Post-Arthroplasty Femoral Fracture | Vancouver Classification | Revision Arthroplasty
- Stem stability assessment is THE critical decision driver
- B1 = Stable Stem → ORIF (Preserve stem)
- B2/B3 = Loose Stem → Revision Arthroplasty
- Obtain full-length femur radiographs (MANDATORY)
- Always screen for infection (ESR/CRP) preoperatively
- “Most common error: Attempting ORIF on a loose stem (guaranteed failure)
- “Intraoperative fracture: STOP, assess, and stabilize immediately
- “Risk factors: Elderly female, osteoporosis, uncemented stems
- “Don't forget the acetabulum (associated loosening or fractures)
Periprosthetic Fractures Around Total Hip Arthroplasty
The Single Most Important Assessment. Differentiating B1 (stable) from B2 (loose) dictates treatment. Getting this wrong is an automatic fail.
Mandatory Pre-op Check. Always rule out septic loosening presenting as fracture. Missed infection leads to catastrophic failure of fixation.
Full-Length Femur Views. Essential to see distal extent of fracture and plan bypass fixation length (2 cortical diameters).
Prevention is Key. Recognize high-risk patients (osteoporotic females, revision cases) and use prophylactic cables or gentle technique.
- Classification
- Vancouver A
- Stem Status
- Stable
- Treatment
- Conservative (unless displaced/unstable)
- Classification
- Vancouver B1
- Stem Status
- Stable
- Treatment
- ORIF (Plate + Cables)
- Classification
- Vancouver B2
- Stem Status
- Loose
- Treatment
- Revision THA (Long Uncemented Stem)
- Classification
- Vancouver B3
- Stem Status
- Loose
- Treatment
- Revision (Impaction Graft or Megaprosthesis)
- Classification
- Vancouver C
- Stem Status
- Stable
- Treatment
- ORIF (Distal Femur Plate)
Overview and Epidemiology
Periprosthetic femoral fracture is now among the top 3-4 reasons for THA revision across major joint registries (NJR, AJRR, AOANJRR, Swedish/Nordic). Incidence is rising globally with ageing populations, the dominance of uncemented stems, and the growing cumulative pool of primary THAs.
- Revision surgery (4-7% risk)
- Uncemented stem insertion (press-fit)
- Undersized canal preparation
- Excessive impaction force
- Rheumatoid arthritis
- Severe osteoporosis
- Anterior femoral cortical defects
- Aseptic loosening with osteolysis
- Stress shielding (cortical thinning)
- Retained cement mantle
- Age over 70 years
- Female sex (2.5x higher risk)
- Frequent falls
Epidemiology of Periprosthetic Fracture (Primary THA)
- Intraoperative fracture in 1.7% overall; 14x more common with uncemented stems (3.0% vs 0.23% cemented)
- 20-year cumulative postoperative fracture probability 3.5% (7.7% uncemented vs 2.1% cemented)
- Within 30 days, postop fracture risk after an uncemented stem was 10x higher than cemented
- Intraoperative fractures most common in women and patients over 65; most occurred during femoral component placement (60%) and involved the calcar (69%)
- Vancouver AG was the most common postoperative type (32%); 67% followed a fall
Anatomy and Biomechanics
Pathophysiology: Rigid metallic stems transfer load distally, bypassing the proximal femur. This leads to adaptive bone resorption (Wolff's Law), causing cortical thinning and osteopenia in the proximal femur, significantly increasing fracture risk from minor trauma.
