Posterior vs Anterior vs Lateral | Nerve Injury Risk | Dislocation Rates | AOANJRR Registry Data
- Posterior approach is the most common approach worldwide (60% in the AOANJRR) - sciatic nerve at risk, higher dislocation without repair
- Direct anterior has lowest dislocation rate (0.6%) - LFCN at risk, steep learning curve, fracture risk
- Anterolateral/lateral approaches risk superior gluteal nerve - abductor dysfunction/Trendelenburg
- Soft tissue repair is critical - posterior capsule repair reduces dislocation from 5% to under 2%
- No single best approach - surgeon experience and patient factors guide selection
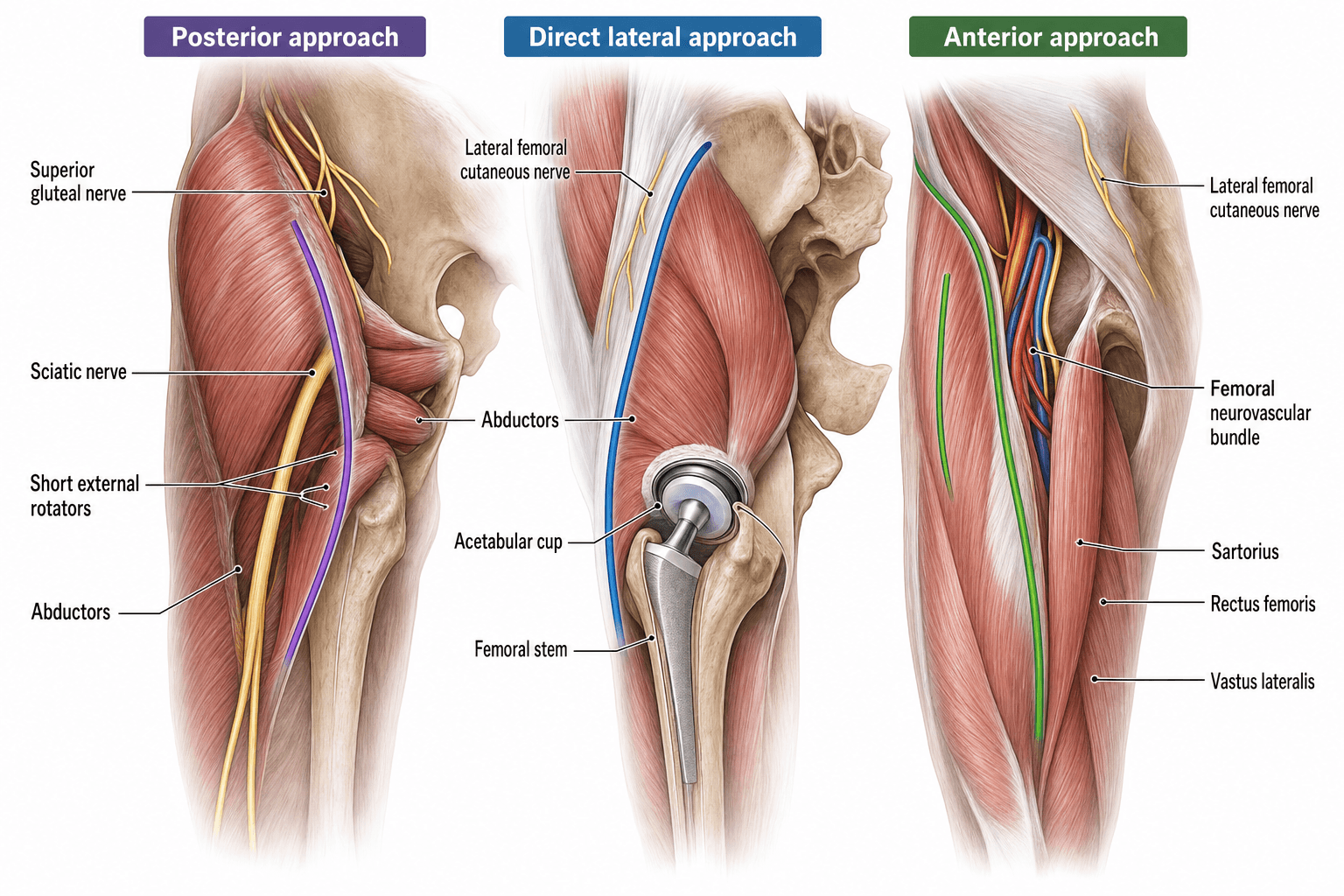
- “Posterior: sciatic nerve, short external rotators, higher dislocation risk without repair
- “Anterior: LFCN paresthesia common, femoral nerve/vessels at risk medially, lower dislocation
- “Lateral: superior gluteal nerve, abductor split/detachment, Trendelenburg gait risk
- “AOANJRR shows posterior most common (60%) followed by lateral (25%) and anterior (15%)
Posterior capsule and short external rotator repair reduces dislocation from 5% to under 2%. The trend toward soft tissue repair has transformed posterior approach outcomes. Know the repair technique.
Each approach has specific nerve risks: Posterior = sciatic (peroneal division), Anterior = LFCN and femoral, Lateral = superior gluteal. Know the anatomy and protection strategies for each.
Approach determines dislocation direction: Posterior approach → posterior dislocation with flexion/adduction/IR. Anterior approach → anterior dislocation with extension/ER. Critical for patient education.
National registries (AOANJRR/NJR/AJRR): the posterior approach predominates; revision rates are similar across approaches when the surgeon is experienced. Level I RCT meta-analyses (Ang 2023; Yan 2023) confirm no clear superiority - experience matters most.
- Interval/Plane
- Through piriformis/short ER
- Nerve Risk
- Sciatic (peroneal)
- Dislocation Rate
- 2-3% (with repair)
- Key Advantage
- Excellent acetabular exposure
- Interval/Plane
- TFL-Sartorius (Smith-Petersen)
- Nerve Risk
- LFCN, femoral
- Dislocation Rate
- 0.6-1%
- Key Advantage
- Lowest dislocation rate
- Interval/Plane
- Split gluteus medius
- Nerve Risk
- Superior gluteal
- Dislocation Rate
- 1-2%
- Key Advantage
- Good exposure both sides
- Interval/Plane
- Through/detach abductors
- Nerve Risk
- Superior gluteal
- Dislocation Rate
- 1-2%
- Key Advantage
- Versatile, extensile
POSTERIORPOSTERIOR - Key Features
Hook:POSTERIOR reminds you of the anatomy, nerve risk, and critical repair
ANTERIORANTERIOR - Direct Anterior Approach (DAA)
Hook:ANTERIOR highlights the internervous plane and supine positioning
LATERALLATERAL - Hardinge/Transglueteal
Hook:LATERAL emphasizes abductor protection and Trendelenburg risk
Overview and Epidemiology
Surgical approach selection is one of the most debated topics in total hip arthroplasty. Despite decades of research, no single approach has emerged as clearly superior across all outcomes. The choice depends on surgeon experience, patient factors, and specific clinical scenarios.
