T10-L2 Junction | TLICS Guides Treatment | PLC is Key
- TLICS score (morphology + PLC + neurology) guides treatment decisions
- Posterior ligamentous complex (PLC) is the key stability determinant
- T12-L1 junction is the most commonly injured level (transition zone)
- Burst fractures may be managed non-op if TLICS less than 4 and neurologically intact
- Short segment fixation (one above, one below) is current trend
- “TLICS 4 or more indicates surgical management
- “Indeterminate PLC on imaging = 2 points, disrupted = 3 points
- “Neurogenic claudication suggests cauda equina level
- “Thoracolumbar junction is transition from rigid kyphotic thoracic to mobile lordotic lumbar
Three components: Morphology (1-4) + PLC status (0-3) + Neurological status (0-3). Score of 5 or more indicates surgery. PLC is worth most points and is the key determinant.
Posterior ligamentous complex = supraspinous, interspinous, ligamentum flavum, facet capsules. MRI essential for assessment. Widened interspinous space and T2 signal = disrupted.
T12-L1 is most vulnerable because it's a transition zone: rigid kyphotic thoracic spine meets mobile lordotic lumbar spine. Energy concentrates here.
Conus ends L1-L2. Above = cord injury (UMN signs). Below = cauda equina (LMN signs, bladder). Incomplete cauda has better prognosis than complete cord.
- Pattern Example
- Compression fracture, PLC intact
- Treatment
- TLSO brace 8-12 weeks
- Key Pearl
- Most common scenario - non-op works well
- Pattern Example
- Burst, indeterminate PLC
- Treatment
- Surgeon preference
- Key Pearl
- MRI critical - PLC status determines treatment
- Pattern Example
- Burst + disrupted PLC
- Treatment
- Posterior stabilization
- Key Pearl
- Short segment pedicle screws
- Pattern Example
- Translation + incomplete neuro deficit
- Treatment
- Urgent posterior decompression + fusion
- Key Pearl
- Consider anterior if significant vertebral body loss
