Rare | T8-T12 Common | Cord at Risk | Anterior Approach Preferred
- Rare pathology - only 0.5-1% of all symptomatic disc herniations
- Lower thoracic predominance - 75% occur at T8-T12 where relatively more motion
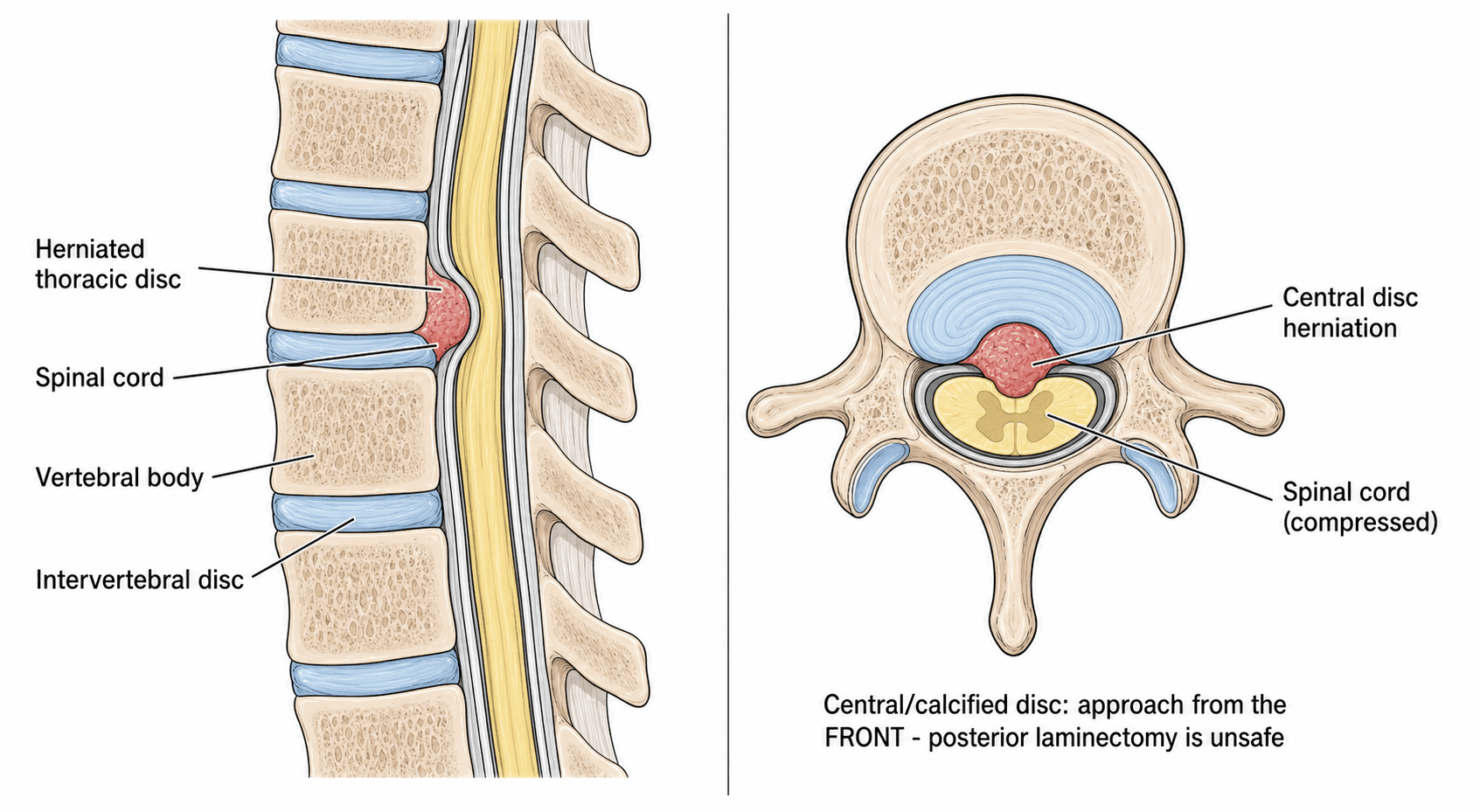
- Myelopathy is primary concern - narrow canal, cord cannot be retracted
- Posterior laminectomy CONTRAINDICATED for central discs - high paraplegia risk
- Anterior/anterolateral approaches - transthoracic, costotransversectomy, thoracoscopic
- Artery of Adamkiewicz at T9-L2 (usually left) - major blood supply to cord
- “40-70% of thoracic discs are calcified (complicates surgical removal)
- “Central disc from posterior = catastrophic cord injury
- “Many thoracic discs asymptomatic (incidental MRI findings)
- “Transthoracic approach provides best visualization but requires thoracotomy
Thoracic spinal cord CANNOT be safely retracted. The canal is narrow with limited CSF space. Attempting to access a central disc posteriorly requires cord manipulation - this causes irreversible paraplegia. This is the most important exam point.
The major radicular artery (arteria radicularis magna) supplying the lower two-thirds of the spinal cord. Located T9-L2 in 80%, predominantly left side (75-80%). Damage causes anterior spinal artery syndrome and paraplegia.
Central disc: Transthoracic, thoracoscopic, or costotransversectomy. Centrolateral: Anterior or posterolateral. Lateral: Transpedicular or lateral extracavitary. Location determines approach.
40-70% of thoracic discs are calcified (increases with age). Calcified discs are harder to remove surgically (like concrete). Requires high-speed burr. CT essential for surgical planning. Increases cord injury risk.
THORACICTHORACIC - Why Central Discs Need Anterior Approach
Hook:THORACIC reminds you why posterior approach to central disc = paraplegia
T8-T12T8-T12 - Most Common Levels
Hook:T8-T12 is the zone - lower thoracic has relatively more motion than upper
Overview and Epidemiology
Thoracic disc herniation is a rare spinal pathology accounting for only 0.5-1% of all symptomatic disc herniations. [1] The thoracic spine's inherent stability from rib cage articulation protects the discs from the degenerative changes commonly seen in cervical and lumbar regions. However, when thoracic disc herniations do occur, they pose unique diagnostic and therapeutic challenges due to the narrow spinal canal and proximity to the spinal cord.