- Osteolysis: Wear debris induces cytokine-mediated bone loss
- Cortical Thinning: less than 4mm cortex increases fracture risk exponentially
- Bone Density: Osteopenia common in THA population
- Anterior Cortex: At femoral bow apex (common perforation site)
- Proximal Lateral Cortex: Aggressive broaching risk
- Calcar: Varus stem malposition
Classification Systems
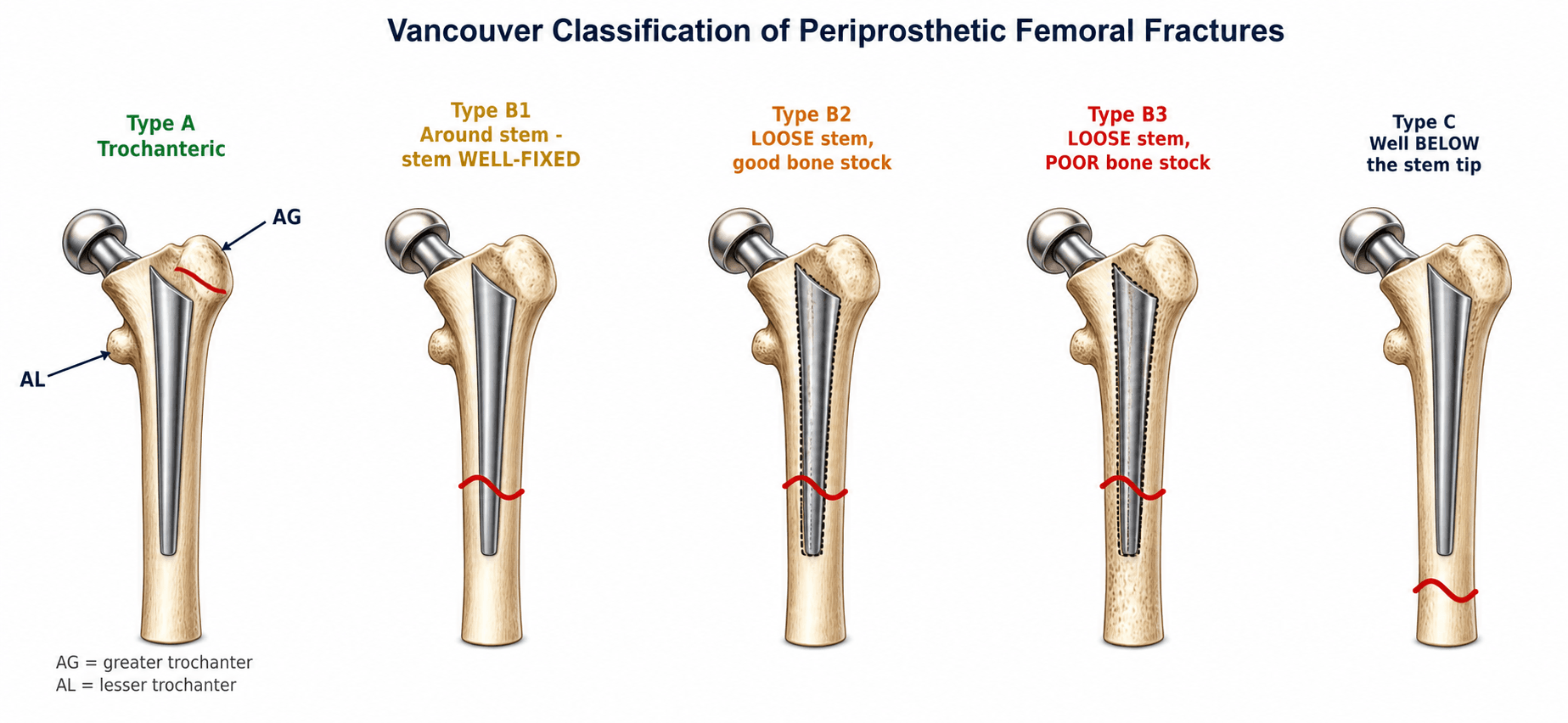
Vancouver Classification
Duncan & Masri (1995) - The universal Gold Standard based on: Location, Stability, and Bone Stock.