The four main approaches:
-
Posterior approach (Moore, Southern, Kocher-Langenbeck modified)
- Most commonly used worldwide (60% in the AOANJRR)
- Through or around piriformis and short external rotators
- Historically higher dislocation rate, now comparable with soft tissue repair
-
Direct anterior approach (Smith-Petersen, Hueter)
- Growing popularity, especially in North America
- True internervous/intermuscular plane (femoral vs superior gluteal)
- Lowest dislocation rates but learning curve and fracture risk
-
Anterolateral approach (Watson-Jones, modified Hardinge)
- Split through gluteus medius and minimus
- Good exposure of both acetabulum and femur
- Risk to superior gluteal nerve
-
Direct lateral approach (Hardinge, transglueteal)
- Detachment or split of abductors from greater trochanter
- Versatile and extensile
- Requires meticulous abductor repair
The AOANJRR data shows similar revision rates across all approaches when performed by experienced surgeons. The "best" approach is the one the surgeon knows best. Patient education about specific dislocation precautions for each approach is critical.
Historical context:
The evolution of THA approaches reflects changing priorities:
- 1950s-1960s: Lateral approaches dominant (Charnley)
- 1970s-1980s: Posterior approach gains popularity (easier acetabular exposure)
- 1990s-2000s: Concern over posterior dislocation drives minimally invasive/anterior interest
- 2010s-present: Posterior capsule repair equalizes dislocation rates; approach choice based on surgeon preference
Approach distribution (AOANJRR 2023):
- Posterior approach: 60% of primary THAs
- Lateral/transglueteal: 25%
- Anterior approaches: 15%
- Revision surgery: posterior approach preferred (70%) for better exposure
Anatomy and Internervous Planes
Posterior Approach Anatomy
- Patient lateral decubitus
- Incision centered over greater trochanter, curving posteriorly
- Landmarks: PSIS, greater trochanter, femoral shaft
- Skin and subcutaneous tissue
- Fascia lata - incise in line with fibers
- Gluteus maximus - split in line with fibers (proximal) or elevate inferior border
- Short external rotators - piriformis, superior gemellus, obturator internus, inferior gemellus
- Posterior capsule - releases with short ERs
- Joint
-
Sciatic nerve: Emerges inferior to piriformis, runs posterior to obturator internus/gemelli
- Peroneal division more lateral and superficial - most vulnerable
- Protect with anterior retractor during femoral preparation
- At risk with: retraction, cement extrusion, leg lengthening over 4cm
-
Superior gluteal nerve and vessels: Enter gluteus medius 5cm proximal to GT
- Safe if stay distal to piriformis
- Risk with proximal dissection
-
Inferior gluteal vessels: Posterior to femur
- Risk with overzealous posterior retraction
The posterior approach is not truly internervous. It splits the gluteus maximus (inferior gluteal nerve) and releases the short external rotators (nerve to quadratus femoris and individual nerve branches). The advantage is excellent exposure, not preservation of innervation.
Direct Anterior Approach Anatomy
- Patient supine on standard or fracture table
- Incision 2-3cm lateral and distal to ASIS
- Extends distally toward lateral patella
- Lateral: Tensor fascia lata (superior gluteal nerve)
- Medial: Sartorius and rectus femoris (femoral nerve)
- Skin and subcutaneous tissue
- Fascia lata - incise between TFL and sartorius
- Internervous plane - develop bluntly
- Reflected head of rectus femoris - release from capsule
- Anterior capsule - T-shaped or cruciate release
- Joint
-
Lateral femoral cutaneous nerve (LFCN)
- Runs just lateral to incision or through operative field
- Injury rate 5-20%, usually temporary paresthesia
- Cannot always be avoided but identify if visible
-
Femoral nerve and vessels
- Medial to surgical field (under sartorius/rectus)
- Protected by staying lateral
- Risk with medial retractor placement
-
Ascending branch LFCA
- Crosses surgical field on anterior capsule
- Ligate or cauterize - can bleed significantly
Keep retractors over bone on medial side. The femoral neurovascular bundle lies under the sartorius and iliopsoas, just medial to the surgical field. Excessive medial retraction or retractors placed under soft tissue can cause nerve palsy.
Lateral Approach Anatomy (Hardinge/Transglueteal)
- Lateral decubitus or supine
- Incision centered over greater trochanter
- Extends proximally and distally
- Skin and subcutaneous tissue
- Fascia lata and IT band - incise longitudinally
- Gluteus medius and minimus - split anterior third or detach from GT
- Capsule - T-shaped release
- Joint
- Enters gluteus medius 5cm proximal to tip of GT
- Runs between medius and minimus
- Injured by:
- Splitting medius more than 5cm proximal to GT
- Splitting posterior to anterior third of muscle
- Excessive retraction
Two rules to protect superior gluteal nerve:
- Limit proximal dissection to 5cm above GT tip
- Split only the anterior one-third of gluteus medius
Violation leads to abductor denervation and Trendelenburg gait.
Abductor repair: The detached anterior third of medius/minimus must be repaired back to greater trochanter with non-absorbable sutures through bone. Failure of repair or healing leads to abductor deficiency.
Anterolateral Approach (Watson-Jones)
Similar to lateral approach but:
- More anterior incision (ASIS toward GT)
- Works anterior to gluteus medius (elevates off femur anteriorly)
- Less abductor damage but still risks superior gluteal nerve
- Capsule release more challenging
Internervous Planes and Surgical Intervals
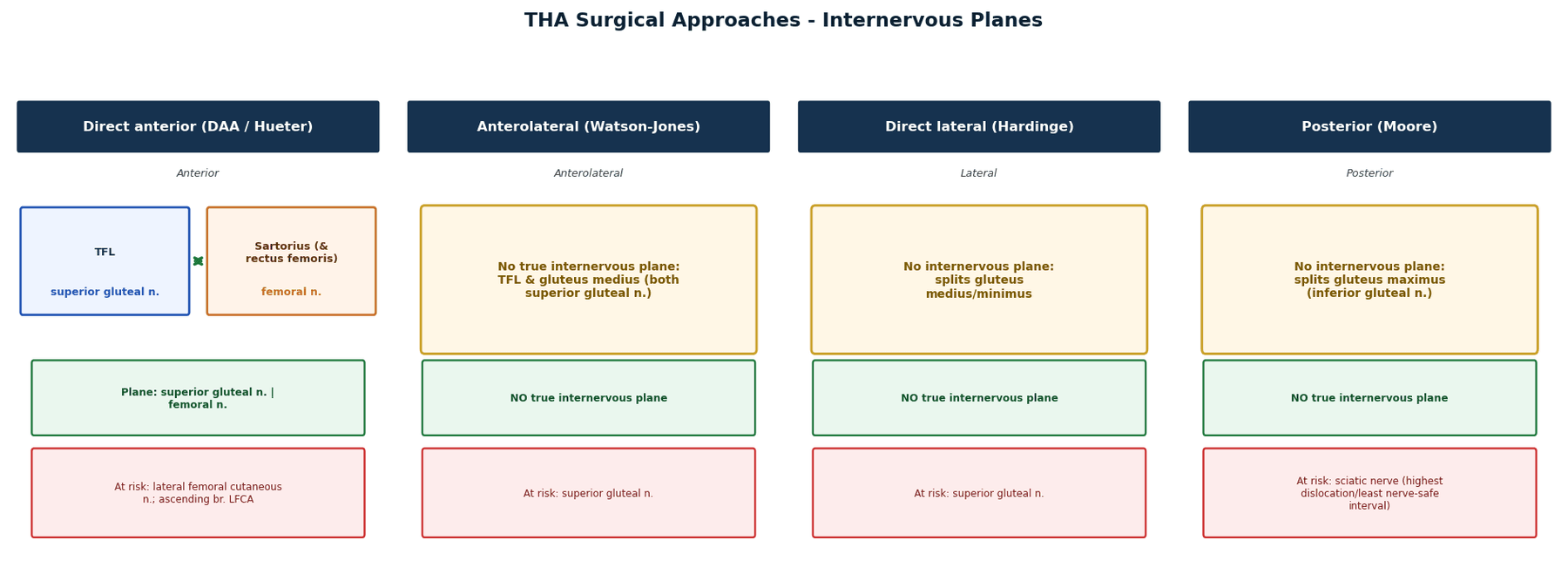
Posterior Approach: NOT truly internervous - splits gluteus maximus (inferior gluteal nerve) and releases short external rotators. The advantage is excellent exposure, not nerve preservation.
