Prevention-First | Recognition Patterns | Salvage Techniques
- Sciatic nerve: 80% of nerve injuries, peroneal division affected more than tibial
- Risk factors: developmental dysplasia, revision surgery, lengthening over 4cm, posterior approach
- Clinical signs: immediate foot drop (peroneal), calf pain with ankle plantarflexion (vascular)
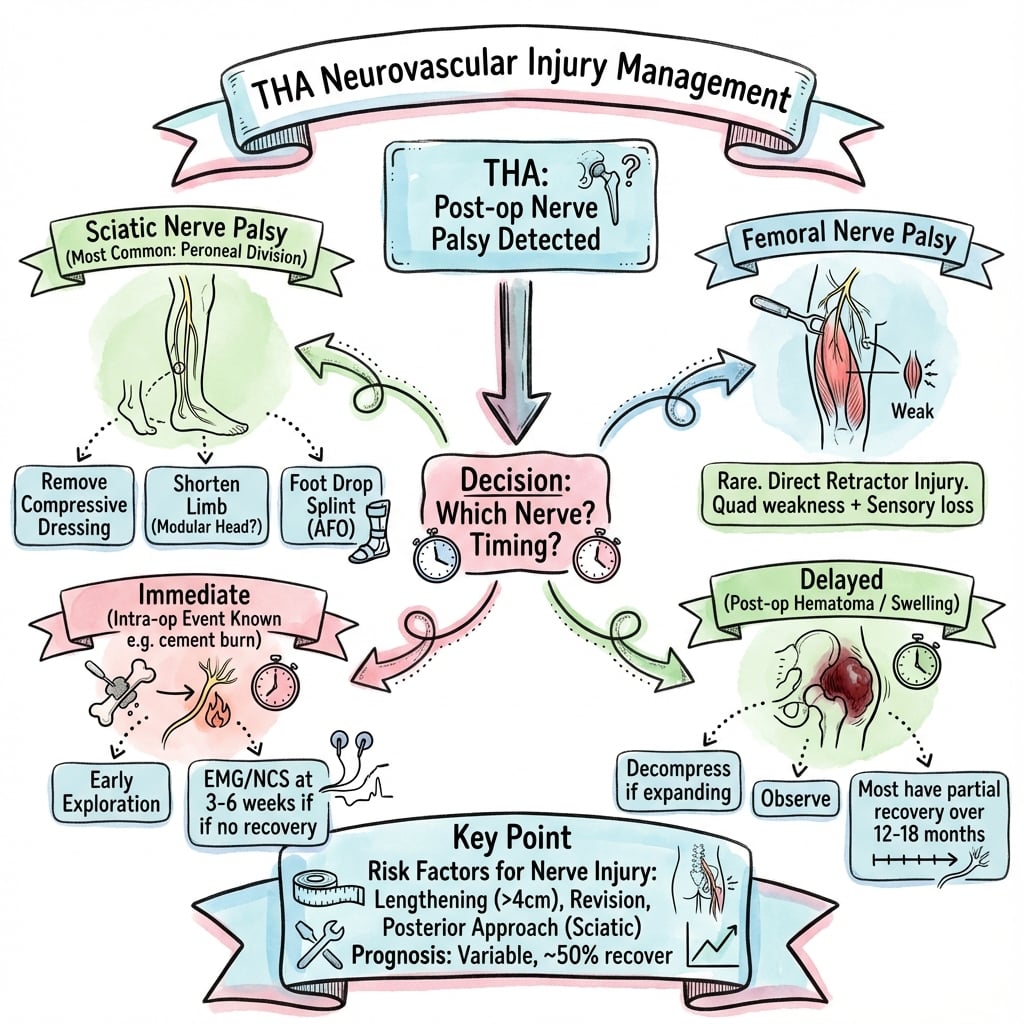
- Management: immediate component removal if lengthening over 4cm with nerve palsy
- Prognosis: 40-70% recovery with neuropraxia, poor recovery with complete nerve division
- “Always check limb length intraoperatively before final component insertion
- “Sciatic nerve most at risk with posterior approach; femoral nerve with anterior approach
- “Vascular injury may present with delayed compartment syndrome (24-48 hours)
- “Early exploration (within 72 hours) improves nerve recovery outcomes
Developmental dysplasia of hip (DDH) requires meticulous planning. Sciatic nerve at risk with inferior hip centre placement and limb lengthening. Femoral nerve vulnerable with anterior retractors.
Post-anaesthesia examination is critical. Test foot dorsiflexion, plantarflexion, and toe movements immediately. Check distal pulses and capillary refill bilaterally.
Limit limb lengthening to under 4cm. Use intraoperative fluoroscopy to verify leg lengths. Position sciatic nerve under direct vision in posterior approaches.
72-hour window for nerve exploration. Early decompression improves outcomes. Vascular injury requires immediate consultation and surgical intervention.
- Diagnosis
- Sciatic nerve injury (peroneal division)
- Immediate Action
- Document deficit, check leg length, consider revision if over 4cm lengthening
- Key Pearl
- Recovery likely if neuropraxia, document baseline EMG at 3 weeks
- Diagnosis
- Probable neurotmesis or vascular compromise
- Immediate Action
- Urgent vascular assessment, MRI/USS, early surgical exploration within 72h
- Key Pearl
- Time to decompression critical for nerve recovery
- Diagnosis
- Vascular injury with ischaemia
- Immediate Action
- Immediate vascular surgery consult, duplex USS, prepare for exploration
- Key Pearl
- Arterial injury may present with delayed compartment syndrome
- Diagnosis
- Femoral nerve injury (anterior approach complication)
- Immediate Action
- Remove anterior retractors, document deficit, observe initially
- Key Pearl
- Usually neuropraxia from retractor pressure, recovers over weeks
PALSYSigns of Sciatic Nerve Injury
Hook:Sciatic PALSY primarily affects the peroneal division - foot drop is the hallmark, recovery takes years if axons are damaged!