- Location
- Greater Trochanter
- Stem Status
- Stable
- Bone Stock
- Variable
- Management
- Conservative vs ORIF
- Location
- Lesser Trochanter
- Stem Status
- Stable
- Bone Stock
- Variable
- Management
- Conservative
- Location
- Around Stem
- Stem Status
- **STABLE**
- Bone Stock
- Good
- Management
- **ORIF** (preserve stem)
- Location
- Around Stem
- Stem Status
- **LOOSE**
- Bone Stock
- Good
- Management
- **Revision** (Long Stem)
- Location
- Around Stem
- Stem Status
- **LOOSE**
- Bone Stock
- Poor
- Management
- **Revision** (Impaction/Megaprosthesis)
- Location
- Below Stem
- Stem Status
- Stable
- Bone Stock
- Variable
- Management
- **ORIF** (Plate/Nail)
Vancouver Classification Reliability
- Interobserver agreement substantial: kappa 0.69 (consultants), 0.61 (trainees)
- Intraobserver kappa 0.74-0.90 (substantial to almost perfect)
- Validity in 37 type B cases: 81% agreement on B1/B2/B3 subgroup, kappa 0.68
- Authors emphasise intraoperative assessment of implant stability when radiographs are equivocal
Clinical Assessment
NO PASSRed Flags (NO PASS)
Hook:If you see these, do NO PASS go - call senior immediately.
- Mechanism: Low energy fall vs trauma
- Pain: Prodromal thigh/groin pain (suggests loosening)
- Pre-injury Function: Independent vs bedbound
- Comorbidities: Osteoporosis, RA, steroids
- Inspection: Shortening, rotation, swelling
- Palpation: Tenderness, crepitus
- Neurovascular: Sciatic/Femoral nerve check MANDATORY
- Systemic: Signs of infection/sepsis
Immediate Orthopaedic Review Required:
- Open Fracture: Rare but critical
- Neurovascular Compromise: Sciatic nerve palsy
- Compartment Syndrome: High index of suspicion
- Septic Loosening: Red, hot, swollen joint with fracture
Investigations
Imaging Protocol
Full-Length Femur (AP/Lat): Mandatory to plan fixation length. AP Pelvis: Assess cup and contralateral side. Hip Views: Detailed fracture pattern.
Indicated for B3 fractures (bone stock), acetabular involvement, or uncertain comminution. Use Metal Artifact Reduction Sequence.
ESR & CRP: Mandatory in ALL cases to rule out septic loosening. Aspiration if elevated.
Reading the Stem for Loosening: Gruen Zones and Radiographic Criteria
Distinguishing a stable B1 from a loose B2 is this topic's single most important decision, and the IMPLANT mnemonic lists the signs — but they are read against a standard map, the Gruen zones, using defined loosening criteria.
- Gruen zones. The femoral component is divided into seven zones on the AP film (1-7, starting at the lateral shoulder/greater trochanter, running down the lateral cortex to the stem tip and back up the medial cortex), with matching zones on the lateral view. They give a reproducible language for where a lucency, osteolysis or debonding sits.
- Cemented-stem loosening (Harris criteria). Definite = stem migration/subsidence or a fractured cement mantle; probable = a continuous radiolucent line at the cement-bone interface around the entire stem; possible = a lucent line over 50 to 100% of the interface. A progressive or circumferential lucency is the key signal.
- Uncemented-stem loosening. Suggested by subsidence or migration on serial films, a continuous reactive line around a porous surface, and a distal pedestal with no proximal bone ongrowth; conversely, spot-welds (endosteal bone bridging to the porous coating) and absence of migration indicate a stable, osseointegrated stem.
- The practical rule. Compare against serial and immediate-postoperative films whenever possible; if the radiographs stay equivocal, test the stem directly at operation before committing — a loose stem fixed as a B1 fails.
Q: How do you decide radiographically whether a periprosthetic-fracture stem is loose (B2) rather than stable (B1)? A: Read the seven Gruen zones on serial films. For a cemented stem, loosening is definite (subsidence/mantle fracture), probable (continuous cement-bone lucency around the whole stem) or possible (lucency over 50-100%). For an uncemented stem, look for subsidence/migration, a continuous reactive line and a distal pedestal (loose) versus spot-welds and no migration (ingrown). If still uncertain, test the stem intraoperatively.
IMPLANTAssessing Stem Stability (B1 vs B2/B3)
Hook:Check the IMPLANT before you plan your fixation strategy.
Differential Diagnosis
The painful THA with a possible fracture must be distinguished from other causes of acute or progressive hip/thigh pain. The two errors that fail candidates are missing infection (septic loosening masquerading as fracture) and missing occult loosening in an apparently intact femur.