- First surgical treatment described by Mixter and Barr in 1934
- Early posterior decompressive laminectomy gave poor results - only 57% success versus over 80% for posterolateral, lateral, and transthoracic approaches [2]
- Modern era defined by anterior and anterolateral approaches pioneered in 1960s-1980s
- Current outcomes significantly improved with proper approach selection
- Incidence: Estimated 1 per 1,000,000 population annually [1]
- Age: Peak presentation in 4th-6th decades (40-60 years)
- Gender: Slight male predominance (male:female ratio approximately 1.5:1)
- Level distribution: 75% occur at T8-T12 (lower thoracic), 25% at T1-T7 (upper/mid thoracic)
Why Lower Thoracic?
The lower thoracic spine experiences relatively more motion than the upper thoracic due to:
- Transitional anatomy approaching thoracolumbar junction
- Reduced rib cage constraint
- Mechanical stress concentration at kyphosis-lordosis transition
- Greater axial loading compared to upper thoracic
In the landmark MRI study of asymptomatic individuals by Wood and colleagues, 73% had at least one positive anatomical finding, including disc herniation in 37%, disc bulge in 53%, and cord deformation in 29%. [3] Not all thoracic disc herniations are symptomatic or require treatment; these are radiological abnormalities and clinical correlation is essential.
Associated Conditions:
- Scheuermann's disease - may predispose to thoracic disc degeneration
- Ankylosing spondylitis - increased fracture risk but also disc disease
- Degenerative scoliosis - asymmetric loading patterns
- Trauma - acute disc herniation rare but possible with high-energy mechanism
Anatomy and Biomechanics
Thoracic Spinal Canal Anatomy:
The thoracic spinal canal is the narrowest region of the vertebral column:
- Spinal cord fills 40-50% of canal (cervical: 25%, lumbar: cauda equina)
- Limited CSF space dorsally - cord is close to posterior elements
- Canal diameter: 12-14mm at T5-T8 (narrowest point)
- Cord diameter: 8-10mm in thoracic region
In the cervical spine, the cord occupies only 25% of the canal with ample CSF allowing safe posterior retraction. In the thoracic spine, the cord occupies 40-50% of the canal with minimal CSF dorsally. Attempting to retract the cord posteriorly causes direct mechanical injury and vascular compromise leading to irreversible paraplegia. This is the fundamental reason posterior laminectomy is contraindicated for central thoracic discs.
Vascular Anatomy - Artery of Adamkiewicz:
The arteria radicularis magna (artery of Adamkiewicz) is the largest anterior segmental medullary artery supplying the lower two-thirds of the spinal cord via the anterior spinal artery. [4]
- Details
- T9-L2 in 80% of population (range T5-L4)
- Details
- Left side in 75-80% of cases
- Details
- T9-T11
- Details
- Lower thoracic and lumbosacral cord segments
- Details
- Injury causes anterior spinal artery syndrome (paraplegia, loss of pain/temperature, preserved proprioception)
Examiner: "What is the artery of Adamkiewicz and why is it important in thoracic surgery?"
Answer: "The artery of Adamkiewicz is the major anterior radicular artery supplying the lower two-thirds of the spinal cord. It's located at T9-L2 in 80% of individuals, more commonly on the left side. During thoracic surgery, especially at these levels, we must be careful with segmental vessel ligation as damaging this artery causes anterior spinal artery syndrome with paraplegia and loss of pain and temperature sensation below the lesion. Some surgeons obtain preoperative CT angiography to identify it, though this is not routine."
Thoracic Disc Anatomy:
Thoracic intervertebral discs are:
- Thinner than lumbar discs (height 5-7mm vs 10-12mm lumbar)
- Less mobile due to rib cage constraints
- More prone to calcification with age (40-70% of symptomatic herniations are calcified) [5]
- Smaller nucleus pulposus relative to annulus compared to lumbar
Biomechanical Considerations:
The thoracic spine is stabilized by:
- Rib cage articulations (costovertebral and costotransverse joints)
- Longer spinous processes (shingled arrangement)
- Coronal plane facet orientation (limits rotation, allows lateral flexion)
- Thoracic kyphosis (anterior column loading)
Relatively less motion in upper/mid thoracic (2-4 degrees per level) increases at thoracolumbar junction (6-8 degrees at T11-T12).
Pathophysiology
Mechanisms of Disc Herniation:
Unlike lumbar discs where extrusion through posterior annulus is common, thoracic disc pathology has distinct features:
- Central herniation - nucleus migrates posteriorly compressing cord centrally
- Posterolateral herniation - most common pattern (60-70%), may cause myelopathy or radiculopathy
- Lateral/foraminal - pure radiculopathy without myelopathy (15-20%)
- Giant herniation - rare, extensive canal compromise
Calcification Pathophysiology:
Thoracic discs undergo dystrophic calcification more frequently than cervical or lumbar discs due to:
- Lower metabolic activity and vascularity in thoracic discs
- Chronic mechanical stress with minimal motion (repetitive microtrauma)
- Age-related degenerative changes with calcium deposition in nucleus and annulus
- Scheuermann's disease association (endplate irregularities promote degeneration)
Calcified thoracic discs:
- Identified on CT scan (essential preoperative imaging)
- Behave like bone during surgery - cannot be removed with rongeurs or curettes
- Require high-speed burr for safe removal (diamond burr reduces heat)
- Increased risk of dural tear and cord injury during removal
- May cause acute traumatic herniation (calcified disc acts as missile with high-energy trauma)
Cord Compression Pathomechanics:
Thoracic disc herniation causes myelopathy through:
- Direct mechanical compression - cord flattened against posterior canal
- Vascular compromise - compression of anterior spinal artery or radicular arteries
- Cord edema - seen as T2 hyperintensity on MRI (reversible in early stages)
- Myelomalacia - chronic compression leads to cord necrosis (irreversible)
Difference from Cervical and Lumbar:
- Cervical
- Cord with space
- Thoracic
- Cord (tight fit)
- Lumbar
- Cauda equina (nerve roots)
- Cervical
- Moderate (CSF buffer)
- Thoracic
- Poor (no buffer)
- Lumbar
- Good (roots mobile)
- Cervical
- Often safe
- Thoracic
- CONTRAINDICATED
- Lumbar
- Standard approach
- Cervical
- 10-20%
- Thoracic
- 40-70%
- Lumbar
- 5-10%
Two high-yield variants examiners test that go beyond the standard disc: the giant disc and the transdural (intradural) herniation. A giant thoracic disc occupies more than roughly 40 percent of the canal and is usually heavily calcified.