Overview and Epidemiology
Neurovascular complications remain among the most feared and devastating complications of total hip arthroplasty. Despite being relatively uncommon, the profound impact on patient function and quality of life makes prevention and early recognition paramount.
Nerve and vascular injuries can result in permanent disability, litigation, and patient dissatisfaction. Understanding the anatomy, risk factors, and prevention strategies is essential for safe THA practice. This is a high-yield exam topic as examiners want to ensure trainees can identify at-risk patients and manage complications appropriately.
- Sciatic nerve: 80% of all nerve injuries
- Peroneal division: affected more than tibial (lateral position, less connective tissue support)
- Femoral nerve: 10-15% of nerve injuries, associated with anterior approach
- Superior gluteal nerve: 5% of injuries, abductor weakness
- Recovery rate: 40-70% for neuropraxia, under 20% for complete transection
- External iliac artery: most commonly injured vessel
- Common femoral artery: at risk with anterior approach
- Superior/inferior gluteal vessels: posterior approach risks
- Presentation: immediate bleeding, delayed pseudoaneurysm, AVF
- Mortality risk: 5-10% with major vascular injury
Anatomy and Biomechanics
Sciatic Nerve Anatomy
The sciatic nerve is the largest nerve in the body, formed from the L4-S3 nerve roots. Understanding its anatomical course and relationships is critical for THA prevention strategies.
The sciatic nerve exits the pelvis through the greater sciatic notch, passing beneath the piriformis muscle in 85% of individuals. At the level of the hip joint, the nerve lies 2-3cm posterior to the posterior acetabular rim. This distance is critical - excessive posterior wall reaming, retractor placement, or cement extrusion can directly injure the nerve.
- Course at Hip Level
- Lateral and posterior to tibial division, 2-3cm behind acetabulum
- Injury Mechanism
- Limb lengthening over 4cm, direct trauma, retractor compression
- Clinical Consequence
- Foot drop, numbness dorsum of foot, poor recovery if axonotmesis
- Course at Hip Level
- Medial division, more connective tissue support
- Injury Mechanism
- Less commonly injured, usually with complete sciatic injury
- Clinical Consequence
- Calf weakness, sole numbness, better prognosis than peroneal
- Course at Hip Level
- Anterior to hip, beneath inguinal ligament lateral to femoral artery
- Injury Mechanism
- Anterior retractor compression, haematoma, cement extravasation
- Clinical Consequence
- Weak quadriceps, anterior thigh numbness, often neuropraxia
- Course at Hip Level
- Exits above piriformis, innervates gluteus medius and minimus
- Injury Mechanism
- Excessive superior dissection, retractor trauma during exposure
- Clinical Consequence
- Trendelenburg gait, abductor weakness, often unrecognised
Vascular Anatomy
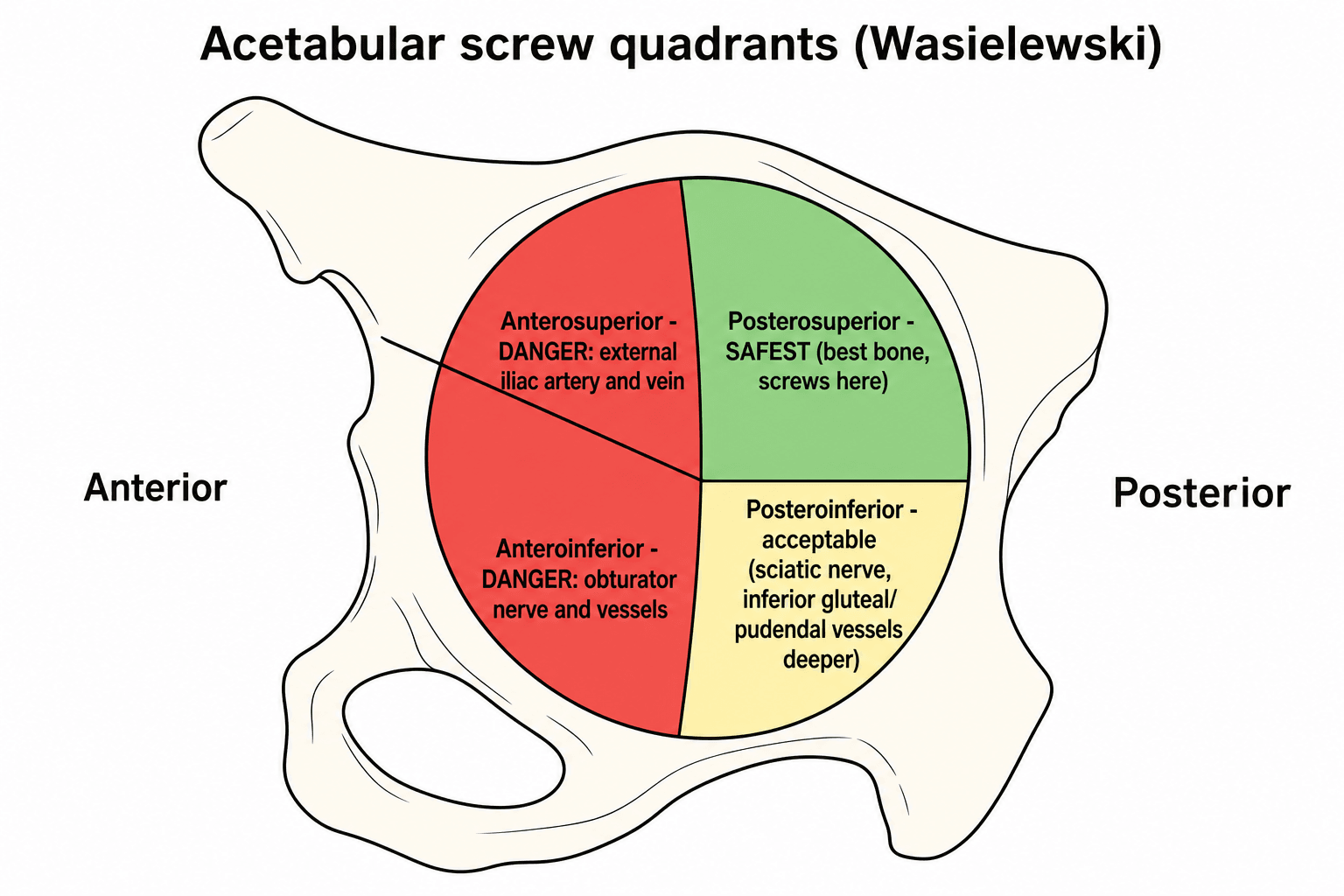
External iliac artery runs along pelvic brim, at risk with:
- Medial acetabular screw penetration
- Intrapelvic cement extravasation
- Anterior retractor overzealous placement
Common femoral artery vulnerable with:
- Anterior approach direct injury
- Femoral neck osteotomy saw injury
- Femoral canal perforation anteriorly
External iliac vein most commonly injured vessel:
- Thinner wall than artery, easily torn
- Presents with bleeding, haematoma formation
- May cause delayed DVT if unrecognised
Gluteal vessels at risk with posterior approach:
- Bleeding controlled with packing usually
- Pseudoaneurysm rare but reported
SPIDERSciatic Nerve Anatomy at Hip
Hook:The sciatic nerve is a SPIDER web of danger - runs posteriorly through the notch, divisions at risk with retraction and lengthening!
Classification Systems