- Key Features
- Trauma/fall, deformity, inability to weight-bear
- Discriminator
- Visible fracture line on full-length femur films
- Action
- Classify (Vancouver) + assess stem stability
- Key Features
- Prodromal start-up thigh pain, gradual onset
- Discriminator
- Radiolucent lines, subsidence, pedestal; no cortical break
- Action
- Workup for revision; exclude infection
- Key Features
- Rest pain, warmth, effusion, raised CRP/ESR
- Discriminator
- Aspiration (cell count, culture, alpha-defensin)
- Action
- Treat as infected loosening; never ORIF over sepsis
- Key Features
- Groin pain, cup migration
- Discriminator
- AP pelvis: cup migration, broken Kohler's line
- Action
- CT pelvis; cup-cage / triflange planning
- Key Features
- Activity-related groin/thigh pain, osteoporosis/bisphosphonate
- Discriminator
- Subtle cortical reaction; MRI/bone scan if films normal
- Action
- Protect, treat bone health, monitor
- Key Features
- Lateral tenderness, pain on resisted abduction
- Discriminator
- Localised soft-tissue signs, normal bone
- Action
- Conservative; injection / abductor imaging
Management Algorithm
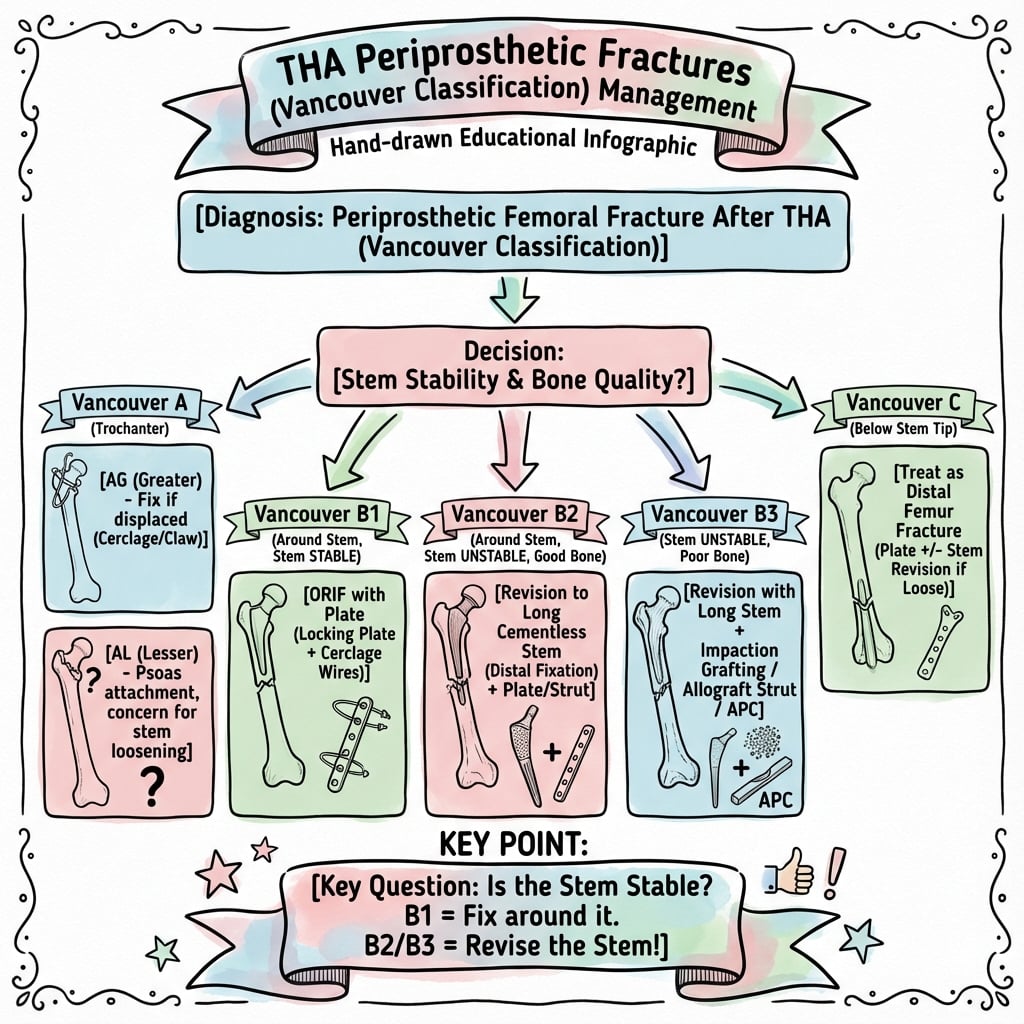
- 1Assessment
Stable vs Loose Stem?