A chronic calcified disc can erode through the ventral dura into the subarachnoid space - a transdural (intradural) herniation (reported in around 5-10 percent of operative series). It is much more common with giant calcified discs.
- Imaging clues: on CT or CT-myelography look for intradural gas and the "comet-tail" sign with discontinuity of the ventral dura; MRI shows the herniation tracking intradurally with loss of the dural plane against the disc.
- Why it matters: a dural defect is already present, so the surgeon must anticipate and plan for a durotomy and dural reconstruction (primary repair, patch/graft, dural sealant, often a lumbar CSF drain) - CSF-leak rates are high and an unrecognised defect leads to a persistent fistula or pseudomeningocele.
- Technique principle: manage these anteriorly with planned dural repair, and never blunt-avulse an adherent calcified disc off the cord (it tears cord and dura). Burr the eggshell and, if a thin shell remains densely adherent to the dura, leaving it is acceptable provided the cord is decompressed.
Exam point: a giant calcified thoracic disc with intradural gas on CT is a transdural herniation - plan for the dural defect, anticipate CSF leak, and do not avulse the disc off the cord.
Classification Systems
Anatomical Location Classification (most clinically relevant)
This classification determines surgical approach selection:
- Definition
- Midline, posterior central canal
- Frequency
- 20-30%
- Clinical Features
- Myelopathy, bilateral findings, no radiculopathy
- Preferred Approach
- Anterior only (transthoracic, thoracoscopic)
- Definition
- Paracentral, eccentric
- Frequency
- 60-70%
- Clinical Features
- Myelopathy plus radiculopathy, most common
- Preferred Approach
- Anterior or posterolateral
- Definition
- Far lateral, in or beyond foramen
- Frequency
- 10-15%
- Clinical Features
- Radiculopathy only, no myelopathy
- Preferred Approach
- Posterolateral safe (transpedicular, lateral extracavitary)
This classification is critical for determining surgical approach and predicting outcomes.
Clinical Presentation
Symptom Patterns:
Thoracic disc herniation presents with three main clinical syndromes:
1. Myelopathy (50-70% of symptomatic cases):
Progressive spinal cord compression causes:
- Lower extremity weakness - UMN pattern (spasticity, hyperreflexia)
- Gait dysfunction - spastic, wide-based, scissoring gait
- Sensory level - at or below level of herniation
- Bowel/bladder dysfunction - urgency, frequency, retention (late finding)
- Positive Babinski sign - UMN lesion
- Hyperreflexia - below level of lesion
- Loss of abdominal reflexes - at level of compression
Lateral thoracic disc herniations may cause Brown-Séquard syndrome (hemicord syndrome):
- Ipsilateral: Motor weakness (corticospinal tract), loss of proprioception and vibration (dorsal columns)
- Contralateral: Loss of pain and temperature (spinothalamic tract crosses) This is classic exam material for thoracic spine pathology.
2. Radiculopathy (25-40%):
Thoracic radicular pain has unique features:
- Band-like pain around chest or abdomen following intercostal nerve distribution
- Mimics visceral pathology - cardiac (chest pain), abdominal (pancreatitis, cholecystitis)
- Worse with cough, sneeze, Valsalva - increased intraspinal pressure
- No classic dermatomal pattern - thoracic dermatomes less distinct than limb dermatomes
- May have sensory changes in thoracic dermatome (hypesthesia or hyperesthesia)
3. Axial Pain Alone (10-20%):
- Chronic midline thoracic back pain
- Mechanical pattern (worse with activity, better with rest)
- May be the only symptom for years
- Often leads to delayed diagnosis
Natural History:
Without treatment:
- A substantial proportion of established myelopathic cases progress to more severe deficit if untreated
- Gradual worsening over months to years (slow progression)
- Acute deterioration rare but possible (especially traumatic herniation)
- Spontaneous improvement uncommon once myelopathy develops
- Lower extremity strength testing (hip flexion, knee extension, ankle dorsi/plantarflexion)
- Spasticity assessment (increased tone, clonus)
- Gait evaluation (spastic, ataxic patterns)
- Pinprick and light touch to identify sensory level
- Proprioception and vibration (dorsal column function)
- Temperature sensation (often lost with pain in spinothalamic dysfunction)
- Lower extremity reflexes (hyperreflexia below lesion)
- Pathological reflexes (Babinski, Hoffman's if cervical involvement)
- Abdominal reflexes (T8-T12 - may be absent at level of lesion)
This completes the neurological examination findings.