MPNTLICS Score Components
Hook:MPN guides treatment: Morphology, PLC, Neurology - TLICS 5+ means surgery!
SFLCPLC Components
Hook:The PLC is the posterior tension band - if disrupted, the spine is unstable in flexion!
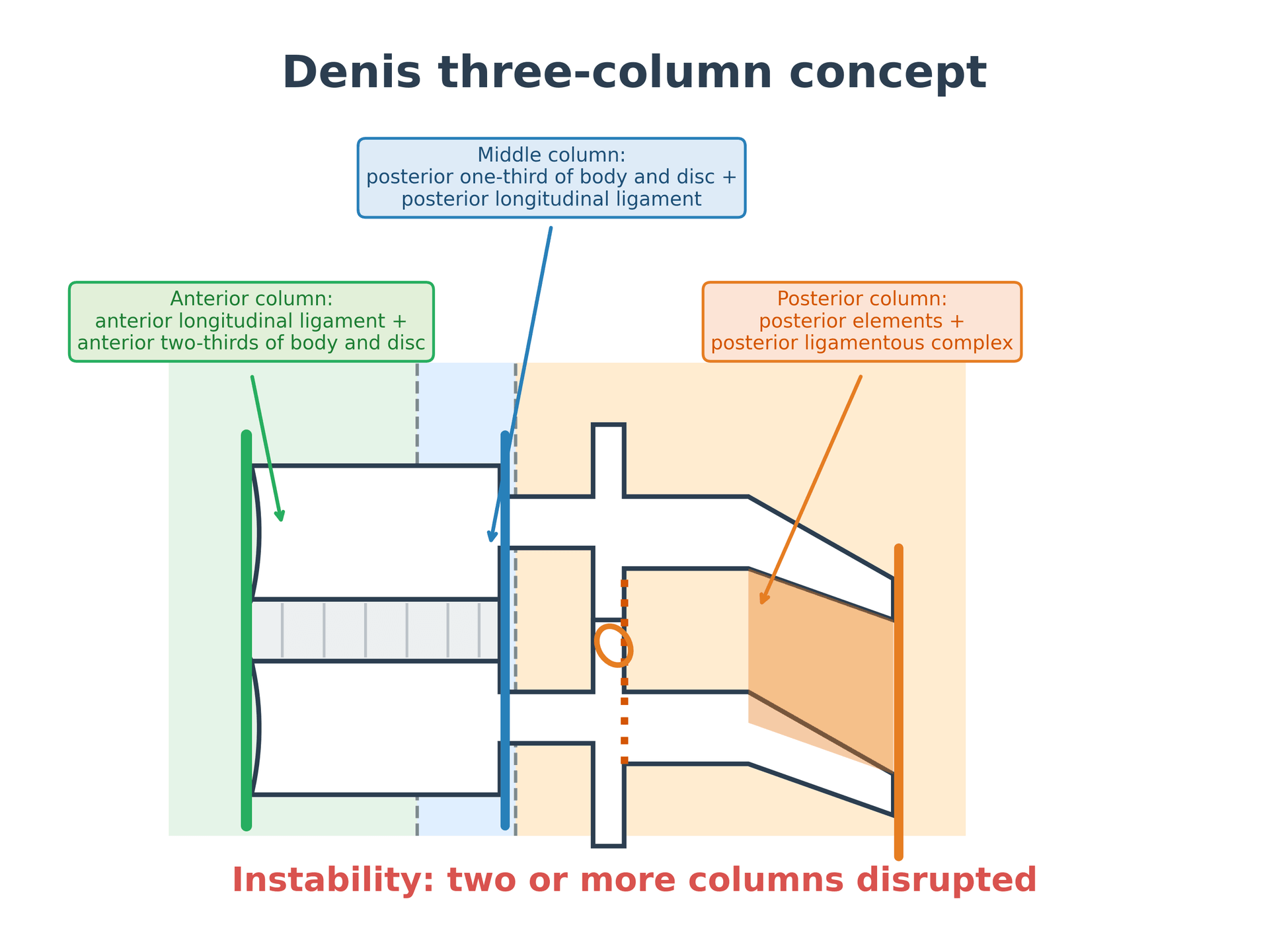
AMPDenis Three-Column Concept
Hook:Denis: Two-column injury = unstable. Middle column is the key to stability!
TRANSThoracolumbar Junction
Hook:TRANS-ition from rigid to mobile is where energy concentrates and fractures occur!
Overview and Epidemiology
Thoracolumbar fractures are the most common spinal fractures, typically occurring at the thoracolumbar junction (T10-L2), with peak incidence at T12-L1.
Epidemiology:
- Bimodal distribution: young trauma, elderly osteoporotic
- Male predominance in high-energy trauma
- Female predominance in osteoporotic fractures
- MVA and falls are primary mechanisms
- Associated injuries common (50% have other injuries)
The thoracolumbar junction (T12-L1) is where the rigid kyphotic thoracic spine (stabilized by rib cage) meets the mobile lordotic lumbar spine (no ribs). This creates a stress concentration - energy focuses here, making it the most common fracture site.
Associated injuries:
- Visceral (liver, spleen, kidneys)
- Other spine levels (10-15% have non-contiguous fractures)
- Lower extremity (calcaneus fractures with axial load)
- Head injuries
Anatomy and Biomechanics
Denis three-column concept:
- Structures
- Anterior 2/3 vertebral body, disc, ALL
- Function
- Compression resistance
- Structures
- Posterior 1/3 vertebral body, disc, PLL
- Function
- Key stability (compression and tension)
- Structures
- Pedicles, facets, laminae, spinous processes, PLC
- Function
- Tension band, flexion resistance
In Denis' concept, the middle column is the key to stability. Injury to the middle column (burst fracture) is more significant than anterior column alone (compression fracture). Two-column injury = unstable.
