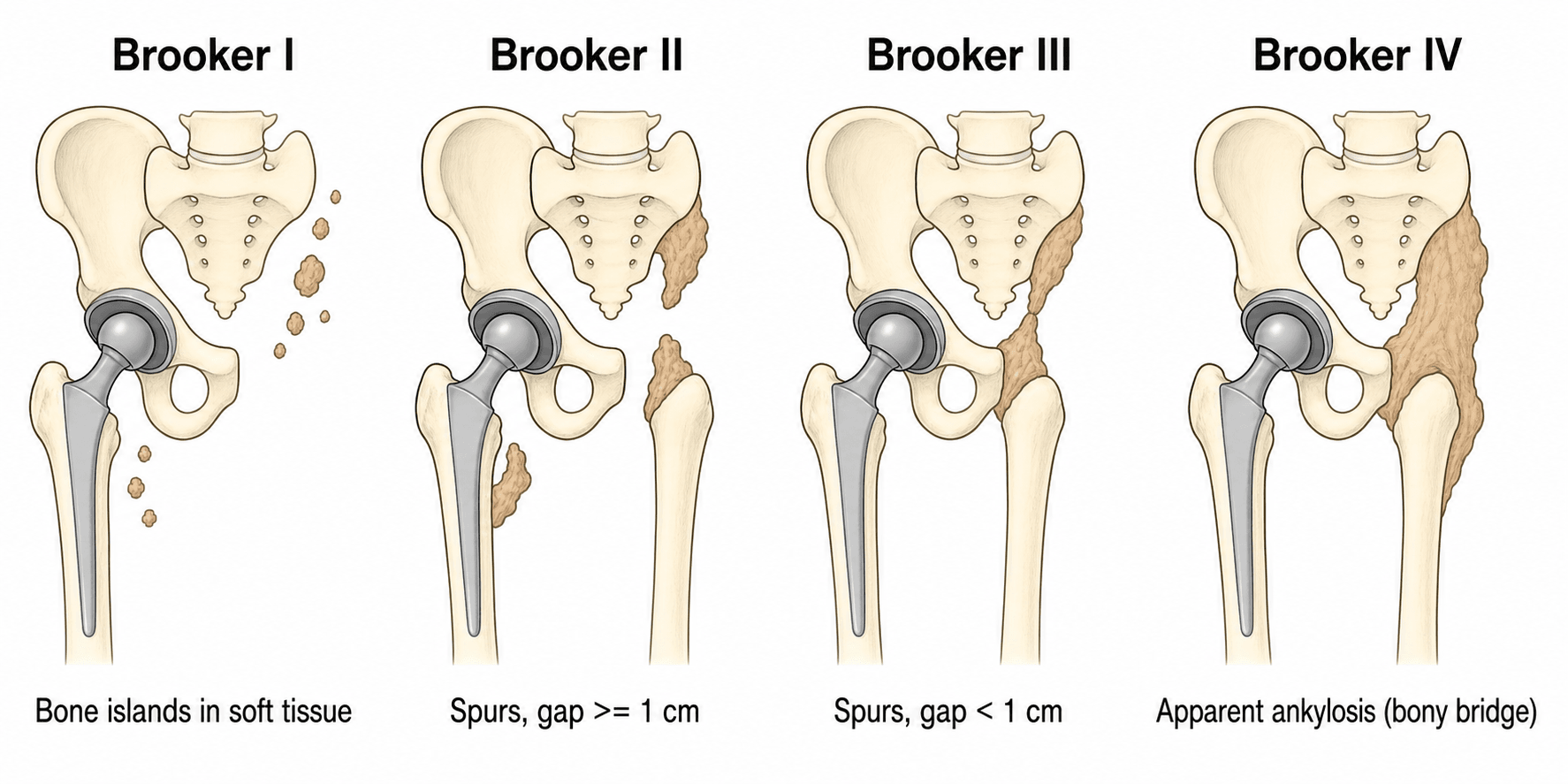
I = islands in soft tissue. II = gap over 1cm between spurs. III = gap under 1cm. IV = ankylosis. Only III-IV functionally significant. Assess at 6-12 months on AP pelvis radiograph.
Wait 12-18 months for maturation (cold bone scan, normal ALP). Re-prophylax at excision (radiation preferred over NSAIDs). Revision THA + HO excision = highest recurrence without prophylaxis.
- Prophylaxis Strategy
- Routine NSAIDs (indomethacin 75mg daily)
- Timing
- Start within 24h, continue 6 weeks
- Key Pearl
- Reduces severe HO from 7% to 2%
- Prophylaxis Strategy
- NSAIDs OR single-dose radiation (700cGy)
- Timing
- NSAID: start within 24h; Radiation: within 72h post-op
- Key Pearl
- Either modality equally effective in high-risk
- Prophylaxis Strategy
- Single-dose radiation (700cGy) preferred
- Timing
- Pre-op (4h before incision) OR within 24h post-op
- Key Pearl
- Recurrence 20-30% without prophylaxis
- Prophylaxis Strategy
- Single-dose radiation only option
- Timing
- Within 24-72 hours post-op
- Key Pearl
- No increased wound complications
ASHAMEDHigh-Risk Factors for HO (ASHAMED)
Hook:Be ASHAMED if you forget prophylaxis in these patients - they WILL form HO!
PROSPERNSAIDs Mechanism (PROSPER)
Hook:NSAIDs help patients PROSPER after THA by preventing the prostaglandin-mediated bone formation!