Direct Anterior (Smith-Petersen/Hueter): TRUE internervous interval between TFL (superior gluteal) and sartorius/rectus femoris (femoral nerve). No muscle cutting required.
Lateral (Hardinge): NOT internervous - splits or detaches gluteus medius/minimus. Superior gluteal nerve at risk if split extends greater than 5cm proximal to GT.
Anterolateral (Watson-Jones): Develops interval between TFL and gluteus medius. Both supplied by superior gluteal nerve but can be safely separated.
Classification Systems
Posterior Approaches
Kocher-Langenbeck modified, Moore, Southern approaches - enter hip posterior to femur through short external rotators.
Anterior Approaches
Smith-Petersen/Hueter direct anterior - true intermuscular approach between sartorius/TFL and rectus femoris.
Lateral Approaches
Hardinge transgluteal and direct lateral - split or detach abductors from trochanter.
Anterolateral Approaches
Watson-Jones approach - between gluteus medius and TFL, anterior capsule access.
Clinical Assessment for Approach Selection
Preoperative Patient Evaluation
-
Body habitus
- BMI over 35: consider posterior (anterior difficult with large pannus)
- Body fat distribution affects exposure
-
Prior surgery
- Previous hip surgery scar location
- Prior approach may influence current choice
- Scar tissue considerations
-
Comorbidities
- Parkinson's disease: consider anterior (lower dislocation risk)
- Spinal fusion: assess spinopelvic mobility
- Neuromuscular disease: dislocation risk assessment
-
Activity level and goals
- High-demand patients: approach with lowest complication risk
- Return to sport considerations
-
Hip pathology
- DDH: posterior preferred (better acetabular exposure)
- Protrusio: posterior or lateral
- Revision cases: extensile approach needed
- Hip range of motion limitations
- Leg length discrepancy
- Spinopelvic mobility assessment
- Prior incision locations
The clinical assessment guides appropriate approach selection based on individual patient factors.
Differential Diagnosis - The Symptomatic Post-Approach Hip
Approach selection is also relevant when a THA patient presents with new symptoms, because each approach predisposes to a recognisable differential. Distinguishing approach-related soft-tissue/nerve problems from intra-articular and extrinsic causes is high-yield.
- Typical presentation
- Sudden pain, shortening, fixed rotation, inability to weight-bear
- Approach association
- Posterior (flexion/adduction/IR); anterior (extension/ER)
- Distinguishing feature
- Radiograph shows head out of socket; direction follows the approach
- Typical presentation
- Lurching gait, lateral hip weakness, positive Trendelenburg sign
- Approach association
- Direct lateral (Hardinge) and anterolateral
- Distinguishing feature
- Weak abduction, intact joint on imaging; superior gluteal nerve or repair failure
- Typical presentation
- Anterolateral thigh numbness/burning, no motor loss
- Approach association
- Direct anterior
- Distinguishing feature
- Pure sensory deficit in LFCN territory; normal strength
- Typical presentation
- Foot drop, lateral leg/foot sensory loss
- Approach association
- Posterior (also lengthening, revision)
- Distinguishing feature
- Motor deficit below knee; check leg-length change and cement
- Typical presentation
- Rest/night pain, warmth, effusion, raised CRP/ESR
- Approach association
- All approaches (similar rates)
- Distinguishing feature
- Aspirate WCC/culture; serology and imaging
- Typical presentation
- Start-up pain, progressive activity-related pain
- Approach association
- All approaches (technique-dependent)
- Distinguishing feature
- Radiolucent lines, migration, component subsidence
- Typical presentation
- Acute pain after load/fall, deformity
- Approach association
- Higher intraoperatively with direct anterior
- Distinguishing feature
- Fracture on radiograph (Vancouver classification)
- Typical presentation
- Groin pain on hip flexion / stairs
- Approach association
- Any (oversized or prominent anterior cup)
- Distinguishing feature
- Pain on resisted flexion; cup overhang on CT; relieved by injection
- Typical presentation
- Pain not reproduced by hip movement
- Approach association
- Independent of approach
- Distinguishing feature
- Normal hip exam/imaging; address lumbar spine or vascular source
Investigations for Approach Planning
Preoperative Imaging
- AP pelvis X-ray: Assess hip anatomy, template implants, measure leg lengths
- Lateral hip X-ray: Assess version, anterior/posterior offset
- Full-length standing X-rays: If leg length discrepancy or spinopelvic concerns
- CT scan with 3D reconstruction: DDH, revision cases, complex acetabular anatomy
- Spinopelvic films (standing and sitting lateral): If stiff spine or flat back syndrome concerns
- MRI: Not routine for approach planning, used for soft tissue pathology assessment
- Essential for all approaches
- Determines component sizes
- Assesses offset and leg length restoration needs
- Digital templating increasingly used
- Anterior approach may use fluoroscopy intraoperatively
- Complex cases benefit from detailed preoperative imaging review
Appropriate imaging helps surgical planning and approach selection based on individual anatomy.
Management - Approach Selection Algorithm
- First-time THA
- Normal anatomy (no dysplasia)
- BMI under 35
- No prior hip surgery
- No major comorbidities
- Primary consideration: Surgeon experience and volume with specific approach
- Secondary consideration: Patient preference after education
- Options (all acceptable):
- Posterior if surgeon experienced (most commonly used approach)
- Anterior if surgeon experienced and trained (growing usage)
- Lateral if surgeon preference
- Surgeon expertise trumps approach selection
- All approaches have similar outcomes when surgeon experienced
- Patient education about specific precautions for chosen approach
For standard anatomy, surgeon mastery of one approach is more important than approach type.
Detailed Approach Comparison
Posterior Approach - Moore/Southern
- Primary THA (most common worldwide)
- Revision THA (best exposure)
- DDH, protrusio (acetabular visualization superior)
- Complex acetabular reconstruction
- Lateral decubitus with supports
- Pelvis perpendicular to floor
- Affected leg free to move
- Incision centered over GT, curve posteriorly
- Split gluteus maximus in line with fibers
- Identify and protect sciatic nerve
- Release/tag short external rotators (piriformis, gemelli, obturator internus)
- Release posterior capsule
- Dislocate posteriorly with flexion/adduction/internal rotation
- Perform arthroplasty
- Repair short ERs and capsule back to greater trochanter or femur
- Excellent acetabular exposure - best of all approaches
- Familiar to most surgeons
- Easy to extend for revisions
- Good femoral exposure
- Can do in any OR (no special table needed)
- Sciatic nerve at risk (0.5-1% palsy rate)
- Higher dislocation historically (now equivalent with repair)
- Requires meticulous soft tissue repair
- Trendelenburg gait if gluteus maximus damaged
- Anterior retractor placement protects sciatic during femoral prep
- Avoid excessive leg lengthening (over 4cm increases risk)
- Gentle retraction
- Prevent posterior cement extrusion
- Posterior soft tissue repair is mandatory
- Repair short ERs to greater trochanter or posterior femur
- Repair posterior capsule
- Consider dual mobility in high-risk patients
- Patient education: avoid flexion over 90 degrees, adduction, internal rotation for 6 weeks
Understanding the repair technique transforms the posterior approach from high dislocation risk to comparable safety with other approaches.