Components that form the posterior "tension band":
- Supraspinous ligament
- Interspinous ligament
- Ligamentum flavum
- Facet joint capsules
- Primary restraint to flexion
- If disrupted, spine fails in flexion
- Brace/cast cannot substitute for PLC
- This is why TLICS weights PLC at 3 points
- Conus medullaris ends T12-L2 (usually L1)
- Above conus: spinal cord injury (UMN)
- At conus: mixed picture
- Below conus: cauda equina (LMN, better prognosis)
- Flexion-compression: Compression and burst fractures
- Flexion-distraction: Chance fractures, seat belt injuries
- Translation/rotation: Fracture-dislocations (most unstable)
- Extension: Hyperextension injuries (rare)
Classification Systems
Thoracolumbar Injury Classification and Severity Score (TLICS)
The TLICS is the most widely used classification for guiding treatment decisions.
Component 1: Morphology (1-4 points)
- Points
- 1
- Description
- Loss of vertebral height, anterior wedge
- Points
- 2
- Description
- Anterior and posterior cortex involvement, canal compromise
- Points
- 3
- Description
- Horizontal displacement or rotation
- Points
- 4
- Description
- Abnormal separation of vertebrae (flexion or extension)
Component 2: Posterior Ligamentous Complex (0-3 points)
- Points
- 0
- Imaging Findings
- Normal anatomy, no widening
- Points
- 2
- Imaging Findings
- Interspinous widening, subtle T2 signal
- Points
- 3
- Imaging Findings
- Facet diastasis, T2 signal in PLC, widened spinous processes
Component 3: Neurological Status (0-3 points)
- Points
- 0
- Description
- No deficit
- Points
- 2
- Description
- Radiculopathy
- Points
- 2
- Description
- Complete deficit
- Points
- 3
- Description
- Incomplete - needs decompression
- Points
- +1
- Description
- Add to score for ongoing compression
- TLICS 0-3: Non-operative (brace)
- TLICS 4: Surgeon discretion (often non-op if PLC intact)
- TLICS 5+: Operative

Clinical Assessment
History:
- Mechanism (MVA, fall from height, fall from standing)
- Energy level guides suspicion
- Neurological symptoms (weakness, numbness, bowel/bladder)
- Previous spine problems
- Osteoporosis risk factors
Physical examination:
- Inspection: Bruising (especially transverse), deformity, swelling
- Palpation: Tenderness, step-off, interspinous gap
- Neurological: Complete lower limb neuro exam
- Log-roll: Full spine palpation
- Abdominal: Seat belt sign = 50% have intra-abdominal injury
- Calcaneus: Axial load mechanism
- Other spine levels: 10-15% non-contiguous
- Head: Altered consciousness affects exam reliability
Neurological examination:
- Cord (above L1)
- Hyperreflexia, Babinski+
- Cauda Equina (below L1)
- Hyporeflexia/areflexia
- Cord (above L1)
- Increased (spasticity)
- Cauda Equina (below L1)
- Decreased (flaccid)
- Cord (above L1)
- Symmetric, level-dependent
- Cauda Equina (below L1)
- Asymmetric, root pattern
- Cord (above L1)
- Spastic, small capacity
- Cauda Equina (below L1)
- Atonic, overflow
- Cord (above L1)
- Variable
- Cauda Equina (below L1)
- Better (peripheral nerve)
- L1: Inguinal region
- L2: Anterior thigh, hip flexion
- L3: Knee, knee extension
- L4: Medial ankle, ankle dorsiflexion
- L5: Dorsal foot, big toe extension
- S1: Lateral foot, ankle plantarflexion
- S2-5: Perianal sensation (critical for complete vs incomplete)
Investigations
Imaging Protocol
First-line in trauma. Thin-cut from T10-L3 (extend as needed). Sagittal and coronal reconstructions. Assess morphology, canal compromise, posterior element injury.