Overview and Epidemiology
Heterotopic ossification (HO) is the formation of mature lamellar bone in soft tissues around the hip following total hip arthroplasty. It represents abnormal differentiation of pluripotent mesenchymal stem cells into osteoblasts in response to local and systemic factors.
While mild HO (Brooker I-II) is often asymptomatic and clinically insignificant, severe HO (Brooker III-IV) occurs in 5-20% of patients without prophylaxis and causes substantial morbidity: restricted range of motion (especially internal rotation and flexion), pain with movement, difficulty with sitting and personal hygiene, and in extreme cases (Brooker IV) complete ankylosis requiring revision surgery.
- Age: Older patients slightly higher risk
- Gender: Males 2-3 times higher risk than females
- Indication: Post-traumatic arthritis 50-90%, ankylosing spondylitis 50%, primary OA 3-7%
- Previous HO: 90% recurrence risk without prophylaxis
- Genetic factors: HLA-B27 association in ankylosing spondylitis
- ROM restriction: Loss of 20-50 degrees flexion/rotation in Brooker III-IV
- Pain: 30-40% of Brooker III patients report pain
- ADL limitation: Difficulty with sitting, shoe tying, toileting
- Revision rate: 1-3% require HO excision for function
- Cost: Prophylaxis cost-effective compared to revision surgery
Pathophysiology and Molecular Mechanisms
HO formation requires three elements: osteogenic precursor cells (mesenchymal stem cells in traumatized tissue), inducing factors (BMPs, inflammatory cytokines), and permissive environment (adequate vascularization, local hypoxia). All three must be present - prophylaxis interrupts the cellular differentiation pathway.
Cellular Cascade
The formation of heterotopic bone follows a predictable sequence initiated at the time of surgical trauma:
Phase 1 (0-48 hours): Inflammation and Induction
- Surgical trauma releases inflammatory mediators (IL-1, IL-6, TNF-alpha)
- Tissue hypoxia and local hematoma formation
- BMPs released from bone debris and soft tissue damage
- Mesenchymal stem cells recruited to trauma site
Phase 2 (2-7 days): Differentiation
- Prostaglandin E2 (PGE2) drives stem cell differentiation toward osteoblasts
- NSAIDs block COX-2 enzyme preventing PGE2 synthesis
- Radiation induces DNA damage in rapidly dividing mesenchymal cells
- Critical window where prophylaxis is effective
Phase 3 (1-6 weeks): Proliferation
- Osteoblast proliferation and matrix production
- Primitive woven bone formation
- Continued NSAID prophylaxis prevents ongoing differentiation
- Late prophylaxis ineffective after osteoblasts established
Phase 4 (6-18 months): Maturation
- Woven bone remodels to mature lamellar bone
- Vascular channels develop
- Bone scan activity decreases
- Alkaline phosphatase normalizes (marker of maturation)
- Target
- Prostaglandin synthesis inhibition
- Timing Window
- Start within 24h, continue 6 weeks
- Clinical Effect
- Prevents mesenchymal stem cell differentiation to osteoblasts
- Target
- DNA damage in dividing cells
- Timing Window
- Within 24-72h post-op (or pre-op)
- Clinical Effect
- Inhibits mesenchymal cell proliferation and osteoblast function
- Target
- Block osteogenic signaling
- Timing Window
- Early post-operative period
- Clinical Effect
- Not yet clinically available - research phase
Classification Systems
Brooker Classification (Most Widely Used)
The Brooker classification is the gold standard for grading HO after THA. It is based on AP pelvis radiograph findings and correlates well with clinical significance.
- Radiographic Features
- Islands of bone within soft tissues around hip
- Functional Impact
- None - incidental finding
- Management
- No treatment required, reassurance
- Radiographic Features
- Bone spurs from pelvis or proximal femur with gap greater than 1cm between opposing surfaces
- Functional Impact
- Minimal - usually asymptomatic
- Management
- Observation, rarely symptomatic
- Radiographic Features
- Bone spurs from pelvis or proximal femur with gap less than 1cm
- Functional Impact
- Moderate - reduced ROM (20-50 degrees), may cause pain
- Management
- Consider excision if symptomatic and mature
- Radiographic Features
- Apparent radiographic ankylosis (bone bridging)
- Functional Impact
- Severe - marked ROM restriction, pain, ADL limitation
- Management
- Excision + prophylaxis if significant functional loss
The key distinction between Brooker II and III is the 1cm gap between opposing bone surfaces. Measure the smallest distance between proximal femoral HO and pelvic HO on AP radiograph. Brooker III-IV are clinically significant because they mechanically block hip motion, whereas I-II do not contact opposing surfaces and thus allow full ROM.
BIGABrooker Classification (B-I-G-A)
Hook:Think B-I-G-A: Brooker classification gets progressively BIGGER and closer until Ankylosis!
Clinical Assessment
- Pain: Location (anterior groin, lateral), character (mechanical vs inflammatory)
- ROM limitation: Which movements restricted (flexion, internal rotation, abduction)
- ADL impact: Difficulty with sitting, shoe tying, toileting, sexual function
- Timeline: When did symptoms develop (early vs late)
- Previous HO: History of HO in contralateral hip or previous surgery
- Risk factors: Ankylosing spondylitis, DISH, post-traumatic arthritis, burns, spinal cord injury
- ROM: Measure active and passive flexion, internal rotation, abduction
- End-feel: Hard block to motion (bone) vs soft tissue restriction
- Palpation: Firm mass in soft tissue (especially anterolateral)
- Gait: Antalgic or Trendelenburg pattern
- Functional tests: Ability to sit in chair, tie shoes, cross legs
- Compare to contralateral: Asymmetry suggests HO vs stiffness
NOT all post-THA stiffness is HO. Differential includes: component malposition (excessive anteversion/retroversion, high offset), adhesive capsulitis, psoas impingement, abductor deficiency (compensatory stiffness), infection (stiffness + pain + systemic signs), instability (patient guards against provocative positions). Always assess for these before attributing stiffness to HO alone.