Investigations
Imaging Modalities:
MRI - Diagnostic Modality of Choice:
- Purpose
- Assess cord signal, CSF, disc
- Key Findings
- Disc appears dark, cord compression visible, T2 hyperintensity in cord indicates edema/myelomalacia
- Purpose
- Determine herniation location
- Key Findings
- Central vs centrolateral vs lateral classification
- Purpose
- Anatomical detail
- Key Findings
- Disc-cord relationship, vertebral body marrow
- Purpose
- Rule out tumor, infection
- Key Findings
- Enhancement suggests neoplasm or infection vs bland disc
MRI Findings:
- Disc herniation - posterior disc protrusion or extrusion
- Cord compression - flattening or displacement of spinal cord
- Cord signal change - T2 hyperintensity indicates edema (reversible) or myelomalacia (irreversible)
- Location - central, centrolateral, or lateral
- Levels involved - single or multiple
Cord signal change on T2-weighted MRI has prognostic significance:
- No signal change - better surgical outcomes, more reversible compression
- Faint/mild hyperintensity - cord edema, still potentially reversible
- Intense hyperintensity - myelomalacia (cord necrosis), poor prognosis, likely permanent deficit
This helps counsel patients on expected recovery and surgical urgency.
- All operative candidates - assess for calcification
- MRI contraindicated - pacemaker, claustrophobia
- CT myelography - if MRI not available (water-soluble contrast via lumbar puncture)
- Disc calcification - appears as high-density material (40-70% of cases)
- Bony anatomy - pedicle size for transpedicular approach
- Ossification - OPLL vs calcified disc
- Extent of calcification - plan for burr use vs rongeur removal
Limited value but may show:
- Disc space narrowing at affected level
- Calcified disc - visible on lateral radiograph (pathognomonic when present)
- Scheuermann's changes - irregular endplates, Schmorl's nodes
- Overall alignment - kyphosis, scoliosis
Not diagnostic but may raise suspicion in appropriate clinical context.
- Baseline - establish preoperative cord function
- Intraoperative monitoring - detect cord ischemia during surgery
- More sensitive than SSEPs for detecting motor pathway injury
- Used during thoracic discectomy to guide safe decompression
- Limited role in thoracic radiculopathy (intercostal muscles difficult to study)
- May help exclude peripheral nerve lesions
Consider other causes of thoracic myelopathy:
- Tumor - MRI with contrast (enhancement)
- Infection - inflammatory markers (CRP, ESR), blood cultures, MRI
- Demyelination - brain MRI, CSF analysis
- Vascular - dural arteriovenous fistula (spinal angiography)
- Metabolic - B12, copper, vitamin E levels
- Distinguishing Features
- Insidious myelopathy or band-like radicular pain; often calcified
- Key Investigation
- MRI (cord compression) + CT (calcification)
- Distinguishing Features
- Known malignancy, constitutional symptoms, rapid progression, night pain
- Key Investigation
- Whole-spine MRI with contrast, staging
- Distinguishing Features
- Fever, raised CRP/ESR, immunosuppression, IVDU
- Key Investigation
- MRI with contrast, CRP/ESR, blood cultures
- Distinguishing Features
- Myelopathy, dense ossification, no disc extrusion
- Key Investigation
- CT (ossification) + MRI
- Distinguishing Features
- Younger, relapsing course, longitudinally extensive cord signal
- Key Investigation
- Brain + cord MRI, CSF oligoclonal bands
- Distinguishing Features
- Stepwise myelopathy, lower-limb claudication, flow voids on MRI
- Key Investigation
- Spinal MRI/MRA, spinal angiography
- Distinguishing Features
- Band-like chest/abdominal pain without neurology; pain pattern atypical for spine
- Key Investigation
- ECG/troponin, abdominal imaging as indicated
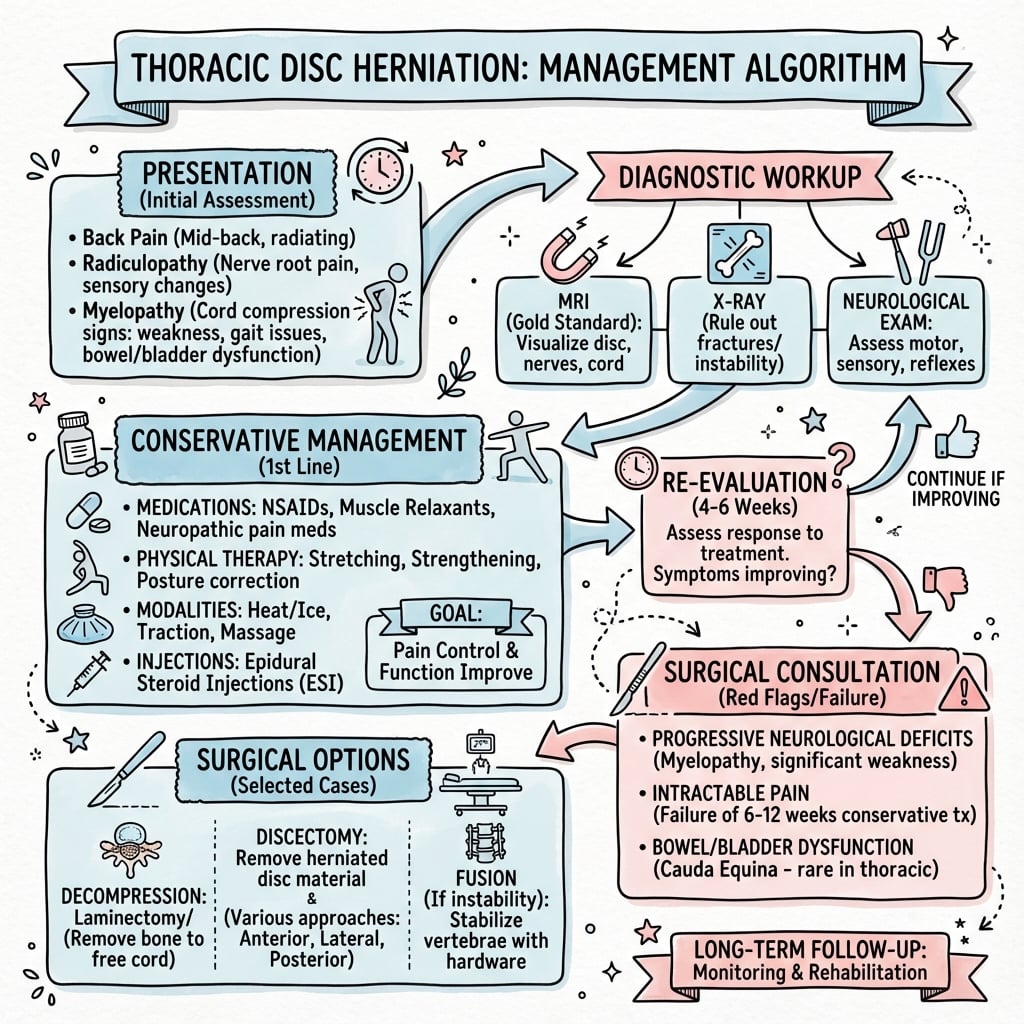
Management
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- Mild radiculopathy without motor weakness
- Axial pain only (no neurological deficit)
- Asymptomatic incidental finding
- Medical comorbidities precluding surgery
- Patient preference after informed discussion
- Analgesia: NSAIDs, acetaminophen, neuropathic pain agents (gabapentin, pregabalin)
- Activity modification: Avoid provocative activities, ergonomic adjustments
- Physical therapy: Core strengthening, posture training (limited role in thoracic disc)