Essential for PLC and cord. STIR best for ligament injury. T2 for cord edema/contusion. Helps differentiate indeterminate from injured PLC.
Bone quality affects treatment. May influence decision for cement augmentation or longer constructs.
Assess fusion. Earlier if concern about hardware or loss of correction.
CT interpretation:
Key features to assess:
- Vertebral body: Loss of height (%), endplate involvement
- Canal compromise: Percentage occlusion
- Posterior elements: Pedicle fractures, facet injuries, lamina fractures
- Spinous process widening: Suggests PLC injury
- Translation/rotation: Highly unstable pattern
MRI for TLICS scoring:
- Widened interspinous space with T2/STIR hyperintensity
- Facet widening or subluxation with fluid
- Disruption of supraspinous ligament (high signal replacing dark line)
- Ligamentum flavum signal change
These findings convert "indeterminate" (2 points) to "injured" (3 points) on TLICS.
- Imaging
- CT thoracolumbar
- Key Question
- Rule out fracture, assess morphology
- Imaging
- MRI if surgical candidate
- Key Question
- PLC status for TLICS
- Imaging
- Urgent MRI
- Key Question
- Cord/cauda compression, surgical planning
- Imaging
- CT, consider MRI if surgery
- Key Question
- Multiple levels, PLC status
Management
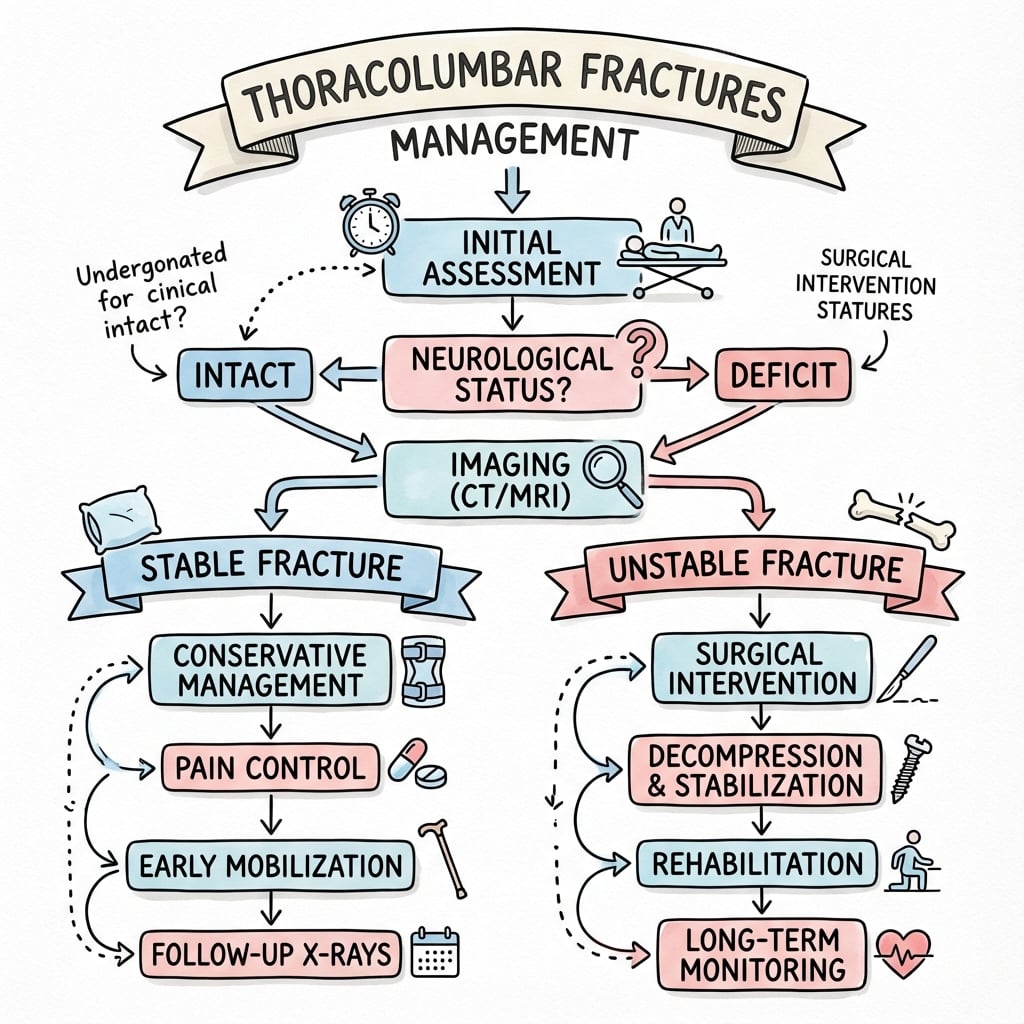
Conservative Treatment
Indications (TLICS 0-3):
- Compression fracture with intact PLC
- Some burst fractures with TLICS less than 4
- Neurologically intact
- Stable fracture pattern
Protocol:
Non-Operative Protocol
Pain control, bed rest as needed, log-roll precautions. May stand with TLSO if tolerated.