- Key Discriminating Features
- Hard bony end-feel, palpable firm mass, ossification on radiograph, often male/high-risk indication
- First-line Investigation
- AP pelvis radiograph (Brooker grade); CT if excision considered
- Key Discriminating Features
- Rest and night pain, warmth, effusion, raised CRP/ESR, sometimes sinus
- First-line Investigation
- CRP/ESR then image-guided aspiration for cell count and culture
- Key Discriminating Features
- Positional pain or clunk, restricted motion in specific arcs, malposition on imaging
- First-line Investigation
- Radiograph plus CT for version and offset measurement
- Key Discriminating Features
- Anterior groin pain on active hip flexion and stairs, prominent or oversized cup
- First-line Investigation
- Targeted radiograph; ultrasound-guided diagnostic injection
- Key Discriminating Features
- Lateral pain, Trendelenburg gait, weakness rather than true bony block
- First-line Investigation
- Clinical examination; MRI of abductor mechanism
- Key Discriminating Features
- Soft end-feel, global loss of motion, no ossification on imaging
- First-line Investigation
- Radiograph to exclude HO; clinical diagnosis of exclusion
Physical Examination Technique
- Flexion: Supine, hip and knee flexed - measure angle between thigh and trunk (normal 120 degrees)
- Internal rotation: Prone or sitting, knee flexed 90 degrees, rotate foot laterally (normal 30-40 degrees)
- External rotation: Prone or sitting, knee flexed 90 degrees, rotate foot medially (normal 40-50 degrees)
- Abduction: Supine, stabilize pelvis, abduct hip (normal 40-50 degrees)
- Adduction: Supine, cross leg over midline (normal 20-30 degrees)
- Extension: Prone or Thomas test position (normal 10-20 degrees)
- Flexion limited to 70-90 degrees (vs normal 120)
- Internal rotation 0-10 degrees (vs normal 30-40)
- Hard end-feel to motion (bone block)
- Pain with forced motion
Acute Early Presentation: Distinguishing Developing HO from Infection and DVT
The pathophysiology section describes an early inflammatory phase, and the differential table above addresses the established stiff hip. Developing HO in the first few post-operative weeks, however, has its own acute presentation that is easily mistaken for periprosthetic joint infection (PJI) or deep vein thrombosis (DVT) - the two diagnoses that must not be missed.
- Early developing HO
- Weeks 2-8: warm, swollen, mildly painful hip with falling range of motion, sometimes low-grade fever
- Periprosthetic infection
- Any time: rest and night pain, effusion, warmth, possible wound discharge or sinus
- DVT
- First post-op weeks: calf pain and swelling more than hip
- Early developing HO
- ESR/CRP mildly raised (often surgery-related); alkaline phosphatase rises with active bone formation
- Periprosthetic infection
- CRP and ESR persistently and markedly raised
- DVT
- Inflammatory markers usually normal; D-dimer non-specific post-op
- Early developing HO
- Three-phase bone scan turns positive before radiographic change; plain radiograph often normal early (immature osteoid not yet mineralised)
- Periprosthetic infection
- Image-guided aspiration: synovial cell count and differential plus culture
- DVT
- Doppler ultrasound of the limb
- Early developing HO
- Exclude infection and DVT first; gentle range of motion; HO is immature so do NOT excise
- Periprosthetic infection
- Treat on the PJI pathway (see THA infection topic)
- DVT
- Anticoagulate per protocol
In the first 2-8 weeks after THA, developing HO can present as a warm, stiff, mildly painful hip with a rising alkaline phosphatase but a NORMAL radiograph, because immature osteoid has not yet mineralised. Exclude the two can't-miss diagnoses first - periprosthetic infection (image-guided aspiration) and DVT (Doppler ultrasound) - before attributing the picture to HO. ALP and ESR/CRP are non-specific after surgery; a three-phase bone scan turns positive before plain films. HO at this stage is immature, so this is a window for gentle range-of-motion - never for excision. Note that NSAID prophylaxis is only effective if started within 24 hours, so a hip first presenting at several weeks is generally past the prophylaxis window.
Investigations

Diagnostic Imaging Protocol
Assess for early HO formation. May show subtle soft tissue ossification. Too early for Brooker classification (bone not yet mature). Compare to immediate post-operative radiograph.
Brooker classification. Bone more mature, pattern clearer. AP pelvis shows full extent of HO. Lateral hip assesses anterior vs posterior location. Document ROM at this visit.
CT: 3D reconstruction shows exact HO location, relationship to prosthesis, bone maturity. Bone scan: "Cold" scan (no increased uptake) confirms maturation - safe to excise. Hot scan = immature = high recurrence if excised.
Normal ALP suggests maturation complete. Elevated ALP indicates active bone formation - delay excision. Trend ALP over 3-6 months. Return to baseline suggests maturity.