- Monitoring: Serial neurological examinations, MRI if worsening
Success Rate: many patients with mild radiculopathy or axial pain (no myelopathy) improve with conservative care; conservative management is not appropriate once myelopathy is established
When to Abandon Conservative Treatment:
- Development of myelopathy
- Progressive motor weakness
- Bowel/bladder dysfunction
- Intractable pain despite optimal management
Progressive myelopathy from thoracic disc herniation is a surgical indication. Unlike cervical myelopathy where some mild cases may stabilize, thoracic myelopathy has a narrow canal with less compensatory capacity. Delaying surgery risks irreversible cord damage. Do not attempt prolonged conservative management in the presence of myelopathy.
Surgical Approaches
- Central or centrolateral disc herniation
- Best visualization of disc-cord interface
- Gold standard for calcified central discs
- Position: Lateral decubitus, affected side up
- Incision: Posterolateral thoracotomy at rib level corresponding to disc (e.g., 9th rib for T8-T9 disc)
- Single lung ventilation: Deflate ipsilateral lung for exposure
- Rib resection: Remove rib, divide intercostal muscles
- Pleural entry: Enter pleural cavity, pack lung anteriorly
- Identify level: Count ribs, confirm with intraoperative radiograph
- Expose vertebral bodies: Dissect parietal pleura, identify disc space
- Segmental vessels: Ligate at disc level (beware Adamkiewicz)
- Discectomy: Remove disc anterior and posterior longitudinal ligament
- Decompress cord: Remove all herniated material, ensure cord decompression
- Fusion: Consider corpectomy and cage if extensive removal (optional)
- Closure: Chest tube, layer closure
- Excellent visualization
- Direct access to disc without cord manipulation
- Can remove calcified disc safely
- Requires thoracotomy (post-thoracotomy pain)
- Single lung ventilation (pulmonary complications)
- May need cardiothoracic surgery assistance
- Longer hospital stay
This completes the transthoracic approach description.
Surgical Pearls:
Calcified thoracic disc removal:
- Use high-speed diamond burr (reduces heat compared to cutting burr)
- Thin posterior shell of calcified disc first (like eggshell)
- Micro-rongeurs to remove fragments through thin shell
- Avoid levering against cord - this causes direct injury
- Copious irrigation during burring to reduce heat
- Monitor SSEPs/MEPs throughout to detect early cord ischemia
Intraoperative Neuromonitoring:
All thoracic disc surgeries should have:
- SSEPs - baseline and continuous monitoring
- MEPs - more sensitive for motor pathway
- Alarm criteria: 50% amplitude decrease or 10% latency increase
- Response to changes: Stop manipulation, increase MAP, consider aborting
Operating on the wrong level is the classic, catastrophic, medicolegal pitfall unique to the thoracic spine - it is the commonest region for wrong-level spine surgery, and "counting ribs" alone is not enough.
- Why it happens: the thoracic spine is a long, featureless segment with no reliable intra-operative landmark; the cord-compressing disc is often not palpable; and anatomical variants defeat simple counting - a transitional thoracolumbar vertebra or a cervical or lumbar rib changes the number of rib-bearing vertebrae and throws off any rib count.
- Pre-operative safeguards: count levels on a whole-spine/long-cassette MRI from a fixed reliable landmark - both down from C2 and up from the sacrum/L5 - and reconcile the two counts; explicitly document any anomalous ribs or transitional vertebra.
- Intra-operative confirmation: rib counting under fluoroscopy is unreliable in isolation - use a true AP/lateral fluoroscopic count referenced to a fixed landmark with a radio-opaque marker.
- The most reliable safeguard for a difficult level is pre-operative marking: a CT-guided percutaneous marker placed the day of/before surgery - methylene blue, a fiducial/coil, a marker screw, or a small dab of vertebroplasty cement at the target pedicle.
- Process: an imaging-confirmed level documented in the notes, plus a surgical "time-out" before incision and again before the discectomy.
Exam point: never rely on rib-counting alone in the thoracic spine - confirm the level against a fixed landmark with fluoroscopy, and for difficult cases use a pre-operative CT-guided marker.