Patient-Related Risk Factors
- Mechanism
- High hip centre requires inferior placement, sciatic nerve on stretch
- Risk Increase
- Up to 10 times higher risk
- Prevention Strategy
- Subtrochanteric shortening osteotomy if lengthening over 4cm planned
- Mechanism
- Scarring distorts anatomy, nerve encased in scar tissue
- Risk Increase
- 5-10 times higher risk than primary
- Prevention Strategy
- Careful dissection, consider nerve monitoring, limit lengthening
- Mechanism
- Altered anatomy from previous fracture, retained hardware
- Risk Increase
- 3-5 times higher risk
- Prevention Strategy
- Pre-operative CT imaging to plan approach and identify nerve course
- Mechanism
- Reduced nerve tolerance to stretch, scarring around nerve
- Risk Increase
- Variable, may be permanent deficit
- Prevention Strategy
- EMG/NCS pre-operatively to document baseline, avoid further trauma
In Crowe IV DDH (femoral head above roof level), the sciatic nerve is often significantly shortened due to chronic hip dislocation. Reducing the hip to anatomical centre without femoral shortening can result in over 5-6cm of limb lengthening and near-certain nerve palsy. Always plan for subtrochanteric shortening osteotomy in these cases.
Clinical Assessment and Diagnosis
Immediate Post-Operative Examination
The single most important step in diagnosing neurovascular injury is a systematic post-anaesthesia examination before the patient leaves the operating theatre.
Post-Operative Neurovascular Assessment Protocol
Before leaving theatre, assess:
- Foot dorsiflexion (peroneal division of sciatic nerve)
- Foot plantarflexion (tibial division)
- Toe extension and flexion
- Hip flexion and knee extension (femoral nerve)
- Distal pulses (dorsalis pedis, posterior tibial)
- Capillary refill bilaterally
- Compare to pre-operative baseline if documented
Document findings in medical record:
- Motor power (0-5 MRC scale)
- Sensory examination (light touch, pinprick)
- Vascular status (pulses, temperature, colour)
- Compare to contralateral limb
- Any change from pre-operative baseline
If deficit identified:
- Inform supervising consultant immediately
- Check leg length differential (clinical and radiographic)
- Review intraoperative notes for risk factors
- Consider urgent imaging if vascular concern
- Initiate management algorithm
Failure to perform immediate post-operative neurovascular examination is the most common reason for delayed diagnosis of nerve injury. Patients emerging from anaesthesia may not recognise or report subtle motor or sensory deficits. A missed nerve injury in the immediate post-operative period becomes far more difficult to prove causation and manage appropriately.
Clinical Patterns by Nerve
- Motor Deficit
- Foot drop, no ankle movement, toe paralysis
- Sensory Loss
- Entire foot below ankle numb except medial ankle
- Special Signs
- High-stepping gait, foot slap when walking
- Motor Deficit
- Foot drop, weak ankle eversion, toe extension loss
- Sensory Loss
- Dorsum of foot and lateral leg numb
- Special Signs
- Most common pattern, foot drop immediately evident
- Motor Deficit
- Weak plantarflexion, toe flexion loss, ankle inversion weak
- Sensory Loss
- Sole of foot numb, sensory loss calf posteriorly
- Special Signs
- Less common, patient may still walk but with abnormal gait
- Motor Deficit
- Weak hip flexion, unable to extend knee, quadriceps wasting
- Sensory Loss
- Anterior thigh and medial leg numbness
- Special Signs
- Unable to straight leg raise, knee buckles with weight bearing
Differential Diagnosis of Post-THA Lower-Limb Neurological Deficit
Not every post-operative motor or sensory deficit is a direct surgical nerve injury. The following differentials must be actively excluded because management differs substantially.