- Brooker grade (I-IV)
- Location: Anterior, lateral, posterior, medial
- Proximity to components: Impinging on acetabular rim, femoral neck
- Maturation: Corticated margins suggest maturity
- Progression: Compare to previous radiographs
- Bilateral: Check contralateral hip for HO
- CT scan: Pre-operative planning for HO excision (3D mapping)
- Bone scan: Assessing maturation before excision (must be cold)
- MRI: Rarely needed - if suspecting soft tissue pathology
- Fluoroscopy: Dynamic assessment of impingement
- Serial ALP: Trending bone formation activity
Management Algorithm
Non-Operative Management (Brooker I-II, Asymptomatic III)
Most HO does not require treatment. Observation with reassurance is appropriate when HO is asymptomatic or minimally symptomatic.
- Brooker I-II: Asymptomatic (90% of cases)
- Brooker III: Minimal symptoms, acceptable ROM for ADLs
- Brooker IV: Patient declines surgery, medical comorbidities prohibit surgery
- Immature HO: Less than 12 months post-op (wait for maturation)
- Stable over time: No progression on serial radiographs
- Physiotherapy: ROM exercises (gentle, within pain limits)
- Analgesia: NSAIDs for symptom control (NOT for regression)
- Activity modification: Avoid extreme positions
- Serial monitoring: Radiographs at 3, 6, 12 months
- Patient education: Natural history, maturation timeline
A common misconception is that established HO can regress with physiotherapy or NSAIDs. Once mature lamellar bone has formed, it does NOT resorb spontaneously. NSAIDs prevent NEW formation but do NOT reverse existing HO. Physiotherapy maintains ROM but does NOT reduce bone mass. Surgical excision is the ONLY method to remove HO.
This approach avoids unnecessary surgery in the majority of patients who have minimal functional impact.
Surgical Technique - Heterotopic Ossification Excision
Surgical Approach Selection
The approach for HO excision depends on the location of the heterotopic bone and the original THA approach used.
- Use previous incision when possible (avoid multiple scars)
- Posterior HO: Posterior approach (Kocher-Langenbeck modification)
- Anterior HO: Anterior or anterolateral approach
- Circumferential HO: May need extensile approach or staged procedures
- Always identify neurovascular structures before excising HO
- CT scan with 3D reconstruction: Essential for surgical planning
- Map HO location: Anterior, lateral, posterior, medial zones
- Neurovascular relationships: Sciatic nerve, femoral vessels at risk
- Proximity to components: Avoid damaging acetabular cup or femoral stem
- Bone maturity: Corticated margins on CT suggest maturity
Patient Positioning
Setup for Posterior Approach (Most Common)
Lateral decubitus position on bean bag or hip positioner. Operative hip up. Pelvis stabilized with anterior and posterior supports. Contralateral leg flexed and padded.
Dependent leg: Pillow between legs, protect peroneal nerve at fibular head. Axilla: Ensure no pressure on brachial plexus. Greater trochanter: Pad to avoid skin pressure.
Landmarks: Expose from iliac crest to mid-thigh, anterior superior iliac spine (ASIS) to posterior superior iliac spine (PSIS). Free draping: Allow hip flexion, rotation for assessment.
This positioning allows access to posterior and lateral HO while preserving ability to assess ROM intraoperatively.
Complications
- Incidence
- 5-10% dyspepsia, 1-2% ulcer
- Risk Factors
- Age over 65, previous ulcer, H. pylori, anticoagulation
- Management
- PPI co-prescription, switch to COX-2 inhibitor, or radiation
- Incidence
- 2-5% transient dysfunction
- Risk Factors
- Pre-existing CKD, dehydration, ACE inhibitors, age over 75
- Management
- Monitor creatinine, hydrate, avoid if eGFR under 30
- Incidence
- 1-2% (COX-2 inhibitors)
- Risk Factors
- Previous MI, stroke, uncontrolled hypertension
- Management
- Use lowest effective dose, shortest duration, consider radiation
- Incidence
- 20-30% with prophylaxis, 80% without
- Risk Factors
- Early excision (less than 12 months), incomplete excision, no prophylaxis
- Management
- Wait for maturation, complete excision, radiation prophylaxis
- Incidence
- 2-5% (sciatic nerve most common)
- Risk Factors
- Extensive posterior HO, adherent to nerve, revision surgery
- Management
- Careful dissection, nerve identification, accept residual HO if needed
- Incidence
- 1-3%
- Risk Factors
- Revision surgery, diabetes, prolonged operative time
- Management
- Standard surgical site infection management, antibiotics
The most common error leading to HO recurrence is excising HO before it has matured (less than 12 months post-op). Immature HO contains active osteoblasts and mesenchymal cells that will rapidly re-form bone after excision. Wait for: (1) Cold bone scan, (2) Normal ALP, (3) Corticated radiographic margins, (4) Minimum 12-18 months post-op. Patience prevents recurrence.
Postoperative Care and Rehabilitation
NSAID Prophylaxis Timeline
Start NSAID immediately (indomethacin 25mg TDS or celecoxib 200mg BD). Administer with food to reduce GI upset. Consider PPI if high GI risk. Monitor for allergic reaction.
Continue NSAID daily. Monitor for GI symptoms (dyspepsia, nausea). Check renal function if at risk (baseline creatinine). Encourage compliance (common to discontinue early). Standard THA rehabilitation proceeds.
Continue NSAID daily. Review for side effects at follow-up visit. ROM exercises progressing. Weight-bearing as per THA protocol. Reassurance that GI symptoms usually improve.