APPROACHESAPPROACHES - Surgical Approach Selection
Hook:APPROACHES covers all surgical options and critical technical points
Complications
Surgical Complications:
- Transthoracic
- 5-10%
- Thoracoscopic
- 5-8%
- Costotransversectomy
- 10-15%
- Transthoracic
- 15-20%
- Thoracoscopic
- 10-15%
- Costotransversectomy
- Less than 5%
- Transthoracic
- 5-10%
- Thoracoscopic
- 5-8%
- Costotransversectomy
- Less than 5%
- Transthoracic
- 2-5%
- Thoracoscopic
- 2-4%
- Costotransversectomy
- Less than 2%
- Transthoracic
- 20-30%
- Thoracoscopic
- 10-15%
- Costotransversectomy
- 5-10%
- Paraplegia - most feared complication
- Worsening myelopathy - cord manipulation or ischemia
- Mechanisms: Direct cord injury, vascular injury (Adamkiewicz), spinal cord ischemia
- Prevention: Avoid cord retraction, neuromonitoring, gentle technique, anterior approach for central disc
- Management: High-dose steroids controversial, supportive care, rehabilitation
- Pneumothorax - inadequate chest tube drainage
- Pleural effusion - post-thoracotomy inflammation
- Pneumonia - single lung ventilation, atelectasis
- Prolonged air leak - pleural space issues
- Prevention: Chest physiotherapy, incentive spirometry, adequate chest tube management
- Management: Chest tube management, antibiotics if pneumonia, supportive care
- Incidental durotomy - especially with calcified disc removal
- CSF fistula - persistent leak through wound
- Pseudomeningocele - CSF collection
- Prevention: Careful dural dissection, burr away from dura
- Management: Primary repair if identified, oversew with 6-0 Prolene, consider lumbar drain if persistent, revision surgery if pseudomeningocele symptomatic
- Artery of Adamkiewicz - anterior spinal artery syndrome (paraplegia)
- Segmental arteries - bleeding, cord ischemia
- Aorta - rare but catastrophic (anterior approaches)
- Prevention: Identify Adamkiewicz preoperatively (CT angiography), careful vessel ligation, maintain MAP during surgery
- Management: Control bleeding, vascular surgery consultation if major vessel, supportive care for cord ischemia
Chronic post-thoracotomy pain affects 20-30% of patients after open transthoracic approach. This is intercostal neuralgia from rib retraction and nerve injury. It can be severe and persistent, affecting quality of life. Counsel patients preoperatively. Consider thoracoscopic approach to reduce this risk. Manage with neuropathic pain medications, nerve blocks, and pain clinic referral if severe.
- Wound infection (2-5%) - superficial or deep, antibiotics or debridement
- Seroma - fluid collection, usually self-limiting
- Intercostal neuralgia - rib retraction injury, chronic pain
- Horner's syndrome - sympathetic chain injury (upper thoracic), ptosis/miosis/anhidrosis
- Chylothorax - thoracic duct injury (left-sided approaches above T6), milky chest tube output, conservative management or ligation
- Progressive myelopathy (25-50%) - delayed surgery may have worse outcomes
- Irreversible cord damage - myelomalacia from prolonged compression
- Chronic pain - persistent radiculopathy or axial pain
- Functional decline - loss of ambulation, wheelchair dependence
Postoperative Care and Outcomes
Immediate Postoperative Management:
Rehabilitation Protocol
- Goals: Pain control, wound healing, basic mobility
- Activities: Walking, gentle range of motion, respiratory exercises
- Restrictions: No lifting over 5kg, no twisting, no strenuous activity
- Goals: Restore function, improve strength
- Activities: Progressive resistance training, core strengthening, balance
- Restrictions: Gradual increase in lifting, avoid high-impact activities
- Goals: Return to full activities, work, sports
- Activities: Sport-specific training, unrestricted activities as tolerated
- Monitoring: Serial neurological examinations, functional outcome measures
- Description
- Modified Japanese Orthopaedic Association (0-11)
- Use
- Myelopathy severity and improvement
- Description
- 0-5 scale of myelopathy
- Use
- Simple grading system
- Description
- Visual Analog Scale for pain (0-10)
- Use
- Pain assessment
- Description
- Oswestry Disability Index
- Use
- Functional limitation
- Description
- Quality of life measure
- Use
- General health status
Surgical Outcomes:
Based on systematic reviews and case series (see Evidence Base - Stillerman et al 1998, Quint et al 2011, Brotis et al 2019, Hamid et al 2023):
- 60-80% improve or stabilize after surgery
- 15-20% no change
- 5-10% worsen (neurological deterioration)
- Shorter duration of symptoms (less than 12 months better than over 24 months)
- No preoperative T2 signal change on MRI (myelomalacia predicts poor recovery)
- Younger age (under 60 years better outcomes)
- Soft disc (calcified discs more difficult, higher complication rate)
- Lateral location (central discs more challenging, worse outcomes)
- Long-standing myelopathy (over 24 months)
- Severe preoperative deficits (non-ambulatory, Nurick grade 4-5)
- Cord signal change (myelomalacia on MRI)
- Older age (over 70 years)
- Multiple medical comorbidities
Neurological recovery after thoracic discectomy:
- Immediate - decompression relieves mechanical pressure
- Weeks to months - cord edema resolves, early motor return
- 6-12 months - continued improvement (cord remyelination)
- 12-18 months - plateau of recovery
Counsel patients that maximum recovery takes 12-18 months. Early postoperative neurological status may not reflect final outcome. Continue therapy and rehabilitation throughout recovery period.