TLSO brace (thoracolumbar sacral orthosis) full-time except sleeping. Serial X-rays at 2, 6, 12 weeks. Monitor for kyphosis progression.
Gradual brace weaning. Physiotherapy for core strengthening. Return to activities based on symptoms and imaging.
Imaging follow-up:
- X-rays at 2, 6, 12 weeks
- Look for kyphosis progression more than 10-15 degrees
- If progressing: consider surgery
Convert to surgery if:
- Kyphosis progresses more than 10-15 degrees
- Neurological deterioration
- Unable to mobilize with brace
- Uncontrolled pain
The other half of the bimodal distribution is the osteoporotic vertebral compression fracture (VCF), where the problem is bone quality, not high-energy instability. Most are managed conservatively (analgesia, early mobilisation, brace if needed, and crucially osteoporosis treatment - calcium/vitamin D, antiresorptives or anabolics, and a fracture-liaison referral). For the subgroup with severe, persistent pain and an unhealed fracture (marrow oedema on STIR confirming acuity), cement augmentation of the vertebral body is an option: vertebroplasty (cement injected directly) or balloon kyphoplasty (a balloon creates a cavity and partly restores height before low-pressure cement). The evidence is genuinely contested: early sham-controlled trials (INVEST, Buchbinder) showed no benefit over placebo, whereas VAPOUR (early, severely painful acute fractures) and the VERTOS trials suggested faster pain relief in carefully selected acute cases - so augmentation is reserved for the acutely painful, non-healing fracture, not routine use. Always exclude a pathological or malignant cause before augmenting, and remember augmentation treats the pain, not the underlying osteoporosis.
TLICS tells you whether to operate; the Load Sharing (McCormack) Classification helps decide how - specifically whether a short-segment posterior construct will survive or whether the anterior column must be supported. It scores the fractured vertebra 0 to 9 from three CT features, each worth 1-3 points: (1) comminution (less than 30% / 30 to 60% / more than 60% of the body), (2) fragment apposition or spread (minimal / spread of about 2 mm over less than half the body / wide spread over more than half), and (3) kyphotic deformity to correct (3 degrees or less / 4 to 9 degrees / 10 degrees or more). A score of 6 or less is generally safe for short-segment posterior fixation alone; a score of 7 or more predicts failure of a short-segment construct and argues for anterior column reconstruction (corpectomy plus cage), a longer posterior construct, or index-level screws. This is the tool the examiner wants behind "why did this short-segment construct fail?" - the L1 burst in the hardware-failure viva had a high load-sharing score.