Complete 6-week course. Stop NSAID at 6 weeks (no taper needed). Beyond 6 weeks no additional benefit. Consider repeat creatinine if renal concerns. First radiograph at 6 weeks.
- Duration: Must complete full 6 weeks (stopping early reduces efficacy)
- Timing: Take with food to reduce stomach upset
- Side effects: Notify if severe abdominal pain, black stools, reduced urine
- Interactions: Avoid other NSAIDs, anticoagulants (discuss with surgeon)
- Alternatives: If intolerable, contact surgeon (can switch to radiation)
- Week 1: Phone follow-up (tolerating medication?)
- Week 2: Review renal function if high-risk
- Week 6: Clinical review, stop NSAID, first radiograph
- Month 3: Radiograph to assess early HO formation
- Month 6-12: Final radiograph, Brooker classification
This protocol ensures optimal prophylaxis compliance while monitoring for complications.
Outcomes and Prognosis
- Key Outcomes
- Reduces severe HO from 20% to 2-5%, well-tolerated in 90%
- Predictors of Success
- Compliance (6 weeks), started within 24h, appropriate dose
- Key Outcomes
- Equal efficacy to NSAIDs, no wound complications
- Predictors of Success
- Appropriate timing (within 72h), correct dose (700cGy), adequate field
- Key Outcomes
- 30-50 degree ROM improvement, 70-80% pain relief, 20-30% recurrence
- Predictors of Success
- Maturity (over 12 months), complete excision, radiation prophylaxis, appropriate patient selection
- Key Outcomes
- Stable over time, minimal symptoms, high satisfaction
- Predictors of Success
- Brooker I-II, asymptomatic, patient reassurance, ROM maintenance
Factors associated with poor outcomes: Early excision (less than 12 months = 80% recurrence), no prophylaxis at excision (recurrence rate doubles), incomplete excision (residual HO = continued symptoms), unrealistic expectations (cannot restore normal hip ROM in all cases), nerve injury during excision (2-5% permanent deficit). Optimal outcomes require patient selection, timing, technique, and prophylaxis.
Long-Term Follow-Up Data
- ROM improvement maintained in 75% (some late loss due to capsular contracture)
- Pain relief sustained in 80% (improved from 70-80% at 1 year)
- Recurrence stabilizes at 20-30% (most occurs within 2 years)
- Patient satisfaction remains high (80%) if appropriate selection
- Revision rate for recurrent HO: 5% (second excision has higher recurrence)
- Revision specifically for HO is uncommon, since most HO is asymptomatic Brooker I-II
- Clinically significant HO is over-represented in post-traumatic and acetabular-fracture arthritis
- Male sex is consistently associated with higher HO rates than female across cohorts
- Bearing surface (ceramic vs polyethylene) is not an established driver of HO risk
Prevention Strategies
NSAID Prophylaxis (First-Line for Most Patients)
Non-selective NSAIDs and selective COX-2 inhibitors are equally effective at preventing HO. The choice depends on patient risk factors, contraindications, and local availability.
- Dose
- 25mg TDS (75mg total daily)
- Duration
- Start within 24h, continue 6 weeks
- Notes
- Most studied, gold standard, higher GI side effects
- Dose
- 200mg BD (400mg total daily)
- Duration
- Start within 24h, continue 6 weeks
- Notes
- Lower GI risk, cardiovascular precautions in high-risk
- Dose
- 500mg BD (1000mg total daily)
- Duration
- Start within 24h, continue 6 weeks
- Notes
- Alternative if indomethacin not tolerated
- Dose
- 50mg TDS (150mg total daily)
- Duration
- Start within 24h, continue 6 weeks
- Notes
- Widely available, intermediate GI risk
Absolute contraindications: Active peptic ulcer disease, recent GI bleed, severe renal impairment (eGFR less than 30), aspirin-sensitive asthma. Relative contraindications: History of peptic ulcer (use PPI cover), hypertension (monitor), heart failure, anticoagulation (increased bleeding risk). Consider radiation prophylaxis instead if contraindications present.
Evidence for NSAIDs
- Efficacy: Reduces severe HO (Brooker III-IV) from 20% to 2-5% in high-risk patients
- Timing critical: Must start within 24 hours - delayed prophylaxis ineffective
- Duration: 6 weeks optimal (shorter duration less effective, longer no additional benefit)
- All NSAIDs equally effective: No single agent superior, choice based on side effect profile
- No effect on osseointegration: Does NOT impair bone-implant interface or fracture healing at standard doses
These prevention strategies work by interrupting the early stem cell differentiation cascade.
Surgical Approach and Intra-operative Measures to Reduce HO
The risk-factor sections repeatedly note that direct lateral and anterolateral exposures carry higher HO rates than the posterior approach. Approach choice and meticulous intra-operative technique are modifiable contributors and are worth setting out alongside pharmacological and radiation prophylaxis.