Positioning and Patient Setup
Lateral decubitus position
- Affected hip up
- Pelvis stabilized with anterior and posterior supports
- Lower leg flexed, upper leg supported
- Ensure no tilt - can cause malposition
Key points:
- Bean bag or posts for stabilization
- Protect peroneal nerve on down leg
- Fluoroscopy challenging but possible
Lateral decubitus offers excellent acetabular and femoral access with stable positioning.
Patient Positioning and Surgical Technique
Posterior Approach Pearls
Capsule and ER tagging: Tag piriformis and conjoined tendon before release using heavy non-absorbable suture (No. 2 FiberWire). Label with clamps to identify for repair.
Sciatic nerve protection: Always place anterior (ilioischial) retractor during femoral preparation - this single maneuver prevents most nerve injuries. Release retractor periodically.
Acetabular exposure: Remove osteophytes from femoral neck before dislocation. Femoral head removal improves visualization. Use superior and inferior retractors.
Femoral preparation: Anterior retractor protects sciatic. External rotation and flexion expose proximal femur. Can use femoral elevator to deliver proximal femur.
Repair technique: Drill holes in GT or use suture anchors. Repair piriformis and conjoined tendon first, then side-to-side capsule repair. Check stability before final closure.
Gluteus maximus closure: Approximate split with absorbable suture to protect repair and improve cosmesis.
Surgical Technique - Step by Step
Steps:
- Skin incision centered over GT
- Incise fascia lata and split/elevate gluteus maximus
- Tag and release piriformis and short ERs
- Capsulotomy - T or H shaped
- Dislocate hip (flex, adduct, IR)
- Prepare acetabulum and femur
- Reduce trial, check stability
- Insert final components
- Repair capsule and short ERs to GT
- Layered closure

Complications
- Posterior
- 2-3% (with repair)
- Anterior
- 0.6-1%
- Lateral
- 1-2%
- Prevention
- Soft tissue repair, component position, head size
- Posterior
- 0.5-1% (sciatic)
- Anterior
- 5-20% (LFCN), under 1% (femoral)
- Lateral
- 1-2% (sup gluteal)
- Prevention
- Gentle retraction, anatomic knowledge
- Posterior
- 1-2%
- Anterior
- 2-3%
- Lateral
- 1-2%
- Prevention
- Careful technique, low threshold to extend
- Posterior
- Rare (if glut max damaged)
- Anterior
- None
- Lateral
- 5-10% (repair failure)
- Prevention
- Meticulous abductor repair, patient compliance
- Posterior
- 1-2%
- Anterior
- 1-2%
- Lateral
- 1-2%
- Prevention
- Antibiotic prophylaxis, surgical technique
- Posterior
- 3-5%
- Anterior
- Lower (some data)
- Lateral
- 3-5%
- Prevention
- NSAIDs or radiation if high risk
Approach-Specific Complications Detail
-
Sciatic nerve palsy (0.5-1%)
- Most serious complication
- Peroneal division typically affected
- Prevention: anterior retractor, limit lengthening, gentle retraction
- Partial recovery in 60-70%
-
Dislocation (2-3% with repair, 5% without)
- Historically biggest concern
- Transformed by soft tissue repair
- Risk factors: prior surgery, neuromuscular disease, obesity
- Prevention: meticulous repair, component position, large head
-
Gluteus maximus damage
- Rare but causes Trendelenburg if severe
- Avoid excessive splitting
- Usually minor functional issue
-
LFCN injury (5-20%)
- Most common complication
- Usually temporary paresthesia
- Most improve over 6-12 months
- Rarely significant functional problem
- Warn patients preoperatively
-
Intraoperative fracture (2-3%)
- Greater trochanter, femoral shaft
- Higher during learning curve
- Related to forceful broaching, poor exposure
- Prevention: adequate hyperextension, gentle technique, low threshold to extend incision
- Recognize intraoperatively and fix (cables, cerclage, plate)
-
Femoral nerve injury (under 1%)
- Rare but devastating
- Related to medial retractor malposition
- Prevention: ensure retractors on bone, avoid soft tissue compression
- If occurs, explore and decompress
-
Wound complications
- Hematoma formation (lower position, gravity)
- May be higher in obese patients
- Good hemostasis critical
-
Superior gluteal nerve injury (1-2%)
- Causes abductor denervation
- Trendelenburg gait
- Prevention: 5cm rule, anterior third only
- Usually permanent
-
Abductor repair failure (5-10%)
- Presents as Trendelenburg, abductor weakness
- Prevention: non-absorbable suture, bone attachment, patient compliance with precautions
- May require revision to trochanteric advancement or abductor reconstruction
-
Heterotopic ossification
- May be higher than posterior (more muscle trauma)
- Consider prophylaxis in high-risk patients
-
Infection (1-2%)
- Similar rates across approaches
- Antibiotic prophylaxis, sterile technique
- Higher risk: obesity, diabetes, immunosuppression
-
DVT/PE
- Chemoprophylaxis per guidelines
- Early mobilization
- Approach does not significantly affect risk
-
Leg length discrepancy
- Related to technique, not approach
- Templating and intraoperative assessment
-
Component malposition
- Can occur with any approach
- Higher during learning curve
- Navigation may help but not proven superior
Postoperative Care and Rehabilitation
General Postoperative Protocol
- Pain management (multimodal analgesia)
- DVT prophylaxis (LMWH or oral anticoagulant per guidelines)
- Drain management if used (remove at 24 hours)
- Mobilization same day or day 1 with physiotherapy
- Weight-bearing as tolerated (all approaches)
- Progressive mobilization with walking aids
- Gait training specific to approach precautions
- Wound monitoring
- Hospital discharge typically day 2-4
- Posterior approach: Avoid flexion over 90 degrees, adduction, internal rotation
- Anterior approach: Minimal or no precautions (some surgeons), avoid extension/ER combinations if precautions given
- Lateral approach: Avoid active abduction against resistance (protect repair), otherwise unrestricted
- Progressive strengthening
- Weaning from walking aids
- Return to desk work typically 6 weeks
- Return to manual work 12 weeks
- Return to sports 3-6 months depending on activity
- No permanent activity restrictions
- Regular follow-up (6 weeks, 12 weeks, 6 months, then annually)
- Registry participation (AOANJRR)
The postoperative care protocol is similar across approaches with variations in specific precautions.
Outcomes and Prognosis - Registry and Trial Data
Approach Distribution (Registry Snapshot)
National registries consistently show the posterior approach as the most commonly used for primary THA, followed by the direct-lateral/anterolateral and the anterior approaches. For revision THA, the posterior approach predominates further because of its extensile exposure. Exact percentages vary by country and change annually, so quote the current AOANJRR / NJR / AJRR annual report rather than a fixed figure.
Revision Risk by Approach
Key finding: revision risk is broadly similar across approaches in experienced hands. Registry analyses repeatedly show that, once surgeon volume and prosthesis are accounted for, cumulative revision rates differ minimally between posterior, lateral, and anterior approaches. Dislocation is one of the leading reasons for early revision and is the diagnosis most sensitive to approach and to soft-tissue repair technique.