Surgical Technique
- Neurological injury: Rare if no deficit pre-op
- Infection: 1-3%
- Hardware failure: 5-15% (higher in short segment)
- Need for revision/additional levels: 5-10%
- Adjacent segment disease: Long-term risk
- DVT/PE: 2-5%
- Imaging: Fluoroscopy or navigation
- Pedicle screws: Appropriate sizes, polyaxial heads
- Rods: Pre-contoured or malleable
- Decompression instruments: If laminectomy planned
- Cell saver: For major reconstructions
Complications
- Incidence
- 5-15%
- Prevention/Management
- Adequate construct length, consider index screws
- Incidence
- 10-20%
- Prevention/Management
- Include index level, cement augmentation in osteoporosis
- Incidence
- 5-10%
- Prevention/Management
- Bone graft, smoking cessation
- Incidence
- Up to 30% long-term
- Prevention/Management
- Short segment when possible
- Incidence
- Less than 1%
- Prevention/Management
- Navigation, neuromonitoring, careful technique
- Incidence
- 1-3%
- Prevention/Management
- Prophylactic antibiotics, meticulous technique
- Incidence
- 2-5%
- Prevention/Management
- Mechanical and chemical prophylaxis
- More common in short segment constructs
- Risk factors: osteoporosis, severe kyphosis, anterior column deficiency
- Prevention: index level screws, cement augmentation, consider anterior column support
- Kyphosis recurrence after initial reduction
- Prevention: adequate construct, address anterior column if significant loss
Postoperative Care
Rehabilitation Timeline
- Wound drain (remove 24-48h)
- DVT prophylaxis
- Pain management
- Early mobilization if neurology intact
- Mobilize with physio
- Brace (TLSO) if additional support desired
- Wound check at 2 weeks
- Progressive activity
- X-rays at 6 weeks
- Core strengthening program
- CT fusion assessment 6-12 months
- Return to work/activity based on imaging and symptoms
- Long-term surveillance for adjacent disease
Bracing post-operatively:
- Variable practice
- Some surgeons use TLSO 6-12 weeks for additional support
- Others rely on instrumentation alone
- Consider in osteoporosis, single-level short segment, compliance concerns
Outcomes and Prognosis
- Intact: Stays intact with appropriate treatment
- Cauda equina: Good potential for recovery if decompressed
- Incomplete cord/conus: Moderate potential
- Complete: Poor neurological prognosis
- Good for stable fractures (TLICS 0-3)
- 10-15% develop progressive kyphosis
- Most return to normal function
- High fusion rates with instrumentation
- Kyphosis correction maintained in 80-85%
- Adjacent segment disease main long-term concern
Guidelines, Registries & Global Practice
Global epidemiology:
Thoracolumbar fractures are the most common spinal column injuries, concentrated at the T10-L2 junction with peak incidence at T12-L1. A bimodal pattern is seen worldwide: high-energy injuries (road trauma, falls from height) in young men, and low-energy osteoporotic fractures in older women. In resource-limited settings, road-traffic and fall mechanisms dominate, and short-segment pedicle screw fixation can be delivered safely and cost-effectively - a Cambodian series reported good neurological recovery in 65% of incomplete spinal cord injuries treated operatively at a cost of US$100-280 per surgery (Chua et al, World Neurosurg 2018, PMID 29550593, DOI).
Guideline and classification landscape (side-by-side):
- Tool
- TLICS score
- Treatment driver
- Morphology + PLC + neurology; surgery if 5 or more
- Evidence basis
- Consensus; reliability validated (Level 4)
- Tool
- AO Spine TL + TL AOSIS
- Treatment driver
- Type A/B/C + neurology + modifiers
- Evidence basis
- International consensus, kappa 0.72 (Level 4)
- Tool
- TLICS-based algorithms
- Treatment driver
- Non-op for intact stable burst
- Evidence basis
- RCT-supported for stable burst (Level 2)
- Tool
- Spinal injury assessment pathway
- Treatment driver
- Imaging triage, early specialist referral
- Evidence basis
- Guideline consensus + evidence review
- Tool
- Spinal clearance & SCI standards
- Treatment driver
- Timely transfer, MRI for cord/PLC
- Evidence basis
- Standards of care (consensus)
- No dedicated international thoracolumbar fracture registry exists comparable to arthroplasty registries; outcome evidence derives from RCTs, prospective cohorts (e.g. STASCIS) and national spinal-injury databases.