- Discriminating Features
- Immediate foot drop, dorsum-of-foot sensory loss, often with lengthening
- Key Investigation
- Clinical exam, leg-length radiograph, EMG/NCS at 3 weeks
- Action if Confirmed
- Assess lengthening; revise if over 4cm with complete palsy
- Discriminating Features
- Absent pulses, cold pale limb, pain out of proportion
- Key Investigation
- ABPI, duplex USS, CT angiography
- Action if Confirmed
- Immediate vascular surgery; theatre within 6h
- Discriminating Features
- Tense compartments, pain on passive stretch, 24-48h onset
- Key Investigation
- Compartment pressures (within 30mmHg of diastolic)
- Action if Confirmed
- Emergency four-compartment fasciotomy
- Discriminating Features
- Progressive (not immediate) deficit, swelling, falling haemoglobin
- Key Investigation
- USS/CT, serial haemoglobin
- Action if Confirmed
- Evacuate if progressive compression
- Discriminating Features
- Bilateral or non-dermatomal pattern, urinary retention, back pain
- Key Investigation
- Neurology review, MRI spine if epidural haematoma suspected
- Action if Confirmed
- Urgent MRI and decompression if epidural haematoma
- Discriminating Features
- Deficit in non-operative pattern or contralateral limb
- Key Investigation
- Clinical pattern recognition, EMG if persists
- Action if Confirmed
- Usually neuropraxia - observe, protect, physiotherapy
Vascular Injury Recognition
Acute vascular injury presents with:
- Absent or diminished distal pulses
- Cold, pale limb compared to contralateral
- Expanding haematoma in wound or thigh
- Hypotension if significant blood loss
- Pain out of proportion (compartment syndrome developing)
Delayed vascular complications:
- Pseudoaneurysm (pulsatile mass, bruit)
- Arteriovenous fistula (continuous thrill)
- Compartment syndrome (24-48 hours post-op)
- DVT from venous injury
- Heterotopic ossification from haematoma
Investigations
Initial Investigations
Investigation Pathway for Suspected Nerve Injury
Bedside examination:
- Systematic motor and sensory testing
- Document deficit with MRC grading
- Measure leg lengths clinically
- Assess for compartment syndrome signs
Plain radiographs (AP pelvis, lateral hip):
- Component position and orientation
- Limb length discrepancy measurement
- Femoral offset restoration
- Cement extrusion medially
- Acetabular screws penetrating medial wall
Electromyography and nerve conduction studies:
- Distinguish neuropraxia from axonotmesis
- Baseline for monitoring recovery
- Localise level of injury
- Guide prognosis discussions
MRI pelvis/hip (if surgical exploration planned):
- Nerve compression from haematoma or cement
- Assess nerve continuity
- Rule out space-occupying lesion
CT angiography (if vascular injury suspected):
- Active extravasation
- Pseudoaneurysm
- Arteriovenous fistula
Vascular Investigation Protocol
Arterial Injury Investigation
Immediate (within 1 hour):
- Duplex ultrasound (bedside) to assess flow
- Ankle-brachial pressure index (ABPI) - compare to contralateral
- Compartment pressure measurement if clinical concern
Urgent (within 6 hours):
- CT angiography (gold standard) - defines level and extent of injury
- Conventional angiography if intervention planned
Management decision:
- ABPI under 0.5 = urgent vascular surgery consultation
- Hard signs of vascular injury = immediate theatre for exploration
- Soft signs = close observation with serial ABPI and duplex
Hard signs requiring immediate exploration include absent pulses, expanding haematoma, pulsatile bleeding, and limb ischaemia.
Q: When should you perform baseline EMG/NCS after suspected nerve injury? A: 3 weeks post-injury. Earlier EMG is unhelpful as Wallerian degeneration takes 2-3 weeks to develop. Performing EMG at 3 weeks establishes baseline severity, allows distinction between neuropraxia and axonotmesis, and provides prognostic information. Repeat studies at 3 months and 6 months monitor recovery trajectory.
Management Algorithm
Nerve Injury Management Algorithm
Immediate Management (0-24 hours):
First 24 Hours
- Document deficit completely (motor, sensory)
- Review intraoperative events
- Measure leg length radiographically
- Assess severity: complete vs partial palsy
- If limb lengthening over 4cm AND complete palsy → urgent revision
- If cement extrusion compressing nerve → urgent revision
- If haematoma causing compression → urgent evacuation
- If neuropraxia likely (partial deficit, no lengthening) → observation
Criteria for urgent component removal:
- Limb lengthening over 4cm with complete sciatic palsy
- Progressive deficit (was partial, now complete)
- Severe pain suggesting nerve compression
- Vascular compromise accompanying nerve injury
If observation chosen, close neurovascular monitoring is essential.
Observation Protocol (if no immediate revision):
- Daily neurovascular examination
- Foot drop splint (ankle-foot orthosis) to prevent contractures
- Physiotherapy for passive range of motion
- EMG/NCS at 3 weeks
- Re-assess at 6 weeks, 3 months, 6 months
If nerve injury fails to improve by 72 hours, or worsens, consider surgical exploration. Early nerve decompression (within 72 hours) has been shown to improve recovery rates. Beyond 72 hours, the benefit of exploration diminishes unless there is clear evidence of compressive pathology.