This is reinforced by the highest-quality trial-level synthesis. According to PubMed, a network meta-analysis of 63 RCTs found no significant difference in the incidence of six complication types between any of eight approaches (Yan et al., JAMA Netw Open 2023, DOI), and an RCT meta-analysis of 24 trials found no significant difference in dislocation, periprosthetic fracture, or neurapraxia between DAA and posterior or lateral approaches (Ang et al., Eur J Orthop Surg Traumatol 2023, DOI).
Approach-Specific Complication Pattern
Rather than differing in overall revision risk, approaches differ in the type of complication they predispose to:
- Dislocation: highest historically with the unrepaired posterior approach; reduced to under 1% with posterior soft-tissue repair (Kwon 2006, DOI; Weeden 2003, DOI).
- Lateral femoral cutaneous nerve symptoms: predominantly with the direct anterior approach.
- Superior gluteal nerve / abductor weakness: with the direct lateral approach.
- Sciatic nerve palsy: rare and chiefly associated with the posterior approach.
Surgeon Volume Effect
Surgeon and unit volume is the dominant modifiable outcome factor. Higher-volume surgeons have lower revision and complication rates regardless of approach. The practical message is to master one approach to high volume rather than spreading across several. The DAA learning curve (~50 cases) affects operative time and blood loss but, with a traction table and fluoroscopy, did not compromise 5-year implant survival (99.2%) in a prospective cohort (Nakamura 2024, DOI).
Learning Curve by Approach
- Approx. cases to proficiency
- ~20-30
- Main early-phase risks
- Dislocation if repair not mastered
- Approx. cases to proficiency
- ~20-30
- Main early-phase risks
- Abductor weakness, superior gluteal nerve
- Approx. cases to proficiency
- ~50
- Main early-phase risks
- Femoral fracture, LFCN injury, component malposition
Registries and Level I trial meta-analyses agree: no clear winner among approaches in experienced hands. Choose the approach you know best, do high volume, perform posterior soft-tissue repair when using the posterior approach, and focus on component position, soft-tissue balance, and bearing choice.
International Practice Variation
Adoption patterns vary by country and reflect training tradition more than evidence. The posterior approach predominates globally. Anterior-approach uptake is highest in parts of North America (influenced by marketing and rapid-recovery programmes) and lowest in the UK; the direct-lateral (Hardinge) approach retains a strong following in parts of Europe rooted in the Charnley/Hardinge tradition. Quote precise country-level percentages only from the relevant current registry report.
Nerve Injury Patterns and Prevention
- Primary Nerve Risk
- Sciatic (peroneal)
- Injury Rate
- 0.5-1%
- Mechanism
- Retraction, lengthening, cement
- Prevention
- Anterior retractor, limit lengthening under 4cm
- Primary Nerve Risk
- LFCN
- Injury Rate
- 5-20%
- Mechanism
- Stretching, division
- Prevention
- Identify and protect; accept some injury
- Primary Nerve Risk
- Femoral nerve
- Injury Rate
- Under 1%
- Mechanism
- Medial retraction
- Prevention
- Retractors over bone, not soft tissue
- Primary Nerve Risk
- Superior gluteal
- Injury Rate
- 1-2%
- Mechanism
- Proximal dissection, posterior split
- Prevention
- Limit to 5cm above GT, anterior third only
- Primary Nerve Risk
- Femoral cutaneous (lateral/post)
- Injury Rate
- Variable
- Mechanism
- Incision placement
- Prevention
- Cannot always avoid; warn patient
Sciatic Nerve Injury (Posterior Approach)
- Emerges from sciatic notch below piriformis
- Composed of tibial and peroneal divisions
- Peroneal division lateral, superficial, tethered → most vulnerable
- Average 1.2cm from posterior capsule
- Direct trauma - retractor placement, sharp dissection
- Traction - leg lengthening over 4cm, retractor pressure
- Compression - cement extrusion, hematoma
- Thermal - cement polymerization (rare with modern techniques)
- Place anterior (ilioischial) retractor to protect nerve during femoral preparation
- Limit leg lengthening to under 4cm (higher risk over 4cm)
- Gentle retraction, release periodically
- Prevent posterior cement extrusion
- Consider nerve monitoring in revision or complex cases (controversial)
- Peroneal division most commonly affected (foot drop, numbness)
- May be immediate or delayed (hematoma, swelling)
- Check postoperatively before leaving OR
- Immediate: Explore if complete palsy noted immediately (rule out impingement)
- Delayed: Observe, nerve studies at 3-4 weeks, AFO for foot drop
- Most improve over 6-12 months
- Incomplete recovery common (60-70% partial/complete recovery)
Lateral Femoral Cutaneous Nerve (Anterior Approach)
- Variable course, usually lateral to ASIS
- Provides sensation to anterolateral thigh
- May cross or run through surgical field
- 5-20% in most series
- Usually temporary (neuropraxia)
- Most recover over 6-12 months
- Rarely permanent functional issue
- Identify nerve if visible and protect
- Cannot always prevent (variant anatomy)
- Warn patient preoperatively about numbness risk
- Reassurance - usually improves
- Rarely requires treatment
- Symptoms diminish even if nerve divided
Superior Gluteal Nerve (Lateral Approaches)
- Exits pelvis through sciatic notch above piriformis
- Runs between gluteus medius and minimus
- Enters gluteus medius 5cm proximal to GT
- Supplies gluteus medius, minimus, TFL
- Proximal dissection beyond 5cm above GT
- Splitting gluteus medius posterior to anterior third
- Excessive retraction
- 5cm rule: Do not dissect more than 5cm proximal to GT tip
- Anterior third rule: Split only anterior one-third of medius
- Gentle retraction
- Trendelenburg gait (drops contralateral pelvis with single leg stance)
- Abductor weakness
- May be masked initially by pain/guarding
- If suspected, abductor strengthening
- Gait training
- Usually does not recover (motor nerve)
- May require revision to trochanteric advancement
SAFESAFE ZONES - Nerve Protection
Hook:SAFE ZONES helps remember nerve protection strategies for each approach
Dislocation Rates and Prevention
Dislocation by Approach (Modern Data)
- Lowest dislocation rate: 0.6-1%
- Direction: Anterior dislocation (extension/external rotation)
- Rare enough that some surgeons give no formal precautions
- AOANJRR confirms lower dislocation risk
- 2-3% dislocation rate
- Historical rate 5% without repair
- Posterior soft tissue repair reduces risk by 50-60%
- Direction: Posterior (flexion/adduction/internal rotation)
- 1-2% dislocation rate
- Direction: Variable (usually anterolateral)
- Less specific precautions needed
Posterior capsule and short external rotator repair has transformed posterior approach outcomes. Techniques include repair to greater trochanter, repair to posterior femur, or capsular/piriformis advancement. Reduces dislocation from 5% to 2-3%, making it comparable to other approaches.
Posterior Soft Tissue Repair Techniques
- Short external rotators (piriformis, gemelli, obturator internus)
- Posterior capsule
- Consider quadratus femoris if released
-
Tag and repair to GT/posterior femur
- Tag short ERs before release with heavy suture
- After implants, repair to GT via drill holes or suture anchors
- Strong, anatomic
-
Capsular repair
- Side-to-side capsule repair
- May use figure-of-8 technique
- Good for thin tissue
-
Piriformis advancement
- Advance piriformis distally for tension
- Can combine with capsule repair
- Multiple studies show 50-60% reduction in dislocation
- No increase in operative time (5-10 minutes)
- Minimal additional morbidity
- Should be standard practice
Patient Precautions by Approach
- Flexion over 90 degrees (especially combined with adduction/IR)
- Adduction across midline
- Internal rotation especially when flexed
- Low chairs, picking items off floor
- Walking with aids
- Hip extension exercises
- External rotation exercises
- Supine or standing activities
- Raised toilet seat
- Shower chair
- Reacher/grabber
- Sock aid
- Long shoe horn
- Driving: 6 weeks (right hip), 4 weeks (left hip, automatic)
- Sports: 3-6 months
- Unrestricted activities after 12 weeks in most patients
Traditional 90-degree flexion rule is being challenged with modern repair techniques, with some advocating earlier mobilization.