- National spinal cord injury registries and trauma networks (e.g. UK Major Trauma Network, Australian state trauma systems, North American Spinal Cord Injury models systems) report epidemiology and rehabilitation outcomes rather than implant survival.
- TLICS 4 (indeterminate): the principal area of global disagreement - surgeon discretion drives wide variation between operative and non-operative care.
- Construct length: short-segment fixation predominates in North America/Europe; longer constructs and routine index-level screws are favoured for higher-energy or osteoporotic patterns.
- Bracing after surgery and for stable burst fractures: practice is inconsistent and increasingly questioned by trials showing equivalence of no-brace protocols.
- Anterior vs posterior approaches: anterior/combined surgery is more common where significant anterior column loss or direct decompression is prioritised.
- Distinguishing features
- High-energy mechanism, acute pain, marrow oedema on STIR
- Key investigation
- CT for morphology, MRI (STIR) for acuity/PLC
- Distinguishing features
- Low-energy/no trauma, older patient, anterior wedging, often multiple
- Key investigation
- MRI for acuity; DEXA; assess for occult malignancy
- Distinguishing features
- Pedicle destruction, posterior wall convexity, soft-tissue mass, known primary
- Key investigation
- MRI with contrast, CT, staging/biopsy
- Distinguishing features
- Benign: retropulsion of a posterior fragment, band-like oedema; malignant: epidural mass, pedicle involvement
- Key investigation
- MRI (diffusion/chemical-shift), biopsy if uncertain
- Distinguishing features
- Rigid fused spine, trivial trauma, transverse 'carrot-stick' fracture, high instability
- Key investigation
- CT whole spine (often unstable; low threshold for fixation)
- Distinguishing features
- Insidious pain, fever, raised inflammatory markers, endplate/disc destruction
- Key investigation
- MRI with contrast, blood cultures, biopsy
- Complete neurological examination at presentation
- TLICS score or equivalent classification
- MRI interpretation for PLC status
- Treatment rationale documented
- Informed consent including hardware failure risks
- Missed diagnosis (inadequate imaging)
- Delayed surgery with neurological deficit
- Failure to document baseline neurology
- Inadequate follow-up and progression to kyphosis
MCQ Practice Points
Q: A patient has an L1 burst fracture with PLC disruption on MRI and is neurologically intact. What is the TLICS score? A: Morphology (burst) = 2 + PLC (disrupted) = 3 + Neurology (intact) = 0 = TLICS 5 (surgical indication)
Q: What structures make up the posterior ligamentous complex? A: Supraspinous ligament, interspinous ligament, ligamentum flavum, and facet joint capsules.
Q: Why is T12-L1 the most common fracture level? A: It is the transition zone between the rigid kyphotic thoracic spine (rib stabilization) and the mobile lordotic lumbar spine. Energy concentrates at this junction.
Q: At what level does the conus medullaris typically end? A: L1-L2 (ranges T12-L2). Injuries above this level involve the cord; below involve only cauda equina.
Q: What modification to short segment fixation reduces failure rates? A: Adding index level screws (screws into the fractured vertebra) improves kyphosis control and reduces implant failure.
Q: What is ligamentotaxis and when does it work? A: Using distraction to reduce retropulsed fragments via the intact PLL. Works best if PLL intact, surgery within 72 hours, and adequate distraction achieved.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old man falls from 4 meters landing on his feet. CT shows an L1 burst fracture with 40% canal compromise. He is neurologically intact. MRI shows no PLC injury. What is your assessment and management?”