Classification A, B1, B2, B3, C
- 2Vancouver A
Trochanteric
Conservative (usually) OR Tension Band/Plate
- 3Vancouver B1
Stable Stem
ORIF (Locking Plate + Cables)
- 4Vancouver B2
Loose Stem, Good Bone
Revision THA (Long Uncemented Stem)
- 5Vancouver B3
Loose Stem, Poor Bone
Impaction Grafting OR Megaprosthesis
- 6Vancouver C
Below Stem
ORIF (Bridge Plating)
Indications: Undisplaced Type A, stable Type C in non-ambulatory patients, medically unfit for surgery. Protocol: Protected weight bearing 6-12 weeks, serial x-rays. Failure: Progressive displacement greater than 5mm or intractable pain requires surgery.
Intraoperative Periprosthetic Fracture: Recognition and Management
The exam pearls warn to "STOP, assess and stabilise immediately" for an intraoperative fracture, and the epidemiology shows it complicates roughly 1.7% of primary and 12% of revision stems — so the on-table response deserves spelling out.
- When and where. Most occur during stem insertion/impaction (press-fit), typically at the calcar in primaries and the diaphysis in revisions; uncemented stems carry roughly a 3-fold (revision) to 14-fold (primary) higher risk than cemented. Highest risk in osteoporotic older women, with undersized broaching, or a sclerotic revision canal.
- Recognise it. A change in the pitch of impaction, a visible or palpable crack, unexpected stem subsidence, or an intraoperative fluoroscopic lucency. If suspected, stop and image the whole femur before proceeding.
- Manage by pattern (the same location logic as the Vancouver scheme):
- Calcar crack (proximal, undisplaced): a single cerclage cable/wire around the proximal femur before seating the stem — the rationale for a prophylactic cable in an at-risk femur.
- Diaphyseal split at the stem tip: cerclage, plus — if stability is doubtful — bypass with a longer diaphyseal-fitting stem by at least two cortical diameters.
- Fracture distal to the intended stem: may need a longer stem, a plate, or both, before or after final component placement.
- Prevention and aftercare. Canal-appropriate gentle broaching, prophylactic cables in fragile bone, and protected weight-bearing afterwards. Undisplaced diaphyseal fractures recognised and cabled on the table generally heal well.
Q: You feel the femur crack while impacting an uncemented stem — what do you do? A: Stop and image the whole femur. A proximal calcar crack is managed with a cerclage cable before final seating; a diaphyseal split needs cerclage and, if unstable, a longer stem bypassing it by two cortical diameters. Then protect weight-bearing. Recognising and stabilising it on the table prevents a displaced postoperative fracture.
Surgical Technique
Vancouver B1: Fixation (Stem Preserving)
Prerequisite: You MUST be certain the stem is STABLE. If in doubt, treat as loose (revision).
Steps
Incision centered on trochanter, split fascia lata. Elevate vastus lateralis anteriorly. Preserve perforators.
Gentle traction and bone clamps. Verify stem alignment fluoroscopically.
Proximal: Cables/screws around stem (unicortical or cable-plate). Distal: Bicortical locking screws (min 4-6). Bypass: Plate must extend 2 cortical diameters (10-15cm) distal to fracture.
Consider concomitant strut allografts for medial comminution or osteopenia.
FIXATIONB1 Fixation Principles
Hook:Good FIXATION saves the stem.