- Effect on HO Risk
- Generally reported with higher HO rates - more abductor dissection and muscle trauma
- Practical Measure
- Apply more aggressive prophylaxis to high-risk hips done through these approaches
- Effect on HO Risk
- Generally reported with lower HO rates than transgluteal approaches
- Practical Measure
- Still prophylax the high-risk hip regardless of approach
- Effect on HO Risk
- Internervous, muscle-sparing; reported HO rates are variable and the data are mixed
- Practical Measure
- Do not assume HO immunity - apply the same risk stratification
- Effect on HO Risk
- Osteogenic precursor cells arise from local operative-field tissue (Pellegrini 1996, PMID 8666605), so bone dust and marrow debris left in soft tissues can seed HO
- Practical Measure
- Copious pulsatile lavage before closure to wash out reamings and bone dust
- Effect on HO Risk
- Muscle crush or devitalisation and post-op haematoma provide an inflammatory substrate for HO
- Practical Measure
- Gentle soft-tissue handling, meticulous haemostasis, consider tranexamic acid and a drain in high-risk excisions
Pellegrini's RCT showed pre-operative irradiation is as effective as post-operative, which tells us the osteogenic precursor cells driving HO arise from LOCAL operative-field tissue rather than the bloodstream (PMID 8666605). The practical corollary in every THA is to remove the local trigger: copious pulsatile lavage to wash out reamings, bone dust and marrow debris before closure, gentle muscle handling, and meticulous haemostasis to avoid a haematoma. Transgluteal (direct lateral or anterolateral) approaches are reported with higher HO rates than the posterior approach, but no approach - including the muscle-sparing direct anterior - confers immunity, so risk-stratify and prophylax accordingly. These intra-operative measures are pragmatic and supported by observational data rather than level-1 trials.
Guidelines, Registries & Global Practice
Global Epidemiology (Evidence-Based)
- Any HO (Brooker I-IV)
- Up to ~50% any-grade radiographic HO
- Severe HO (Brooker III-IV)
- Roughly 0 to 10% severe
- Source
- Shapira 2021 meta-analysis (PMID 33736491)
- Any HO (Brooker I-IV)
- ~28% develop any HO (Brooker 0 in ~72%)
- Severe HO (Brooker III-IV)
- Brooker III-IV ~1%
- Source
- Migliorini 2022 meta-analysis (PMID 35809109)
- Any HO (Brooker I-IV)
- Confirmed high rate (~48% in trial population)
- Severe HO (Brooker III-IV)
- Substantial without prophylaxis
- Source
- Pellegrini 1996 RCT (PMID 8666605)
- Any HO (Brooker I-IV)
- Relative risk of ectopic bone 0.69 with NSAID
- Severe HO (Brooker III-IV)
- No improvement in pain or function despite less bone
- Source
- HIPAID 2006 (PMID 16885182)
Guideline & Society Positions (Side-by-Side)
- Position on Routine NSAID Prophylaxis
- No mandate for universal prophylaxis; NSAIDs or radiation reserved for high-risk hips and post-excision
- Evidence Basis
- Pooled RCT/meta-analysis evidence (Joice 2018, PMID 29954195)
- Position on Routine NSAID Prophylaxis
- No specific NICE technology guidance mandating HO prophylaxis; practice is risk-stratified and surgeon-led
- Evidence Basis
- Absence of high-quality functional benefit data (HIPAID, PMID 16885182)
- Position on Routine NSAID Prophylaxis
- Selective prophylaxis for recognised high-risk patients rather than blanket use
- Evidence Basis
- Registry and RCT evidence; bleeding signal in HIPAID
- Position on Routine NSAID Prophylaxis
- NSAIDs or single-fraction radiotherapy accepted as equivalent options in high-risk hips
- Evidence Basis
- NSAID vs radiotherapy meta-analysis (Shapira 2021, PMID 33736491)
No major society mandates universal HO prophylaxis for all THA. The pivotal HIPAID randomised trial showed NSAIDs reduce radiographic ectopic bone (relative risk 0.69) but produced no improvement in pain or function and increased major bleeding. Modern guidance is therefore risk-stratified: prophylax the demonstrably high-risk hip (previous HO, ankylosing spondylitis, DISH, post-traumatic/acetabular arthritis, hypertrophic OA), and avoid blanket prescribing.
Practice Variation
- Agent choice: Selective (COX-2) and non-selective NSAIDs are equally effective, so prescribing is driven by GI, renal and cardiovascular risk rather than anti-HO potency (Migliorini 2022, PMID 35809109).
- NSAIDs vs radiotherapy: Both reduce HO in high-risk hips; some meta-analytic data favour NSAIDs on efficacy while radiation is favoured when NSAIDs are contraindicated or after excision (Shapira 2021, PMID 33736491).
- Trauma caveat: In patients with concurrent long-bone fractures, indomethacin increases non-union risk, so radiation is preferred in this group (Burd 2003, PMID 12892193).
- Approach effect: Direct lateral/anterolateral exposures are generally reported with higher HO rates than posterior approaches, influencing local protocols.
- Registry role: National joint registries (e.g. AOANJRR) primarily capture revision events; symptomatic HO requiring excision is an uncommon indication for revision
- Reoperation for HO is rare: Few THAs are revised specifically for HO, consistent with most HO being asymptomatic Brooker I-II
- Higher-risk cohorts: Post-traumatic and acetabular-fracture arthritis carry a disproportionate share of clinically significant HO
- Approach effect: Anterolateral/direct lateral exposures are reported with higher HO rates than posterior approaches
- Sex effect: Males consistently show higher HO rates than females across cohorts
Key documentation requirements for informed consent:
HO Risk Discussion: Document that patient was counseled about HO risk factors (if present) and prevention options. Failure to offer prophylaxis in high-risk patients (previous HO, ankylosing spondylitis, post-traumatic arthritis) is defensible only if contraindications exist and documented.
Prophylaxis Consent: Document discussion of NSAID risks (GI, renal, cardiovascular) vs radiation (no increased wound/infection risk, gonadal shielding). Patient refusal of prophylaxis should be documented.