Surgical Technique - Prevention Strategies
Prevention is far superior to management. This section outlines specific intraoperative techniques to minimise neurovascular injury risk.
Patient Positioning and Setup
Positioning for Nerve Protection
Standard positioning:
- Lateral position, affected side up
- Lower limb flexed at hip and knee for stability
- Upper limb (operative) free to move through range
- Pelvic posts anterior and posterior to stabilise pelvis
Nerve protection:
- Avoid excessive flexion at hip (over 90 degrees) - increases sciatic nerve tension
- Avoid extreme internal rotation - stretches sciatic nerve
- Position operative limb in 20-30 degrees flexion, neutral rotation at rest
Standard positioning:
- Supine on radiolucent table
- Operative leg on extension attachment
- Perineal post for countertraction
Nerve protection:
- Limit hip extension beyond neutral (femoral nerve stretch)
- Release anterior retractors every 15-20 minutes
- Avoid excessive lateral translation of femoral shaft (femoral nerve compression)
Proper positioning sets the foundation for safe exposure and reduces baseline nerve tension throughout the case.
Intraoperative Neuromonitoring in High-Risk THA
The guidelines section notes that some high-volume centres use intraoperative SSEP/EMG neuromonitoring for Crowe III-IV cases while routine use is not evidence-supported. The modalities and their role are worth setting out, because monitoring gives a real-time warning that allows correction before injury becomes permanent.
- What It Monitors
- Dorsal-column sensory pathway; near-continuous
- Alert / Limitation
- Alert at an amplitude drop over 50% or a latency increase over 10% from baseline; affected by anaesthesia, temperature and blood pressure (false positives)
- What It Monitors
- Corticospinal motor tracts; more sensitive to motor injury
- Alert / Limitation
- Loss of MEP signals motor compromise; requires total intravenous anaesthesia with no neuromuscular blockade
- What It Monitors
- Real-time mechanical irritation or traction of the nerve
- Alert / Limitation
- Bursts or trains warn of nerve stretch during reduction or retraction, prompting immediate correction
Neuromonitoring (SSEP, MEP, EMG) gives a real-time warning, letting the surgeon release traction, reduce lengthening or reposition a retractor before injury becomes permanent. Its role is in HIGH-RISK cases - Crowe III-IV dysplasia with large planned lengthening, complex revision, distorted post-traumatic anatomy - not routine THA, where it has not been shown to reduce permanent palsy and adds cost and false positives. MEP requires total intravenous anaesthesia without paralysis.
REVISERisk Factors for Nerve Injury in THA
Hook:REVISE your surgical plan when these risk factors are present - prevention is key to avoiding nerve complications!
The Intrapelvic Component: Vascular-Protected Revision
The topic flags medial cement extrusion and a migrated acetabular component against the external iliac vessels. When a component, screw or cement mass has breached the quadrilateral plate, removal demands a planned vascular-protected strategy, because blind extraction from the hip can be catastrophic.
- Detail
- An acetabular cup, screw or cement mass medial to the quadrilateral plate lies against the external iliac / common femoral vessels (and obturator); blind extraction from the hip risks fatal haemorrhage
- Detail
- CT, ideally CT angiography, to define the relationship of the intrapelvic hardware to the vessels; involve vascular surgery before the day of surgery
- Detail
- For hardware intimate with the vessels, plan a retroperitoneal (ilioinguinal/Stoppa) approach to control the iliac vessels first, or keep vascular surgery and an endovascular balloon-occlusion catheter on standby - do not simply pull it out from the hip
- Detail
- A well-fixed intrapelvic fragment encasing the vessels may be safer left in situ than risking vascular catastrophe; have cross-matched blood and cell salvage ready
A cup, screws or cement that has migrated medial to the quadrilateral plate sits on the external iliac vessels - the highest-stakes vascular scenario in revision THA. Before removal, obtain CT (with angiography), involve vascular surgery, and plan vessel control (retroperitoneal exposure, or an endovascular balloon-occlusion catheter on standby). Sometimes the safest decision is to leave a well-fixed intrapelvic fragment rather than precipitate uncontrollable haemorrhage.
Complications
Beyond the primary nerve and vascular injuries, several secondary complications can arise from neurovascular injury or its management.
- Incidence
- 20-60% of nerve injuries have residual deficit
- Risk Factors
- Complete transection, delayed diagnosis, axonotmesis
- Management
- AFO splint, tendon transfer (tibialis posterior to dorsum), arthrodesis
- Incidence
- 30-40% of patients with nerve injury
- Risk Factors
- Incomplete recovery, neuroma formation
- Management
- Neuropathic pain medications (gabapentin, pregabalin), pain clinic referral
- Incidence
- 5-10% of vascular injuries
- Risk Factors
- Delayed presentation, haematoma, reperfusion injury
- Management
- Immediate fasciotomy all four compartments, may require amputation if delayed
- Incidence
- Under 1% of THAs, more common in revision
- Risk Factors
- Arterial wall injury with contained rupture
- Management
- Endovascular coiling or open repair, risk of rupture if untreated
- Incidence
- Increased with haematoma and revision surgery
- Risk Factors
- Large haematoma, compromised soft tissues, multiple surgeries
- Management
- Irrigation and debridement, antibiotic suppression, may require implant removal
- Incidence
- Up to 20% with large haematoma
- Risk Factors
- Soft tissue trauma, haematoma, re-operation
- Management
- Prophylaxis with indomethacin or radiation, excision if symptomatic at 1 year
Nerve injury after THA is a common source of litigation. Key factors in defensibility:
- Documentation: Pre-operative documentation of baseline neurovascular exam
- Informed consent: Specific discussion of nerve injury risk (especially in high-risk cases)
- Intraoperative measurement: Document leg length measurement before closing
- Immediate recognition: Post-operative neurovascular exam documented in recovery room
- Appropriate management: Timely revision or observation with clear rationale documented
Failure in any of these areas significantly weakens the medicolegal position.