Complications
- Infection: 3-8% (higher than primary)
- Dislocation: 20-40% in revisions (use dual mobility/constrained liners)
- DVT/PE: 1-2% symptomatic VTE
- Nerve Injury: Sciatic (cable passage)
- Nonunion: 5-20% (poor biology/stability)
- Loosening: Subsequent aseptic loosening
- Refracture: At plate tip (stress riser)
- Hardware Failure: Plate breakage
Outcomes & the 'Loose Stem' Signal (National Registry)
- A loose stem was present at the time of fracture in 66% (after primary THA) and 51% (after revision)
- 88% of fractures were Vancouver type B, but radiographic preoperative subgrouping was difficult
- High failure rate: 66-month survival (reoperation as endpoint) only 74.8% (plus or minus 5.0%)
- Implant design was associated with fracture risk
Postoperative Care
Rehabilitation Protocol
Toe-touch or restricted (20kg) weight bearing. Hip precautions (prevent dislocation). DVT prophylaxis (35 days).
Progress weight bearing as callus appears. Abductor strengthening. Transition to cane.
Full weight bearing once united. Return to baseline function. Osteoporosis management (Bisphosphonates).
Fragility-fracture bone-health workup (consistent across international osteoporosis guidance):
- Correct vitamin D deficiency (target greater than 50 nmol/L)
- Ensure adequate calcium intake (diet plus supplement to ~1000 mg/day)
- Start anti-resorptive therapy (bisphosphonate or denosumab) once fracture healing is established, with DXA and falls-risk assessment.
Outcomes and Prognosis
- Union Rate
- 90-95%
- Revision Rate (5y)
- 5-10%
- Functional Return
- 60-70% baseline
- Union Rate
- 85-90%
- Revision Rate (5y)
- 15-25%
- Functional Return
- 40-60% baseline
- Union Rate
- N/A
- Revision Rate (5y)
- 20-30%
- Functional Return
- 30-50% baseline
- Union Rate
- greater than 90%
- Revision Rate (5y)
- 5%
- Functional Return
- 70-80% baseline
Guidelines, Registries & Global Practice
Global epidemiology. Periprosthetic femoral fracture complicates roughly 1% of primary and up to ~5% of revision THAs over the implant lifetime, and is consistently among the top reasons for revision in every major registry. Risk is concentrated in elderly women, osteoporotic/inflammatory-arthritis bone, and uncemented femoral fixation. As the global volume of primary arthroplasty rises, absolute fracture numbers are increasing worldwide.
- Region
- US
- Emphasis
- Stem-stability-driven algorithm; revision for loose stems (B2/B3); ORIF for stable (B1) and Vancouver C
- Region
- UK
- Emphasis
- Combined ortho-geriatric pathway, early surgery, senior decision-maker, network referral for complex revision
- Region
- Global
- Emphasis
- Locked plating with bypass of 2 cortical diameters, cable/locking-attachment plates, biological reduction
- Region
- Multi-region
- Emphasis
- Higher fracture rates with uncemented stems, especially older women; cemented fixation protective in the elderly
- Region
- Global
- Emphasis
- Fracture-liaison-style assessment; vitamin D, calcium, anti-resorptive once healing established
Across NJR, AJRR, AOANJRR and the Nordic registries, uncemented stems in older patients (especially women over 70-75) carry a higher periprosthetic fracture rate than cemented stems. This is the single most reproducible registry message and underpins selective cemented fixation in the frail elderly.
High-resource: modular fluted tapered revision stems, locking-attachment cable plates, CT with metal-artifact reduction, dual-mobility/constrained liners, orthogeriatric co-management. Limited-resource: conventional cerclage plus long-stem or interlocking constructs, allograft struts where banks exist, cemented revision; emphasis on definitive single-stage fixation given limited revision implant availability.
Controversies & Areas of Uncertainty
The dogma is revision for any loose stem. Selected series suggest ORIF of a B2 around a well-fixed-design cemented or polished-tapered stem may succeed in low-demand or high-risk patients, but the dominant registry signal (loose stem to high failure) keeps revision as the default. Reserve fixation for the unfit.
For B2/B3, modular fluted tapered uncemented stems dominate modern practice with reliable distal fixation. Impaction grafting with a cemented stem restores bone stock (younger patients) but demands restricted weight-bearing. No high-level RCT settles the choice.