Excision Consent: If excising HO, must document discussion of: (1) Recurrence risk 20-30%, (2) Nerve injury risk 2-5%, (3) Realistic ROM expectations, (4) Alternative of observation if minimal symptoms. Excising immature HO (less than 12 months) without documenting urgent indication is difficult to defend if recurrence occurs.
Adverse Outcomes: If severe HO develops despite prophylaxis (2-5% even with prophylaxis), documentation of appropriate prophylaxis dose, timing, and duration protects against litigation. If patient developed GI bleed on NSAIDs, documentation of pre-prescription risk assessment and PPI consideration is critical.
Common litigation scenarios: (1) No prophylaxis offered in high-risk patient who develops severe HO, (2) NSAID-related GI bleed without documented risk assessment, (3) Early HO excision (less than 12 months) leading to recurrence, (4) Nerve injury during HO excision without documented consent discussion.
MCQ Practice Points
Q: What is the primary mechanism by which NSAIDs prevent heterotopic ossification? A: NSAIDs inhibit cyclooxygenase (COX) enzymes, preventing prostaglandin E2 (PGE2) synthesis. PGE2 is a critical mediator of mesenchymal stem cell differentiation into osteoblasts. By blocking PGE2 production during the early post-operative period (0-6 weeks), NSAIDs prevent the cellular cascade that leads to heterotopic bone formation. This is why timing is critical - NSAIDs must be started within 24 hours to interrupt the initial stem cell differentiation phase.
Q: What is the key distinguishing feature between Brooker grade II and grade III heterotopic ossification? A: The distance between opposing bone surfaces: greater than 1cm = Brooker II; less than 1cm = Brooker III. Both grades involve bone spurs projecting from the pelvis or proximal femur, but Brooker III has spurs that are close enough (less than 1cm gap) to mechanically impinge and restrict range of motion. Brooker II maintains a gap greater than 1cm and is usually asymptomatic. This distinction is critical because Brooker III-IV are functionally significant and may require treatment, while I-II are typically observed.
Q: A patient with ankylosing spondylitis requires THA. What is the most appropriate HO prophylaxis strategy? A: Either NSAIDs (indomethacin 75mg daily × 6 weeks) OR single-dose radiation (700cGy) - both are equally effective in high-risk patients. Ankylosing spondylitis is a very high-risk condition for HO (50% severe HO without prophylaxis). The choice depends on patient factors: if NSAID contraindications (GI, renal), use radiation; if radiation unavailable or patient preference, use NSAIDs. There is NO additional benefit to combining both modalities. Key is to ensure whichever modality is chosen is given at the correct dose and timing.
Q: At what minimum time point post-THA is it safe to excise heterotopic ossification, and how do you confirm maturation? A: Minimum 12-18 months post-operatively, confirmed by cold technetium-99m bone scan and normalized alkaline phosphatase. Excising immature HO leads to 80% recurrence because active osteoblasts and mesenchymal stem cells remain viable and rapidly re-form bone. Mature HO shows corticated margins on radiograph, no increased uptake on bone scan (cold scan), and normal serum ALP. Time alone is insufficient - maturation must be confirmed biochemically and scintigraphically. For Brooker IV, wait 18-24 months to ensure complete maturation.
Q: A patient undergoes HO excision 15 months post-THA. What prophylaxis should be given, and what is the expected recurrence rate? A: Single-dose radiation 700cGy (preferred) given pre-operatively or within 24 hours post-operatively; recurrence rate 20-30% with radiation, 50-80% without. Radiation is more effective than NSAIDs at preventing recurrence after HO excision, likely because the local environment is already primed for bone formation and radiation directly targets proliferating osteoblasts. NSAIDs can be used but have higher recurrence. Complete excision of all HO is essential - incomplete excision dramatically increases recurrence. Even with optimal technique and prophylaxis, recurrence occurs in 20-30% of cases.
Q: What are the key findings from randomized trials comparing NSAIDs to radiation for HO prophylaxis? A: Equally effective (both reduce severe HO from 20% to 2-5%), no difference in wound complications or infection rates, choice based on patient factors and logistics. Multiple RCTs have shown equivalent efficacy. NSAIDs have GI and renal side effects (10-15% discontinuation rate) but are simple to prescribe. Radiation has no systemic side effects but requires radiation oncology coordination. Combination therapy (NSAIDs + radiation) provides NO additional benefit over single modality. Patient contraindications and institutional resources guide choice.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You are planning a primary total hip arthroplasty for a 62-year-old male with primary osteoarthritis. He has hypertrophic osteophytes on radiographs. What is your strategy for heterotopic ossification prophylaxis?”
“A 58-year-old male had a right total hip arthroplasty 3 years ago and developed Brooker grade III heterotopic ossification. He now requires a left total hip arthroplasty for symptomatic osteoarthritis. His right hip is pain-free but has reduced flexion to 80 degrees and internal rotation 5 degrees. How do you manage HO risk for the planned left THA?”
“A 55-year-old male is 14 months post-THA for post-traumatic arthritis following an acetabular fracture. He has Brooker grade IV heterotopic ossification with hip flexion limited to 60 degrees and internal rotation 0 degrees. He has significant difficulty sitting and toileting. AP pelvis radiograph shows extensive anterior and lateral HO bridging the femur and pelvis. How do you manage this patient?”