Postoperative Care and Rehabilitation
Immediate Post-Operative Management (0-48 hours)
First 48 Hours Care
- Neurovascular examination before leaving OR
- Document baseline neurological status
- Check leg lengths radiographically (AP pelvis)
- Ensure distal pulses present and documented
- Pain management protocol initiated
- Neurovascular checks every 4 hours for first 24 hours
- Monitor for compartment syndrome signs (pain, paraesthesia, pressure)
- Drain output monitoring (excessive bleeding may indicate vascular injury)
- Weight bearing as per protocol (protected if nerve injury suspected)
- Physiotherapy assessment for gait and transfers
- If foot drop present: AFO splint fitted
- Passive range of motion exercises to prevent contractures
- Continue neurovascular observations if deficit present
Early recognition and appropriate initial management set the foundation for optimal recovery outcomes.
Outcomes and Prognosis
Recovery Patterns by Injury Severity
- Recovery Timeline
- Days to weeks, complete by 3 months
- Expected Outcome
- Full recovery in 70-90% of cases
- Prognostic Factors
- Early signs of recovery (within 6 weeks) predict full recovery
- Recovery Timeline
- Months to years, 1mm per day regeneration
- Expected Outcome
- Partial recovery in 40-60%, significant functional deficit common
- Prognostic Factors
- Proximal injuries (at hip) have worse prognosis than distal (below knee)
- Recovery Timeline
- No spontaneous recovery expected
- Expected Outcome
- Poor outcome despite repair, under 10% useful function
- Prognostic Factors
- Surgical repair within 72 hours improves outcomes slightly
Functional Outcomes After Nerve Injury
- Partial deficit at presentation (incomplete nerve injury)
- Early improvement (within 6 weeks suggests neuropraxia)
- Young patient (better neuronal regeneration capacity)
- No lengthening (injury from transient compression, not traction)
- Isolated peroneal division (less disability than complete sciatic)
- Complete palsy from time of surgery (suggests neurotmesis)
- Limb lengthening over 4cm (traction injury, poor prognosis)
- No improvement by 6 months (unlikely to recover significantly)
- Elderly patient (reduced regeneration capacity)
- Complete sciatic nerve injury (severe functional impairment)
When counselling patients with nerve injury post-THA:
Initial conversation (first week): "We have identified a nerve injury affecting your foot movement. The majority of these injuries recover over time, though it may take many months. We will monitor closely with nerve studies at 3 weeks and 3 months."
If no recovery by 3 months: "Unfortunately, your nerve injury appears to be more severe than we initially hoped. While some continued recovery is possible over the next 12-18 months, we need to discuss adaptive strategies including ankle braces and the possibility of future tendon transfer surgery if recovery plateaus."
At 12-18 months if no recovery: "Based on the lack of significant improvement, we do not expect further spontaneous recovery. We should discuss secondary procedures such as tendon transfer or ankle fusion to improve your function and quality of life."
Honest, staged discussions aligned with recovery trajectory maintain trust and set realistic expectations.
Guidelines, Registries & Global Practice
Global Epidemiology (Evidence-Based)
- Reported Figure
- Approximately 1%
- Source
- Schmalzried 1997 (PMID 9372771)
- Note
- Canonical pooled estimate; 80% sciatic/peroneal
- Reported Figure
- 0.17% (47/27,004)
- Source
- Farrell/Morrey 2005 (PMID 16322610)
- Note
- Large single-institution series actively screening for palsy
- Reported Figure
- 0.8% overall, 1.4% in revision
- Source
- Navarro/Schmalzried 1995 (PMID 7730818)
- Note
- Revision and complexity, not approach, drive risk
- Reported Figure
- Over 90%
- Source
- De Fine 2017 systematic review (PMID 29270435)
- Note
- Peroneal division most affected
- Reported Figure
- Approximately two-thirds of cases
- Source
- De Fine 2017 (PMID 29270435); Schmalzried 1997
- Note
- Early residual motor function is the key favourable sign
The widely taught 4cm lengthening threshold is a useful pragmatic limit, but the De Fine 2017 systematic review (PMID 29270435) found no single lengthening value that reliably separates safe from unsafe. Risk reflects a combination of patient factors (DDH, prior surgery, female sex) and intra-operative handling, so it should be assessed individually rather than treated as an absolute cut-off.