Risk Factors for Dislocation (All Approaches)
- Prior hip surgery (2-3x risk)
- Neuromuscular disease (cerebral palsy, Parkinson's)
- Cognitive impairment (non-compliance)
- Alcohol abuse
- Younger age (higher activity)
- Inadequate soft tissue repair
- Component malposition (especially combined anteversion issues)
- Small femoral head (22mm vs 32mm or larger)
- Soft tissue tension (offset restoration)
- Assess component position (CT if needed)
- Consider closed reduction and bracing
- Revision if malposition
- Dual mobility bearing
- Constrained liner (last resort)
Component Orientation: Lewinnek Safe Zone and Combined Anteversion
Stability after THA depends as much on component orientation as on the approach - which is why a malpositioned cup (as in the recurrent-dislocation scenario) drives instability regardless of how the hip was opened. Every approach is ultimately judged on whether it allows the components to be placed in a stable orientation.
- Lewinnek "safe zone" (the classic radiographic target): acetabular inclination 40 degrees plus or minus 10 (i.e., 30-50 degrees) and anteversion 15 degrees plus or minus 10 (i.e., 5-25 degrees). Cups outside this zone had a markedly higher dislocation rate in the original series.
- Combined (functional) anteversion = acetabular anteversion + femoral stem anteversion, targeted around 25-50 degrees (Widmer's rule of thumb: cup anteversion + 0.7 times stem anteversion is approximately 37 degrees). The cup and stem must be orientated relative to each other - deficient combined anteversion predisposes to anterior impingement and posterior dislocation, while excessive combined anteversion does the reverse. This is why isolated assessment of the cup on an AP film is inadequate and CT is used for recurrent instability.
- Approach relevance: each approach has characteristic malposition tendencies (lateral-decubitus posterior/lateral approaches can introduce cup-version error from uncontrolled pelvic tilt; supine direct anterior with fluoroscopy aids intra-operative control of inclination and version). Orientation targets are the common denominator for stability across all approaches.
- The key limitation: the Lewinnek zone is necessary but not sufficient - a substantial proportion of dislocations occur with components measured inside the safe zone, because a static radiographic target ignores the dynamic change in pelvic tilt (and therefore functional cup version) between standing and sitting. That hip-spine/spinopelvic dimension (the stiff or fused lumbar spine that fails to tilt) and the use of functional/patient-specific targets and dual-mobility bearings are developed in the dedicated hip-spine relationship and dual-mobility topics.
Key principle: aim for the Lewinnek safe zone (inclination 40 plus or minus 10, anteversion 15 plus or minus 10) and an appropriate combined anteversion (about 25-50 degrees), but remember the cup and stem are orientated as a pair, and that many dislocations occur with components technically "in the zone". The static target must be combined with functional/spinopelvic assessment in patients with a stiff or fused spine - the limitation that drives patient-specific targets and dual mobility.
Minimally Invasive and Modified Techniques
Minimally Invasive Surgery (MIS) Concepts
- Smaller incision (under 10cm)
- Muscle-sparing techniques
- Often requires specialized instruments/retractors
- MIS posterior: Single or two-incision
- MIS anterior: Direct anterior is inherently muscle-sparing
- MIS lateral: Mini-incision transglueteal
- Less tissue trauma
- Faster recovery
- Reduced blood loss
- Improved cosmesis
- Earlier return to function
- Learning curve steeper than standard approaches
- Component malposition risk if visualization limited
- Femoral fracture risk (especially anterior)
- May need to extend incision (should have low threshold)
- Limited benefit in obese patients (adipose, not muscle, creates depth)
- Early enthusiasm has been tempered
- Meta-analyses show minimal clinical benefit over well-performed standard approaches
- Complication rates higher during learning curve
- Long-term outcomes (component position, survival) similar
- Cosmetic benefit real but functional benefit questionable
The size of the incision matters less than the quality of the procedure. A small incision with malpositioned components is worse than a standard incision with perfect technique. MIS should not compromise surgical fundamentals.
Muscle-Sparing Modifications
- Preserve piriformis: Work below piriformis, release only inferior rotators
- Minimize gluteus maximus split: Use inferior border elevation instead
- Claims of less Trendelenburg, unproven benefit
- Standard DAA is already muscle-sparing (internervous)
- Focus on learning curve reduction, fracture prevention
- Superior capsulotomy without abductor detachment
- Requires specialized retractors
- May reduce abductor dysfunction
Two-Incision MIS (Historical)
- Anterior incision for acetabulum
- Posterior incision for femur
- Proposed in 2000s
- High complication rate
- Femoral component malposition
- No clear benefit
- Steep learning curve
Visualization and precision trump incision size.
Direct Superior Approach (SuperPATH, Others)
- Superior capsulotomy preserving anterior and posterior capsule
- In situ neck cut
- Femoral and acetabular work through superior window
- Preserve capsule (low dislocation)
- Muscle-sparing
- Limited visualization
- Component position concerns
- Requires specific instruments
- Long-term data limited
- Growing use in Asia and some US centers
- Remains controversial
- Requires specialized training
Patient Selection and Approach Choice
Matching Approach to Patient
- First-time THA
- Normal anatomy
- BMI under 35
- No prior surgery
- Surgeon preference is primary determinant
- Posterior: excellent choice, most versatile
- Anterior: good choice if surgeon experienced, patient desires lowest dislocation risk
- Lateral: excellent choice if surgeon experienced with this approach
- Surgeon experience and volume with specific approach
- Patient goals and concerns (dislocation risk, recovery speed)
- Anesthesia considerations (lateral vs supine positioning)
- Facility capabilities (special tables for anterior)
For standard anatomy, surgeon expertise trumps approach selection.
Extended Trochanteric Osteotomy (ETO) for Revision Exposure
When a well-fixed femoral stem or an intact cement mantle must be removed, or the femur exposed for difficult revision, the extended trochanteric osteotomy is the workhorse extensile manoeuvre - and it is compatible only with the posterior or (antero-)lateral approaches, not the direct anterior approach. This is one of the principal reasons the direct anterior approach is a poor choice for complex femoral revision.
- What it is: a longitudinal osteotomy of the lateral femur that elevates the greater trochanter in continuity with the abductors proximally and the vastus lateralis distally (a vascularised myo-osseous sleeve), hinged anteriorly on its soft-tissue attachments and reflected to expose the canal.
- Length: templated to the construct - typically about one-third of the femur (roughly 12-15 cm), ending distal to a cemented mantle or a well-fixed stem tip so the whole interface can be addressed.
- Indications: extraction of a well-fixed cementless or cemented stem, removal of a full cement mantle, correction of femoral deformity or malrotation, and access in periprosthetic infection or fracture revision.
- Key technical points: preserve perfusion through the anterior soft-tissue sleeve; round the distal corner of the osteotomy to reduce the stress-riser fracture risk; the revision stem must bypass the osteotomy distally with diaphyseal fixation (a long, often fluted/tapered stem); reduce and secure the fragment with cerclage cables (commonly 2-3).