“A 35-year-old restrained passenger in an MVA presents with T12-L1 distraction injury on CT. She has ASIA D incomplete paraparesis. MRI confirms PLC disruption and cord edema. Describe your surgical approach.”
“A 55-year-old diabetic smoker presents 6 weeks after posterior short segment fixation (T12-L2) for an L1 burst fracture. X-rays show screw pullout and progressive kyphosis to 30 degrees. How do you manage this?”
TLICS Classification
- Morphology: Compression=1, Burst=2, Translation=3, Distraction=4
- PLC: Intact=0, Indeterminate=2, Injured=3
- Neurology: Intact=0, Root=2, Complete=2, Incomplete=3
- TLICS 0-3=non-op, 4=indeterminate, 5+=surgical
Key Anatomy
- T12-L1 most common (transition zone)
- Conus ends L1-L2 (above=cord, below=cauda)
- Denis three columns: anterior, middle, posterior
- PLC is the key stability determinant
Treatment Algorithm
- TLICS less than 4, PLC intact: TLSO brace 8-12 weeks
- TLICS 5+: Posterior pedicle screw fixation
- Incomplete neuro deficit: Urgent surgery
- Significant anterior loss: Consider combined approach
Surgical Pearls
- Short segment + index screws reduces failure
- Distraction injuries: use COMPRESSION (not distraction)
- Ligamentotaxis works if PLL intact and less than 72h
- Cement augmentation in osteoporosis
Complications
- Hardware failure: 5-15%
- Loss of correction: 10-20%
- Adjacent segment disease: up to 30%
- Risk factors: smoking, diabetes, osteoporosis
Evidence Base
TLICS: Defining Classification
- Introduced the Thoracolumbar Injury Classification and Severity Score (TLICS)
- Three components: injury morphology, posterior ligamentous complex integrity, neurological status
- Composite score stratifies patients into operative and non-operative groups
- Developed by international Spine Trauma Group consensus
AO Spine Thoracolumbar Classification
- International consensus morphological system: Type A (compression), Type B (tension band), Type C (displacement/translation)
- Adds neurological grade (N0-N4, NX) and patient-specific modifiers (M1-M2)
- Substantial interobserver reliability for injury type (kappa = 0.72)
- Designed to harmonise global communication and research
Operative vs Non-operative for Stable Burst Fractures (Long-term RCT)
- Prospective RCT: 47 patients with stable burst fracture and no neurological deficit
- Operative (arthrodesis/instrumentation) vs non-operative (cast/orthosis)
- No significant difference in pain or return to work at mean 44 months
- Complications more frequent in the operative group
Fracture-level (Index) Screw in Short-segment Fixation
- Prospective RCT, 72 patients with unstable thoracolumbar burst fractures, 4 groups
- Adding a screw at the fractured level improved intraoperative correction and its maintenance
- Benefit most pronounced in the short-segment fixation subgroup
- Mean follow-up 50 months
PLC Disruption on CT/MRI: Reliability
- Spine Trauma Study Group inter-rater study of PLC injury indicators
- Facet diastasis on CT was the most reliable single indicator of PLC disruption (kappa = 0.40)
- Posterior oedema-like signal on T2 FAT SAT MRI showed fair agreement (70.5%)
- Identification of frankly disrupted PLC on T1 MRI was poor (48.9% agreement)
Cement Augmentation of Pedicle Screws in Osteoporotic Bone
- Human osteoporotic cadaveric biomechanical study
- PMMA cement augmentation significantly increased pedicle screw pullout strength
- Fenestrated screws confined cement to the vertebral body, reducing canal extrusion risk
- High-viscosity PMMA was safely injectable through fenestrations
Surgical Timing in Acute SCI (STASCIS)
- Prospective multicentre cohort, 313 patients with acute cervical SCI
- Early (less than 24h) vs late decompression
- Early surgery: 19.8% achieved 2 or more grade AIS improvement vs 8.8% late (adjusted OR 2.8)
- No increase in complications or mortality with early surgery