Return to Activities:
- Desk work: 6-8 weeks (sooner if minimally invasive approach)
- Manual labor: 12-16 weeks
- Contact sports: 6 months (after full recovery and rehabilitation)
- Driving: 4-6 weeks (when off narcotics and able to perform emergency stop)
Guidelines, Registries & Global Practice
Global Epidemiology
- Figure
- 0.25-0.75%
- Source
- Arce & Dohrmann, Surg Neurol 1985 (PMID 3975822)
- Figure
- Approximately 1 per 1,000,000 per year
- Source
- Stillerman et al, J Neurosurg 1998 (PMID 9525706)
- Figure
- 4th decade
- Source
- Arce & Dohrmann 1985 (PMID 3975822)
- Figure
- 75% below T8
- Source
- Arce & Dohrmann 1985 (PMID 3975822)
- Figure
- Approximately 65%
- Source
- Stillerman et al 1998 (PMID 9525706)
- Figure
- 37%
- Source
- Wood et al, JBJS Am 1995 (PMID 7593072)
Guidance and Consensus, Side by Side
There is no high-level randomised guideline for this rare condition; practice is driven by case series, meta-analyses, and society/spine-unit consensus. The points where bodies genuinely converge or differ:
- Position
- Posterior decompressive laminectomy is contraindicated for central/calcified discs; favour anterior or posterolateral routes
- Evidence base
- Level IV series; laminectomy 57% vs over 80% success (PMID 3975822)
- Position
- All approaches acceptable; posterolateral carries lower medical/surgical morbidity than anterior/lateral
- Evidence base
- Level III, 1036 patients (PMID 31493617)
- Position
- Thoracoscopic microdiscectomy is a safe alternative to open thoracotomy for soft centrolateral discs in experienced units
- Evidence base
- Level IV, 167 cases (PMID 22160099)
- Position
- Lower-morbidity posterolateral option for centrolateral discs
- Evidence base
- Level III, 328 patients (PMID 37475044)
- Position
- Progressive thoracic myelopathy warrants urgent specialist referral and decompression; observation reserved for radiculopathy/axial pain without cord compromise
- Evidence base
- Consensus / Level IV
Registry Evidence
National joint registries (NJR, AJRR, AOANJRR, SHAR) do not capture thoracic discectomy, and no dedicated thoracic disc registry exists, reflecting the rarity of the condition. The best pooled evidence is therefore from systematic reviews and network meta-analyses rather than registry data: surgery carries minimal mortality but overall morbidity up to 29%, with approach-specific differences (PMID 31493617).
Global Practice Variation
- High-resource settings: Care concentrated in tertiary/quaternary spine units with intraoperative neuromonitoring (SSEPs/MEPs); growing use of thoracoscopic and tubular minimally invasive approaches; cardiothoracic collaboration for transthoracic exposure.
- Limited-resource settings: Open transthoracic or costotransversectomy predominate where thoracoscopic equipment and neuromonitoring are unavailable; later presentation with established myelopathy is more common, worsening prognosis.
- Regional preference: Endoscopic spine techniques have been adopted earliest and most widely in parts of Asia, while open and tubular posterolateral approaches remain standard in many Western units.
- Perioperative care (universal principles): Single-shot antibiotic prophylaxis at induction (e.g. cefazolin), mechanical and chemical VTE prophylaxis, neuropathic agents (gabapentin/pregabalin) for radicular pain, and structured rehabilitation for myelopathic patients. Outcomes converge internationally at 60-80% neurological improvement.
MCQ Practice Points
Q: Why is posterior laminectomy contraindicated for central thoracic disc herniation?
A: The thoracic spinal cord cannot be safely retracted. The thoracic canal is narrow (12-14mm diameter) with the cord occupying 40-50% of the space. There is minimal CSF dorsally. Attempting to access a central disc from behind requires retracting the cord posteriorly, which causes direct mechanical injury and vascular compromise resulting in irreversible paraplegia. In contrast, the cervical canal has more space (cord occupies only 25%) allowing safer posterior retraction. The lumbar spine has nerve roots (cauda equina) which can be retracted. This is the single most important concept in thoracic disc surgery.
Q: What is the artery of Adamkiewicz and why is it clinically important?
A: The arteria radicularis magna (artery of Adamkiewicz) is the largest anterior segmental medullary artery supplying the lower two-thirds of the spinal cord via the anterior spinal artery. It is located at T9-L2 in 80% of individuals, most commonly at T9-T11, and enters from the left side in 75-80%. Clinically, it's important because injury during thoracic surgery (especially when ligating segmental vessels during transthoracic approach or anterior spinal procedures) can cause anterior spinal artery syndrome with paraplegia, loss of pain and temperature sensation below the lesion, but preservation of proprioception (dorsal columns spared). Some surgeons obtain preoperative CT angiography to identify its location, though this is not routine.
Q: What imaging modality best assesses calcification in thoracic disc herniation and why is this important?
A: CT scan is the best modality for assessing disc calcification. 40-70% of symptomatic thoracic disc herniations are calcified, and this is critical surgical information because calcified discs behave like bone - they cannot be removed with standard rongeurs or curettes. The surgeon must use a high-speed diamond burr to carefully thin the posterior shell of the calcified disc (like an eggshell) and then remove fragments. This increases operative time, difficulty, and risk of dural tear and cord injury. Preoperative knowledge of calcification allows proper surgical planning and patient counseling about increased risks.
Q: What is the prognostic significance of T2 hyperintensity in the spinal cord on MRI?
A: T2 hyperintensity (increased signal) in the spinal cord indicates cord edema or myelomalacia:
- Mild/faint hyperintensity suggests cord edema which is potentially reversible with decompression
- Intense hyperintensity suggests myelomalacia (cord necrosis) which is irreversible
- Patients with no T2 signal change have better surgical outcomes
- Patients with myelomalacia have poor recovery potential - many deficits will be permanent despite adequate surgical decompression
This information helps counsel patients about realistic expectations. A patient with severe myelomalacia should understand that surgery prevents further deterioration but may not restore lost function.
Q: How do you select surgical approach for thoracic disc herniation?
- Central disc → Anterior approach mandatory (transthoracic, thoracoscopic) - posterior contraindicated
- Centrolateral disc → Anterior or posterolateral (transthoracic, costotransversectomy) - surgeon preference and patient factors
- Lateral/foraminal disc → Posterolateral acceptable (transpedicular, lateral extracavitary) - no need for thoracotomy
- Calcified disc → Anterior approach preferred (better visualization for burr work)
- COPD/pulmonary disease → Favor costotransversectomy or VATS over open thoracotomy
- Surgeon expertise → Thoracoscopic requires specialized training
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old male presents with 6-month history of progressive lower limb weakness and gait dysfunction. MRI shows a central T10-T11 disc herniation with cord compression and T2 signal change. CT confirms the disc is heavily calcified. How would you manage this patient?”