- Healing and complications: union rates are high when cabled securely, but risks include trochanteric escape/non-union (abductor insufficiency and Trendelenburg gait), intra-operative fracture, and cable-related problems. Because the abductors remain attached to the elevated fragment, anatomic bony reduction is what protects abductor function.
Examiner question: "How do you remove a well-fixed femoral stem at revision, and why does the approach matter?"
Answer: "Through an extended trochanteric osteotomy - a lateral femoral osteotomy that lifts the trochanter with the abductor-vastus lateralis sleeve in continuity, hinged anteriorly, giving controlled circumferential access to the stem and cement. The new stem must bypass the osteotomy with diaphyseal fixation and the fragment is cabled back. Crucially the ETO is only feasible through a posterior or lateral approach - it cannot be performed via the direct anterior approach, which is a key limitation of DAA for complex femoral revision."
Guidelines, Registries & Global Practice
Global Epidemiology and Burden
THA is one of the most successful and most frequently performed elective operations worldwide, with demand driven by an ageing population and rising osteoarthritis prevalence. Surgical-approach choice is one of the few aspects of the operation with genuine practice variation between countries and surgeons; the highest-quality comparative evidence (network meta-analysis of 63 RCTs, 4,859 patients) finds no consistent superiority of any approach for the six commonest complication types. According to PubMed (Yan et al., JAMA Netw Open 2023, DOI), the direct lateral approach gives the smallest early functional gain, while the posterior approach has the shortest operative time.
What the High-Quality Evidence Shows (Side-by-Side)
- Position on approach choice
- No single approach mandated; informed-consent emphasis on approach-specific risks and recovery. Supports shared decision-making.
- Evidence basis
- Evidence-based clinical practice guidelines / appropriate-use criteria
- Position on approach choice
- Focus on prosthesis selection and unit/surgeon outcomes (NJR) rather than mandating an approach; minimally invasive techniques not recommended over standard.
- Evidence basis
- NICE TA / BOA Blue Book standards
- Position on approach choice
- Cumulative revision risk differs minimally by approach once surgeon volume and implant are accounted for; dislocation a leading early revision cause.
- Evidence basis
- National registry observational data
- Position on approach choice
- DAA: faster early recovery, shorter stay, longer operative time; NO significant dislocation/fracture/nerve advantage at RCT level.
- Evidence basis
- Ang 2023 (PMID 37010580); Yan 2023 (PMID 36719679)
- Position on approach choice
- Equivalent, not superior, for revision, instability, infection, fracture, function.
- Evidence basis
- Clesham 2022 (PMID 35346808)
Major bodies (AAOS, NICE/BOA, EFORT, AO) deliberately avoid endorsing a single approach because Level I evidence shows equivalence in hard outcomes. The consistent message across guidelines and registries is that surgeon experience and accurate component position matter more than the approach itself.
Registry Evidence and Practice Variation
National joint registries (AOANJRR, NJR, and AJRR) capture near-complete primary THA data and are the best source of real-world revision risk by approach. Across these registries:
- The posterior approach is the most commonly used worldwide, with direct-lateral/anterolateral and anterior approaches making up the remainder; the exact split varies by country (anterior adoption is highest in parts of North America and lowest in the UK).
- Cumulative revision rates differ minimally between approaches once surgeon volume and prosthesis are accounted for.
- Dislocation is a leading early-revision diagnosis; it is reduced in the posterior approach by routine posterior soft-tissue repair (Kwon 2006, DOI).
Approach-distribution and revision percentages change year to year. Quote the latest annual report of the relevant registry (AOANJRR, NJR, AJRR) rather than a fixed figure, and frame the headline message: the posterior approach predominates and revision risk is broadly similar across approaches in experienced hands.
Surgeon Volume and Training
The dominant modifiable factor in outcome is surgeon (and unit) volume, not approach. Higher-volume surgeons have lower revision and complication rates regardless of approach, and the steep DAA learning curve (~50 cases) affects perioperative metrics without compromising mid-term implant survival when a traction table and fluoroscopy are used (Nakamura 2024, DOI). The practical corollary for trainees and examiners alike: master one approach to high volume rather than dabbling across several.
For orthopaedic vivas, do not over-index on one country's numbers. Know the global picture: posterior approach predominates worldwide; Level I RCT meta-analyses (Ang 2023; Yan 2023) show no hard-outcome winner; registries (AOANJRR/NJR/AJRR) show similar revision risk by approach; posterior soft-tissue repair (Kwon 2006) and surgeon volume are the real levers. Be ready to discuss approach selection for specific scenarios (obesity, DDH, revision) and the approach-specific nerve risks.
MCQ Practice Points
Q: A patient undergoing THA via direct anterior approach develops numbness over the anterolateral thigh postoperatively. Which nerve is most likely injured?
A: Lateral femoral cutaneous nerve (LFCN). This is the most common nerve injury with the anterior approach (5-20% incidence). It provides sensation to the anterolateral thigh. Most cases are temporary neuropraxia that improves over 6-12 months. The femoral nerve (motor to quadriceps, sensory to medial thigh) is rarely injured and would cause different symptoms.
Q: A patient who had posterior approach THA presents with hip dislocation. What position/movement most likely caused this dislocation?
A: Flexion, adduction, and internal rotation (e.g., getting out of a low chair, bending to tie shoes). Posterior approach disrupts posterior soft tissues, making the hip vulnerable to posterior dislocation with this movement combination. In contrast, anterior approach is at risk for anterior dislocation with extension and external rotation.
Q: During lateral approach THA, the superior gluteal nerve is at risk if the dissection extends how far proximal to the greater trochanter?
A: Greater than 5cm proximal to the tip of the greater trochanter. The superior gluteal nerve enters gluteus medius approximately 5cm proximal to the GT. Dissection beyond this point or splitting the posterior two-thirds of the muscle risks nerve injury, leading to abductor denervation and Trendelenburg gait.
Q: What is the effect of posterior capsule and short external rotator repair in posterior approach THA?
A: Reduces dislocation rate by approximately 50-60%, from historical 5% to modern 2-3%. The repair of piriformis, conjoined tendon (superior and inferior gemelli, obturator internus), and posterior capsule restores posterior stability. This has transformed posterior approach outcomes and should be standard practice.
Q: According to the AOANJRR 2023, what is the most commonly used approach for primary THA?
A: Posterior approach at approximately 60%, followed by lateral approaches (25%) and anterior approaches (15%). Despite marketing of newer approaches, posterior remains most common due to surgeon familiarity, excellent exposure, and comparable outcomes when soft tissue repair is performed.
Q: Which THA approach uses a true internervous plane?
A: Direct anterior approach (Smith-Petersen interval) between tensor fascia lata (superior gluteal nerve) and sartorius/rectus femoris (femoral nerve). The posterior approach is NOT truly internervous - it splits gluteus maximus (inferior gluteal nerve) and releases short ERs (various nerve branches). The lateral approach splits gluteus medius (superior gluteal nerve).
Q: What is the most important intraoperative maneuver to protect the sciatic nerve during posterior approach THA?
A: Placement of an anterior (ilioischial) retractor during femoral preparation. This single retractor protects the sciatic nerve from posterior retractor pressure and from instruments during femoral broaching and implantation. Additionally, limiting leg lengthening to under 4cm and preventing posterior cement extrusion are important.
Q: How many cases are typically required to achieve proficiency with the direct anterior approach to THA?