Distal locked plating is standard, but plate-tip stress risers cause refracture. Some advocate overlapping the stem ('plate-stem overlap') or nail-plate combinations to avoid an unprotected segment between implants.
Whether to revise a fractured cemented stem versus fix-around remains debated, as disturbing the cement mantle is destabilising. Most polished-tapered cemented stems that subside within an intact mantle still behave as 'loose' once the bone fractures.
State the default evidence-based answer first (loose stem to revision; bypass by 2 cortical diameters), then acknowledge the nuance (B2 fixation in the unfit; impaction grafting in the young). Examiners reward candidates who know both the rule and its exceptions.
MCQ Practice Points
Q: What is the most significant predictor of failure after ORIF of periprosthetic fractures? A: Loose stem (Misdiagnosis of B2 as B1). Fixation of a loose stem leads to cantilever failure of the plate or nonunion.
Q: What is the minimum recommended distal fixation length beyond the fracture? A: 2 cortical diameters (typically 10-15cm). Short plates create stress risers and lead to refracture.
Q: What is the approximate 1-year mortality after periprosthetic hip fracture? A: 10-15%. This reflects the frailty and comorbidities of the population, similar to native hip fractures.
Q: When do you use cables versus screws in periprosthetic fracture fixation? A: Cables proximally (where the stem occupies the canal), screws distally (where biocortical purchase is possible). This "cable-plate" construct provides optimal fixation.
Q: What is the indication for cortical strut grafts? A: Significant bone loss or cortical defects (B2/B3). Strut grafts provide biological healing scaffold and mechanical support. Can be allograft or autograft.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“78F falls at home. Primary THA 8 years ago. X-ray shows fracture around stem.”
“You decide a patient has a B1 fracture (stable stem). Describe your fixation.”
“82F with B3 fracture (loose stem, severe bone loss). Medically frail.”
Classification (Vancouver)
- Type A: Trochanteric (Stable)
- Type B1: Around stem, Stable to ORIF
- Type B2: Around stem, Loose to Revision (Long Stem)
- Type B3: Around stem, Loose, Poor bone to Salvage
- Type C: Below stem to ORIF
Key Assessment
- Stem Stability is the #1 Factor
- Full length femur X-ray Mandatory
- Pre-op Infection Screen Mandatory
- IMPLANT mnemonic for loosening signs
Surgical Principles
- Bypass fracture by 2 cortical diameters
- Cables proximally, Screws distally
- Strut grafts for poor bone
- Revision stems must achieve distal fixation
Complications
- Infection (3-8%)
- Dislocation (High risk in revisions)
- Nonunion/Refracture
- 1-year mortality 10-15%
Evidence Base
Demographics & Implant Factors (Swedish Register)
- 1049 fractures (1979-2000); a majority of late fractures occurred around a loose stem
- Implant-related factors were significantly associated with fracture occurrence
- Treatment results were poor with low long-term survivorship and high complication rates
- Established the periprosthetic fracture burden as a rising, costly complication
Epidemiology in Revision THA
- Intraoperative fracture incidence 12% in revision THA (3x higher than primary)
- Intraoperative fractures 3x more common with uncemented stems (19% vs 6% cemented)
- 20-year probability of postoperative fracture 11%; risk similar for cemented and uncemented
- Most common postoperative type was Vancouver B1 (31%)
Mortality After Periprosthetic Femoral Fracture
- Postoperative fracture after primary THA: modestly increased death risk (HR 1.19), confined to patients with comorbid orthopaedic conditions
- Intraoperative fracture in primary THA: no excess mortality (HR 1.03)
- In revision THA, neither intra- nor post-operative fracture carried excess mortality
- 1112 intraoperative and 704 postoperative fractures analysed across 30,782 THAs
Patient-Specific Risk Calculator
- 16,696 primary THAs; 5-year patient-specific risk ranged 0.5-25% by comorbid profile
- Non-modifiable: female (HR 1.6), older age, osteoporosis (HR 1.7), non-OA indication (fracture HR 2.2)
- Modifiable: uncemented fixation (HR 2.5), collarless stem (HR 1.3), non-anterior approach (lateral HR 2.9)
- Demonstrates surgeon decisions (fixation, implant, approach) materially shift risk