High-Risk Factors (ASHAMED)
- Ankylosing spondylitis (50% severe HO without prophylaxis)
- Spinal cord injury (neurologic HO risk)
- Hypertrophic osteoarthritis (large osteophytes predict HO)
- Acetabular fracture/post-traumatic OA (50-90% risk)
- Male gender (2-3× higher risk than females)
- Extensive soft tissue damage (revision THA, difficult exposures)
- DISH - diffuse idiopathic skeletal hyperostosis
Brooker Classification
- I = Islands of bone in soft tissue (asymptomatic, observe)
- II = Spurs with gap greater than 1cm (usually asymptomatic)
- III = Spurs with gap less than 1cm (may restrict ROM, consider excision)
- IV = Ankylosis (significant functional loss, excision often needed)
- Assess on AP pelvis at 6-12 months post-op
Prophylaxis Protocol
- NSAIDs: Indomethacin 75mg daily × 6 weeks (start within 24h)
- COX-2 inhibitors: Celecoxib 200mg BD × 6 weeks (lower GI risk)
- Radiation: 700cGy single dose within 24-72h post-op (or pre-op)
- Both modalities equally effective (reduce severe HO from 20% to 2-5%)
- NO benefit from combining NSAIDs + radiation
- Previous HO = 90% recurrence without prophylaxis (radiation preferred)
Excision Pearls
- Wait 12-18 months minimum (Brooker III) or 18-24 months (Brooker IV)
- Confirm maturation: cold bone scan + normal ALP + corticated margins
- Pre-op CT with 3D reconstruction for surgical planning
- Complete excision essential (incomplete = recurrence)
- Radiation prophylaxis 700cGy at excision (preferred over NSAIDs)
- Recurrence: 20-30% with prophylaxis; 50-80% without; 82% if excised before 12 months
- Nerve injury risk 2-5% (sciatic most common)
- ROM improvement: 30-50 degrees; Pain relief: 70-80%
Complications to Counsel
- NSAID GI toxicity: 5-10% dyspepsia, 1-2% ulcer (use PPI in high-risk)
- NSAID renal impairment: 2-5% (monitor creatinine, avoid if eGFR under 30)
- NSAID CV events: 1-2% with COX-2 inhibitors (caution in cardiac patients)
- HO recurrence post-excision: 20-30% with prophylaxis, 80% without
- Nerve injury during excision: 2-5% (sciatic - permanent deficit possible)
- Infection after excision: 1-3% (standard wound infection management)
Evidence Base and Key Trials
Brooker Classification of Ectopic Ossification After THR (Original Description)
- Original case series defining the four-grade radiographic classification still used worldwide today
- Grade I: islands of bone within soft tissues; Grade II: bone from pelvis or femur leaving over 1cm between opposing surfaces
- Grade III: bone spurs leaving less than 1cm between opposing surfaces; Grade IV: apparent bony ankylosis
- Provided a reproducible method to report incidence and severity of ectopic bone after hip replacement
Routine Ibuprofen Prophylaxis After Hip Replacement (HIPAID RCT)
- Double-blind placebo-controlled RCT of 902 primary or revision THA patients across 20 Australian and New Zealand centres
- Ibuprofen 1200mg daily for 14 days started within 24h reduced ectopic bone formation (relative risk 0.69, 95% CI 0.56 to 0.83)
- Despite less ectopic bone, there was NO improvement in WOMAC hip pain or physical function at 6 to 12 months
- Ibuprofen significantly increased major bleeding complications during admission (relative risk 2.09, 95% CI 1.00 to 4.39)
- Authors concluded the data do not support routine NSAID prophylaxis for unselected THA patients
Pre-operative vs Post-operative Irradiation for HO Prevention (RCT)
- 86 high-risk hips randomised to a single 800cGy fraction given pre-operatively (within ~6h) or post-operatively (within ~51h)
- No new HO in 76% of pre-operatively irradiated hips and 73% of post-operatively irradiated hips (equivalent efficacy)
- Extra-field ossification was more common after pre-operative irradiation (24% vs 8%, p = 0.05)
- Findings support that osteogenic precursor cells arise from local operative-field tissue rather than blood-borne cells
Reliability of the Brooker System and a Simplified Classification
- Six observers graded 169 THA radiographs using the Brooker classification and a simplified three-grade system
- Interobserver agreement for the four-grade Brooker system was poor (mean kappa 0.43)
- A simplified three-grade system improved interobserver reliability (mean kappa 0.59) and intraobserver agreement (kappa 0.78)
- Consistency for detecting clinically significant (severe) HO improved from 52% to 76% with the simplified system
Selective vs Non-selective NSAIDs for HO Prophylaxis (Meta-analysis)
- Meta-analysis of 8 studies and 1526 patients comparing selective (COX-2) versus non-selective NSAIDs after THA
- No statistically significant difference in efficacy between selective and non-selective NSAIDs
- 72% of patients were Brooker 0 and only ~1% reached clinically significant Brooker III-IV across the pooled cohort
- Choice of agent can therefore be guided by side-effect profile rather than anti-HO potency
Indomethacin HO Prophylaxis and Long-bone Non-union Risk (RCT Subanalysis)
- 112 patients with an acetabular fracture plus a concomitant long-bone fracture, randomised to indomethacin, focal radiation, or no HO prophylaxis
- Long-bone non-union occurred in 26% of those receiving indomethacin versus 7% of those who did not (p = 0.004)
- Radiation prophylaxis was not associated with the increased non-union risk seen with indomethacin
- Demonstrates a clinically important systemic harm of NSAID HO prophylaxis in patients with other fractures