A: 30-50 cases, which is longer than the learning curve for posterior approach (20-30 cases). Early complications during the learning curve include intraoperative femoral fracture (2-3%), LFCN injury, component malposition, and wound complications. Mentorship and starting with ideal anatomy is recommended.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“You are in a multi-disciplinary meeting and a colleague states that 'the direct anterior approach is clearly superior because of the lower dislocation rate and should be the standard approach for all primary THAs.' How do you respond? What does the evidence actually show?”
“You are performing a posterior approach THA. At the end of the case, you ask the patient to dorsiflex the foot before leaving the OR and they cannot. You have a sciatic nerve palsy. What is your immediate management and what are the potential causes?”
“You review a 68-year-old patient who has had two posterior dislocations following a posterior approach THA performed 6 months ago. Both dislocations occurred with flexion and internal rotation (getting out of low chair). X-rays show the cup appears quite vertical at approximately 55 degrees inclination, anteversion difficult to assess on AP. What is your systematic approach to this problem?”
FOUR MAIN APPROACHES
- Posterior (60% AOANJRR): through piriformis/short ERs, sciatic nerve risk, 2-3% dislocation with repair
- Direct Anterior (15%): Smith-Petersen interval, LFCN injury common, 0.6% dislocation, learning curve 30-50 cases
- Lateral (25%): split/detach abductors, superior gluteal nerve risk, 1-2% dislocation, Trendelenburg if repair fails
- Anterolateral: between TFL and glut medius, less common now, similar risks to lateral
NERVE INJURY PATTERNS
- Posterior → Sciatic (peroneal division): 0.5-1%, protect with anterior retractor, avoid lengthening over 4cm
- Anterior → LFCN: 5-20% (mostly temporary), femoral nerve under 1% (medial retractor risk)
- Lateral → Superior gluteal: 1-2%, avoid dissection greater than 5cm above GT, anterior third only
- All approaches → cutaneous nerves variable (incision placement)
DISLOCATION RATES
- Anterior: 0.6-1% (lowest) - direction is anterior (extension/ER)
- Posterior with repair: 2-3% (was 5% without repair) - direction is posterior (flexion/add/IR)
- Lateral: 1-2% - variable direction
- Posterior soft tissue repair reduces dislocation by 50-60% (game-changer)
POSTERIOR APPROACH KEYS
- Tag short ERs before release (piriformis, conjoined tendon)
- Anterior retractor protects sciatic nerve during femoral prep
- Best acetabular exposure of all approaches
- Repair posterior capsule and short ERs to GT (mandatory)
- Precautions: avoid flexion over 90deg, adduction, IR for 6 weeks
ANTERIOR APPROACH KEYS
- Smith-Petersen interval (TFL lateral, sartorius/rectus medial)
- Supine positioning on fracture table or with positioning devices
- Learning curve 30-50 cases (fracture risk, LFCN injury early)
- Hyperextend hip for femoral exposure (fracture prevention)
- Medial retractors MUST be on bone (femoral nerve protection)
LATERAL APPROACH KEYS
- Split anterior one-third of gluteus medius/minimus
- 5cm rule: do NOT dissect greater than 5cm above GT (superior gluteal nerve)
- Repair abductors to GT with heavy non-absorbable suture
- Abductor precautions: no active abduction x 6 weeks
- Trendelenburg gait if nerve injury or repair failure
APPROACH SELECTION
- Standard primary: surgeon preference and expertise (no clear winner)
- High dislocation risk: anterior or dual mobility
- Obesity (BMI over 35): posterior preferred (anterior difficult with pannus)
- DDH/complex acetabulum: posterior (best acetabular exposure)
- Revision THA: posterior 70% (extensile, can extend proximally/distally)
AOANJRR 2023 DATA
- Posterior 60%, Lateral 25%, Anterior 15% (AOANJRR)
- Revision rates similar across approaches (7.0-7.5% at 10 years) when surgeon experienced
- Surgeon volume effect: high volume (over 30 cases/year) has 6.8% revision vs 10.2% for low volume
- Approach choice less important than surgeon experience and volume
EXAM TRAPS
- Stating one approach is definitively best (wrong - depends on surgeon and patient)
- Not knowing posterior soft tissue repair reduces dislocation by 50-60%
- Forgetting superior gluteal nerve 5cm rule for lateral approach
- Not knowing LFCN injury rate with anterior approach (5-20%, mostly temporary)
- Forgetting AOANJRR data (posterior 60%, similar revision rates across approaches)
Evidence Base
- Landmark meta-analysis of the posterior approach with versus without posterior soft tissue repair. Dislocation rate was 0.49% with repair and 4.46% without repair, giving an 8.21-fold relative risk of dislocation without repair (95% CI 4.05-16.67). A separate review of 11 studies showed comparable dislocation rates for anterolateral (0.70%), direct lateral (0.43%), and repaired posterior (1.01%) approaches.
- Meta-analysis of 24 randomised controlled trials (2,010 patients) comparing the direct anterior approach (DAA) with posterior (PA) or lateral (LA) approaches. DAA had a longer operative time (mean +17.4 min) but shorter length of stay and better early Harris Hip Scores. Critically, there was NO significant difference in dislocation, neurapraxia, periprosthetic fracture, or VTE between approaches when restricted to RCT-level evidence.
- Network meta-analysis of 63 RCTs (4,859 patients) across 8 approaches (2-incision, DAA, direct lateral, MIS variants, posterior, SuperPath). DAA and most approaches gave similar hip-score improvement and were superior to the direct lateral approach, which had the smallest functional gain. The posterior approach had the shortest operative time. The incidence of six complication types did not differ significantly between any approaches (GRADE moderate-to-high certainty).
- The AOANJRR provides near-complete national registry capture of primary THA. The posterior approach remains the most commonly used approach for primary THA, with the lateral/anterolateral and anterior approaches making up the remainder. Cumulative revision rates differ minimally across approaches once surgeon and prosthesis factors are accounted for, and dislocation remains a leading early revision diagnosis. Figures should be quoted from the current annual report, which is updated each year.
- Prospective cohort of 402 DAA THAs (first 50 cases per surgeon defined the learning curve). The 5-year implant survival rate was 99.2% both during and after the learning curve. Operative time fell by ~20 min and intraoperative blood loss decreased after the first 50 cases. The 2-year complication rate was 8.9% during versus 5.9% after the learning curve (not statistically significant). Cup safe-zone success was 96.4% during versus 98.7% after.
- Meta-analysis of 20 studies (1,282 minimally invasive vs 1,351 conventional THAs), including a level I-only sensitivity analysis. There was NO difference between minimally invasive intermuscular and conventional approaches for all-cause revision, aseptic revision, instability, infection, periprosthetic fracture, or functional outcome at early or intermediate follow-up.
- Cadaveric dissection of 15 limbs defining the safe distance for the most inferior branch of the superior gluteal nerve in the direct lateral (Hardinge) approach. Mean distance from the trochanteric tip to the nerve branch was 44 mm, but in three hips it was less than 30 mm. The distance was highly variable and did NOT correlate with femoral length or body height, so short patients are not at higher risk and tall patients are not exempt.
- Retrospective series of 945 primary THAs via the posterior approach with transosseous repair of the posterior capsule and short external rotators to the greater trochanter. At a mean 6.4-year follow-up, only 8 hips (0.85%) dislocated. With correct component orientation plus enhanced soft-tissue repair, the posterior approach achieved an extremely low dislocation rate.
- The original description of the direct lateral (transgluteal) approach to the hip, which detaches the anterior portion of the gluteus medius and minimus in continuity with the vastus lateralis to expose the joint while preserving posterior stability. This eponymous approach remains one of the three most commonly used THA approaches worldwide.