Guidance Across Bodies
- Position
- Nerve injury is a recognised THA complication requiring documented informed consent; no level-1 evidence supports routine intra-operative neuromonitoring
- Evidence Level
- Consensus / low-level evidence
- Practical Implication
- Counsel explicitly in high-risk hips; monitoring is selective, not routine
- Position
- Joint replacement guidance and BOA standards (BOAST) emphasise consent, complication recognition and clear post-operative observation pathways
- Evidence Level
- Guideline / standard of care
- Practical Implication
- Documented post-op neurovascular check expected; escalate deficits promptly
- Position
- Teach nerve at risk by approach (posterior - sciatic; anterior/direct anterior - femoral and LFCN) and limb-length control
- Evidence Level
- Educational consensus
- Practical Implication
- Approach-specific protection and intra-operative length checks
- Position
- Informed consent, documented pre- and post-operative neurovascular examination, and incident reporting for nerve injury
- Evidence Level
- Safety/quality standard
- Practical Implication
- Root-cause analysis for permanent deficits
There is genuine international variation: some high-volume DDH centres use intra-operative SSEP/EMG neuromonitoring for Crowe III-IV cases, while most units rely on direct nerve visualisation and limb-length control alone. Evidence that routine neuromonitoring reduces palsy rates is weak (mixed results in older series), so its use remains selective and centre-dependent rather than standard of care.
Key documentation requirements for defensible practice:
-
Pre-operative documentation:
- Baseline neurovascular examination documented in medical record
- Pre-operative leg length measurement or apparent LLD noted
- Specific consent discussion documented if high-risk case (DDH, revision, protrusio)
-
Intraoperative documentation:
- Approach used and any anatomical difficulties encountered
- Leg length measurement technique and result (pin-to-pin, fluoroscopy)
- Final leg length differential documented before closure
- Any intraoperative concerns about nerve or vascular structures
-
Post-operative documentation:
- Neurovascular examination in recovery room before patient leaves theatre
- Motor power graded (0-5 MRC scale) for foot dorsiflexion, plantarflexion, toe movements
- Sensory examination of foot and leg dermatomes
- Vascular status (pulses, capillary refill, temperature)
- Documentation of normal findings is as important as abnormal
-
Management documentation:
- If deficit identified: rationale for revision vs observation clearly stated
- Timing of any intervention and reason for timing
- Patient counselling about injury, prognosis, and treatment plan
- Follow-up plan including EMG timing and specialist referrals
|Common litigation issues:
- Failure to document pre-operative neurological examination
- Excessive limb lengthening (over 4cm) without documented consent discussion
- Delayed recognition of nerve injury (no post-operative examination)
- Failure to revise when indicated (over 4cm lengthening with complete palsy)
- Inadequate informed consent discussion in high-risk cases
Legal precedents in high-income settings emphasise that nerve injury itself is a recognised complication and not necessarily negligent, but failure to recognise, document, or appropriately manage the injury can constitute negligence.
MCQ Practice Points
Q: The sciatic nerve at the level of the hip joint runs approximately how far posterior to the posterior acetabular rim? A: 2-3cm posterior. This distance is critical for safe posterior approach. The nerve exits the pelvis through the greater sciatic notch beneath the piriformis muscle and runs posterior to the acetabulum protected by the short external rotators. Excessive posterior wall reaming, retractor placement directly posterior, or cement extrusion can directly injure the nerve at this level.
Q: What is the single strongest modifiable risk factor for sciatic nerve palsy after THA? A: Limb lengthening over 4cm. Multiple studies demonstrate exponential increase in nerve injury risk beyond 4cm lengthening. This is modifiable through careful templating, intraoperative measurement, and femoral shortening osteotomy when indicated. Other risk factors like DDH diagnosis and revision surgery are not modifiable, but lengthening can be controlled by surgical technique.
Q: When is the optimal timing for baseline EMG/NCS after suspected nerve injury? A: 3 weeks post-injury. Wallerian degeneration takes 2-3 weeks to develop, so earlier EMG is unhelpful. At 3 weeks, EMG can distinguish neuropraxia (no denervation changes) from axonotmesis (fibrillation potentials, positive sharp waves). Repeat studies at 3 months and 6 months monitor recovery trajectory and guide prognosis.
Q: What is the indication for urgent revision surgery in immediate post-operative sciatic nerve palsy? A: Limb lengthening over 4cm with complete sciatic palsy. This combination indicates traction injury that is unlikely to recover without removing the cause of traction. Component revision to reduce leg length to under 4cm differential should be performed urgently (within 24-72 hours). Partial palsies with less than 4cm lengthening can be observed initially with close monitoring.
Q: What is the expected recovery rate for neuropraxia after THA? A: 70-90% full recovery. Neuropraxia is a temporary conduction block without structural nerve damage. Recovery typically occurs over days to weeks (maximum 3 months). If no recovery by 3 months, the injury was likely more severe than neuropraxia (axonotmesis or neurotmesis), and prognosis worsens significantly. Early signs of recovery within 6 weeks are a positive prognostic indicator.
Q: Which vessel is most commonly injured during THA and what is the typical mechanism? A: External iliac artery, injured by medial acetabular screw penetration or cement extrusion. The external iliac artery runs along the pelvic brim just medial to the acetabulum. In acetabular protrusio repair or revision with medial wall defects, screws or cement can penetrate the thin medial wall and directly injure the vessel. This may present immediately with bleeding or in delayed fashion as pseudoaneurysm. Pre-operative CT to measure medial wall thickness and intraoperative fluoroscopy during screw insertion reduce this risk.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You have just completed a primary THA via posterior approach for severe secondary osteoarthritis in a 55-year-old man. The anaesthetist calls you to recovery as the patient is unable to dorsiflex his right foot. What is your assessment and management?”
“You are planning a THA for a 42-year-old woman with Crowe IV developmental dysplasia of the hip. The hip is dislocated 8cm superiorly. Walk me through your approach to minimising nerve injury risk.”
“A 68-year-old man underwent revision THA for aseptic loosening 6 weeks ago. He presents to the emergency department with a painful, pulsatile mass in his groin. Examination reveals a 4cm pulsatile swelling with a bruit. Distal pulses are present. What is your diagnosis and management?”