“A 45-year-old female presents with 3-month history of band-like chest pain around the left T8 dermatome. No lower limb weakness. MRI shows a lateral T7-T8 disc herniation in the left foramen. How would you manage this?”
“A 60-year-old patient with significant COPD and FEV1 of 45% predicted has thoracic myelopathy from a centrolateral T9-T10 disc herniation. How do you approach surgical decision-making?”
Key Epidemiology
- 0.5-1% of all disc herniations (RARE)
- 75% occur at T8-T12 (lower thoracic)
- Peak age 40-60 years
- 40-70% are calcified (complicates surgery)
Critical Anatomy
- Narrow thoracic canal (12-14mm diameter)
- Cord occupies 40-50% of canal (vs 25% cervical)
- Limited CSF space dorsally
- Artery of Adamkiewicz at T9-L2 (usually LEFT)
Why Posterior is Contraindicated
- Cord CANNOT be safely retracted in thoracic spine
- Historical posterior laminectomy: only 57% success vs over 80% other approaches
- Central disc from posterior = PARAPLEGIA
- Must use anterior or anterolateral approach
Clinical Presentation
- Myelopathy 50-70%: weakness, spasticity, gait dysfunction
- Radiculopathy 25-40%: band-like chest/abdominal pain
- Axial pain 10-20%: chronic thoracic back pain
- T2 hyperintensity = myelomalacia (poor prognosis)
Investigations
- MRI: Diagnostic modality of choice
- CT: Essential for calcification assessment
- T2 signal change: Edema vs myelomalacia (prognosis)
- Neuromonitoring: SSEPs and MEPs intraoperatively
Approach Selection
- CENTRAL: Anterior only (transthoracic, VATS)
- CENTROLATERAL: Anterior or posterolateral (costotransversectomy)
- LATERAL: Posterolateral OK (transpedicular)
- Calcified disc: Anterior preferred (better visualization)
Transthoracic Approach
- Lateral decubitus, single lung ventilation
- Rib resection, enter pleural cavity
- Ligate segmental vessels (beware Adamkiewicz)
- Direct anterior disc access, burr for calcified disc
Calcified Disc Technique
- High-speed DIAMOND burr (reduces heat)
- Thin posterior shell like eggshell
- Remove fragments through thin shell
- Copious irrigation, NO levering against cord
Complications
- Neurological deterioration 5-15% (paraplegia worst)
- Pulmonary 10-20% (pneumothorax, effusion, pneumonia)
- CSF leak/dural tear 5-10%
- Chronic post-thoracotomy pain 20-30%
Outcomes
- 60-80% improve or stabilize
- Recovery takes 12-18 months (counsel patient)
- Better if: short duration, no T2 change, younger, soft disc
- Worse if: long-standing, myelomalacia, older, calcified
Viva Killer Points
- Posterior laminectomy for central disc = CONTRAINDICATED
- Why: Cord cannot be retracted (narrow canal)
- Adamkiewicz: T9-L2, LEFT side, anterior spinal artery supply
- Calcified disc (40-70%): CT essential, requires burr
Evidence Base
- Review of 280 reported thoracic disc herniations with CT-improved diagnosis
- Peak incidence in the fourth decade; 75% of protruded discs occurred below T8
- Surgical success ranged from 57% for decompressive laminectomy to over 80% for posterolateral, lateral, and transthoracic approaches
- Favourable prognostic group: history of trauma, symptoms less than one month, soft disc
- Single-surgeon series of 82 herniated thoracic discs in 71 patients (1971-1995)
- Calcification present in 65%; intradural extension in 7%; multiple herniations in 14%
- Four approaches used: transthoracic (60%), transfacet pedicle-sparing (28%), lateral extracavitary (10%), transpedicular (2%)
- Postoperative improvement: pain 87%, spasticity 95%, sensory 84%, bladder 76%, motor 58%; overall complication rate 14.6%
- Prospective cohort of 167 consecutive single-level thoracoscopic microdiscectomies
- Mean VAS pain reduced by 4.4 points; ASIA motor score improved by mean 4.6 points
- At 2 years, 79% reported excellent/good pain outcome and 80% excellent/good motor outcome
- Overall complication rate 15.6%
- Systematic review and network meta-analysis of 15 studies, 1036 patients
- Surgery carried minimal mortality (3 deaths) but overall morbidity as high as 29%
- Complications: medical 21%, surgical-site 11%, CSF-related 8%, neurological 5%
- Anterior and lateral approaches carried higher medical and surgical complication risk than the posterolateral approach
- Systematic review and meta-analysis of the transfacet pedicle-sparing approach, 328 patients across 11 studies
- Significant improvement in VAS pain and Nurick myelopathy scores after surgery
- Pooled overall complication rate 12.4% with 3.5% neurological worsening
- Lower complication rates and shorter hospital stay than alternative approaches in selected patients
- MRI of 90 asymptomatic individuals to define the prevalence of incidental thoracic findings
- 73% had at least one positive anatomical finding
- Disc herniation in 37%, disc bulge in 53%, annular tear in 58%, cord deformation in 29%
- Findings represent radiological abnormalities only and require clinical correlation
- Some advocate leaving small calcified fragments vs complete removal
- Risk of incomplete decompression vs risk of cord injury during aggressive removal
- No high-quality comparative data
- Some surgeons perform fusion after extensive discectomy or corpectomy
- Others perform discectomy alone without fusion
- Thoracic spine stability from rib cage may allow discectomy without fusion
- No RCT data comparing outcomes
- Incidental thoracic disc herniations common on MRI
- No clear consensus on surveillance vs prophylactic surgery
- Generally observe unless developing symptoms