Key Anatomy
- Sciatic nerve: 2-3cm posterior to acetabular rim, exits below piriformis in 85%
- Peroneal division: lateral and more vulnerable, less connective tissue support
- Femoral nerve: lies lateral to femoral artery beneath inguinal ligament
- External iliac artery: runs along pelvic brim, at risk with medial screws/cement
Injury Classification
- Neuropraxia: conduction block, recovers weeks-months (70-90% full recovery)
- Axonotmesis: axon disruption, 1mm/day regeneration (40-60% partial recovery)
- Neurotmesis: complete transection, poor prognosis (under 10% recovery)
- Distinguish with EMG at 3 weeks (Wallerian degeneration takes 2-3 weeks)
Risk Factors and Prevention
- Lengthening over 4cm: strongest modifiable risk factor (limit with shortening osteotomy)
- DDH: 3-10x higher risk, plan subtrochanteric shortening if Crowe III-IV
- Revision THA: 5-10x higher risk than primary, careful dissection essential
- Posterior approach: visualise nerve, blunt retractors medially, release every 20 min
Recognition and Diagnosis
- Post-anaesthesia exam MANDATORY: test foot dorsiflexion, plantarflexion, toe movements
- Sciatic (peroneal): foot drop, dorsum foot numbness (80% of nerve injuries)
- Femoral nerve: weak quadriceps, anterior thigh numbness (anterior approach)
- EMG/NCS at 3 weeks baseline, repeat at 3 and 6 months to monitor recovery
Management Algorithm
- Lengthening over 4cm + complete palsy = urgent revision within 24-72h
- Lengthening under 4cm + partial palsy = observe with AFO, close monitoring
- Vascular injury (absent pulses, cold limb) = immediate vascular surgery consult
- No recovery by 6 months = consider secondary procedures (tendon transfer at 12-18 months)
Key Evidence and Prognosis
- Schmalzried 1997: overall palsy ~1%, 80% sciatic/peroneal, ~41% full recovery
- Farrell/Morrey 2005 (Mayo): 0.17% motor palsy; DDH, lengthening and posterior approach are risk factors; only 36% of complete palsies fully recover
- De Fine 2017 review: sciatic palsy is over 90% of nerve injuries; no single safe lengthening threshold; ~two-thirds recover
- Recovery timeline: neuropraxia weeks-3 months, axonotmesis 24-36 months maximum
Evidence Base and Key Studies
Motor Nerve Palsy Following Primary Total Hip Arthroplasty (Mayo Clinic series)
- 47 motor nerve palsies among 27,004 primary THAs (0.17%) at a single institution 1970-2000
- Peroneal/sciatic predominated (30 peroneal, 14 sciatic, 3 femoral across complete and incomplete palsies)
- Independent risk factors: DDH, post-traumatic arthritis, posterior approach, limb lengthening, and cementless femoral fixation
- Only 36% (10/28) of complete palsies recovered full motor strength, taking a mean of 21.1 months
- 21 patients required walking aids and 15 required permanent ankle-foot orthosis
Surgical Approach and Nerve Palsy in Total Hip Arthroplasty
- Prospective study of 1,000 consecutive THAs, overall neuropathy prevalence 0.8%
- Posterior approach 0.6% versus lateral transtrochanteric 1.0%; difference not statistically significant
- Revision surgery prevalence 1.4%, higher than primary regardless of approach
- Authors conclude anatomical variation and reconstructive complexity, not approach per se, drive nerve injury
Update on Nerve Palsy Associated With Total Hip Replacement
- Overall prevalence of nerve palsy after THR approximately 1%
- Sciatic nerve or its peroneal division involved in nearly 80% of cases
- Risk increased in female patients, developmental dysplasia and revision surgery
- Recovery: approximately 41% complete or near-complete, 44% mild residual deficit, 15% poor outcome
- Some motor function immediately post-op or recovery within ~2 weeks predicts good prognosis
Sciatic Nerve Palsy Following THR: Are Patient Characteristics More Important Than Limb Lengthening? (Systematic Review)
- Systematic review of 14 studies of post-arthroplasty sciatic nerve palsy
- Sciatic palsy accounts for over 90% of neurological injuries after THR
- No single safe limb-lengthening threshold could be reliably identified across studies
- DDH and previous hip surgery are the most consistently reported risk factors
- Full nerve recovery occurs in roughly two-thirds of cases irrespective of initial damage severity
Exploration and Neurolysis for Neuropathic Pain in Sciatic Nerve Palsy After Total Hip Replacement
- 56 patients explored for sciatic nerve palsy after THR at a specialist peripheral nerve unit
- 46 palsies followed primary THR, 5 revision THR, 5 hip resurfacing
- Mean pre-operative pain score 7.6 fell to 3.8 after neurolysis (mean improvement 3.8, p less than 0.001)
- Authors recommend exploration and neurolysis over conservative care for established neuropathic pain
National Joint Replacement Registries (AOANJRR / NJR) - Registry Context
- Large arthroplasty registries (AOANJRR, NJR) capture procedure volumes, implant survivorship and revision cause but do not systematically code peripheral nerve or vascular injury as a primary outcome
- Registry data confirm revision and dysplasia/deformity diagnoses carry higher complication and re-revision burden, consistent with the higher nerve-injury risk reported in clinical series
- Approach-specific nerve-injury rates are best taken from clinical cohorts rather than registries, which capture revision-for-instability and dislocation more reliably than transient neuropraxia